
Assessment of COVID-19 Vaccine Acceptance and Its Associated Factors during the Crisis: A Community-Based Cross-Sectional Study in Benin
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area and Design
2.2. Study Population and Sample Size
2.3. Participant Selection
2.4. Study Questionnaire and Data Collection Procedures
2.5. General Data
- −
- Data on the household’s demographic characteristics (including age and sex, education of individuals, and occupation).
- −
- Housing characteristics and asset ownership, which were used to build a socioeconomic score.
2.6. Specific Data
- −
- Data on the knowledge, attitudes, and practices (KAP) related to COVID-19, including the knowledge of the symptoms and the modes of transmission of COVID-19; the knowledge and use of preventive measures against COVID-19 (e.g., hand washing and physical distancing); and the knowledge of who is at risk for COVID-19 infection.
- −
- Data on vaccination against COVID-19 (existing treatment, type of vaccines, and information channel for the vaccine).
- −
- Data on the acceptability of being vaccinated against COVID-19 (non-vaccination and unwillingness to be vaccinated, and the reason).
2.7. Data Management and Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. COVID-19 Vaccine Status and Acceptance Level
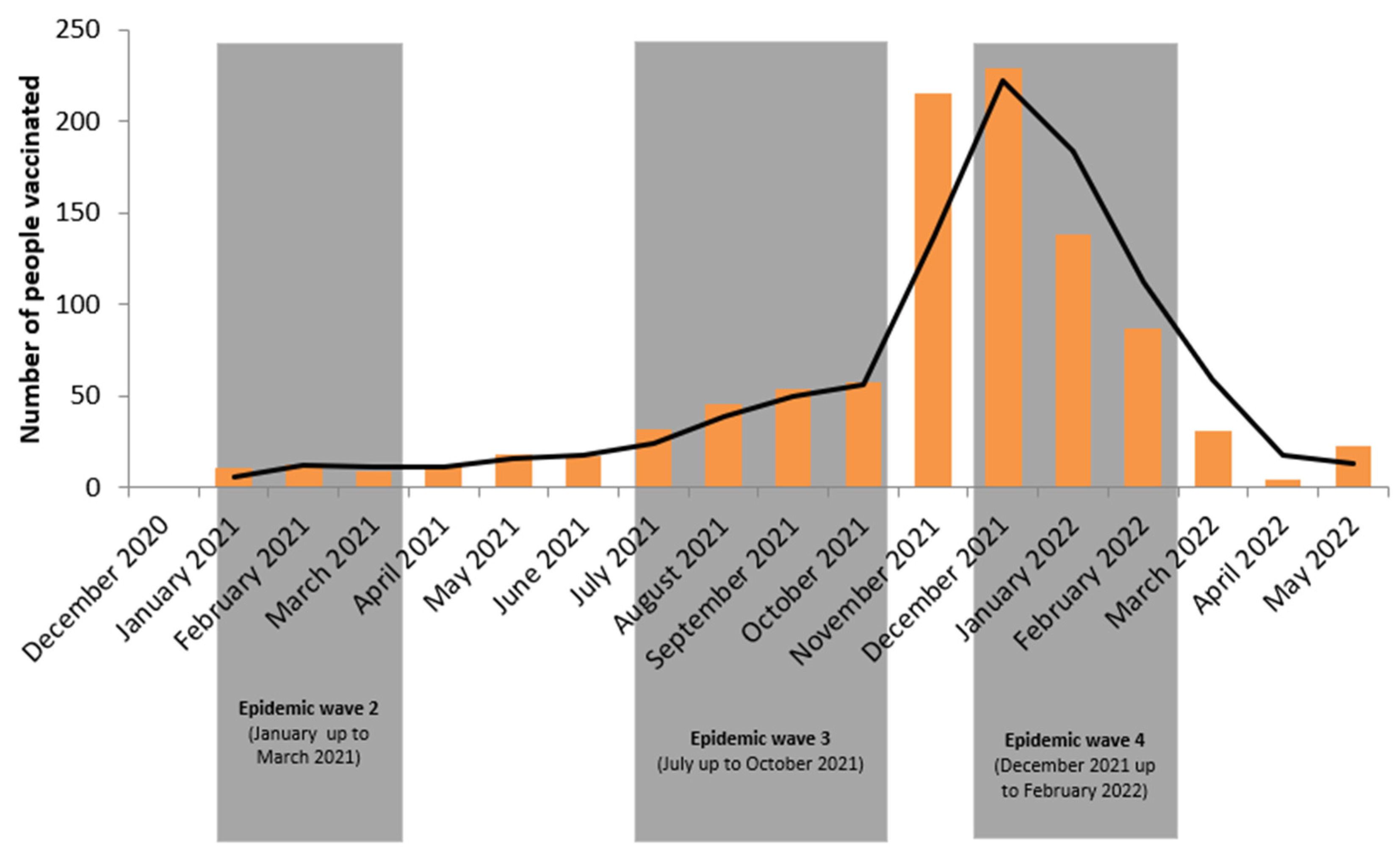
3.3. COVID-19 Vaccine Demand Trend
3.4. Analysis of Potential Factors
4. Discussion
5. Study Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 4 December 2022).
- Chakraborty, C.; Sharma, A.R.; Sharma, G.; Bhattacharya, M.; Saha, R.P.; Lee, S.-S. Extensive Partnership, Collaboration, and Teamwork Is Required to Stop the COVID-19 Outbreak. Arch. Med. Res. 2020, 51, 728–730. [Google Scholar] [CrossRef] [PubMed]
- Lindholt, M.F.; Jørgensen, F.; Bor, A.; Petersen, M.B. Public Acceptance of COVID-19 Vaccines: Cross-National Evidence on Levels and Individual-Level Predictors Using Observational Data. BMJ Open 2021, 11, e048172. [Google Scholar] [CrossRef] [PubMed]
- Mathieu, E.; Ritchie, H.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Hasell, J.; Macdonald, B.; Dattani, S.; Beltekian, D.; Ortiz-Ospina, E.; et al. Coronavirus Pandemic (COVID-19); Our World Data 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Attwell, K.; Betsch, C.; Dubé, E.; Sivelä, J.; Gagneur, A.; Suggs, L.S.; Picot, V.; Thomson, A. Increasing Vaccine Acceptance Using Evidence-Based Approaches and Policies: Insights from Research on Behavioural and Social Determinants Presented at the 7th Annual Vaccine Acceptance Meeting. Int. J. Infect. Dis. 2021, 105, 188–193. [Google Scholar] [CrossRef] [PubMed]
- Fadda, M.; Albanese, E.; Suggs, L.S. When a COVID-19 Vaccine Is Ready, Will We All Be Ready for It? Int. J. Public Health 2020, 65, 711–712. [Google Scholar] [CrossRef]
- Solís Arce, J.S.; Warren, S.S.; Meriggi, N.F.; Scacco, A.; McMurry, N.; Voors, M.; Syunyaev, G.; Malik, A.A.; Aboutajdine, S.; Adeojo, O.; et al. COVID-19 Vaccine Acceptance and Hesitancy in Low- and Middle-Income Countries. Nat. Med. 2021, 27, 1385–1394. [Google Scholar] [CrossRef] [PubMed]
- Grossman, V.A. The COVID-19 Vaccine: Why the Hesitancy? J. Radiol. Nurs. 2021, 40, 116–119. [Google Scholar] [CrossRef] [PubMed]
- Gouvernement de la Ministry of Health. République du Bénin Coronavirus (COVID-19) Information. Available online: https://www.gouv.bj/coronavirus/ (accessed on 10 May 2022).
- Worldometer Benin Population. 2023. Available online: https://www.worldometers.info/world-population/benin-population/ (accessed on 10 June 2023).
- Osseni, I.A. Benin Responds to COVID-19: Sanitary Cordon without Generalized Containment or Lockdown? Trop. Med. Health 2020, 48, 46. [Google Scholar] [CrossRef] [PubMed]
- Dean, A.G.; Sullivan, K.M.; Soe, M.M. OpenEpi: Open Source Epidemiologic Statistics for Public Health, Version. Available online: www.openepi.com (accessed on 10 January 2021).
- National Institute of Statistics and Economic Analysis (INSAE). Benin Demographic and Health Survey 2017–2018; National Institute of Statistics and Economic Analysis (INSAE): Calverton, MD, USA, 2018. [Google Scholar]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef]
- McAbee, L.; Tapera, O.; Kanyangarara, M. Factors Associated with COVID-19 Vaccine Intentions in Eastern Zimbabwe: A Cross-Sectional Study. Vaccines 2021, 9, 1109. [Google Scholar] [CrossRef]
- Acheampong, T.; Akorsikumah, E.A.; Osae-Kwapong, J.; Khalid, M.; Appiah, A.; Amuasi, J.H. Examining Vaccine Hesitancy in Sub-Saharan Africa: A Survey of the Knowledge and Attitudes among Adults to Receive COVID-19 Vaccines in Ghana. Vaccines 2021, 9, 814. [Google Scholar] [CrossRef]
- Iliyasu, Z.; Umar, A.A.; Abdullahi, H.M.; Kwaku, A.A.; Amole, T.G.; Tsiga-Ahmed, F.I.; Garba, R.M.; Salihu, H.M.; Aliyu, M.H. “They Have Produced a Vaccine, but We Doubt If COVID-19 Exists”: Correlates of COVID-19 Vaccine Acceptability among Adults in Kano, Nigeria. Hum. Vaccines Immunother. 2021, 17, 4057–4064. [Google Scholar] [CrossRef] [PubMed]
- Mudenda, S.; Hikaambo, C.N.; Daka, V.; Chileshe, M.; Mfune, R.L.; Kampamba, M.; Kasanga, M.; Phiri, M.; Mufwambi, W.; Banda, M.; et al. Prevalence and Factors Associated with COVID-19 Vaccine Acceptance in Zambia: A Web-Based Cross-Sectional Study. Pan Afr. Med. J. 2022, 41, 112. [Google Scholar] [CrossRef] [PubMed]
- Ackah, B.B.B.; Woo, M.; Stallwood, L.; Fazal, Z.A.; Okpani, A.; Ukah, U.V.; Adu, P.A. COVID-19 Vaccine Hesitancy in Africa: A Scoping Review. Glob. Health Res. Policy 2022, 7, 21. [Google Scholar] [CrossRef] [PubMed]
- Stojanovic, J.; Boucher, V.G.; Gagne, M.; Gupta, S.; Joyal-Desmarais, K.; Paduano, S.; Aburub, A.S.; Sheinfeld Gorin, S.N.; Kassianos, A.P.; Ribeiro, P.A.B.; et al. Global Trends and Correlates of COVID-19 Vaccination Hesitancy: Findings from the ICARE Study. Vaccines 2021, 9, 661. [Google Scholar] [CrossRef] [PubMed]
- Alqudeimat, Y.; Alenezi, D.; AlHajri, B.; Alfouzan, H.; Almokhaizeem, Z.; Altamimi, S.; Almansouri, W.; Alzalzalah, S.; Ziyab, A.H. Acceptance of a COVID-19 Vaccine and Its Related Determinants among the General Adult Population in Kuwait. Med. Princ. Pract. 2021, 30, 262–271. [Google Scholar] [CrossRef]
- Williams, L.; Gallant, A.J.; Rasmussen, S.; Brown Nicholls, L.A.; Cogan, N.; Deakin, K.; Young, D.; Flowers, P. Towards Intervention Development to Increase the Uptake of COVID-19 Vaccination among Those at High Risk: Outlining Evidence-Based and Theoretically Informed Future Intervention Content. Br. J. Health Psychol. 2020, 25, 1039–1054. [Google Scholar] [CrossRef] [PubMed]
- Ba, M.F.; Faye, A.; Kane, B.; Diallo, A.I.; Junot, A.; Gaye, I.; Bonnet, E.; Ridde, V. Factors Associated with COVID-19 Vaccine Hesitancy in Senegal: A Mixed Study. Hum. Vaccines Immunother. 2022, 18, 2060020. [Google Scholar] [CrossRef]
- Faye, S.L.B.; Krumkamp, R.; Doumbia, S.; Tounkara, M.; Strauss, R.; Ouedraogo, H.G.; Sagna, T.; Barry, A.M.; Mbawah, A.K.; Doumbia, C.O.; et al. Factors Influencing Hesitancy towards Adult and Child COVID-19 Vaccines in Rural and Urban West Africa: A Cross-Sectional Study. BMJ Open 2022, 12, e059138. [Google Scholar] [CrossRef]
- One Africa Data Dive: The Astoundingly Unequal Global COVID-19 Response. Available online: https://www.one.org/africa/issues/covid-19-tracker/explore-covid-response/ (accessed on 17 August 2022).
- Berkley, S. COVAX: More than a Beautiful Idea. Lancet Lond. Engl. 2021, 398, 388. [Google Scholar] [CrossRef]
- Wouters, O.J.; Shadlen, K.C.; Salcher-Konrad, M.; Pollard, A.J.; Larson, H.J.; Teerawattananon, Y.; Jit, M. Challenges in Ensuring Global Access to COVID-19 Vaccines: Production, Affordability, Allocation, and Deployment. Lancet 2021, 397, 1023–1034. [Google Scholar] [CrossRef]
- Ozawa, S.; Stack, M.L. Public Trust and Vaccine Acceptance--International Perspectives. Hum. Vaccines Immunother. 2013, 9, 1774–1778. [Google Scholar] [CrossRef] [PubMed]
- Loomba, S.; Figueiredo, A.; Piatek, S.J.; Graaf, K.; Larson, H.J. Measuring the Impact of COVID-19 Vaccine Misinformation on Vaccination Intent in the UK and USA. Nat. Hum. Behav. 2021, 5, 337–348. [Google Scholar] [CrossRef] [PubMed]
- Kumar, D.; Chandra, R.; Mathur, M.; Samdariya, S.; Kapoor, N. Vaccine Hesitancy: Understanding Better to Address Better. Isr. J. Health Policy Res. 2016, 5, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adjaottor, E.S.; Addo, F.-M.; Ahorsu, F.A.; Chen, H.-P.; Ahorsu, D.K. Predictors of COVID-19 Stress and COVID-19 Vaccination Acceptance among Adolescents in Ghana. Int. J. Environ. Res. Public. Health 2022, 19, 7871. [Google Scholar] [CrossRef] [PubMed]
- Glik, D.; Massey, P.; Gipson, J.; Dieng, T.; Rideau, A.; Prelip, M. Health-Related Media Use among Youth Audiences in Senegal. Health Promot. Int. 2016, 31, 73–82. [Google Scholar] [CrossRef] [Green Version]
- Du, F.; Chantler, T.; Francis, M.R.; Sun, F.Y.; Zhang, X.; Han, K.; Rodewald, L.; Yu, H.; Tu, S.; Larson, H.; et al. Access to Vaccination Information and Confidence/Hesitancy towards Childhood Vaccination: A Cross-Sectional Survey in China. Vaccines 2021, 9, 201. [Google Scholar] [CrossRef]
- Borzekowski, D.L.G.; Fobil, J.N.; Asante, K.O. Online Access by Adolescents in Accra: Ghanaian Teens’ Use of the Internet for Health Information. Dev. Psychol. 2006, 42, 450–458. [Google Scholar] [CrossRef] [Green Version]
- Denno, D.M.; Hoopes, A.J.; Chandra-Mouli, V. Effective Strategies to Provide Adolescent Sexual and Reproductive Health Services and to Increase Demand and Community Support. J. Adolesc. Health Off. Publ. Soc. Adolesc. Med. 2015, 56, S22–S41. [Google Scholar] [CrossRef] [Green Version]
- Zheng, H.; Jiang, S.; Wu, Q. Factors Influencing COVID-19 Vaccination Intention: The Roles of Vaccine Knowledge, Vaccine Risk Perception, and Doctor-Patient Communication. Patient Educ. Couns. 2022, 105, 277–283. [Google Scholar] [CrossRef]
- Adedeji-Adenola, H.; Olugbake, O.A.; Adeosun, S.A. Factors Influencing COVID-19 Vaccine Uptake among Adults in Nigeria. PloS One 2022, 17, e0264371. [Google Scholar] [CrossRef]
- Katoto, P.D.M.C.; Parker, S.; Coulson, N.; Pillay, N.; Cooper, S.; Jaca, A.; Mavundza, E.; Houston, G.; Groenewald, C.; Essack, Z.; et al. Predictors of COVID-19 Vaccine Hesitancy in South African Local Communities: The VaxScenes Study. Vaccines 2022, 10, 353. [Google Scholar] [CrossRef] [PubMed]
- Gisondi, M.A.; Barber, R.; Faust, J.S.; Raja, A.; Strehlow, M.C.; Westafer, L.M.; Gottlieb, M. A Deadly Infodemic: Social Media and the Power of COVID-19 Misinformation. J. Med. Internet Res. 2022, 24, e35552. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Proportion, % (n) | |
|---|---|---|
| Study districts | Cotonou | 20.1% (416) |
| Abomey-Calavi | 36.6% (758) | |
| Porto-Novo | 29.3% (607) | |
| Djougou | 13.9% (288) | |
| Residence | Urban | 59.9% (1241) |
| Rural | 35.6% (736) | |
| Semi-rural | 4.5% (92) | |
| Age (years) | 12–17 | 2.6% (53) |
| 18–29 | 32.7% (677) | |
| 30–39 | 26.9% (557) | |
| 40–49 | 16.0% (331) | |
| 50–59 | 10.8% (224) | |
| ≥60 | 11.0% (227) | |
| Sex | Female | 53.7% (1111) |
| Male | 46.3% (958) | |
| Number of people living in the household | <4 | 42.5% (880) |
| ≥4 | 57.5% (1189) | |
| Education | None | 16.9% (350) |
| Primary | 26.0% (538) | |
| Secondary | 23.4% (484) | |
| High secondary | 17.1% (354) | |
| College | 16.6% (343) | |
| Ethnic group | Fon and related | 30.3% (626) |
| Goun | 20.3% (421) | |
| Dendi | 6.8% (141) | |
| Aizo | 5.2% (107) | |
| Others * | 30.1% (622) | |
| Marital status | Single | 19.6% (405) |
| Married | 68.3% (1413) | |
| Divorced | 5.0% (104) | |
| Widowed | 7.1% (147) | |
| Religion | Christian | 60.4% (1249) |
| Muslim | 26.9% (556) | |
| Traditional | 7.5% (155) | |
| Others | 5.3% (109) | |
| Channel of COVID-19 information | ||
| Radio | Yes | 77.5% (1604) |
| Television | Yes | 69.4% (1435) |
| Newspaper | Yes | 9.4% (194) |
| Social network | Yes | 46.9% (972) |
| Internet | Yes | 18.6% (385) |
| Healthcare workers | Yes | 21.1% (436) |
| Community political leaders | Yes | 31.8% (658) |
| Religious leaders | Yes | 42.6% (882) |
| Word-of-mouth | Yes | 80.1% (1658) |
| Others | Yes | 0.9% (18) |
| Characteristics | Proportion, % (n) | |
|---|---|---|
| Medical conditions | ||
| High blood pressure | Yes | 11.0% (220) |
| Diabetes | Yes | 2.8% (58) |
| Cardiac disease | Yes | 1.0% (21) |
| Thromboembolic disease | Yes | 0.2% (4) |
| Tumors | Yes | 0.3% (6) |
| Immunodeficiency | Yes | 0.3% (6) |
| Tobacco history | Yes | 3.8% (78) |
| COVID-19 infection | Yes | 3.7% (77) |
| Overall knowledge of COVID-19 | Poor | 29.6% (612) |
| Moderate | 30.6% (633) | |
| Good | 39.8% (824) | |
| Knowledge of mode of transmission | Poor | 30.3% (627) |
| Moderate | 37.7% (779) | |
| Good | 32.0% (663) | |
| Knowledge of symptoms | Poor | 34.9% (722) |
| Moderate | 18.8% (389) | |
| Good | 46.3% (958) | |
| Prevention, own behaviors (attitude) | Poor | 38.9% (804) |
| Moderate | 34.5% (713) | |
| Good | 26.7% (552) | |
| Behaviors (practices) | Poor | 51.0% (1056) |
| Moderate | 12.5% (259) | |
| Good | 36.4% (754) | |
| The scale of fear of being infected * | Low (<6) | 74.2% (1536) |
| Moderate (6–7) | 7.3% (151) | |
| High (≥8) | 18.5% (382) |
| Characteristics | Proportion, % (n) | |
|---|---|---|
| Declared vaccine status | Not vaccinated | 43.2% (895) |
| Willing to be vaccinated | 8.1% (167) | |
| Vaccinated | 48.7% (1007) | |
| Confirmed vaccine status | No, proof was not accessible | 6.8% (141) |
| No, proof was not found | 17.3% (358) | |
| No, refused to show proof | 0.4% (8) | |
| Yes, proof was presented | 24.2% (500) | |
| Not applicable * | 51.3% (1062) | |
| Vaccine status with proof | No | 76.8% (1569) |
| Yes | 24.2% (500) | |
| Crude vaccine acceptance 1 | No | 32.1% (665) |
| Yes | 67.9% (1404) | |
| Adjusted vaccine acceptance 2 | No | 56.6% (1172) |
| Yes | 43.4% (897) |
| Factors | Vaccine Acceptance (%), n/N | Crude Analysis | Adjusted Analysis | |||
|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | aOR (95% CI) | p-Value | |||
| District of residence | Cotonou | 61.3% (255/416) | 1 | 1 | ||
| Abomey-Calavi | 66.2% (502/758) | 1.21 (0.81–1.81) | 0.3560 | 1.23 (0.87–1.73) | 0.1205 | |
| Porto-Novo | 69.4% (421/607) | 1.71 (1.14–2.56) | 0.4120 | 1.59 (1.10–2.29) | 0.0041 | |
| Djougou | 78.5% (226/288) | 2.55 (1.57–4.12) | 0.0007 | 2.70 (1.71–4.28) | 0.0002 | |
| Residence area | Urban | 66.4% (824/1241) | 1 | |||
| Semi-rural | 77.2% (71/92) | 1.51 (0.75–3.08) | 0.2410 | 1.08 (0.86–1.36) | 0.2506 | |
| Rural | 69.2% (509/736) | 1.26 (0.95–1.66) | 0.1787 | 1.91 (0.55–1.5) | 0.3156 | |
| Gender | Male | 70.5% (675/958) | 1 | |||
| Female | 65.6% (729/1111) | 0.79 (0.65–0.96) | 0.0189 | 0.91 (0.97–1.45) | 0.2012 | |
| Age (years) | 12–17 | 58.5% (31/53) | 1 | |||
| 18–29 | 67.1% (454/677) | 1.73 (0.95–3.17) | 0.4231 | 1.93 (0.85–2.37) | 0.7142 | |
| 30–39 | 67.7% (377/557) | 1.85 (1.00–3.40) | 0.3450 | 1.94 (0.75–4.14) | 0.6025 | |
| 40–49 | 69.5% (230/331) | 1.96 (1.04–3.67) | 0.6120 | 1.69 (0.84–3.71) | 0.5014 | |
| 50–59 | 72.8% (163/224) | 2.58 (1.33–4.98) | 0.8410 | 1.85 (0.83–4.98) | 0.9085 | |
| ≥60 | 65.6% (149/227) | 1.67 (0.88–3.19) | 0.0747 | 1.67 (0.98–2.19) | 0.0512 | |
| Education level | None | 63.4% (222/350) | 1 | 1 | ||
| Primary | 65.1% (350/538) | 1.27 (0.94–1.71) | 0.2410 | 1.21 (0.89–1.66) | 0.3541 | |
| Secondary | 65.5% (317/484) | 1.21 (0.89–1.65) | 0.2651 | 1.13 (0.82–1.57) | 0.4120 | |
| High secondary | 69.2% (245/354) | 1.43 (1.02–2.01) | 0.1510 | 1.26 (0.88–1.81) | 0.2520 | |
| College | 78.7% (270/343) | 2.41 (1.67–3.48) | 0.0001 | 1.88 (1.25–2.81) | 0.0305 | |
| Religion | Others | 65.1% (71/109) | 1 | 1 | ||
| Christian | 64.9% (811/1249) | 1.06 (0.69–1.64) | 0.4521 | 1.22 (0.42–3.35) | 0.7120 | |
| Muslim | 75.9% (422/556) | 1.52 (0.95–2.46) | 0.1241 | 1.12 (0.82, 1.53) | 0.5120 | |
| Traditional | 64.5% (100/155) | 1.05 (0.61–1.80) | 0.0569 | 1.05 (0.85, 1.82) | 0.3121 | |
| Scale of fear of being infected * | Low | 65.5% (1006/1536) | 1 | 1 | ||
| Moderate | 76.2% (115/151) | 1.72 (1.15–2.57) | 0.0002 | 1.60 (1.06–2.41) | 0.0001 | |
| High | 74.1% (283/382) | 1.34 (1.03–1.76) | 0.0055 | 1.25 (0.94–1.65) | 0.0319 | |
| Channel of information | ||||||
| Television | 70.6% (1013/1435) | 1.34 (1.08–1.66) | 0.0074 | 5.43 (1.56–2.3) | 0.0081 | |
| Newspaper | 74.2% (144/194) | 1.35 (0.94–1.94) | 0.1060 | 1.97 (0.61–3.26) | 0.1256 | |
| Social network | 74.9% (728/972) | 1.72 (1.39–2.12) | <0.0001 | 1.81 (1.25–2.68) | <0.0001 | |
| Internet | 77.7% (299/385) | 1.77 (1.34–2.34) | 0.0001 | 1.32 (1.15–2.62) | <0.0001 | |
| Healthcare workers | 78.9% (344/436) | 1.75 (1.33–2.31) | 0.0001 | 1.33 (1.05–2.62) | <0.0001 | |
| Community political leaders | 75.4% (496/658) | 1.47 (1.16–1.86) | 0.0016 | 1.32 (1.03–1.69) | 0.0277 | |
| Religious leaders | 73.4% (647/882) | 1.38 (1.11–1.72) | 0.0043 | 1.63 (1.05–1.68) | 0.0325 | |
| Word-of-mouth | 69.7% (1155/1658) | 1.30(1.01–1.68) | 0.0413 | 1.47 (1.05–1.88) | 0.0452 | |
| Medical conditions | ||||||
| High blood pressure | 71.8% (158/220) | 1.29 (0.93–1.77) | 0.1225 | 1.43 (1.03–1.99) | 0.0326 | |
| Cardiac disease | 42.9% (9/21) | 0.34 (0.14–0.84) | 0.0199 | 0.30 (0.12–0.77) | 0.0128 | |
| Kidney failure | 42.9% (3/7) | 0.35 (0.07–1.63) | 0.1794 | 0.25 (0.06–1.43) | 0.2135 | |
| Overall knowledge of COVID-19 | Poor | 58.5% (358/612) | 1 | |||
| Moderate | 66.8% (423/633) | 1.52 (1.19–1.94) | 0.0051 | 1.52 (1.19–1.94) | 0.0004 | |
| Good | 75.6% (623/824) | 2.24 (1.76–2.86) | <0.0001 | 2.24 (1.76–2.86) | <0.0001 | |
| Knowledge of the mode of transmission | Poor | 64.1% (402/627) | 1 | 1 | ||
| Moderate | 70.3% (548/779) | 1.46 (1.15–1.87) | 0.0042 | 1.04 (0.80–1.35) | 0.0512 | |
| Good | 68.5% (454/663) | 1.29 (1.01–1.67) | 0.0078 | 0.76 (0.57–1.01) | 0.0478 | |
| Knowledge of symptoms | Poor | 59% (426/722) | 1 | 1 | ||
| Moderate | 68.1% (265/389) | 1.51 (1.14–1.99) | <0.0001 | 1.48 (1.11–1.99) | <0.0001 | |
| Good | 74.4% (713/958) | 1.98 (1.59–2.48) | <0.0001 | 1.62 (1.24–2.12) | 0.0004 | |
| Own behaviors (attitude) | Poor | 59.7% (480/804) | 1 | 1 | ||
| Moderate | 72.2% (515/713) | 1.69 (1.35–2.13) | <0.0001 | 1.41 (1.10–1.79) | <0.0001 | |
| Good | 74.1% (409/552) | 2.05 (1.58–2.65) | <0.0001 | 1.69 (1.27–2.24) | 0.0006 | |
| Behaviors (practices) | Poor | 64.8% (684/1056) | 1 | 1 | ||
| Moderate | 67.9% (176/259) | 1.19 (0.87–1.61) | 0.0651 | 1.39 (0.70–1.77) | 0.2317 | |
| Good | 72.1% (544/754) | 1.49 (1.20–1.87) | 0.0017 | 1.60 (1.28–2.61) | <0.0001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Padonou, S.G.R.; Kakaï Glèlè, C.; Accrombessi, M.; Adegbite, B.R.; Dangbenon, E.; Bah, H.; Akogbeto, E.; Bah Chabi, A.I.; Kaucley, L.; Sourakatou, S.; et al. Assessment of COVID-19 Vaccine Acceptance and Its Associated Factors during the Crisis: A Community-Based Cross-Sectional Study in Benin. Vaccines 2023, 11, 1104. https://doi.org/10.3390/vaccines11061104
Padonou SGR, Kakaï Glèlè C, Accrombessi M, Adegbite BR, Dangbenon E, Bah H, Akogbeto E, Bah Chabi AI, Kaucley L, Sourakatou S, et al. Assessment of COVID-19 Vaccine Acceptance and Its Associated Factors during the Crisis: A Community-Based Cross-Sectional Study in Benin. Vaccines. 2023; 11(6):1104. https://doi.org/10.3390/vaccines11061104
Chicago/Turabian StylePadonou, Sètondji Géraud Roméo, Clément Kakaï Glèlè, Manfred Accrombessi, Bayode Romeo Adegbite, Edouard Dangbenon, Houssaïnatou Bah, Enangnon Akogbeto, Ali Imorou Bah Chabi, Landry Kaucley, Salifou Sourakatou, and et al. 2023. "Assessment of COVID-19 Vaccine Acceptance and Its Associated Factors during the Crisis: A Community-Based Cross-Sectional Study in Benin" Vaccines 11, no. 6: 1104. https://doi.org/10.3390/vaccines11061104