
COVID-19 Impact on DTP Vaccination Trends in Africa: A Joinpoint Regression Analysis
 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ota, M.O.C.; de Moraes, J.C.; Vojtek, I.; Constenla, D.; Doherty, T.M.; Cintra, O.; Kirigia, J.M. Unveiling the Contributions of Immunization for Progressing towards Universal Health Coverage. Hum. Vaccin. Immunother. 2022, 18, e2036048. [Google Scholar] [CrossRef] [PubMed]
- Suffel, A.M.; Ojo-Aromokudu, O.; Carreira, H.; Mounier-Jack, S.; Osborn, D.; Warren-Gash, C.; McDonald, H.I. Exploring the Impact of Mental Health Conditions on Vaccine Uptake in High-Income Countries: A Systematic Review. BMC Psychiatry 2023, 23, 15. [Google Scholar] [CrossRef] [PubMed]
- Hassan, M.N. A Survey on Hygienic Practices and Immunization Coverage among 12–59 Months Old Children in Urban Slum, Barishal, Bangladesh. Asian J. Med. Biol. Res. 2022, 8, 277–285. [Google Scholar] [CrossRef]
- Stein, R.A. Vaccination: A Public Health Intervention That Changed History & Is Changing with History. Am. Biol. Teach. 2011, 73, 513–519. [Google Scholar] [CrossRef]
- Pan, J.; Wang, Y.; Cao, L.; Wang, Y.; Zhao, Q.; Tang, S.; Gong, W.; Guo, L.; Liu, Z.; Wen, Z.; et al. Impact of Immunization Programs on 11 Childhood Vaccine-Preventable Diseases in China: 1950–2018. Innovation 2021, 2, 100113. [Google Scholar] [CrossRef] [PubMed]
- Espinal, M.A. The Pan American Health Organization: 120 Years in the Americas Hemisphere. Lancet Reg. Health Am. 2023, 21, 100488. [Google Scholar] [CrossRef]
- Zulfan, G.P.; Sihombing, J.A.; Amin, D.M.; Widiantari, A.D.; Berti, M.P.E.; Murtiani, F. Clinical Manifestation of Childhood Diphtheria. J. Ilm. Kedokt. Wijaya. Kusuma 2023, 12, 1. [Google Scholar] [CrossRef]
- WHO. Global. Vaccine Action Plan 2011–2020; WHO Press: Geneva, Switzerland, 2013; Available online: https://www.who.int/teams/immunization-vaccines-and-biologicals/strategies/global-vaccine-action-plan#:~:text=The%20Global%20Vaccine%20Action%20Plan%20(GVAP)%20%E2%80%95%20endorsed%20by%20the,for%20people%20in%20all%20communities (accessed on 29 April 2023).
- Macina, D.; Evans, K.E. Bordetella Pertussis in School-Age Children, Adolescents, and Adults: A Systematic Review of Epidemiology, Burden, and Mortality in Africa. Infect. Dis. Ther. 2021, 10, 1097–1113. [Google Scholar] [CrossRef]
- Ayipe, F.I.; Tanko, M. Public Health Expenditure and Under-Five Mortality in Low-Income Sub-Saharan African Countries: A Panel Data Analysis. SSRN. 2023. Available online: https://Ssrn.Com/Abstract=4389168 (accessed on 29 April 2023).
- Shahid, A.S.M.S.B.; Rahman, A.E.; Shahunja, K.M.; Afroze, F.; Sarmin, M.; Nuzhat, S.; Alam, T.; Chowdhury, F.; Sultana, M.S.; Ackhter, M.M.; et al. Vaccination Following the Expanded Programme on Immunization Schedule Could Help to Reduce Deaths in Children under Five Hospitalized for Pneumonia and Severe Pneumonia in a Developing Country. Front. Pediatr. 2023, 11, 1–6. [Google Scholar] [CrossRef]
- Budu, E.; Ahinkorah, B.O.; Guets, W.; Ameyaw, E.K.; Essuman, M.A.; Yaya, S. Socioeconomic and Residence-based Related Inequality in Childhood Vaccination in Sub-Saharan Africa: Evidence from Benin. Health Sci. Rep. 2023, 6, e1198. [Google Scholar] [CrossRef]
- Santoli, J.M.; Lindley, M.C.; DeSilva, M.B.; Kharbanda, E.O.; Daley, M.F.; Galloway, L.; Gee, J.; Glover, M.; Herring, B.; Kang, Y.; et al. Effects of the COVID-19 Pandemic on Routine Pediatric Vaccine Ordering and Administration—United States, 2020. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 591–593. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Y.; Clapham, H.E.; Aishworiya, R.; Chua, Y.X.; Mathews, J.; Ong, M.; Wang, J.; Murugasu, B.; Chiang, W.C.; Lee, B.W.; et al. Childhood Vaccinations: Hidden Impact of COVID-19 on Children in Singapore. Vaccine 2021, 39, 780–785. [Google Scholar] [CrossRef] [PubMed]
- Tolera, S.T.; Kaweti, G.; Aboma, L.M. Article Review on Potential Impact of COVID-19 Pandemic on Socioeconomic of Ethiopia, Africa. Health Sci. 2022, 11, 19–30. [Google Scholar]
- He, K.; Mack, W.J.; Neely, M.; Lewis, L.; Anand, V. Parental Perspectives on Immunizations: Impact of the COVID-19 Pandemic on Childhood Vaccine Hesitancy. J. Community Health 2022, 47, 39–52. [Google Scholar] [CrossRef] [PubMed]
- McDonald, H.I.; Tessier, E.; White, J.M.; Woodruff, M.; Knowles, C.; Bates, C.; Parry, J.; Walker, J.L.; Scott, J.A.; Smeeth, L.; et al. Impact of the Coronavirus Disease (COVID-19) Pandemic and Physical Distancing Measures on Routine Childhood Vaccinations in England, January to April 2020. Euro Surveill. 2020, 25, 2000848. [Google Scholar] [CrossRef]
- Lassi, Z.S.; Naseem, R.; Salam, R.A.; Siddiqui, F.; Das, J.K. The Impact of the COVID-19 Pandemic on Immunization Campaigns and Programs: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 988. [Google Scholar] [CrossRef]
- Alsuhaibani, M.; Alaqeel, A. Impact of the COVID-19 Pandemic on Routine Childhood Immunization in Saudi Arabia. Vaccines 2020, 8, 581. [Google Scholar] [CrossRef]
- Palo, S.K.; Dubey, S.; Negi, S.; Sahay, M.R.; Patel, K.; Swain, S.; Mishra, B.K.; Bhuyan, D.; Kanungo, S.; Som, M.; et al. Effective Interventions to Ensure MCH (Maternal and Child Health) Services during Pandemic Related Health Emergencies (Zika, Ebola, and COVID-19): A Systematic Review. PLoS ONE 2022, 17, e0268106. [Google Scholar] [CrossRef]
- Kiely, M.; Mansour, T.; Brousseau, N.; Rafferty, E.; Paudel, Y.R.; Sadarangani, M.; Svenson, L.W.; Robinson, J.L.; Gagneur, A.; Driedger, S.M.; et al. COVID-19 Pandemic Impact on Childhood Vaccination Coverage in Quebec, Canada. Hum. Vaccin. Immunother. 2022, 18, e2007707. [Google Scholar] [CrossRef]
- Verrier, F.; de Lauzanne, A.; Diouf, J.-B.N.; Zo, A.Z.; Ramblière, L.; Herindrainy, P.; Sarr, F.D.; Sok, T.; Vray, M.; Collard, J.-M.; et al. Vaccination Coverage and Risk Factors Associated With Incomplete Vaccination Among Children in Cambodia, Madagascar, and Senegal. Open Forum Infect. Dis. 2023, 10, ofad136. [Google Scholar] [CrossRef]
- Alexander, C.; Cabrera, M.; Moore, M.; Lomazzi, M. Driving Paediatric Vaccine Recovery in Europe. Vaccines 2023, 11, 184. [Google Scholar] [CrossRef] [PubMed]
- Causey, K.; Fullman, N.; Sorensen, R.J.D.; Galles, N.C.; Zheng, P.; Aravkin, A.; Danovaro-Holliday, M.C.; Martinez-Piedra, R.; Sodha, S.V.; Velandia-González, M.P.; et al. Estimating Global and Regional Disruptions to Routine Childhood Vaccine Coverage during the COVID-19 Pandemic in 2020: A Modelling Study. Lancet 2021, 398, 522–534. [Google Scholar] [CrossRef] [PubMed]
- Wiysonge, C.S.; Uthman, O.A.; Ndumbe, P.M.; Hussey, G.D. Individual and Contextual Factors Associated with Low Childhood Immunisation Coverage in Sub-Saharan Africa: A Multilevel Analysis. PLoS ONE 2012, 7, e37905. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Usman, H.R.; Kristensen, S.; Rahbar, M.H.; Vermund, S.H.; Habib, F.; Chamot, E. Determinants of Third Dose of Diphtheria-Tetanus-Pertussis (DTP) Completion among Children Who Received DTP1 at Rural Immunization Centres in Pakistan: A Cohort Study. Trop. Med. Int. Health 2010, 15, 140–147. [Google Scholar] [CrossRef] [Green Version]
- WHO. Global Routine Immunization Strategies and Practices (GRISP) A Companion Document to the Global Vaccine Action Plan (GVAP); WHO: Geneva, Swtizerland, 2016; Available online: https://apps.who.int/iris/handle/10665/204500 (accessed on 29 April 2023).
- WHO. Immunization Coverage. Available online: https://www.who.int/news-room/fact-sheets/detail/immunization-coverage (accessed on 29 April 2023).
- Clark, A.; Sanderson, C. Timing of Children’s Vaccinations in 45 Low-Income and Middle-Income Countries: An Analysis of Survey Data. Lancet 2009, 373, 1543–1549. [Google Scholar] [CrossRef]
- Gebeyehu, N.A.; Asmare Adela, G.; Dagnaw Tegegne, K.; Birhan Assfaw, B. Vaccination Dropout among Children in Sub-Saharan Africa: Systematic Review and Meta-Analysis. Hum. Vaccin. Immunother. 2022, 18, e2145821. [Google Scholar] [CrossRef]
- Cutts, F.T.; Izurieta, H.S.; Rhoda, D.A. Measuring Coverage in MNCH: Design, Implementation, and Interpretation Challenges Associated with Tracking Vaccination Coverage Using Household Surveys. PLoS Med. 2013, 10, e1001404. [Google Scholar] [CrossRef] [Green Version]
- UNICEF. COVID-19 Pandemic Fuels Largest Continued Backslide in Vaccinations in Three Decades. Available online: https://www.unicef.org/press-releases/WUENIC2022release (accessed on 29 April 2023).
- Rachlin, A.; Danovaro-Holliday, M.C.; Murphy, P.; Sodha, S.V.; Wallace, A.S. Routine Vaccination Coverage—Worldwide, 2021. MMWR. Morb. Mortal. Wkly. Rep. 2022, 71, 1396–1400. [Google Scholar] [CrossRef]
- Munyangaju, I.; López-Varela, E.; Bassat, Q. Closing the Gap in Childhood Immunisation after the Pandemic. BMJ 2023, 380, 627. [Google Scholar] [CrossRef]
- Data Warehouse—UNICEF DATA. Available online: https://data.unicef.org/resources/data_explorer/unicef_f/?ag=UNICEF&df=IMMUNISATION&ver=1.0&dq=.IM_DTP3..&startPeriod=2000&endPeriod=2022 (accessed on 18 April 2023).
- World Bank. Population, Total. Data. Available online: https://data.worldbank.org/indicator/SP.POP.TOTL (accessed on 29 April 2023).
- Onambele, L.; Ortega-Leon, W.; Guillen-Aguinaga, S.; Forjaz, M.J.; Yoseph, A.; Guillen-Aguinaga, L.; Alas-Brun, R.; Arnedo-Pena, A.; Aguinaga-Ontoso, I.; Guillen-Grima, F. Maternal Mortality in Africa: Regional Trends (2000–2017). Int. J. Environ. Res. Public Health 2022, 19, 13146. [Google Scholar] [CrossRef]
- White, K.J. The Durbin-Watson Test for Autocorrelation in Nonlinear Models. Rev. Econ. Stat. 1992, 74, 370. [Google Scholar] [CrossRef]
- Imai, C.; Armstrong, B.; Chalabi, Z.; Mangtani, P.; Hashizume, M. Time Series Regression Model for Infectious Disease and Weather. Environ. Res. 2015, 142, 319–327. [Google Scholar] [CrossRef] [Green Version]
- UNICEF. Number of Births. Data Warehouse—UNICEF DATA. Available online: https://data.unicef.org/resources/data_explorer/unicef_f/?ag=UNICEF&df=GLOBAL_DATAFLOW&ver=1.0&dq=.DM_BRTS..&startPeriod=2019&endPeriod=2021 (accessed on 29 April 2023).
- Joinpoint Regression Program; version 4.3.1.0; Statistical Methodology and Applications Branch, Surveillance Research Program; National Cancer Institute: Bethesda, MD, USA, 2016.
- Kim, H.J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation Tests for Joinpoint Regression with Applications to Cancer Rates. Stat. Med. 2000, 19, 335–351. [Google Scholar] [CrossRef]
- Muhoza, P.; Danovaro-Holliday, M.C.; Diallo, M.S.; Murphy, P.; Sodha, S.V.; Requejo, J.H.; Wallace, A.S. Routine Vaccination Coverage—Worldwide, 2020. MMWR. Morb. Mortal. Wkly. Rep. 2021, 70, 1495–1500. [Google Scholar] [CrossRef]
- Watts, E.; Mak, J.; Patenaude, B. Benefit–Cost Ratios of Continuing Routine Immunization During the COVID-19 Pandemic in Africa. J. Benefit-Cost Anal. 2022, 13, 91–106. [Google Scholar] [CrossRef]
- Ministry of Health and Population Egypt; El-Zanaty and Associates Egypt; ICF International. Egypt Demographic and Health Survey 2014; Ministry of Health and Population Egypt: Cairo, Egypt; ICF International: Rockville, MD, USA, 2015.
- El-Zanaty, F.; Way, A. Egypt Demographic and Health Survey 2008; Ministry of Health, El-Zanaty and Associates, and Macro International: Cairo, Egypt, 2009.
- Atnafu Gebeyehu, N.; Abebe Gelaw, K.; Asmare Adella, G.; Dagnaw Tegegne, K.; Adie Admass, B.; Mesele Gesese, M. Incomplete Immunization and Its Determinants among Children in Africa: Systematic Review and Meta-Analysis. Hum. Vaccines Immunother. 2023, 2202125. [Google Scholar] [CrossRef] [PubMed]
- Périères, L.; Séror, V.; Boyer, S.; Sokhna, C.; Peretti-Watel, P. Reasons given for Non-Vaccination and under-Vaccination of Children and Adolescents in Sub-Saharan Africa: A Systematic Review. Hum. Vaccines Immunother. 2022, 18, e2076524. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira Roque e Lima, J.; Pagotto, V.; Rocha, B.S.; Scalize, P.S.; Guimarães, R.A.; de Lima, M.D.; da Silva, L.N.; da Silva Oliveira, M.D.; Moura, W.É.A.; Teles, S.A.; et al. Low Vaccine Coverage and Factors Associated with Incomplete Childhood Immunization in Racial/Ethnic Minorities and Rural Groups, Central Brazil. Vaccines 2023, 11, 838. [Google Scholar] [CrossRef] [PubMed]
- Tan, N.C.; Pang, J.; Koh, E. The Impact of a Revised National Childhood Immunization Schedule on Vaccination Defaulters. Vaccines 2023, 11, 859. [Google Scholar] [CrossRef]
- Saidu, Y.; Di Mattei, P.; Nchinjoh, S.C.; Edwige, N.N.; Nsah, B.; Muteh, N.J.; Ndoula, S.T.; Abdullahi, R.; Zamir, C.S.; Njoh, A.A.; et al. The Hidden Impact of the COVID-19 Pandemic on Routine Childhood Immunization Coverage in Cameroon. Vaccines 2023, 11, 645. [Google Scholar] [CrossRef]
- Sambala, E.Z.; Uthman, O.A.; Adamu, A.A.; Ndwandwe, D.; Wiyeh, A.B.; Olukade, T.; Bishwajit, G.; Yaya, S.; Okwo-Bele, J.-M.; Wiysonge, C.S. Mind the Gap: What Explains the Education-Related Inequality in Missed Opportunities for Vaccination in Sub-Saharan Africa? Compositional and Structural Characteristics. Hum. Vaccines Immunother. 2018, 14, 2365–2372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biset, G.; Woday, A.; Mihret, S.; Tsihay, M. Full Immunization Coverage and Associated Factors among Children Age 12–23 Months in Ethiopia: Systematic Review and Meta-Analysis of Observational Studies. Hum. Vaccines Immunother. 2021, 17, 2326–2335. [Google Scholar] [CrossRef] [PubMed]
- Kamadjeu, R.; Mulugeta, A.; Gupta, D.; Abshir Hirsi, A.; Belayneh, A.; Clark-Hattingh, M.; Adams, C.; Abed, P.; Kyeyune, B.; Ahmed, T.; et al. Immunizing Nomadic Children and Livestock—Experience in North East Zone of Somalia. Hum. Vaccines Immunother. 2015, 11, 2637–2639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saxena, K.; Marden, J.R.; Carias, C.; Bhatti, A.; Patterson-Lomba, O.; Gomez-Lievano, A.; Yao, L.; Chen, Y.-T. Impact of the COVID-19 Pandemic on Adolescent Vaccinations: Projected Time to Reverse Deficits in Routine Adolescent Vaccination in the United States. Curr. Med. Res. Opin. 2021, 37, 2077–2087. [Google Scholar] [CrossRef]
- Patel Murthy, B.; Zell, E.; Kirtland, K.; Jones-Jack, N.; Harris, L.; Sprague, C.; Schultz, J.; Le, Q.; Bramer, C.A.; Kuramoto, S.; et al. Impact of the COVID-19 Pandemic on Administration of Selected Routine Childhood and Adolescent Vaccinations—10 US Jurisdictions, March–September 2020. MMWR. Morb. Mortal. Wkly. Rep. 2021, 70, 840–845. [Google Scholar] [CrossRef] [PubMed]
- Diedrich, D.; Northcote, N.; Röder, T.; Sauer-Sidor, K. Strategic Resilience during the COVID-19 Crisis. Available online: https://www.mckinsey.com/capabilities/strategy-and-corporate-finance/our-insights/strategic-resilience-during-the-COVID-19-crisis (accessed on 29 April 2023).
- WHO and UNICEF Warn of a Decline in Vaccinations during COVID-19. Available online: https://www.who.int/news/item/15–07−2020-who-and-unicef-warn-of-a-decline-in-vaccinations-during-COVID-19 (accessed on 29 April 2023).
- Moraga-Llop, F.A.; Fernández-Prada, M.; Grande-Tejada, A.M.; Martínez-Alcorta, L.I.; Moreno-Pérez, D.; Pérez-Martín, J.J. Recovering Vaccine Coverage Lost Due to the COVID-19 Pandemic. Vacunas 2020, 21, 129–135. [Google Scholar] [CrossRef]
- WHO. Scale-Up Routine Immunization along with COVID-19 Vaccination: WHO. Available online: https://www.who.int/southeastasia/news/detail/08–09−2021-scale-up-routine-immunization-along-with-COVID-19-vaccination-who (accessed on 29 April 2023).
- African Union. The signing of a New Agreement to Drive Vaccine Impact in Africa. Available online: https://africacdc.org/news-item/the-signing-of-a-new-agreement-to-drive-vaccine-impact-in-africa/ (accessed on 29 April 2023).




















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
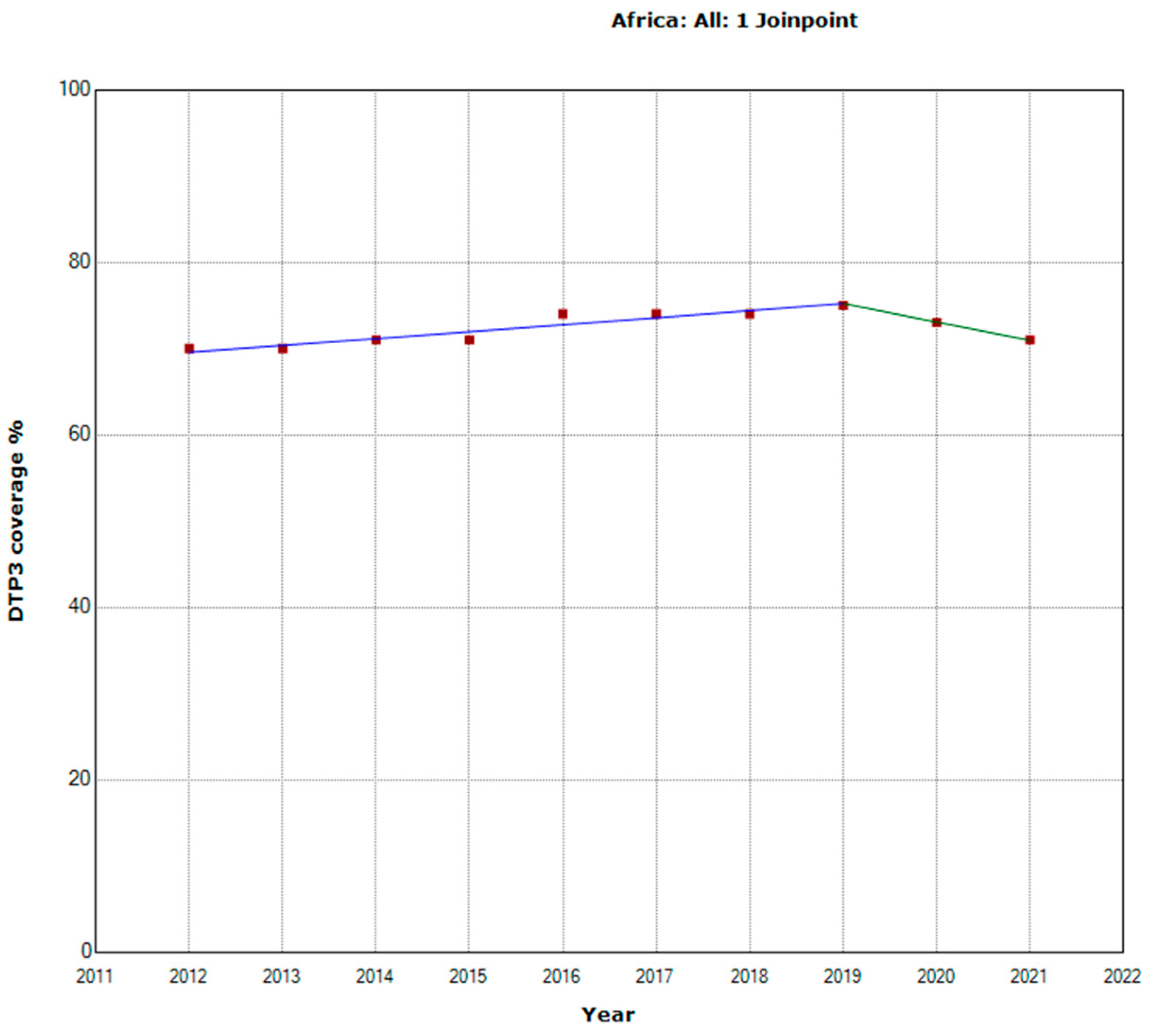
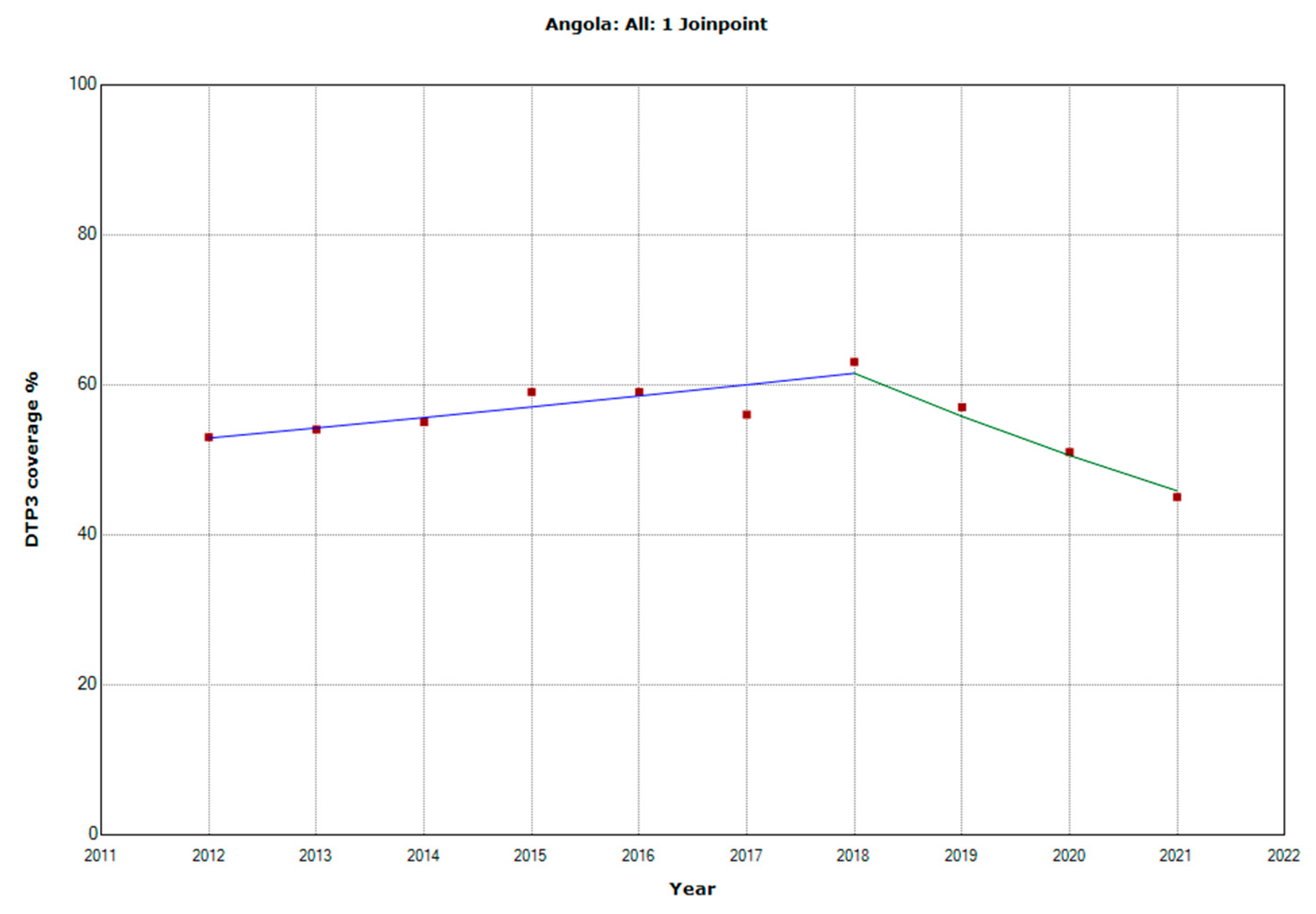
| Periods | Years | APC (95% CI) | p |
|---|---|---|---|
| Total Period | 2012–2021 | 0.5 (0; 1.1) | 0.052 |
| Period 1 | 2012–2019 | 1.1 (0.7; 1.6) | 0.001 |
| Period 2 | 2019–2021 | −2.9 (−6.9; 1.3) | 0.134 |
| Periods | Years | APC (95% CI) | p |
|---|---|---|---|
| North | |||
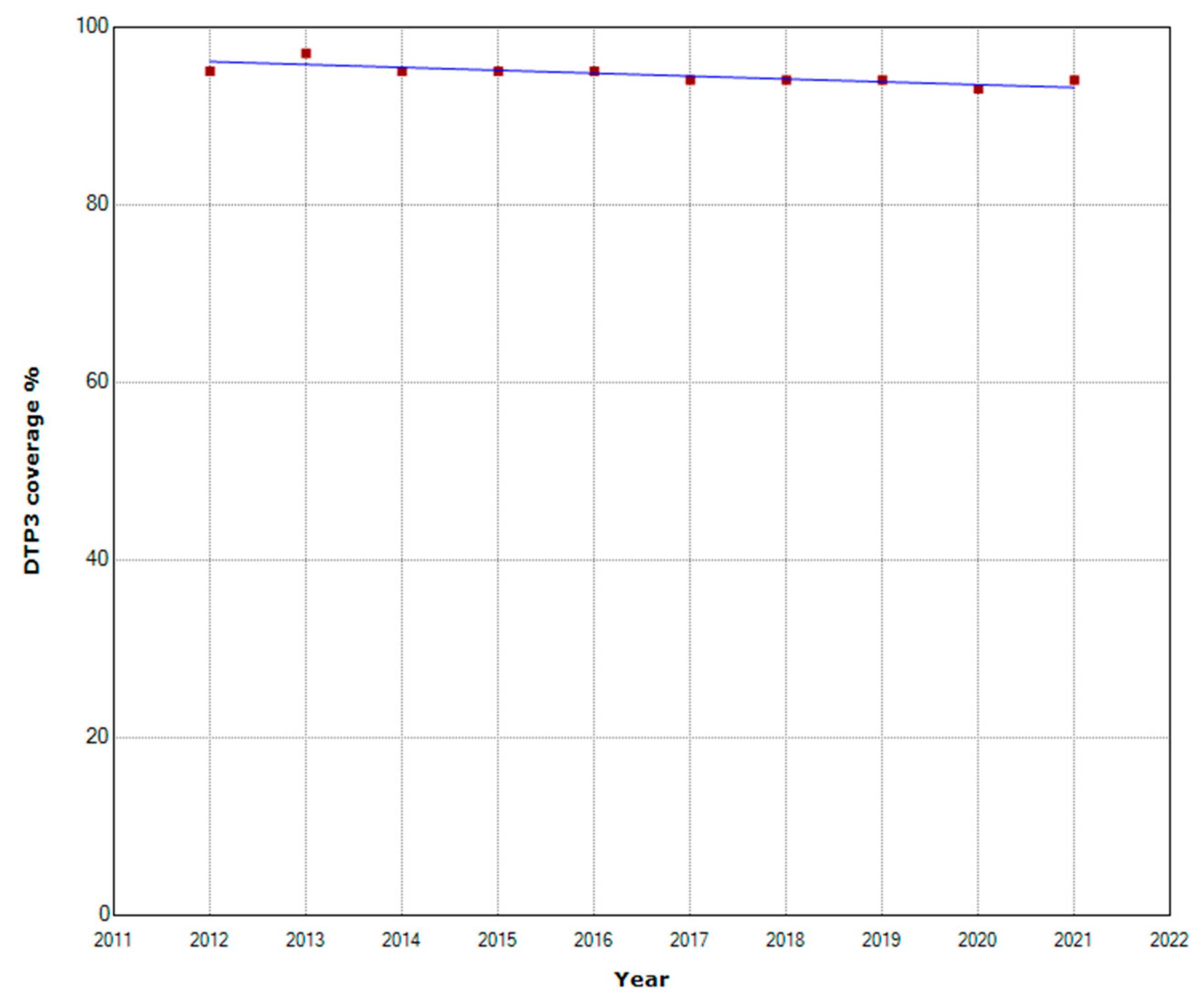
| Total Period | 2012–2021 | −0.3 (−0.4; −0.2) | 0.001 |
| Sub-Saharan Africa | |||
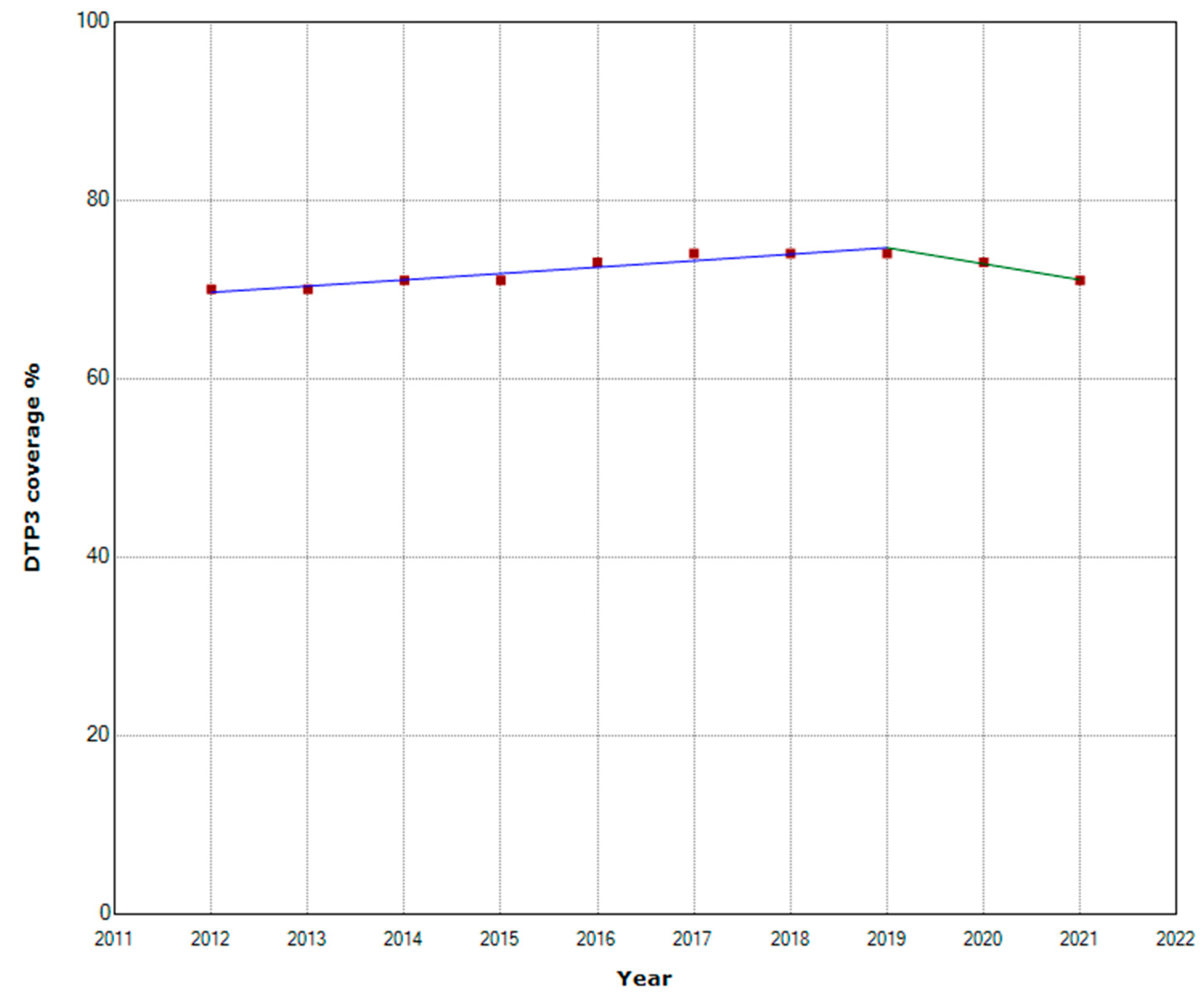
| Total Period | 2012–2021 | 0.5 (0; 1.0) | 0.053 |
| Period 1 | 2012–2019 | 1.0 (0.6; 1.4) | 0.001 |
| Period 2 | 2020–2021 | −2.4 (−5.2; 1.4) | 0.078 |
| West and Central Africa | |||
| Total Period | 2012–2021 | 1.1 (0.5; 1.8) | 0.004 |
| East and South Africa | |||
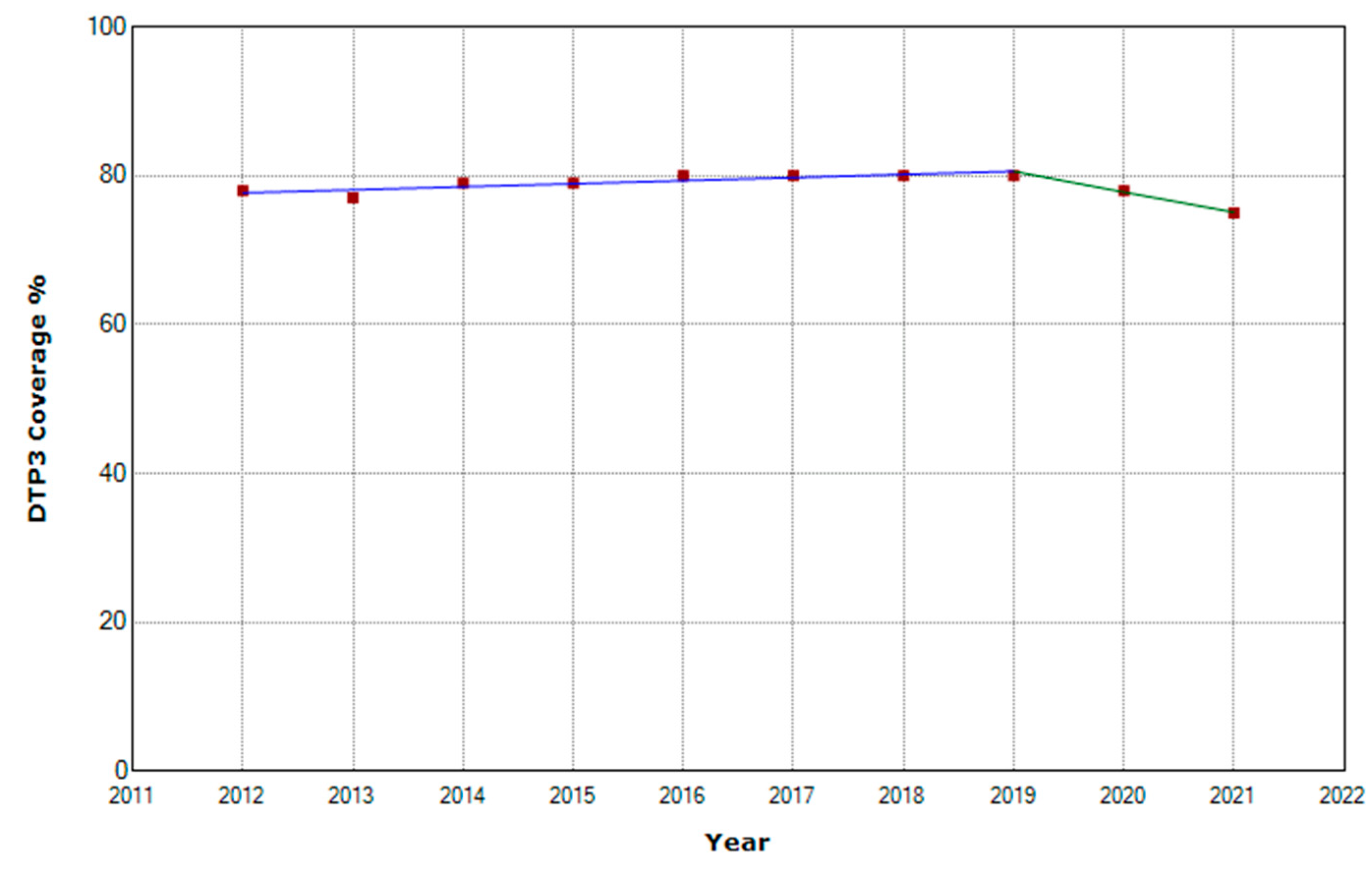
| Total Period | 2012–2021 | −0.6 (0; 0.5) | 0.835 |
| Period 1 | 2012–2019 | 0.5 (0.2; 0.8) | 0.006 |
| Period 2 | 2020–2021 | −3.5 (−6.3; −0.5) | 0.029 |
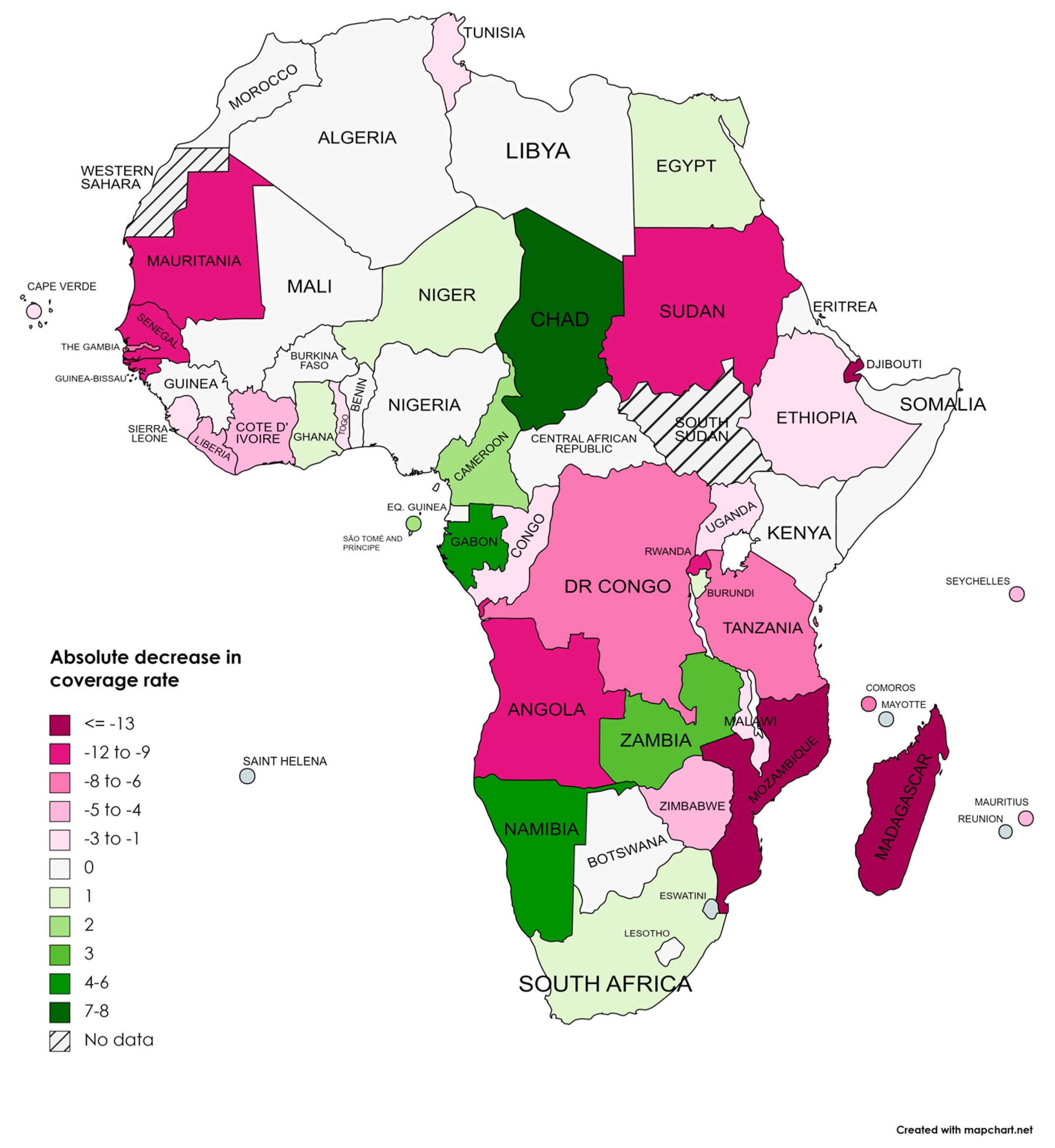
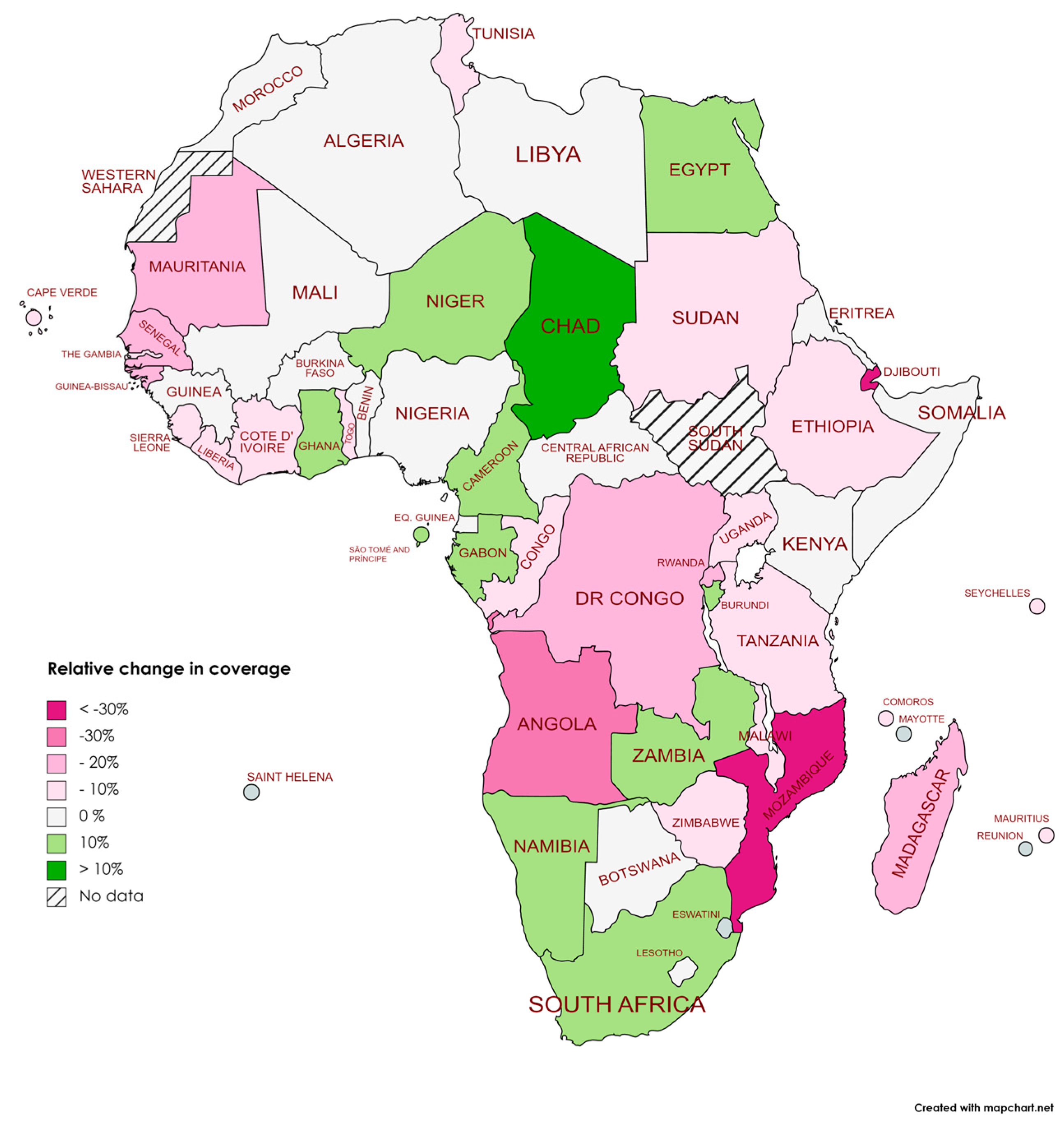
| Region | 2019 | 2021 | Absolute Changes | Relative Changes |
|---|---|---|---|---|
| Africa | 75 | 71 | −4 | −5.33% |
| West and Central Africa | 69 | 67 | −2 | −2.90% |
| Eastern and Southern Africa | 80 | 75 | −5 | −6.25% |
| Sub-Saharan Africa | 74 | 71 | −3 | −4.05% |
| North Africa | 94 | 94 | 0 | 0.00% |
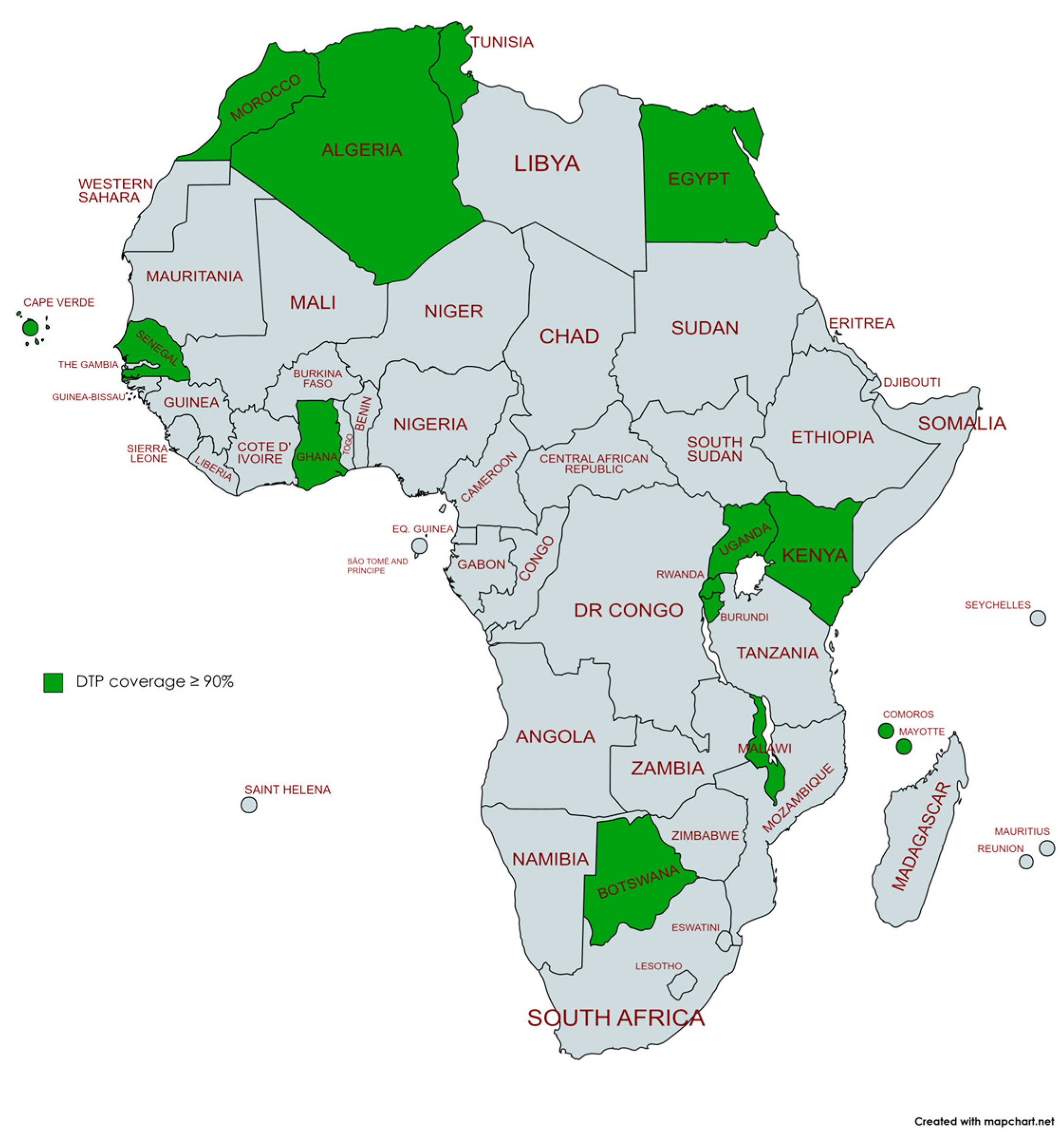
| Country | 2019 | 2021 | Absolute Changes | Relative Changes | p * |
|---|---|---|---|---|---|
| Algeria | 91 | 91 | 0 | 0.0% | ns |
| Angola | 57 | 45 | −12 | −21.1% | <0.001 |
| Benin | 76 | 76 | 0 | 0.0% | ns |
| Botswana | 95 | 95 | 0 | 0.0% | ns |
| Burkina Faso | 91 | 91 | 0 | 0.0% | ns |
| Burundi | 93 | 94 | 1 | 1.1% | ns |
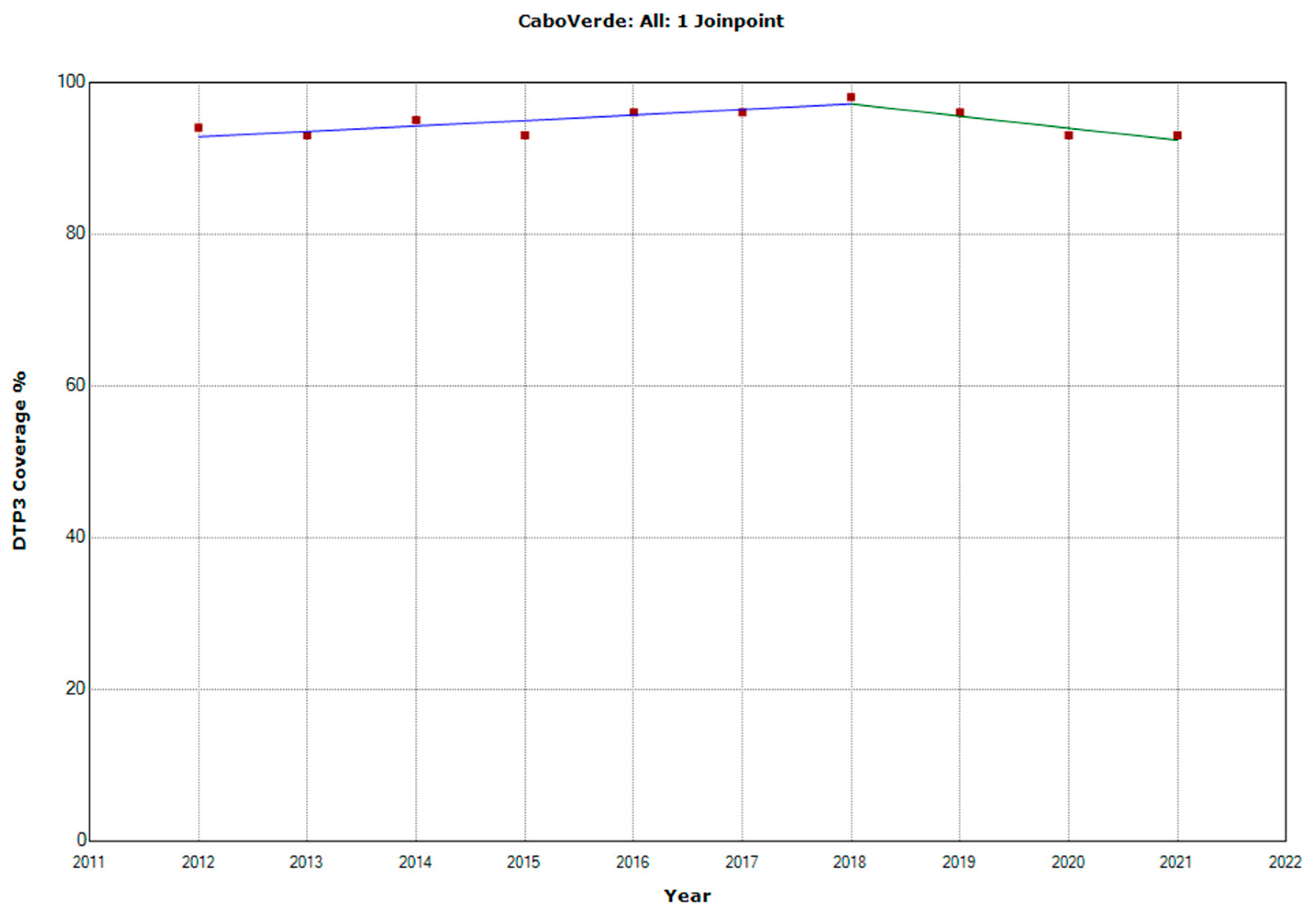
| Cabo Verde | 96 | 93 | −3 | −3.1% | <0.001 |
| Cameroon | 67 | 69 | 2 | 3.0% | <0.001 |
| Central African Republic | 42 | 42 | 0 | 0.0% | ns |
| Chad | 50 | 58 | 8 | 16.0% | <0.001 |
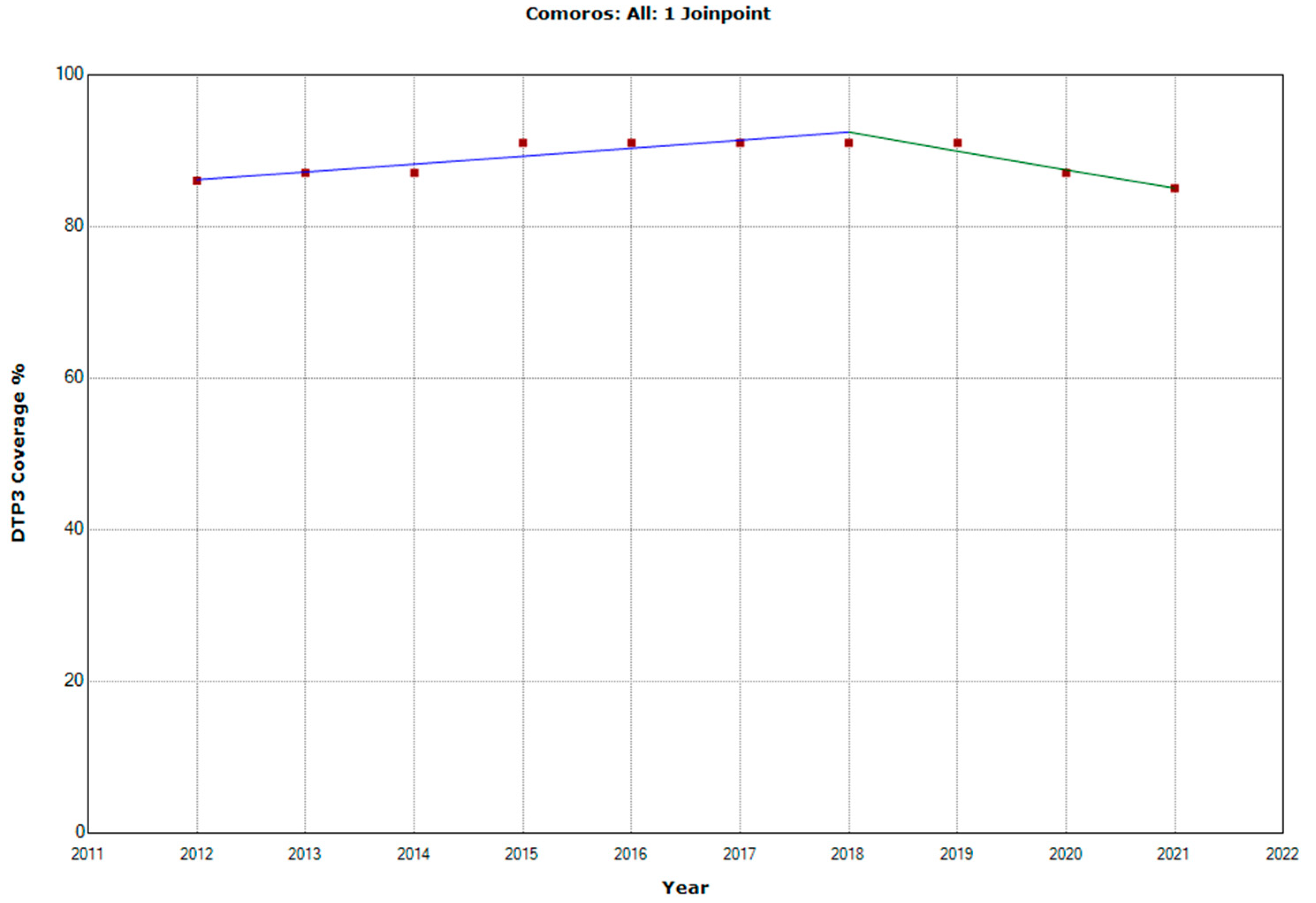
| Comoros | 91 | 85 | −6 | −6.6% | <0.001 |
| Congo | 79 | 77 | −2 | −2.5% | <0.001 |
| Côte d’Ivoire | 81 | 76 | −5 | −6.2% | <0.001 |
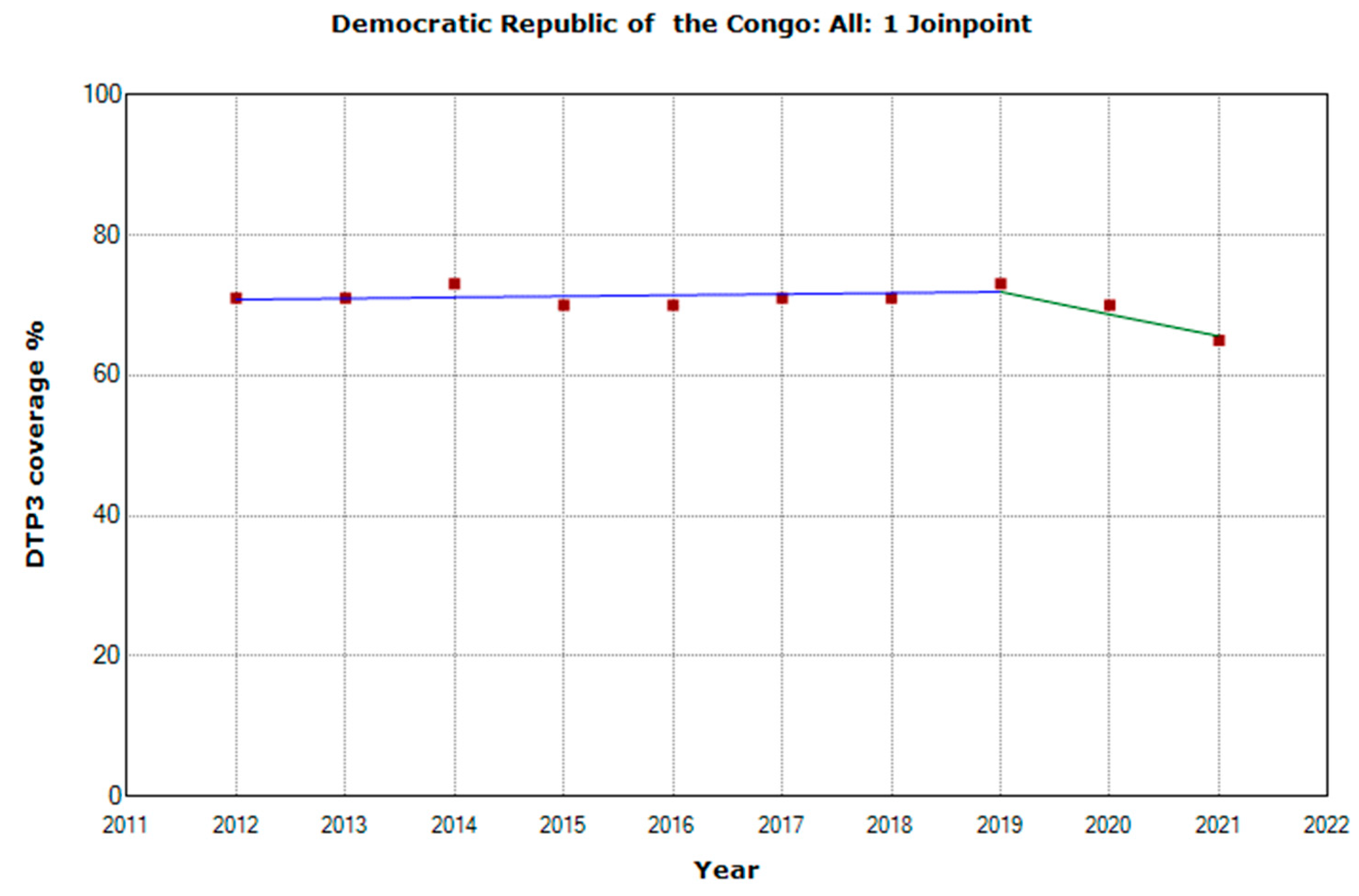
| Democratic Republic of the Congo | 73 | 65 | −8 | −11.0% | <0.001 |
| Djibouti | 85 | 59 | −26 | −30.6% | <0.001 |
| Egypt | 95 | 96 | 1 | 1.1% | <0.001 |
| Equatorial Guinea | 53 | 53 | 0 | 0.0% | ns |
| Eritrea | 95 | 95 | 0 | 0.0% | ns |
| Ethiopia | 68 | 65 | −3 | −4.4% | <0.001 |
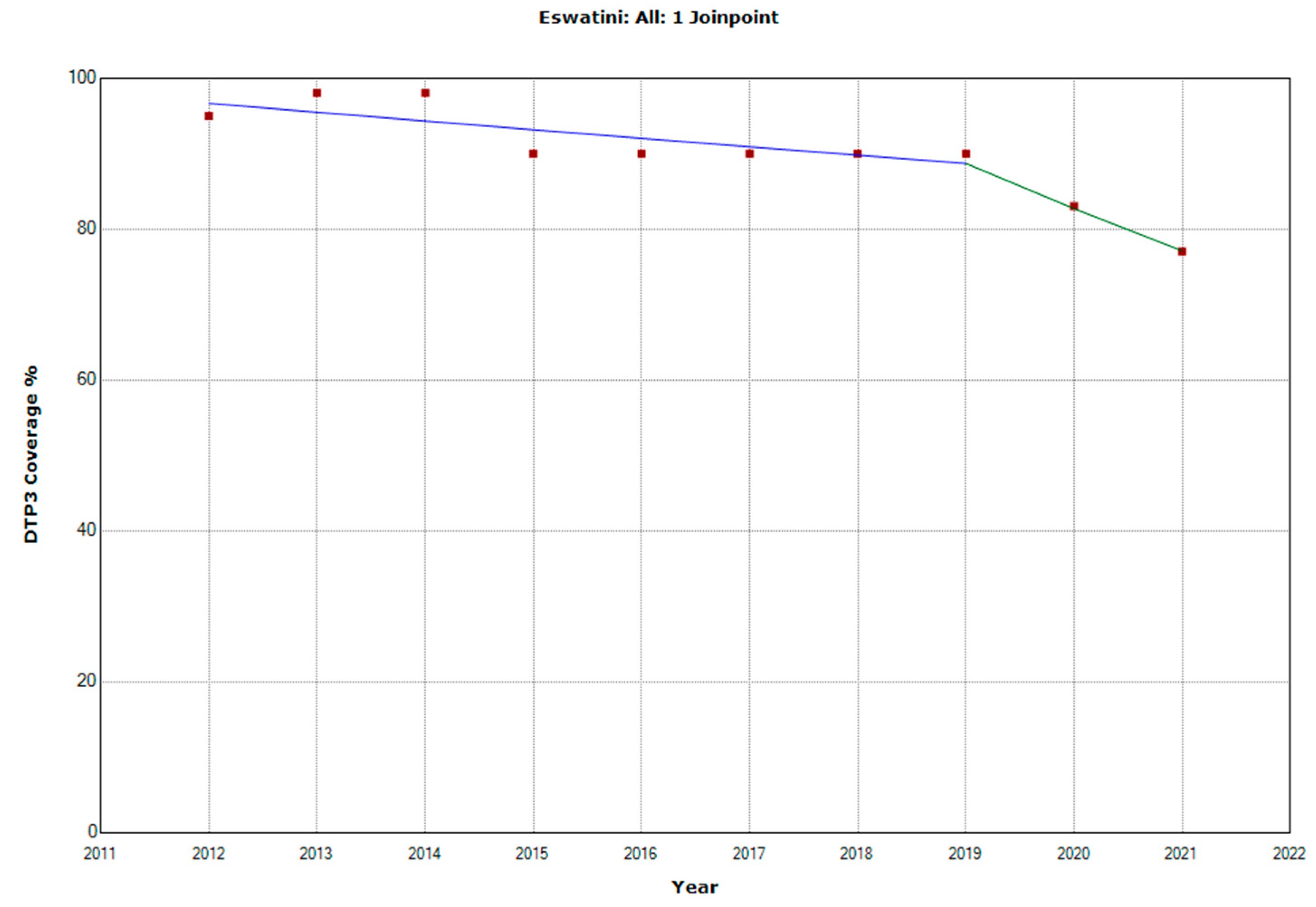
| Eswatini | 90 | 77 | −13 | −14.4% | <0.001 |
| Gabon | 70 | 75 | 5 | 7.1% | <0.001 |
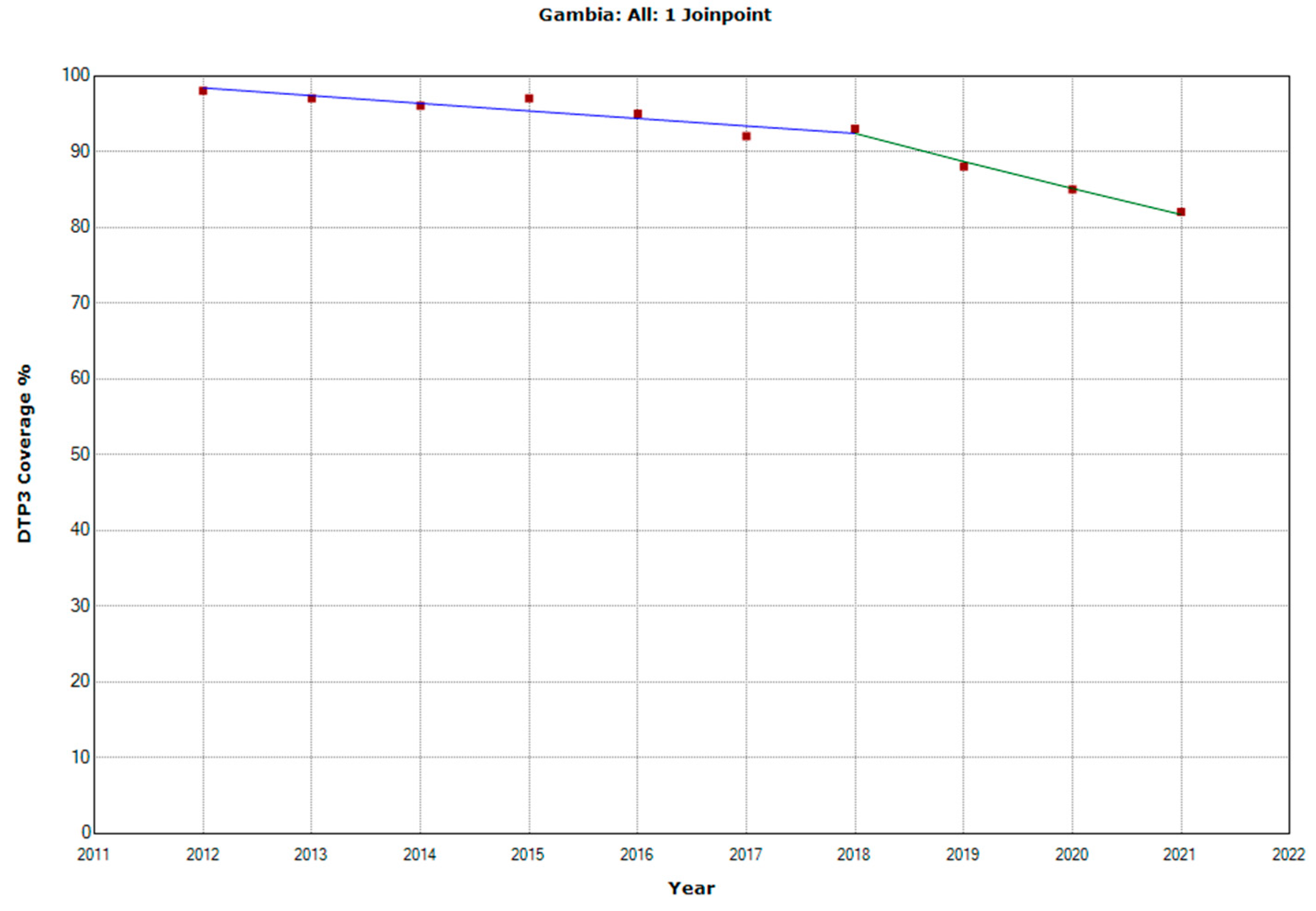
| The Gambia | 88 | 82 | −6 | −6.8% | <0.001 |
| Ghana | 97 | 98 | 1 | 1.0% | <0.001 |
| Guinea | 47 | 47 | 0 | 0,0% | ns |
| Guinea-Bissau | 78 | 67 | −11 | −14,1% | <0.001 |
| Kenya | 91 | 91 | 0 | 0.0% | ns |
| Lesotho | 87 | 87 | 0 | 0.0% | ns |
| Liberia | 70 | 66 | −4 | −5.7% | <0.001 |
| Libya | 73 | 73 | 0 | 0.0% | ns |
| Madagascar | 68 | 55 | −13 | −19.1 | <0.001 |
| Malawi | 95 | 93 | −2 | −2.1% | <0.001 |
| Mali | 77 | 77 | 0 | 0.0% | ns |
| Mauritania | 80 | 68 | −12 | −15.0% | <0.001 |
| Mauritius | 96 | 92 | −4 | −4.2% | <0.001 |
| Morocco | 99 | 99 | 0 | 0.0% | ns |
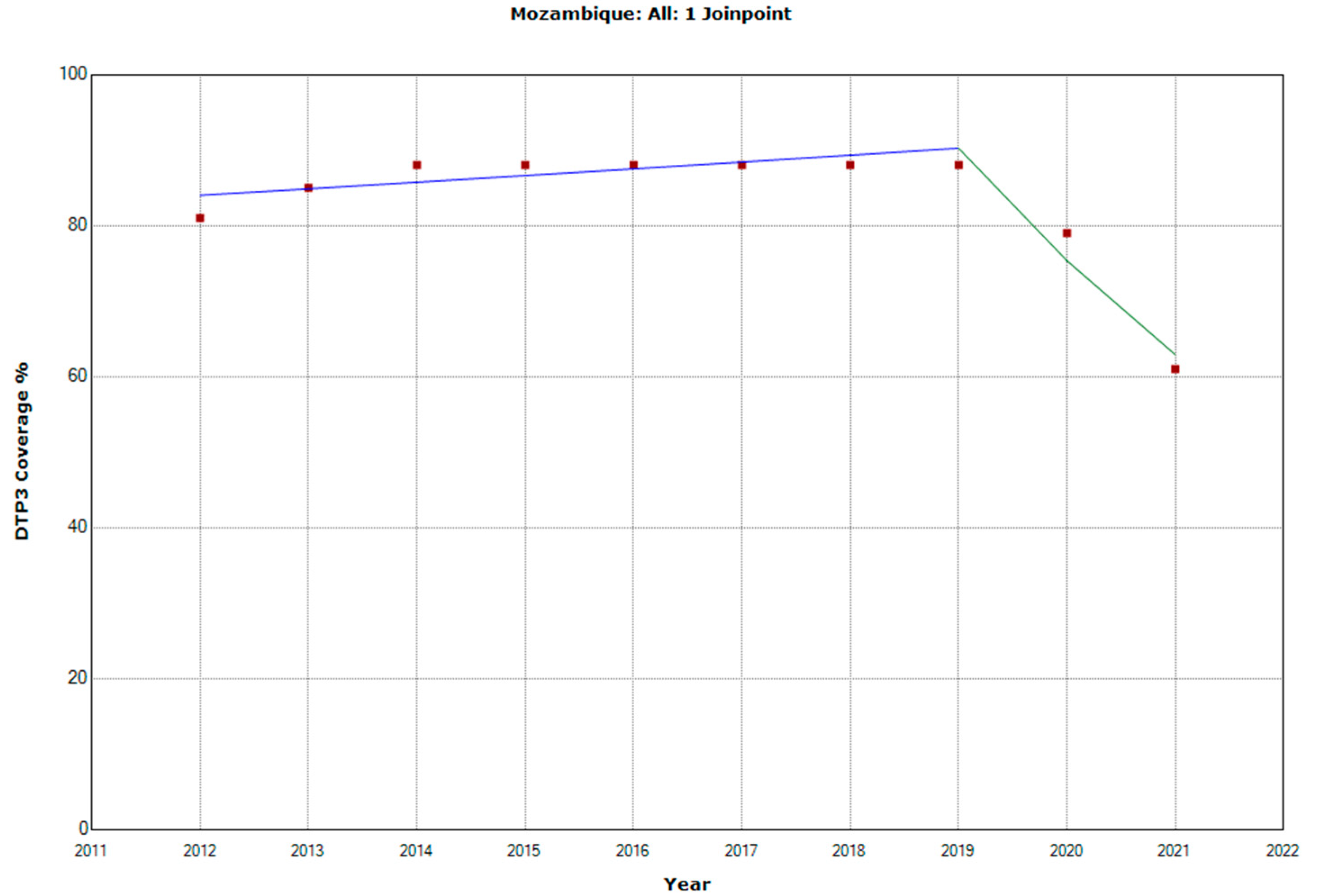
| Mozambique | 88 | 61 | −27 | −30.7% | <0.001 |
| Namibia | 87 | 93 | 6 | 6.9% | <0.001 |
| Niger | 81 | 82 | 1 | 1.2% | <0.001 |
| Nigeria | 56 | 56 | 0 | 0.0% | ns |
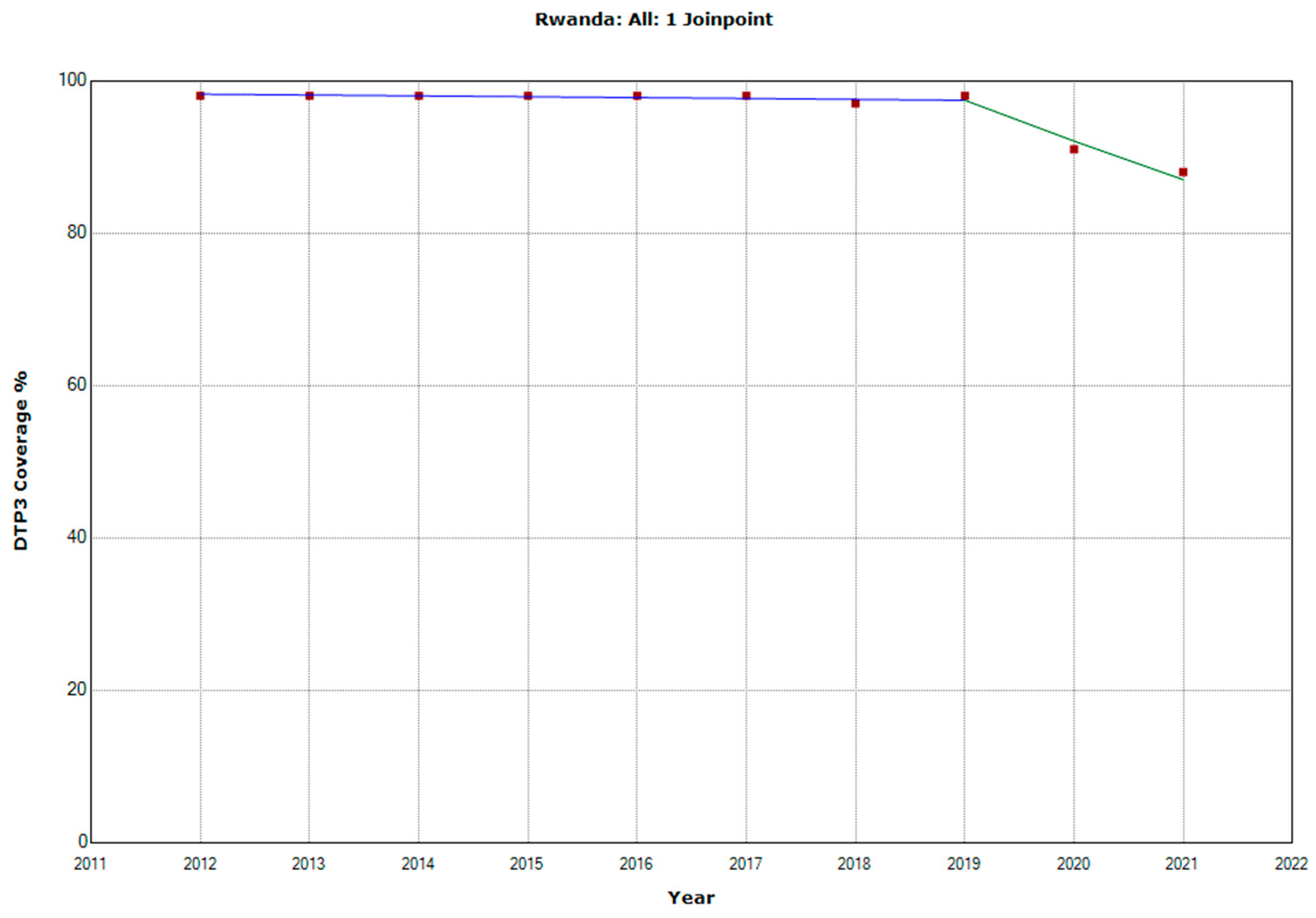
| Rwanda | 98 | 88 | −10 | −10.2% | <0.001 |
| Sao Tome and Principe | 95 | 97 | 2 | 2.1% | <0.001 |
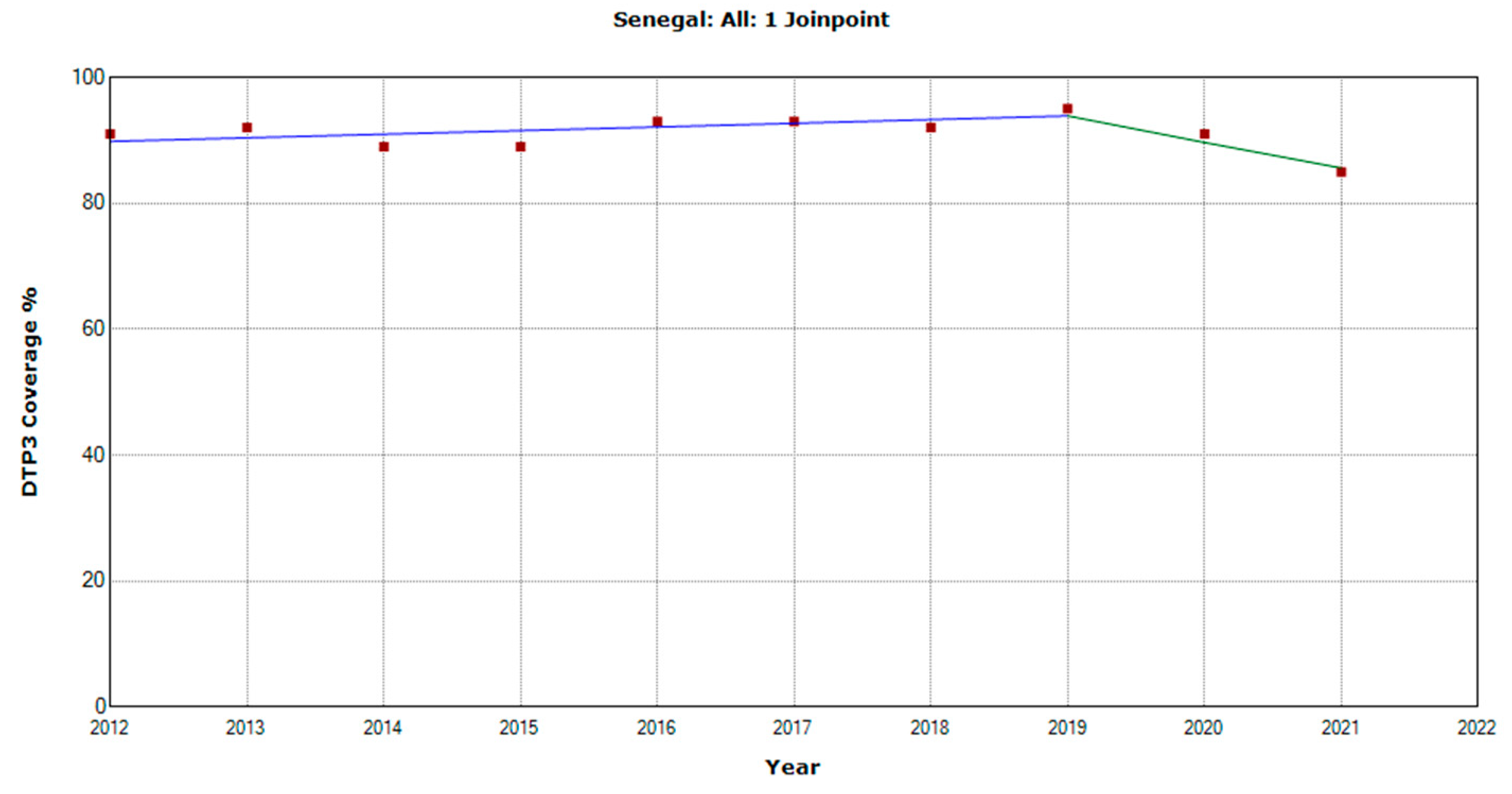
| Senegal | 95 | 85 | −10 | −10.5% | <0.001 |
| Seychelles | 99 | 94 | −5 | −5.1% | <0.001 |
| Sierra Leone | 95 | 92 | −3 | −3.2% | <0.001 |
| Somalia | 42 | 42 | 0 | 0.0% | ns |
| South Africa | 85 | 86 | 1 | 1.2% | <0.001 |
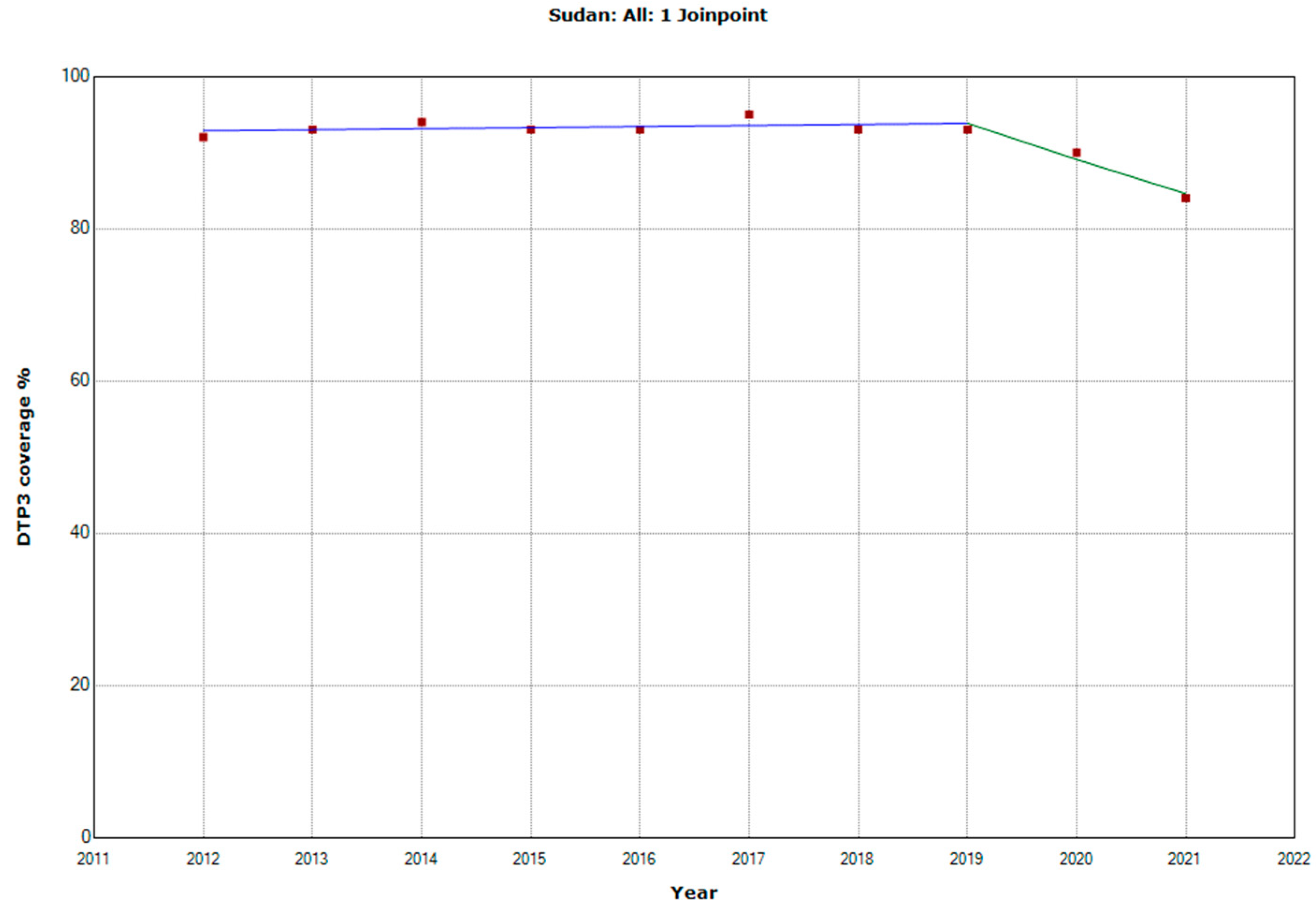
| Sudan | 93 | 84 | −9 | −9.7% | <0.001 |
| Tanzania | 89 | 81 | −8 | −1.2% | <0.001 |
| Togo | 84 | 83 | −1 | −3.4% | <0.001 |
| Tunisia | 98 | 97 | −1 | −1.0% | <0.001 |
| Uganda | 93 | 91 | −2 | −2.2% | <0.001 |
| Zambia | 88 | 91 | 3 | 9.0% | <0.001 |
| Zimbabwe | 90 | 86 | −4 | 0.0% | <0.001 |
| Country | Years | APC (95% CI) | p |
|---|---|---|---|
| Angola | |||
| Period 1 | 2012–2018 | 2.6 (1.3; 4.1) | 0.013 |
| Period 2 | 2018–2021 | −9.3 (−14.4; −6.1) | 0.007 |
| Cabo Verde | |||
| Period 1 | 2012–2018 | 0.8 (0.3; 1.2) | 0.006 |
| Period 2 | 2018–2021 | −1.7 (−3.2; −0.1) | 0.040 |
| Comoros | |||
| Period 1 | 2012–2018 | 1.2 (0.6; 1.8) | 0.004 |
| Period 2 | 2018–2021 | −2.7 (−4.6; −0.8) | 0.014 |
| Democratic Republic of the Congo | |||
| Period 1 | 2012–2019 | 0.2 (−0.5; 1.0) | 0.489 |
| Period 2 | 2019–2021 | −4.5 (−9.5; 0.8) | 0.079 |
| Eswatini | |||
| Period 1 | 2012–2019 | −1.2 (−2.6; 0.2) | 0.078 |
| Period 2 | 2019–2021 | −6.8 (−15.7; 3.1) | 0.134 |
| The Gambia | |||
| Period 1 | 2012–2018 | −1.0 (−1.6; −0.4) | 0.007 |
| Period 2 | 2018–2021 | −4.0 (−5.9; −2.1) | 0.003 |
| Mozambique | |||
| Period 1 | 2012–2019 | 1.0 (0.0; 2.0) | 0.047 |
| Period 2 | 2019–2021 | −16.5 (−24.4; −7.8) | 0.006 |
| Rwanda | |||
| Period 1 | 2012–2019 | −0.1 (−0.2; 0.0) | 0.063 |
| Period 2 | 2019–2021 | −5.5 (−7.4; −3.6) | 0.001 |
| Senegal | |||
| Period 1 | 2012–2019 | 0.6 (−0.3; 1.6) | 0.141 |
| Period 2 | 2019–2021 | −4.5 (−10.7; 2.1) | 0.138 |
| Sudan | |||
| Period 1 | 2012–2019 | 0.1 (−0.2; 0.5) | 0.294 |
| Period 2 | 2019–2021 | −5.1 (−8.6; −1.4) | 0.017 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aguinaga-Ontoso, I.; Guillen-Aguinaga, S.; Guillen-Aguinaga, L.; Alas-Brun, R.; Onambele, L.; Aguinaga-Ontoso, E.; Guillen-Grima, F. COVID-19 Impact on DTP Vaccination Trends in Africa: A Joinpoint Regression Analysis. Vaccines 2023, 11, 1103. https://doi.org/10.3390/vaccines11061103
Aguinaga-Ontoso I, Guillen-Aguinaga S, Guillen-Aguinaga L, Alas-Brun R, Onambele L, Aguinaga-Ontoso E, Guillen-Grima F. COVID-19 Impact on DTP Vaccination Trends in Africa: A Joinpoint Regression Analysis. Vaccines. 2023; 11(6):1103. https://doi.org/10.3390/vaccines11061103
Chicago/Turabian StyleAguinaga-Ontoso, Ines, Sara Guillen-Aguinaga, Laura Guillen-Aguinaga, Rosa Alas-Brun, Luc Onambele, Enrique Aguinaga-Ontoso, and Francisco Guillen-Grima. 2023. "COVID-19 Impact on DTP Vaccination Trends in Africa: A Joinpoint Regression Analysis" Vaccines 11, no. 6: 1103. https://doi.org/10.3390/vaccines11061103