
Serological Responses after a Fourth Dose of SARS-CoV-2 Vaccine in Solid Organ Transplant Recipients: A Systematic Review and Meta-Analysis
Abstract
:1. Introduction
2. Methods
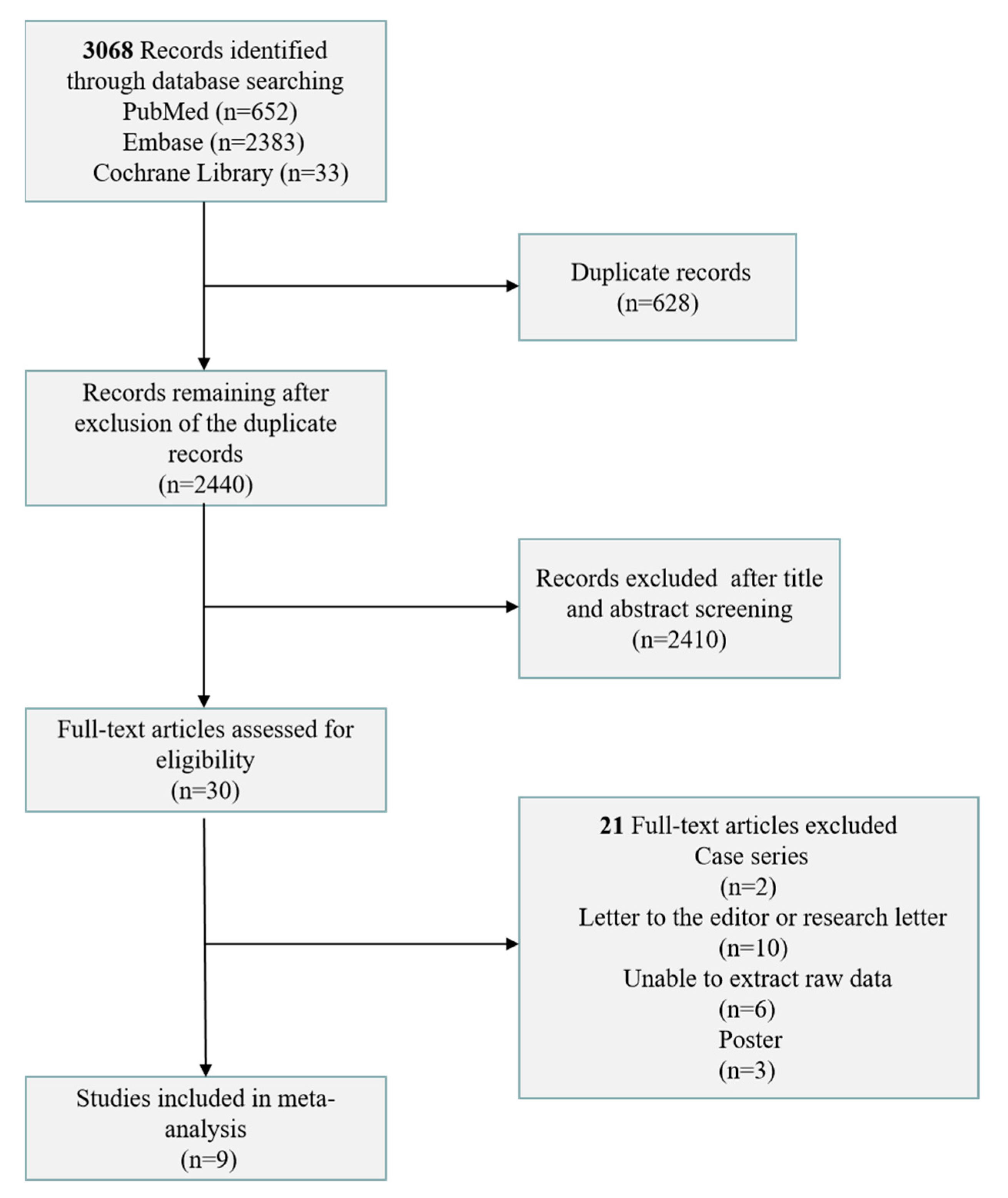
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction
2.4. Outcomes
2.5. Data Analysis
2.6. Assessment of Study Quality
3. Results
3.1. Characteristics of the Included Studies
3.2. Primary Outcome Measurement
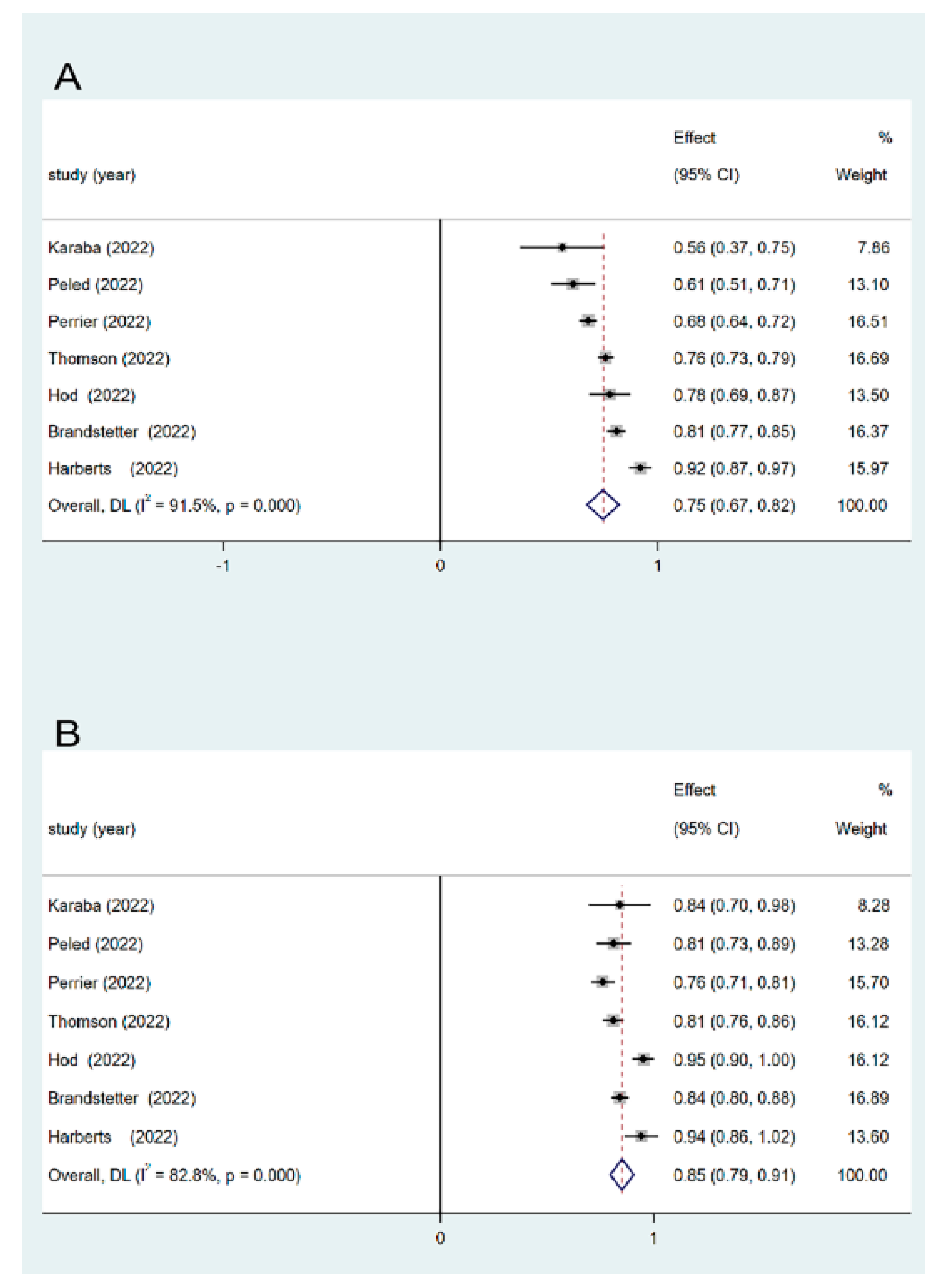
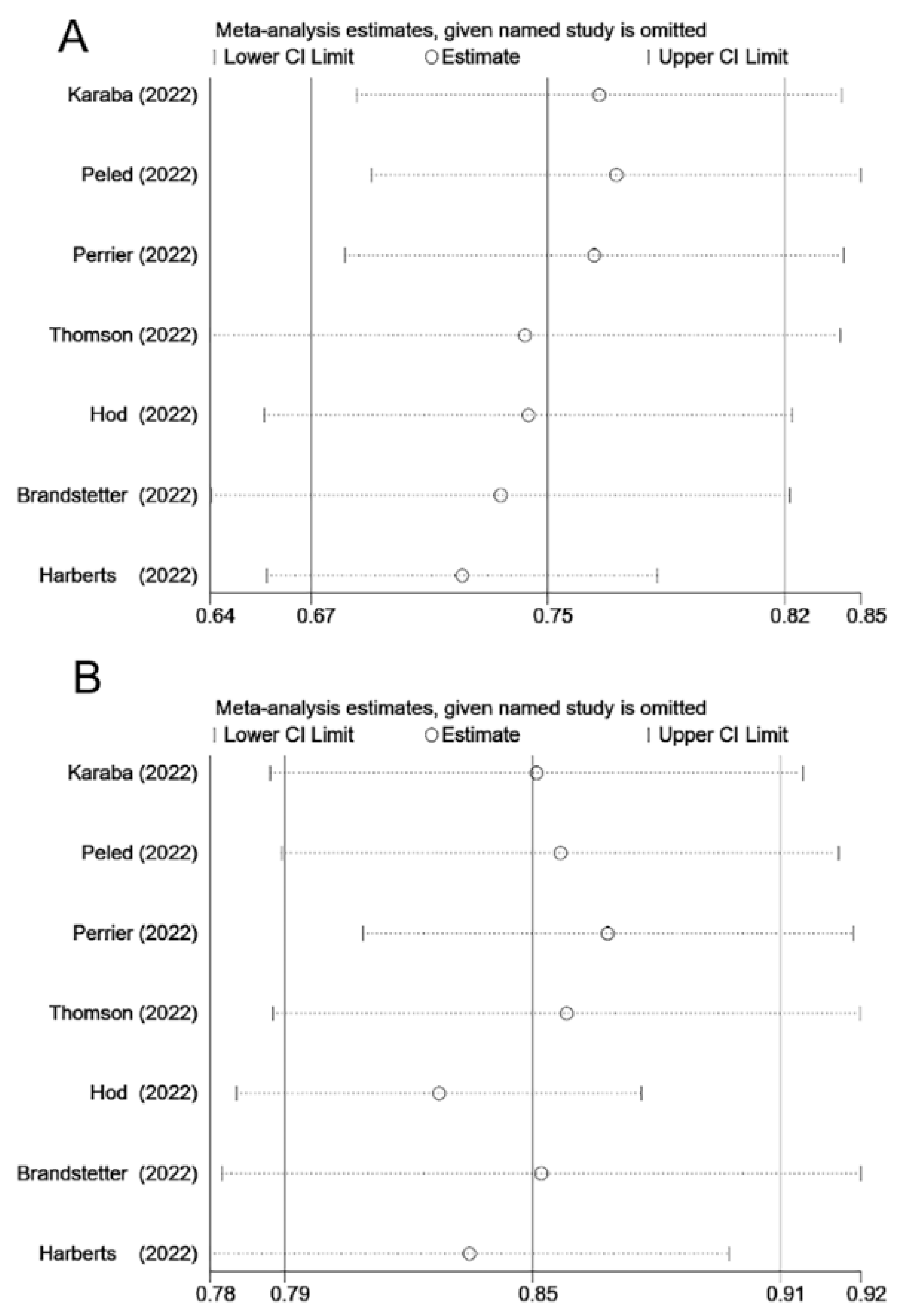
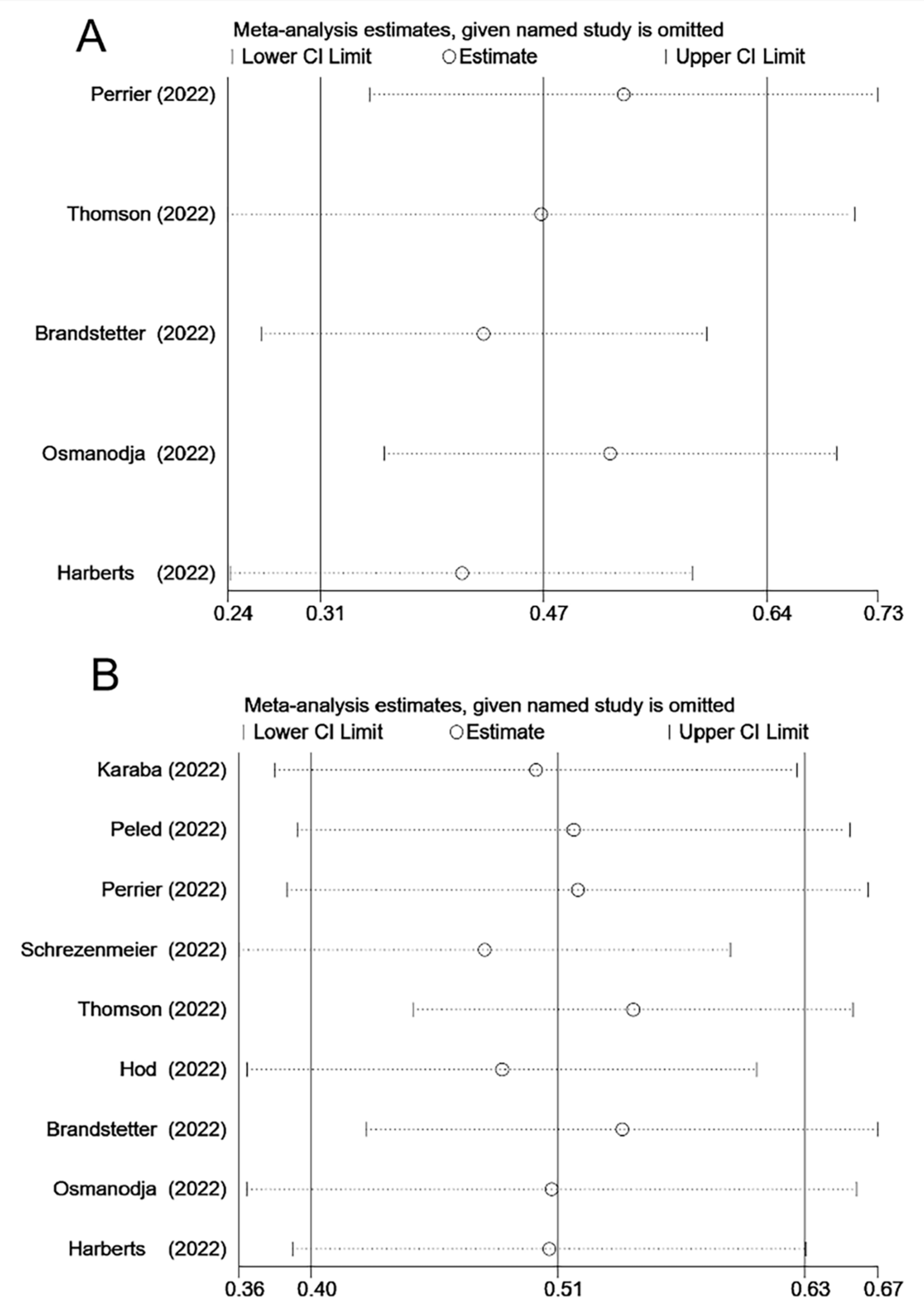
3.3. Seroprevalence Rate in SOT Recipients
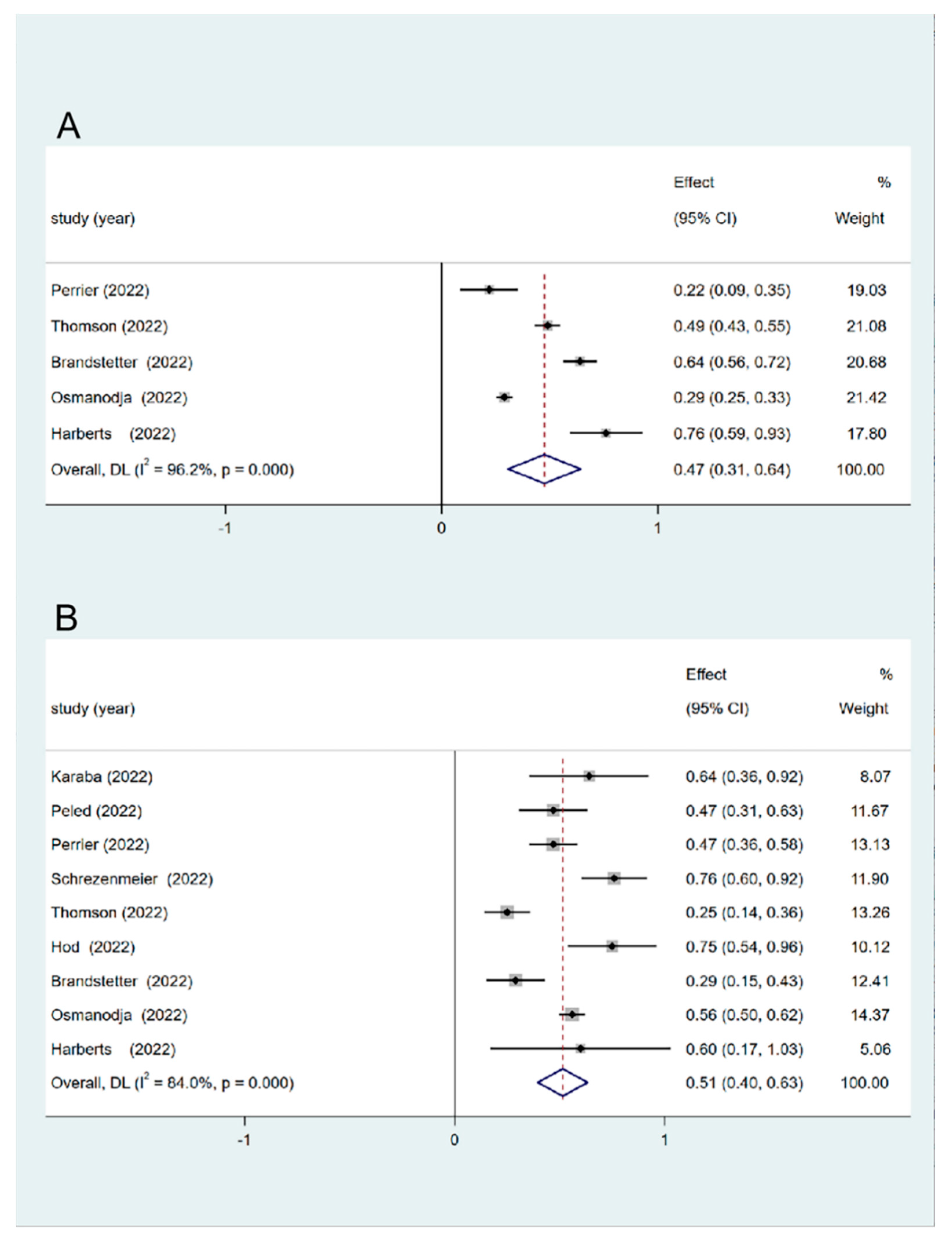
3.4. Seroconversion Rate in SOT Recipients
3.5. Antibody Titers in SOT Recipients
3.6. Factors Associated with a Humoral Immune Response after Vaccination in SOT Patients
3.7. Safety
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Malinis, M.; Cohen, E.; Azar, M.M. Effectiveness of SARS-CoV-2 vaccination in fully vaccinated solid organ transplant recipients. Am. J. Transplant. 2021, 21, 2916–2918. [Google Scholar] [CrossRef]
- Benotmane, I.; Risch, S.; Doderer-Lang, C.; Caillard, S.; Fafi-Kremer, S. Long-term shedding of viable SARS-CoV-2 in kidney transplant recipients with COVID-19. Am. J. Transplant. 2021, 21, 2871–2875. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cardenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against Covid-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef]
- Hall, V.G.; Ferreira, V.H.; Ierullo, M.; Ku, T.; Marinelli, T.; Majchrzak-Kita, B.; Yousuf, A.; Kulasingam, V.; Humar, A.; Kumar, D. Humoral and cellular immune response and safety of two-dose SARS-CoV-2 mRNA-1273 vaccine in solid organ transplant recipients. Am. J. Transplant. 2021, 21, 3980–3989. [Google Scholar] [CrossRef]
- Balsby, D.; Nilsson, A.C.; Petersen, I.; Lindvig, S.O.; Davidsen, J.R.; Abazi, R.; Poulsen, M.K.; Holden, I.K.; Justesen, U.S.; Bistrup, C.; et al. Humoral immune response following a third SARS-CoV-2 mRNA vaccine dose in solid organ transplant recipients compared with matched controls. Front. Immunol. 2022, 13, 1039245. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.; Wong, S.Y.; Chai, L.Y.A.; Lee, S.C.; Lee, M.X.; Muthiah, M.D.; Tay, S.H.; Teo, C.B.; Tan, B.K.J.; Chan, Y.H.; et al. Efficacy of covid-19 vaccines in immunocompromised patients: Systematic review and meta-analysis. BMJ 2022, 376, e068632. [Google Scholar] [CrossRef] [PubMed]
- Manothummetha, K.; Chuleerarux, N.; Sanguankeo, A.; Kates, O.S.; Hirankarn, N.; Thongkam, A.; Dioverti-Prono, M.V.; Torvorapanit, P.; Langsiri, N.; Worasilchai, N.; et al. Immunogenicity and Risk Factors Associated With Poor Humoral Immune Response of SARS-CoV-2 Vaccines in Recipients of Solid Organ Transplant: A Systematic Review and Meta-Analysis. JAMA Netw. Open 2022, 5, e226822. [Google Scholar] [CrossRef]
- Chen, X.; Luo, D.; Mei, B.; Du, J.; Liu, X.; Xie, H.; Liu, L.; Su, S.; Mai, G. Immunogenicity of COVID-19 vaccines in solid organ transplant recipients: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2023, 29, 441–456. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, J.; Alejo, J.L.; Chiang, T.P.Y.; Kim, J.; Chang, A.; Abedon, A.T.; Avery, R.K.; Tobian, A.A.R.; Massie, A.B.; Levan, M.L.; et al. Antibody Response to a Fourth Dose of SARS-CoV-2 Vaccine in Solid Organ Transplant Recipients: An Update. Transplantation 2022, 106, e338–e340. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Hod, T.; Ben-David, A.; Mor, E.; Olmer, L.; Halperin, R.; Indenbaum, V.; Beckerman, P.; Doolman, R.; Asraf, K.; Atari, N.; et al. Humoral Response to the Fourth BNT162b2 Vaccination and Link Between the Fourth Dose, Omicron Infection, and Disease Severity in Renal Transplant Recipients. Transplantation 2023, 107, 192–203. [Google Scholar] [CrossRef]
- Brandstetter, C.; Haller, M.C.; Berger, J.M.; Kerschner, H.; Apfalter, P.; Cejka, D. Humoral response after a third and fourth dose of mRNA-based SARS-CoV-2 vaccine in previously seronegative kidney transplant recipients. Wien. Klin. Wochenschr. 2022, 134, 815–821. [Google Scholar] [CrossRef]
- Harberts, A.; Schaub, G.M.; Ruether, D.F.; Duengelhoef, P.M.; Brehm, T.T.; Karsten, H.; Fathi, A.; Jahnke-Triankowski, J.; Fischer, L.; Addo, M.M.; et al. Humoral and Cellular Immune Response After Third and Fourth SARS-CoV-2 mRNA Vaccination in Liver Transplant Recipients. Clin. Gastroenterol. Hepatol. 2022, 20, 2558–2566 e2555. [Google Scholar] [CrossRef]
- Thomson, T.; Prendecki, M.; Gleeson, S.; Martin, P.; Spensley, K.; De Aguiar, R.C.; Sandhu, B.; Seneschall, C.; Gan, J.; Clarke, C.L.; et al. Immune responses following 3rd and 4th doses of heterologous and homologous COVID-19 vaccines in kidney transplant recipients. EClinicalMedicine 2022, 53, 101642. [Google Scholar] [CrossRef]
- Perrier, Q.; Lupo, J.; Gerster, T.; Augier, C.; Falque, L.; Rostaing, L.; Pelletier, L.; Bedouch, P.; Blanc, M.; Saint-Raymond, C.; et al. SARS-CoV-2 anti-spike antibodies after a fourth dose of COVID-19 vaccine in adult solid-organ transplant recipients. Vaccine 2022, 40, 6404–6411. [Google Scholar] [CrossRef] [PubMed]
- Osmanodja, B.; Ronicke, S.; Budde, K.; Jens, A.; Hammett, C.; Koch, N.; Seelow, E.; Waiser, J.; Zukunft, B.; Bachmann, F.; et al. Serological Response to Three, Four and Five Doses of SARS-CoV-2 Vaccine in Kidney Transplant Recipients. J. Clin. Med. 2022, 11, 2565. [Google Scholar] [CrossRef] [PubMed]
- Karaba, A.H.; Johnston, T.S.; Aytenfisu, T.Y.; Akinde, O.; Eby, Y.; Ruff, J.E.; Abedon, A.T.; Alejo, J.L.; Blankson, J.N.; Cox, A.L.; et al. A Fourth Dose of COVID-19 Vaccine Does Not Induce Neutralization of the Omicron Variant Among Solid Organ Transplant Recipients With Suboptimal Vaccine Response. Transplantation 2022, 106, 1440–1444. [Google Scholar] [CrossRef] [PubMed]
- Peled, Y.; Afek, A.; Nemet, I.; Rahav, G.; Raanani, E.; Patel, J.K.; Mandelboim, M. Fourth BNT162b2 vaccination neutralization of omicron infection after heart transplantation. J. Heart Lung Transplant. 2022, 41, 1210–1213. [Google Scholar] [CrossRef]
- Schrezenmeier, E.; Rincon-Arevalo, H.; Jens, A.; Stefanski, A.L.; Hammett, C.; Osmanodja, B.; Koch, N.; Zukunft, B.; Beck, J.; Oellerich, M.; et al. Temporary antimetabolite treatment hold boosts SARS-CoV-2 vaccination-specific humoral and cellular immunity in kidney transplant recipients. JCI Insight 2022, 7, e157836. [Google Scholar] [CrossRef]
- Gatti, M.; Rinaldi, M.; Bussini, L.; Bonazzetti, C.; Pascale, R.; Pasquini, Z.; Fani, F.; Pinho Guedes, M.N.; Azzini, A.M.; Carrara, E.; et al. Clinical outcome in solid organ transplant recipients affected by COVID-19 compared to general population: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2022, 28, 1057–1065. [Google Scholar] [CrossRef]
- Hall, V.G.; Solera, J.T.; Al-Alahmadi, G.; Marinelli, T.; Cardinal, H.; Poirier, C.; Huard, G.; Prasad, G.V.R.; De Serres, S.A.; Isaac, D.; et al. Severity of COVID-19 among solid organ transplant recipients in Canada, 2020-2021: A prospective, multicentre cohort study. CMAJ 2022, 194, E1155–E1163. [Google Scholar] [CrossRef]
- Verleye, A.; Wijtvliet, V.; Abrams, S.; Hellemans, R.; Bougrea, R.; Massart, A.; Pipeleers, L.; Wissing, K.M.; Arien, K.K.; De Winter, B.Y.; et al. Seroconversion rate after primary vaccination with two doses of BNT162b2 versus mRNA-1273 in solid organ transplant recipients: A systematic review and meta-analysis. Nephrol. Dial. Transplant. 2022, 37, 1566–1575. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.J.; Yon, D.K.; Lee, S.W.; Shin, J.I.; Kim, B.K. Humoral Immunogenicity to SARS-CoV-2 Vaccination in Liver Transplant Recipients: A Systematic Review and Meta-Analysis. Int. J. Biol. Sci. 2022, 18, 5849–5857. [Google Scholar] [CrossRef] [PubMed]
- Boyarsky, B.J.; Werbel, W.A.; Avery, R.K.; Tobian, A.A.R.; Massie, A.B.; Segev, D.L.; Garonzik-Wang, J.M. Antibody Response to 2-Dose SARS-CoV-2 mRNA Vaccine Series in Solid Organ Transplant Recipients. JAMA 2021, 325, 2204–2206. [Google Scholar] [CrossRef] [PubMed]
- Mazzola, A.; Todesco, E.; Drouin, S.; Hazan, F.; Marot, S.; Thabut, D.; Varnous, S.; Soulie, C.; Barrou, B.; Marcelin, A.G.; et al. Poor Antibody Response After Two Doses of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Vaccine in Transplant Recipients. Clin. Infect. Dis. 2022, 74, 1093–1096. [Google Scholar] [CrossRef]
- Kamar, N.; Abravanel, F.; Marion, O.; Couat, C.; Izopet, J.; Del Bello, A. Three Doses of an mRNA Covid-19 Vaccine in Solid-Organ Transplant Recipients. N. Engl. J. Med. 2021, 385, 661–662. [Google Scholar] [CrossRef]
- Chavarot, N.; Morel, A.; Leruez-Ville, M.; Vilain, E.; Divard, G.; Burger, C.; Serris, A.; Sberro-Soussan, R.; Martinez, F.; Amrouche, L.; et al. Weak antibody response to three doses of mRNA vaccine in kidney transplant recipients treated with belatacept. Am. J. Transplant. 2021, 21, 4043–4051. [Google Scholar] [CrossRef]
- Allison, A.C.; Eugui, E.M. Mechanisms of action of mycophenolate mofetil in preventing acute and chronic allograft rejection. Transplantation 2005, 80, S181–S190. [Google Scholar] [CrossRef] [Green Version]
- de Graav, G.N.; Hesselink, D.A.; Dieterich, M.; Kraaijeveld, R.; Weimar, W.; Baan, C.C. Down-Regulation of Surface CD28 under Belatacept Treatment: An Escape Mechanism for Antigen-Reactive T-Cells. PLoS ONE 2016, 11, e0148604. [Google Scholar] [CrossRef] [Green Version]
- Beatty, A.L.; Peyser, N.D.; Butcher, X.E.; Cocohoba, J.M.; Lin, F.; Olgin, J.E.; Pletcher, M.J.; Marcus, G.M. Analysis of COVID-19 Vaccine Type and Adverse Effects Following Vaccination. JAMA Netw. Open 2021, 4, e2140364. [Google Scholar] [CrossRef] [PubMed]
- Massa, F.; Cremoni, M.; Gerard, A.; Grabsi, H.; Rogier, L.; Blois, M.; Couzin, C.; Hassen, N.B.; Rouleau, M.; Barbosa, S.; et al. Safety and cross-variant immunogenicity of a three-dose COVID-19 mRNA vaccine regimen in kidney transplant recipients. EBioMedicine 2021, 73, 103679. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clearly Stated Aim | Inclusion of Consecutive Patients | Prospective Data Collection | Endpoints Appropriate to Study Aim | Unbiased Assessment of Study Endpoint | Follow-Up Period Appropriate To Study Aim | <5% Loss to Follow-Up | Prospective Calculation of Study Size | Adequate Control Group | Contemporary Groups | Baseline Equivalence of Groups | Adequate Statistical Analyses | Total Score | Quality | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Karaba et al. [18] | 2 | 1 | 2 | 1 | 1 | 1 | 2 | 0 | 0 | 0 | 0 | 0 | 10 | low |
| Peled et al. [19] | 2 | 1 | 2 | 2 | 1 | 1 | 2 | 1 | 0 | 0 | 0 | 0 | 12 | low |
| Perrier et al. [16] | 2 | 2 | 2 | 2 | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 2 | 18 | moderate |
| Schrezenmeier et al. [20] | 2 | 1 | 2 | 2 | 1 | 2 | 2 | 0 | 0 | 0 | 0 | 0 | 12 | low |
| Thomson et al. [15] | 2 | 1 | 2 | 2 | 2 | 1 | 1 | 0 | 1 | 2 | 2 | 2 | 18 | moderate |
| Hod et al. [12] | 2 | 2 | 2 | 2 | 1 | 1 | 2 | 1 | 2 | 2 | 2 | 2 | 21 | high |
| Brandstetter et al. [13] | 2 | 1 | 2 | 2 | 2 | 1 | 1 | 1 | 2 | 2 | 2 | 2 | 20 | high |
| Osmanodja et al. [17] | 2 | 2 | 2 | 2 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 2 | 14 | moderate |
| Harberts et al. [14] | 2 | 2 | 2 | 2 | 1 | 2 | 1 | 0 | 2 | 2 | 2 | 2 | 20 | high |
| Study | Country | Population | Sample Size | Male (%) | Age (y), Mean ± SD/ Median (IQR/Range) | Time Post-Transplant (y), Mean ± SD/ Median (IQR/Range) | Type of Vaccine | Immunogenicity Detection Method | Time Interval between 3–4 Dose (d), Mean ± SD/ Median (IQR) | Immunotherapy Drugs |
|---|---|---|---|---|---|---|---|---|---|---|
| Karaba et al. [18] | USA | KT LIT HT LUT PT | 25 | 11 (44%) | 59 (45–66) | 4.3 (2.7–8.8) | BNT162b2 mRNA-1273 Ad26.COV2.S (D3) | CLIA | 93 (28–134) | Prednisone (72%) CNI (96%) MMF (84%) mTOR inhibitor (8%) Belatacept (4%) |
| Peled et al. [19] | USA | HT | 90 | 62 (68.9%) | 57.2 ± 13.8 | 6.5 (3.5–14.1) | BNT162b2 | ELISA | 173.4 ± 4.2 | CNI + MPA + prednisone (54.4%) CNI + MPA (21.1%) CNI + everolimus + prednisone (15.7%) MPA + everolimus + prednisone (2.2%) Everolimus + CNI (3.3%) Everolimus + MPA (1.1%) CNI + prednisone (2.2%) |
| Perrier et al. [16] | France | KT LIT HT LUT | Total: 825 D3: 257 D4: 523 | 550 (66.7%) | 61.2 (50.9–69.3) | 6.7 (3.3–11.9) | BNT162b2 | ELISA | 201 (173–221) | NA |
| Schrezenmeier et al. [20] | Germany | KT | 29 | 17 (58.6%) | 59.8 ± 14.8 | 9.9 ± 5.9 | BNT162b2 | ELISA | 59.1 ± 12.6 | Tac + MPA (13.8%) CS + Tac + MPA (51.7%) CS + CyA + MPA (20.7%) CyA + MPA (3.4%) Belatacept + Aza ± CS (3.4%) Belatacept + MPA ± CS (6.8%) Belatacept + MPA (3.4%) |
| Thomson et al. [15] | UK | KT | D3: 586 D4: 239 | D3: 384 (65.5%) D4: 149 (62.3%) | NA | NA | BNT162b2 mRNA-1273 ChAdOx1-S | ELISA | NA | CNI D3: (46.6%); D4: (40.6%) CNI + MMF/Aza D3: (26.6%); D4: (31.4%) CNI + MMF + prednisone D3: (16.9%); D4: (17.2%) CNI + prednisone D3: (8.7%); D4: (9.2%) MMF/Aza + prednisone D3: (0.3%); D4: (0.4%) |
| Hod et al. [12] | Israel | KT | 74 | 50 (67.6%) | 60.2 (53.3–69.8) | 3.1 (1.5–8.3) | BNT162b2 | ELISA | 173 (172–174) | Tac + MPA + prednisone (44.6%) Tac + MPA (14.9%) Tac + prednisone (27%) CyA (5.4%) Aza (4%) mTOR inhibitor (5.4%) |
| Brandstetter et al. [13] | Austria | KT | Total: 324 D3:147 D4:41 | 217 (67%) | 60.6 (51.4–68.2) | 7.0 (3.4–11.3) | BNT162b2 mRNA-1273 | ELISA | NA | Tac (77.5%) MPA (70.4%) CyA (10.8%) Aza (8.0%) CS (68.5%) mTOR inhibitor (9.3%) |
| Osmanodja et al. [17] | Germany | KT | D3: 603 D4: 250 | D3: 374 (62%) D4: 167 (67%) | D3: 59 (48–68) D4: 61 (51–70) | D3: 8.2 (3.1–13.5) D4: 7.7 (3.0–12.7) | BNT162b2 mRNA-1273 ChAdOx1-S Ad26.COV2.S | ELISA | 64 (55–84) | Tac D3: (73.6%); D4: (73.6%) CyA D3: (16.8%); D4: (16.4%) Belatacept D3: (7.6%); D4: (10%) MPA D3: (93.7%); D4: (50.4%) mTOR inhibitor D3: (1%) Aza D3: (0.8%) |
| Harberts et al. [14] | Germany | LIT | D3: 106 D4: 36 | D3: 64 (60.4%) D4: 23 (63.9%) | D3: 59 (51.0–68.3) D4: 61 (52.5–67.0) | D3: 8.8 (2.6–14.8) D4: 10 (2.6–21.3) | NA | ELISA | 126 (93–148) | Tac D3: (17.9%); D4: (16.7%) CyA D3: (1.9%); D4: (2.8%) mTOR inhibitor D3: (21.7%); D4: (11.1%) MMF D3: (43.4%); D4: (44.4%) CNI D3: (65.1%); D4: (63.9%) Aza D3: (1.9%); D4: (2.8%) prednisone D3: (10.4%); D4: (19.4%) ≥3 immunosuppressants D3: (7.5%); D4: (8.3%) |
| Study | Days from D3 to Antibody Measurement | Seropositive Rate of D3 (%) | Seroconversion Rate of D3 (%) | Antibody Titers of D3 | Days from D4 to Antibody Measurement | Seropositive Rate of D4 (%) | Seroconversion Rate of D4 (%) | Antibody Titers of D4 | Adverse Effect |
|---|---|---|---|---|---|---|---|---|---|
| Karaba et al. [18] | 14 d | 56% | NA | Anti-RBD IgG 43 (83, 115) BAU/mL Anti-S IgG 42 (5134) BAU/mL | 29 (17–38) d | 84% | 64% | Anti-RBD IgG 255 (97, 873) BAU/mL Anti-S IgG 229 (115, 656) BAU/mL | NA |
| Peled et al. [19] | 173 ± 4 d | 61% | NA | Anti-RBD IgG 12.5 AU/mL | 16 ± 4 d | 81% | 47% | Anti-RBD IgG 97 AU/mL | NA |
| Perrier et al. [16] | 122 (72–160) d | 68% | 22% | NA | 32 (28–54) d | 76% | 47% | NA | NA |
| Schrezenmeier et al. [20] | NA | NA | NA | NA | 32 (28–35) d | 76% | NA | NA | |
| Thomson et al. [15] | NA | 76% | 49% | Anti-S IgG 295 (91,611) BAU/mL | NA | 81% | 25% | Anti-S IgG 437 (26, 2211) BAU/mL | NA |
| Hod et al. [12] | 3 wk | 78% | NA | Anti-RBD IgG 38 (95%CI 21, 71) NAb 66 (95%CI 41, 108) | 21 (21, 21) d | 95% | 75% | Anti-RBD IgG 647 (95% CI 361, 1159) NAb 950 (95% CI 550, 1641) | D4: AEs 82.4% (local AEs 75.7% and systemic AEs 37.8%) Injection site pain 76% Fatigue 27% No episodes of rejection were observed. No allergic responses were documented. |
| Brandstetter et al. [13] | 37 (32–40) d | 81% | 64% | Anti-RBD IgG 243 (40, 821) BAU/mL | 26 (26, 27) d | 84% | 29% | Anti-RBD IgG 45 (18, 112) BAU/mL | D3: 1 Biopsy-proven acute rejection |
| Osmanodja et al. [17] | NA | NA | 29% | NA | NA | NA | 56% | NA | NA |
| Harberts et al. [14] | 29.5 (23–49) d | 92% | 76% | Anti-RBD IgG 1891 AU/mL | NA | 94% | 60% | Anti-RBD IgG 1196 AU/mL | D3: pain/swelling, fatigue, headache, vomiting, muscle pain, joint pain, and diarrhea; D4: pain/swelling, fatigue, headache, and muscle pain. |
| Study | Factors | Third Dose | Fourth Dose | ||||
|---|---|---|---|---|---|---|---|
| N | Multivariate OR (95% CI) | p Value | N | Multivariate OR (95% CI) | p Value | ||
| Thomson et al. [15] | CNI monotherapy | 273 | 4.48 (2.69–7.63) | <0.0001 | 97 | 2.44 (1.11–5.80) | 0.033 |
| Diabetes | 200 | 0.49 (0.32–0.75) | 0.001 | NA | NA | NA | |
| Vaccine within the 1st year post-transplant | 534 | 0.28 (0.15–0.54) | 0.0001 | 17 | 0.57 (0.19–1.87) | 0.33 | |
| Osmanodja et al. [17] | Low positive anti-S IgG before vaccination | NA | 28.5 (7.18–201) | <0.001 | NA | 18.7 (4.68–134) | 0.001 |
| Age | NA | 0.98 (0.96–0.99) | 0.016 | NA | 0.96 (0.94–0.99) | 0.004 | |
| BMI | NA | 1.06 (1.01–1.11) | 0.012 | NA | NA | NA | |
| Transplant age | NA | 1.06 (1.03–1.09) | <0.001 | NA | 1.09 (1.04–1.16) | 0.002 | |
| Belatacept | NA | 0.15 (0.03–0.45) | 0.008 | NA | 0.03 (0.004–0.13) | <0.001 | |
| MPA dose in MMF equivalent in g | NA | 0.29 (0.20–0.43) | <0.001 | NA | 0.34 (0.18–0.59) | 0.001 | |
| eGFR in mL/min/1.73 m2 | NA | 1.02 (1.01–1.04) | <0.001 | NA | NA | NA | |
| Hemoglobin | NA | 1.29 (1.13–1.49) | 0.001 | NA | NA | NA | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mu, Y.; Wu, H.; Jiang, Z.; Liu, K.; Xue, X.; Zhang, W.; Chen, Z. Serological Responses after a Fourth Dose of SARS-CoV-2 Vaccine in Solid Organ Transplant Recipients: A Systematic Review and Meta-Analysis. Vaccines 2023, 11, 1130. https://doi.org/10.3390/vaccines11071130
Mu Y, Wu H, Jiang Z, Liu K, Xue X, Zhang W, Chen Z. Serological Responses after a Fourth Dose of SARS-CoV-2 Vaccine in Solid Organ Transplant Recipients: A Systematic Review and Meta-Analysis. Vaccines. 2023; 11(7):1130. https://doi.org/10.3390/vaccines11071130
Chicago/Turabian StyleMu, Yameng, Hongxiao Wu, Zhouling Jiang, Kehang Liu, Xiaoyu Xue, Wei Zhang, and Zhihai Chen. 2023. "Serological Responses after a Fourth Dose of SARS-CoV-2 Vaccine in Solid Organ Transplant Recipients: A Systematic Review and Meta-Analysis" Vaccines 11, no. 7: 1130. https://doi.org/10.3390/vaccines11071130