

Investigating the Marginal and Herd Effects of COVID-19 Vaccination for Reducing Case Fatality Rate: Evidence from the United States between March 2021 to January 2022

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.2. Models
3. Results
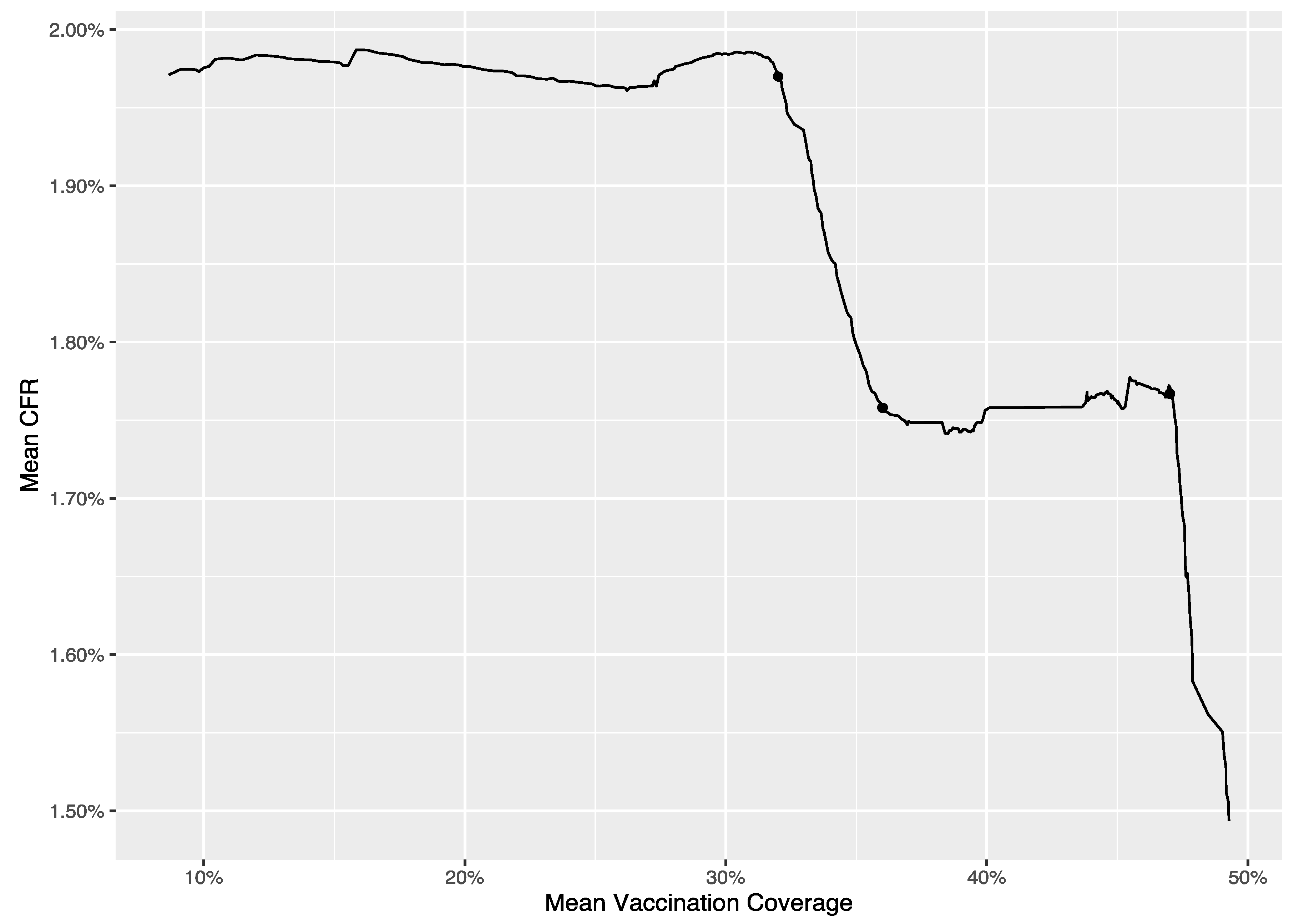
3.1. The Results of the Analysis at National Level
3.2. The Results of the Analysis at County Level
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Capalbo, C.; Aceti, A.; Simmaco, M.; Bonfini, R.; Rocco, M.; Ricci, A.; Napoli, C.; Rocco, M.; Alfonsi, V.; Teggi, A.; et al. The exponential phase of the COVID-19 pandemic in central Italy: An Integrated Care Pathway. Int. J. Environ. Res. Public Health 2020, 17, 3792. [Google Scholar] [CrossRef] [PubMed]
- Dal-Ré, R.; Bekker, L.G.; Gluud, C.; Holm, S.; Jha, V.; A Poland, G.; Rosendaal, F.R.; Schwarzer-Daum, B.; Sevene, E.; Tinto, H.; et al. Ongoing and future COVID-19 vaccine clinical trials: Challenges and opportunities. Lancet Infect. Dis. 2021, 21, e342–e347. [Google Scholar] [CrossRef] [PubMed]
- Yan, Z.P.; Yang, M.; Lai, C.L. COVID-19 vaccines: A review of the safety and efficacy of current clinical trials. Pharmaceuticals 2021, 14, 406. [Google Scholar] [CrossRef]
- Ahmed, S.; Khan, S.; Imran, I.; Al Mughairbi, F.; Sheikh, F.S.; Hussain, J.; Khan, A.; Al-Harrasi, A. Vaccine development against COVID-19: Study from pre-clinical phases to clinical trials and global use. Vaccines 2021, 9, 836. [Google Scholar] [CrossRef]
- World Health Organization. Global COVID-19 Vaccination Strategy in a Changing World. 2022. Available online: https://www.who.int/publications/m/item/global-covid-19-vaccination-strategy-in-a-changing-world--july-2022-update (accessed on 24 November 2022).
- Mathieu, E.; Ritchie, H.; Ortiz-Ospina, E.; Roser, M.; Hasell, J.; Appel, C.; Giattino, C.; Rodés-Guirao, L. A global database of COVID-19 vaccinations. Nat. Hum. Behav. 2021, 5, 947–953. [Google Scholar] [CrossRef]
- Hodge, J.G. Nationalizing public health emergency legal responses. J. Law Med. Ethics 2021, 49, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Freedman, L.; Kalkstein, N.; Mizrahi, B.; Alroy-Preis, S.; Ash, N.; Milo, R.; et al. Protection of BNT162b2 vaccine booster against COVID-19 in Israel. N. Engl. J. Med. 2021, 385, 1393–1400. [Google Scholar] [CrossRef]
- Mahase, E. COVID-19 booster vaccines: What we know and who’s doing what. BMJ 2021, 374, n2082. [Google Scholar] [CrossRef]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Sachdeva, R.; Gower, C.; Ramsay, M.; Bernal, J.L. Effectiveness of COVID-19 booster vaccines against COVID-19-related symptoms, hospitalization and death in England. Nat. Med. 2022, 28, 831–837. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. COVID Data Tracker. 2022. Available online: https://covid.cdc.gov/covid-data-tracker (accessed on 24 November 2022).
- Zhao, S.; Lou, J.; Cao, L.; Chong, K.C.; Zee, B.C.; Chan, P.K.; Wang, M.H. Differences in the case fatality risks associated with SARS-CoV-2 Delta and non-Delta variants in relation to vaccine coverage: An early ecological study in the United Kingdom. Infect. Genet. Evol. 2022, 97, 105162. [Google Scholar] [CrossRef]
- Lee, Y.C.; Chang, K.Y.; Mirsaeidi, M. Association of COVID-19 case-fatality rate with state health disparity in the United States. Front. Med. 2022, 9, 853059. [Google Scholar] [CrossRef]
- Lipsitch, M.; Dean, N.E. Understanding COVID-19 vaccine efficacy. Science 2020, 370, 763–765. [Google Scholar] [CrossRef] [PubMed]
- Halloran, M.E.; Haber, M.; Longini, I.M., Jr.; Struchiner, C.J. Direct and indirect effects in vaccine efficacy and effectiveness. Am. J. Epidemiol. 1991, 133, 323–331. [Google Scholar] [CrossRef]
- Morens, D.M.; Folkers, G.K.; Fauci, A.S. The concept of classical herd immunity may not apply to COVID-19. J. Infect. Dis. 2022, 226, 195–198. [Google Scholar] [CrossRef]
- Randolph, H.E.; Barreiro, L.B. Herd immunity: Understanding COVID-19. Immunity 2020, 52, 737–741. [Google Scholar] [CrossRef]
- Plans-Rubió, P. Percentages of vaccination coverage required to establish herd immunity against SARS-CoV-2. Vaccines 2022, 10, 736. [Google Scholar] [CrossRef]
- Gallagher, M.E.; Sieben, A.J.; Nelson, K.N.; Kraay, A.N.M.; Orenstein, W.A.; Lopman, B.; Handel, A.; Koelle, K. Indirect benefits are a crucial consideration when evaluating SARS-CoV-2 vaccine candidates. Nat. Med. 2021, 27, 4–5. [Google Scholar] [CrossRef] [PubMed]
- Flanagan, B.E.; Hallisey, E.J.; Adams, E.; Lavery, A. Measuring community vulnerability to natural and anthropogenic hazards: The centers for disease control and prevention’s social vulnerability index. J. Environ. Health 2018, 80, 34–36. [Google Scholar] [PubMed]
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef] [PubMed]
- Center for Systems Science and Engineering. COVID-19 Data Repository by the Center for Systems Science and Engineering at Johns Hopkins University. 2022. Available online: https://github.com/CSSEGISandData/COVID-19 (accessed on 24 November 2022).
- Place and Health, Agency for Toxic Substances and Disease Registry. CDC SVI 2018 Data and Documentation. 2020. Available online: https://www.atsdr.cdc.gov/placeandhealth/svi/data_documentation_download.html (accessed on 7 June 2022).
- Muggeo, V.M.R. Estimating regression models with unknown breakpoints. Stat. Med. 2003, 22, 3055–3071. [Google Scholar] [CrossRef]
- Muggeo, V.M.R. Segmented: An R package to fit regression models with broken-line relationships. R News 2008, 8, 20–25. [Google Scholar]
- Moghadas, S.M.; Sah, P.; Fitzpatrick, M.C.; Shoukat, A.; Pandey, A.; Vilches, T.N.; Singer, B.H.; Schneider, E.C.; Galvani, A.P. COVID-19 deaths and hospitalizations averted by rapid vaccination rollout in the United States. medRxiv 2021. [Google Scholar] [CrossRef]
- Shoukat, A.; Vilches, T.N.; Moghadas, S.M.; Sah, P.; Schneider, E.C.; Shaff, J.; Ternier, A.; Chokshi, D.A.; Galvani, A.P. Lives saved and hospitalizations averted by COVID-19 vaccination in New York City: A modeling study. Lancet Reg. Health Am. 2022, 5, 100085. [Google Scholar] [CrossRef] [PubMed]
- Vilches, T.N.; Sah, P.; Moghadas, S.M.; Shoukat, A.; Fitzpatrick, M.C.; Hotez, P.J.; Schneider, E.C.; Galvani, A.P. COVID-19 hospitalizations and deaths averted under an accelerated vaccination program in northeastern and southern regions of the USA. Lancet Reg. Health Am. 2022, 6, 100147. [Google Scholar] [CrossRef]
- McKee, M.; Rajan, S. What can we learn from Israel’s rapid roll out of COVID 19 vaccination? Isr. J. Health Policy Res. 2021, 10, 5. [Google Scholar] [CrossRef] [PubMed]
- Sah, P.; Vilches, T.N.; Moghadas, S.M.; Fitzpatrick, M.C.; Singer, B.H.; Hotez, P.J.; Galvani, A.P. Accelerated vaccine rollout is imperative to mitigate highly transmissible COVID-19 variants. eClinicalMedicine 2021, 35, 100865. [Google Scholar] [CrossRef] [PubMed]
- Aguilera, X.; Mundt, A.P.; Araos, R.; Weitzel, T. The story behind Chile’s rapid rollout of COVID-19 vaccination. Travel Med. Infect. Dis. 2021, 42, 102092. [Google Scholar] [CrossRef] [PubMed]
- Glied, S. Strategy drives implementation: COVID vaccination in Israel. Isr. J. Health Policy Res. 2021, 10, 9. [Google Scholar] [CrossRef]
- Vilches, T.N.; Moghadas, S.M.; Sah, P.; Fitzpatrick, M.C.; Shoukat, A.; Pandey, A.; Galvani, A.P. Estimating COVID-19 infections, hospitalizations, and deaths following the US vaccination campaigns during the pandemic. JAMA Netw. Open 2022, 5, e2142725. [Google Scholar] [CrossRef]
- Monge, S.; Olmedo, C.; Alejos, B.; Lapeña, M.F.; Sierra, M.J.; Limia, A. Direct and indirect effectiveness of mRNA vaccination against severe acute respiratory syndrome Coronavirus 2 in long-term care facilities, Spain. Emerg. Infect. Dis. 2021, 27, 2595–2603. [Google Scholar] [CrossRef] [PubMed]
- Clemente-Suárez, V.J.; Hormeño-Holgado, A.; Jiménez, M.; Benitez-Agudelo, J.C.; Navarro-Jiménez, E.; Perez-Palencia, N.; Maestre-Serrano, R.; Laborde-Cárdenas, C.C.; Tornero-Aguilera, J.F. Dynamics of population immunity due to the herd effect in the COVID-19 pandemic. Vaccines 2020, 8, 236. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.C.; Young, S.G.; Pro, G.C. COVID-19 vaccination rates vary by community vulnerability: A county-level analysis. Vaccine 2021, 39, 4245–4249. [Google Scholar] [CrossRef]
- Chen, Y.; Ma, Z.F.; Yu, D.; Jiang, Z.; Wang, B.; Yuan, L. Geographical distribution of trace elements (selenium, zinc, iron, copper) and case fatality rate of COVID-19: A national analysis across conterminous USA. Environ. Geochem. Health 2022, 44, 4423–4436. [Google Scholar] [CrossRef] [PubMed]
- Weisel, O. Vaccination as a social contract: The case of COVID-19 and US political partisanship. Proc. Natl. Acad. Sci. USA 2021, 118, e2026745118. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; White, L.F. Bayesian back-calculation and nowcasting for line list data during the COVID-19 pandemic. PLoS Comput. Biol. 2021, 17, e1009210. [Google Scholar] [CrossRef]
- Bergen, N.; Kirkby, K.; Fuertes, C.V.; Schlotheuber, A.; Menning, L.; Feely, S.; O’Brien, K.; Hosseinpoor, A.S. Global state of education-related inequality in COVID-19 vaccine coverage, structural barriers, vaccine hesitancy, and vaccine refusal: Findings from the Global COVID-19 Trends and Impact Survey. Lancet Glob. Health 2023, 11, e207–e217. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Zhang, L.; Li, T.; Li, L. Amplified effect of social vulnerability on health inequality regarding COVID-19 mortality in the USA: The mediating role of vaccination allocation. BMC Public Health 2022, 22, 2131. [Google Scholar] [CrossRef]
- Buscot, M.J.; Wotherspoon, S.S.; Magnussen, C.G.; Juonala, M.; Sabin, M.A.; Burgner, D.P.; Lehtimäki, T.; Viikari, J.S.A.; Hutri-Kähönen, N.; Raitakari, O.T.; et al. Bayesian hierarchical piecewise regression models: A tool to detect trajectory divergence between groups in long-term observational studies. BMC Med. Res. Methodol. 2017, 17, 86. [Google Scholar] [CrossRef] [Green Version]
- Basso, P.; Negro, C.; Cegolon, L.; Larese Filon, F. Risk of vaccine breakthrough SARS-CoV-2 infection and associated factors in healthcare workers of Trieste teaching hospitals (north-eastern Italy). Viruses 2022, 14, 336. [Google Scholar] [CrossRef]
- Cegolon, L.; Ronchese, F.; Ricci, F.; Negro, C.; Larese-Filon, F. SARS-CoV-2 infection in health care workers of Trieste (North-eastern Italy), 1 October 2020-7 February 2022: Occupational risk and the impact of the Omicron variant. Viruses 2022, 14, 1663. [Google Scholar] [CrossRef]
- Li, T. The Bayesian Paradigm of Robustness Indices of Causal Inferences; Michigan State University: East Lansing, MI, USA, 2018. [Google Scholar]
- Li, T.; Frank, K. The probability of a robust inference for internal validity. Sociol. Methods Res. 2022, 51, 1947–1968. [Google Scholar] [CrossRef]
- Li, T.; Frank, K.A. The probability of a robust inference for internal validity and its applications in regression models. arXiv 2020, arXiv:2005.12784. [Google Scholar]
- Li, T. On the probability of invalidating a causal inference due to limited external validity. arXiv 2022, arXiv:2206.08649. [Google Scholar]


{kind=link}
| Parameter | Estimate | T Ratio | p-Value |
|---|---|---|---|
| 1.976 | 624.70 | <0.001 | |
| 0.000 | 0.28 | 0.78 | |
| −0.003 | −0.90 | 0.37 | |
| −0.057 | −45.32 | <0.001 | |
| −0.236 | −80.67 | <0.001 | |
| 0.003 | 7.50 | <0.001 | |
| −0.227 | −55.09 | <0.001 | |
| −0.115 | −47.03 | <0.001 |
| Effect | Location | Estimate | p-Value |
|---|---|---|---|
| 1st marginal effect | 0.000 | 0.78 | |
| 1st herd effect | −0.003 | 0.37 | |
| 2nd marginal effect | −0.057 | <0.001 | |
| 2nd herd effect | −0.233 | <0.001 | |
| 3rd marginal effect | 0.003 | <0.001 | |
| 3rd herd effect | 0.009 | 0.02 | |
| 4th marginal effect | −0.115 | <0.001 |
| Parameter | F.E. Est | F.E. T Ratio | F.E. p-Value | VRE Est |
|---|---|---|---|---|
| 1.64 | 28.88 | <0.001 | 1.33 | |
| −0.004 | −8.85 | <0.001 | 0.0005 | |
| −0.025 | −7.35 | <0.001 | 0.024 | |
| −0.007 | −3.74 | <0.001 | 0.007 | |
| −0.018 | −2.84 | 0.005 | 0.091 | |
| −0.02 | −13.07 | <0.001 | 0.006 | |
| −0.004 | −0.35 | 0.728 | 0.2 | |
| −0.039 | −23.49 | <0.001 | 0.004 | |
| 0.0004 | 0.33 | 0.744 | n/a 1 | |
| 0.807 | 11.00 | <0.001 | n/a | |
| −0.057 | −0.73 | 0.467 | n/a | |
| 0.004 | 0.05 | 0.961 | n/a |
| Effect | Location | F.E. Est | F.E. p-Value | VRE Est |
|---|---|---|---|---|
| 1st marginal effect | −0.004 | <0.001 | 0.0005 | |
| 1st herd effect | −0.025 | <0.001 | 0.024 | |
| 2nd marginal effect | −0.01 | <0.001 | 0.008 | |
| 2nd herd effect | 0.008 | 0.70 | 0.115 | |
| 3rd marginal effect | −0.023 | <0.001 | 0.006 | |
| 3rd herd effect | 0.014 | 0.545 | 0.29 | |
| 4th marginal effect | −0.043 | <0.001 | 0.005 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, T.; Wang, Z.; He, S.; Chen, Y. Investigating the Marginal and Herd Effects of COVID-19 Vaccination for Reducing Case Fatality Rate: Evidence from the United States between March 2021 to January 2022. Vaccines 2023, 11, 1078. https://doi.org/10.3390/vaccines11061078
Li T, Wang Z, He S, Chen Y. Investigating the Marginal and Herd Effects of COVID-19 Vaccination for Reducing Case Fatality Rate: Evidence from the United States between March 2021 to January 2022. Vaccines. 2023; 11(6):1078. https://doi.org/10.3390/vaccines11061078
Chicago/Turabian StyleLi, Tenglong, Zilong Wang, Shuyue He, and Ying Chen. 2023. "Investigating the Marginal and Herd Effects of COVID-19 Vaccination for Reducing Case Fatality Rate: Evidence from the United States between March 2021 to January 2022" Vaccines 11, no. 6: 1078. https://doi.org/10.3390/vaccines11061078