

Assessing the Impact of Vaccination on the Dynamics of COVID-19 in Africa: A Mathematical Modeling Study

 , ,
, ,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
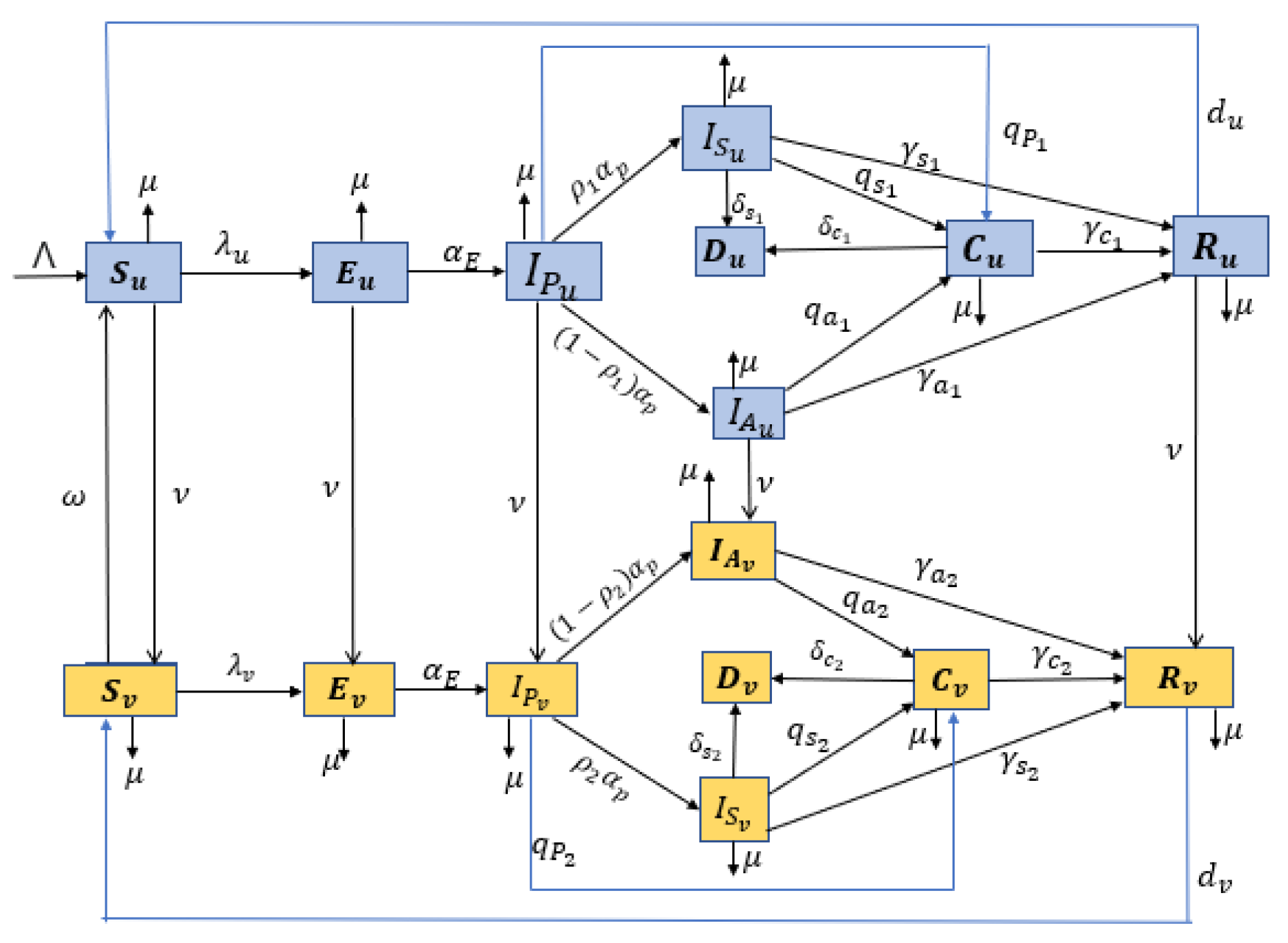
2.1. Model Formulation
- (i)
- Vaccination is administered to unvaccinated individuals that are susceptible, exposed, pre-symptomatic, asymptomatic, and naturally recovered from the virus. The model does not consider the vaccination of symptomatic and confirmed infectious individuals.
- (ii)
- The COVID-19 vaccine administered is imperfect, i.e., it provides only partial protection against COVID-19 infections. Thus, infections for the vaccinated can occur but at a reduced rate compared to that of the unvaccinated susceptible individuals.
- (iii)
- (iv)
- We assume that there is homogeneous mixing among the population, which means that every individual in the community is equally likely to mix and acquire infections from each member when they make contact.
- (v)
- Since the COVID-19 pandemic has persisted for a long time, we include the vital dynamics (birth and natural death) in the model.
2.2. Data
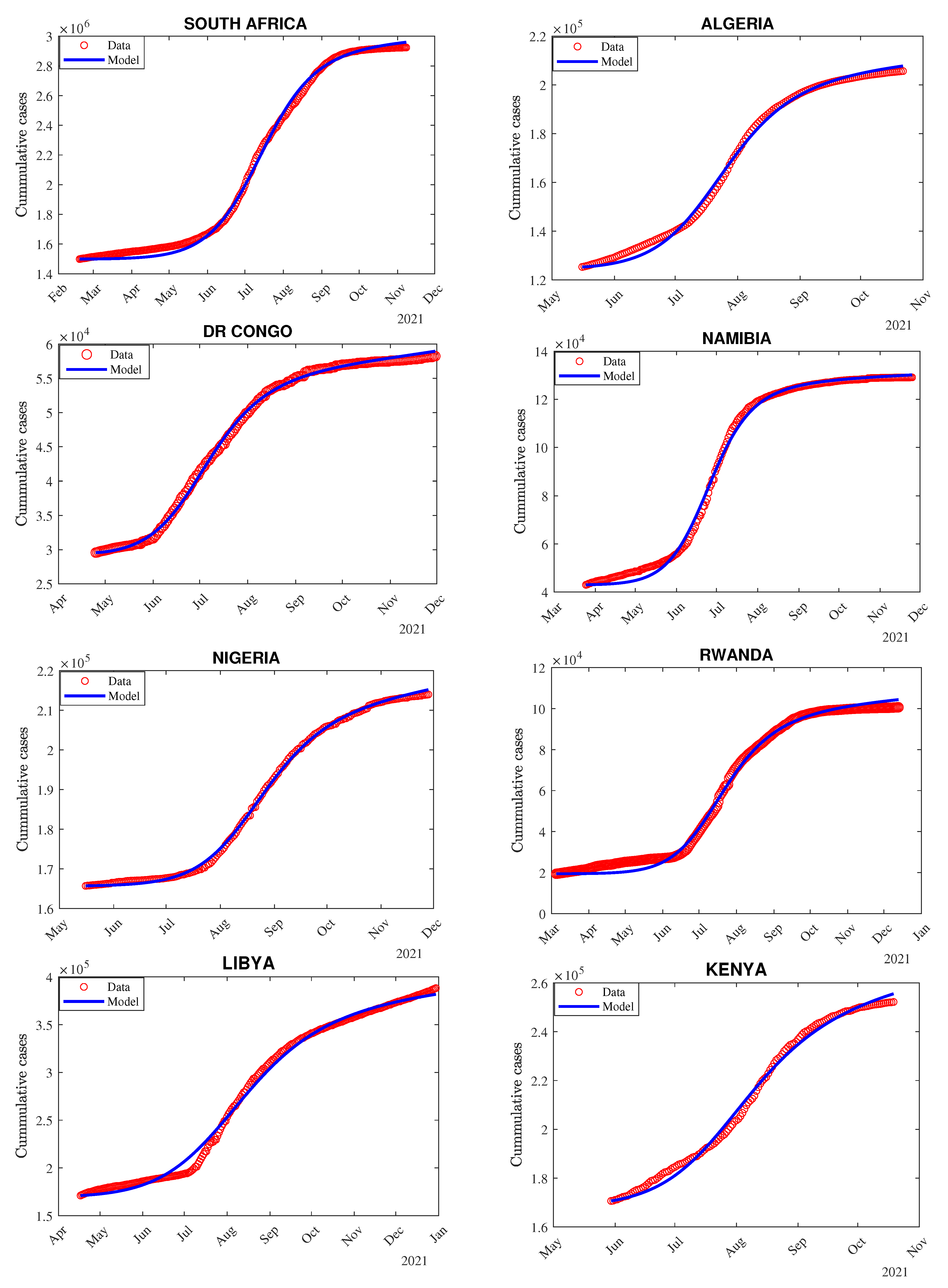
2.3. Model Fitting and Parameter Estimation Procedure
3. Results
3.1. Analytical Results
3.1.1. Computation of Control Reproduction Number
- Let be a column vector for all new infections and be the jacobian of at disease-free equilibrium,where
- Let be the matrix of net transitions
- The Jacobian matrix () of matrix V, at disease-free equilibrium, is given as:where
3.1.2. Computation of Basic Reproduction Number
3.2. Numerical Results
3.2.1. Dynamics of COVID-19 Infectious Classes Over Time
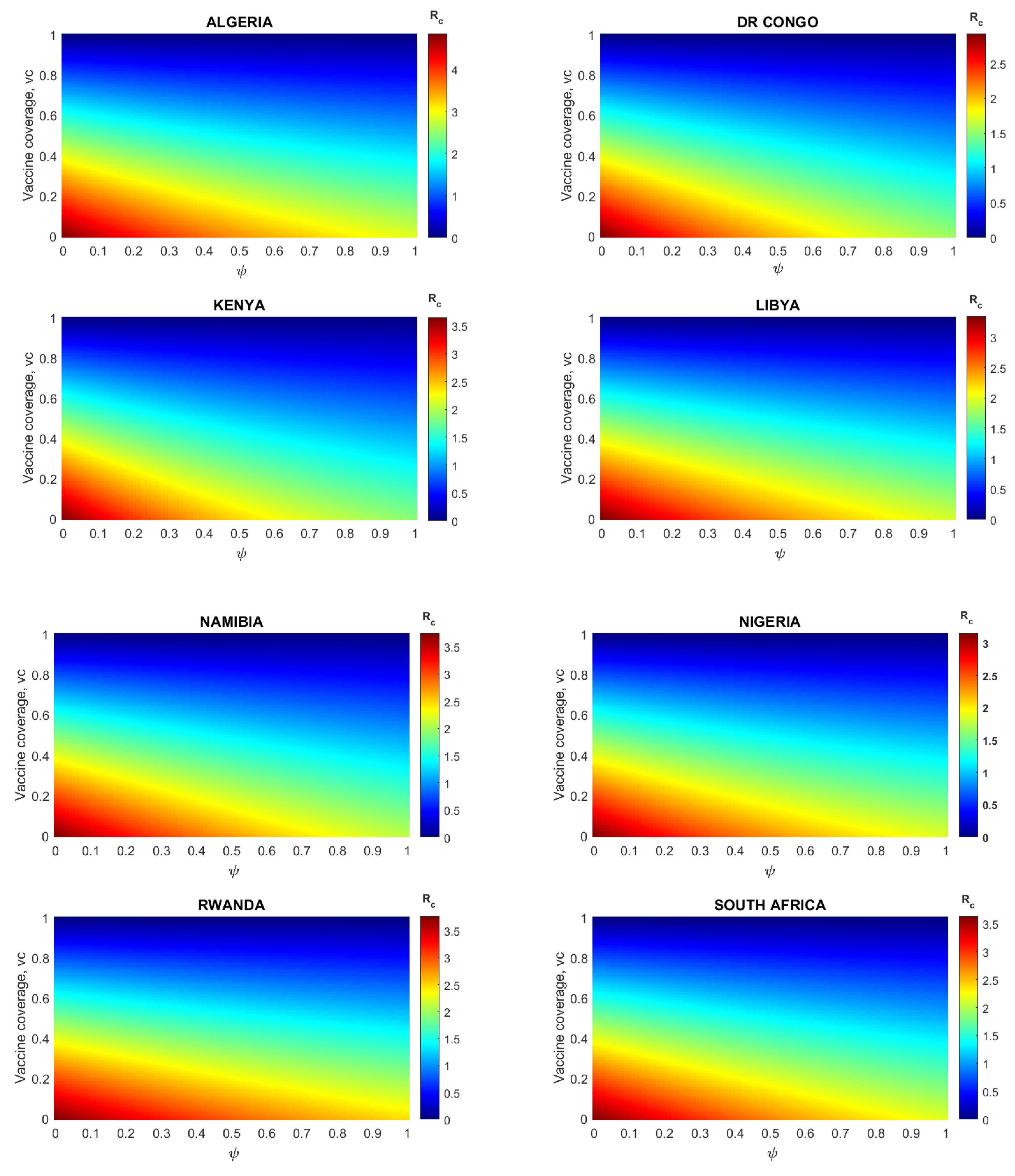
3.2.2. Impact of Vaccination on the Control Reproduction Number per Country
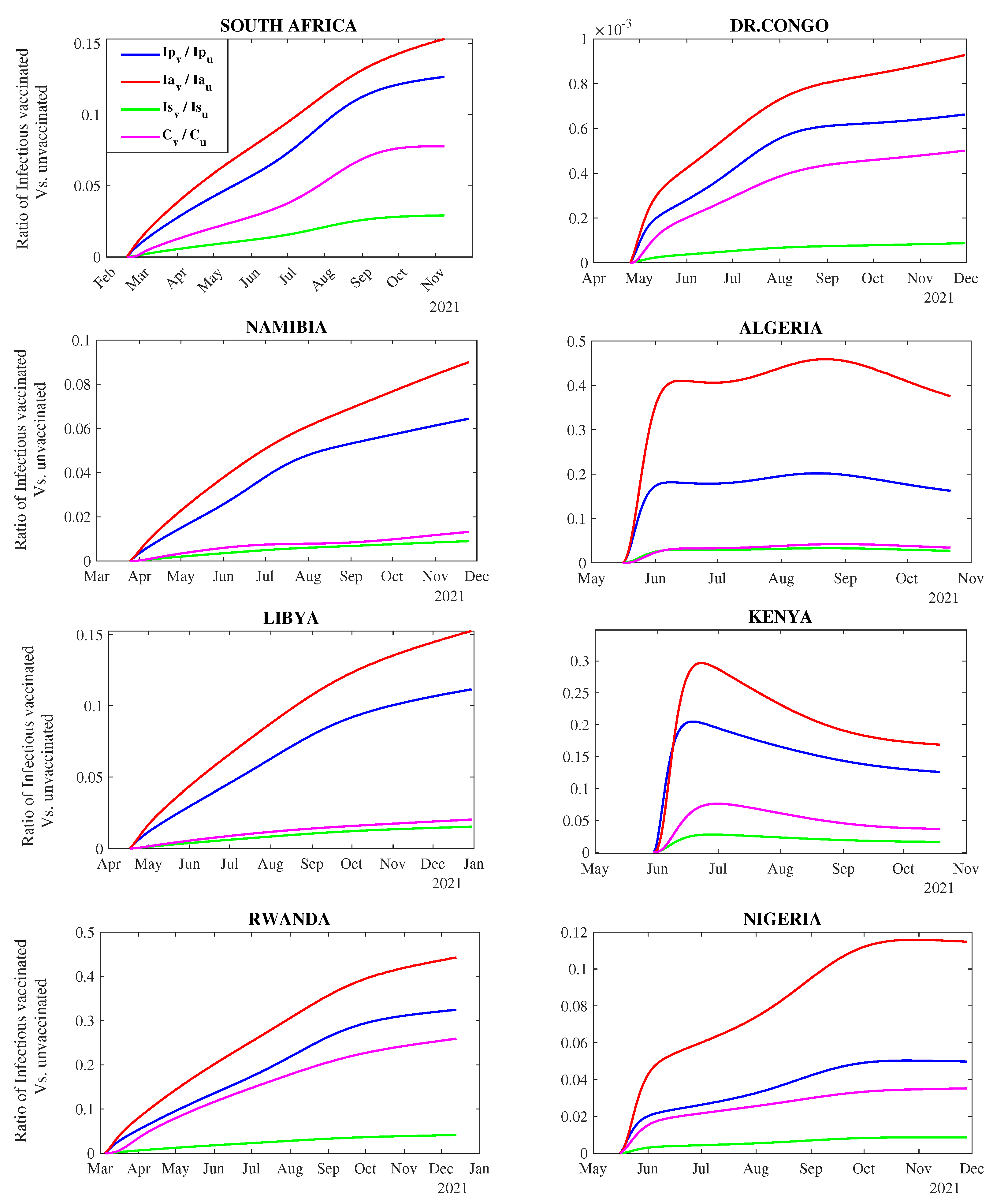
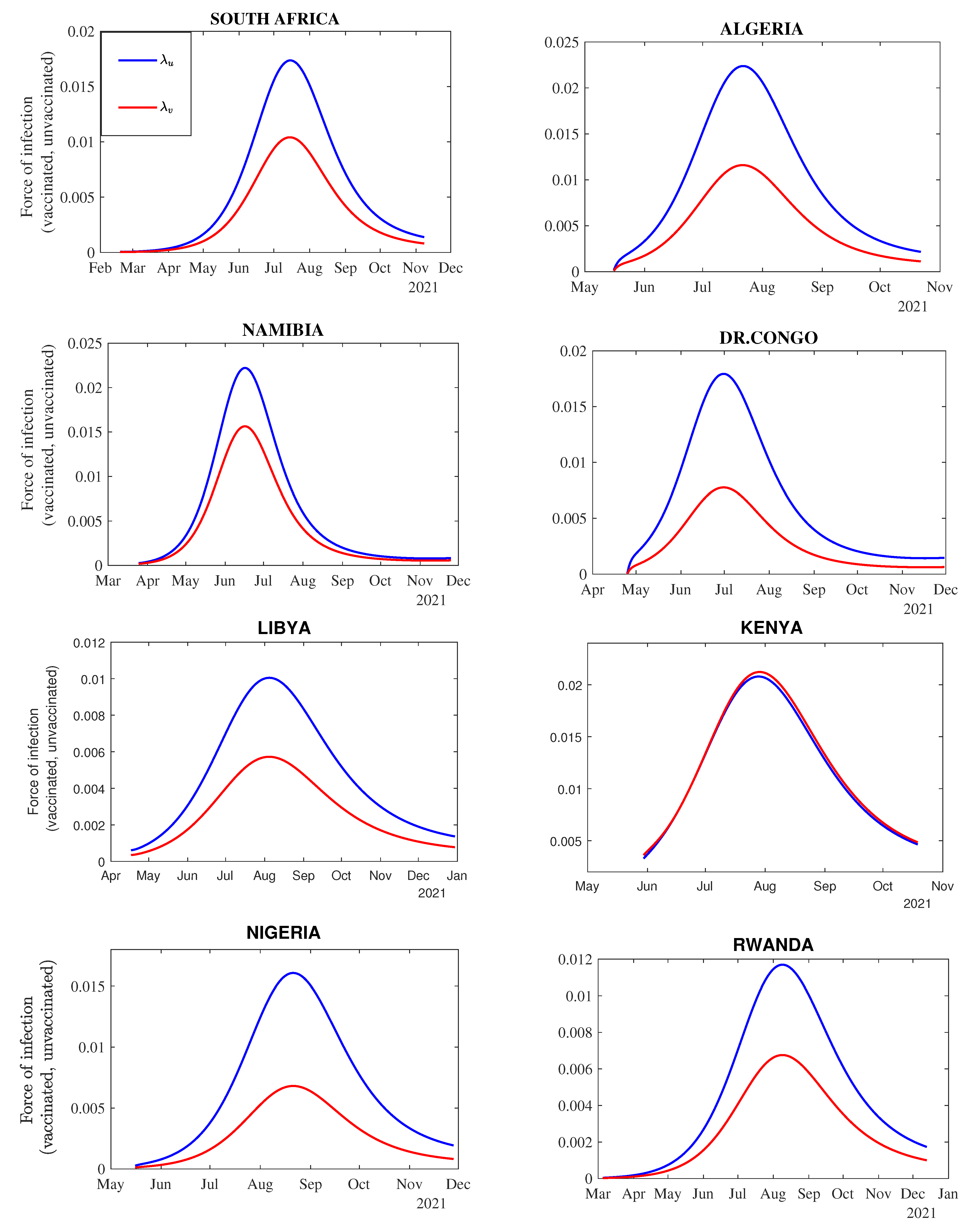
3.2.3. Impact of Vaccination on the Transmission Dynamics
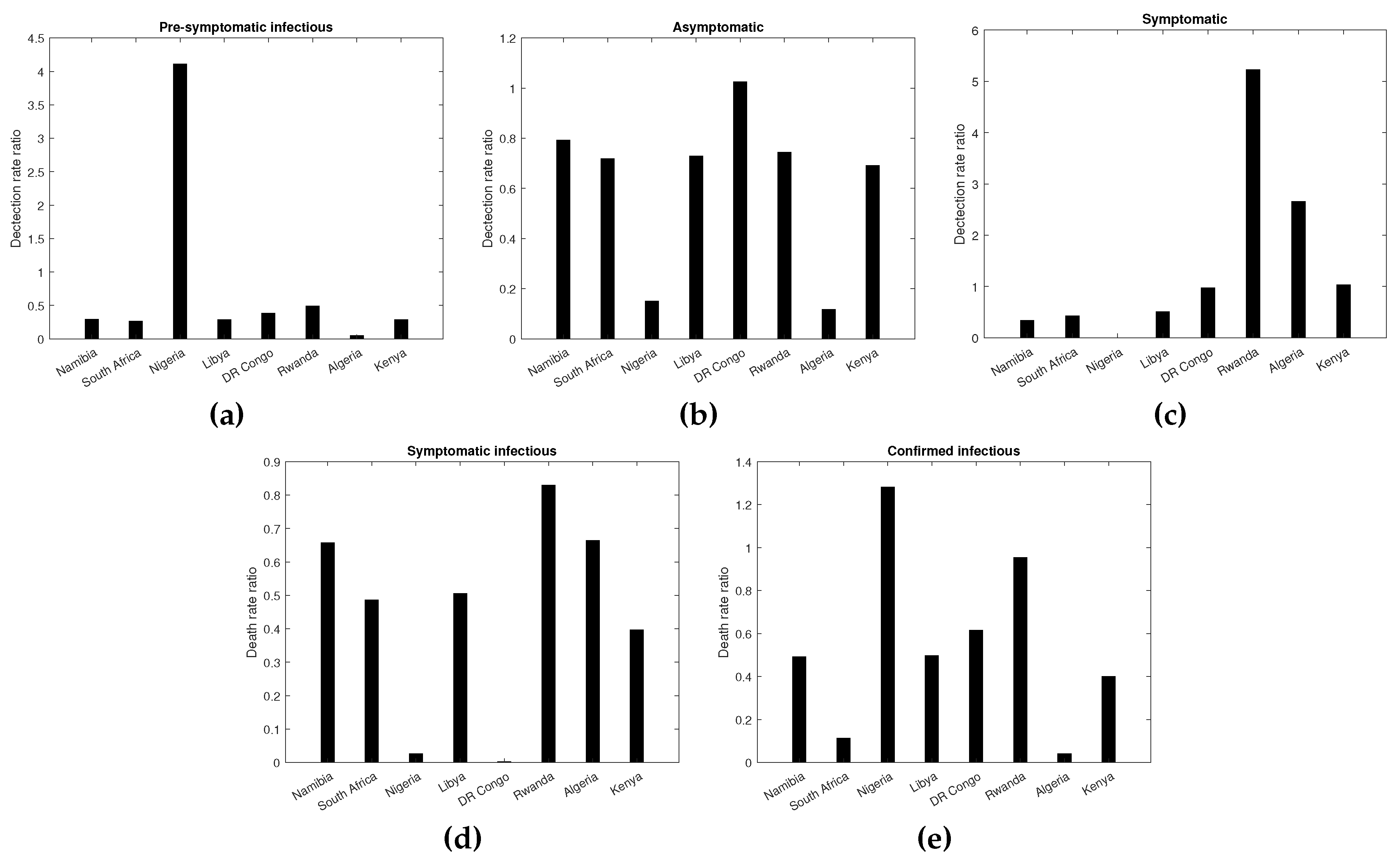
3.2.4. Impact of Vaccination on COVID-19 Incidence among the Vaccinated and Unvaccinated Individuals
3.2.5. Impact of Vaccination on COVID-19 Mortality among the Vaccinated and Unvaccinated Individuals
3.2.6. Impact of Vaccine Coverage with Different Levels of Reduction in the Transmission Rate due to NPIs () among Unvaccinated and Vaccinated Individuals
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Selected Countries | Start Date | End Date |
|---|---|---|
| DR Congo | 25 April 2021 | 30 November 2021 |
| Rwanda | 5 March 2021 | 13 December 2021 |
| Kenya | 30 May 2021 | 19 October 2021 |
| Algeria | 4 January 2021 | 29 October 2021 |
| Libya | 13 January 2021 | 13 December 2021 |
| Namibia | 25 March 2021 | 25 November 2021 |
| South Africa | 18 February 2021 | 8 November 2021 |
| Nigeria | 16 May 2021 | 28 November 2021 |
| Parameter | Value | References |
|---|---|---|
| [50] | ||
| [51] | ||
| [52] | ||
| [53] | ||
| [25] | ||
| 0.6 | [54] | |
| 0.1 | [55] | |
| [29,54] | ||
| [29,54] | ||
| [29,54] | ||
| [29,54] | ||
| [29,54] | ||
| [29,54] |




| Parameters | Countries | |||||||
|---|---|---|---|---|---|---|---|---|
| Algeria | DR Congo | Kenya | Libya | Namibia | Nigeria | Rwanda | South Africa | |
| L.E | 77.5 | 61.6 | 67.5 | 73.4 | 64.9 | 55.8 | 70.0 | 64.9 |
| 44,177,969 | 95,894,118 | 53,005,614 | 6,735,277 | 2,530,151 | 213,401,323 | 13,461,888 | 59,392,255 | |
| 6227.61 | 17,591.26 | 10,285.07 | 433.56 | 264.94 | 39,787.80 | 1424.71 | 4999.12 | |
| VC | 13.62% | 0.15% | 6.38% | 27.5% | 13.69% | 3.00% | 35.5% | 26.6% |
| 160 | 220 | 143 | 258 | 246 | 197 | 284 | 264 | |
| 0.00085 | 0.00001 | 0.00045 | 0.00107 | 0.00056 | 0.00015 | 0.00125 | 0.00101 | |
| 0.35 | 0.30 | 0.15 | 0.35 | 0.30 | 0.45 | 0.45 | 0.45 | |
| 0.25 | 0.25 | 0.18 | 0.25 | 0.25 | 0.25 | 0.25 | 0.45 |
| Country | ||||||
| Namibia | 1.66 [1.57, 1.74] | 1500.00 [1365.29, 1634.70] | 700.15 [641.35, 758.9] | 706.06 [675.15, 736.97] | 700.00 [672.02, 727.97] | 144.62 [105.10, 184.14] |
| South Africa | 44.87 [43.13, 46.60] | 4763.61 [4179.73, 5347.49] | 5499.92 [5214.45, 5785.39] | 1322.84 [970.52, 1675.16] | 265.16 [223.47, 306.86] | 455.28 [416.41, 494.15] |
| Nigeria | 49.94 [30.06, 69.72] | 76,207.26 [72,089.64, 80,324.87] | 39,377.52 [36,424.84, 242,330.20] | 12,989.71 [11,127.50, 14,851.92] | 571.77 [425.02, 718.52] | 346.74 [194.97, 498.51] |
| Libya | 4.19 [3.80, 4.58] | 10043.62 [9799.05, 10,288.17] | 7097.94 [6808.63, 7387.25] | 5144.00 [4593.28, 5694.72] | 2500.26 [2252.15, 2748.37] | 1159.89 [1058.219, 1261.57] |
| DR.Congo | 7.14 [2.09, 12.19] | 69,889.75 [66,287.98, 73,491.51] | 1002.16 [902.45, 1101.87] | 541.19 [442.15, 640.22] | 784.58 [734.78, 834.37] | 249.44 [230.28, 268.59] |
| Rwanda | 13.35 [12.58, 14.13] | 3191.59 [2882.33, 3500.86] | 1120.60 [1041.19, 1200.01] | 1011.78 [858.52, 1165.04] | 741.58 [714.24, 768.93] | 251.03 [208.27, 293.79] |
| Algeria | 9.58 [5.42, 13.72] | 93,208.19 [88,602.33, 97,814.04] | 4344.26 [3988.51, 4700.00] | 530.67 [115.97, 945.38] | 581.77 [ 542.56, 620.99] | 100.51 [63.13, 137.89] |
| Kenya | 4.32 [4.06, 4.55] | 77,571.99 [68,155.25, 86,988.73] | 44,589.27 [41,245.57, 47,932.96] | 34,186.64 [31,497.56, 36,875.72] | 13,641.08 [12,529.16, 14,753.01] | 962.79 [924.76, 1000.82] |
| Parameter | Namibia | South Africa | Nigeria | Libya |
|---|---|---|---|---|
| 0.69943 [0.66876, 0.73010] | 0.75138 [0.70816, 0.79461] | 0.68895 [0.64075, 0.73716] | 0.34566 [0.31123, 0.38009] | |
| 0.49986 [0.46100, 0.53872] | 0.47487 [0.43008, 0.51967] | 0.29131 [0.25009, 0.33253] | 0.19777 [0.18971, 0.20583] | |
| 0.49949 [0.44789, 0.55109] | 0.69237 [0.62429, 0.76045] | 0.20114 [0.14281, 0.25947] | 0.13348 [0.11327, 0.15354] | |
| 0.09929 [0.09199, 0.10658] | 0.09903 [0.09701, 0.10105] | 0.09582 [0.09138, 0.10026] | 0.05061 [0.04610, 0.05513] | |
| 0.99999 [0.90132, 1.09866] | 0.94265 [0.85095, 1.03434] | 0.81294 [0.69935, 0.92650] | 0.97356 [0.88567, 1.06144] | |
| 0.25624 [0.17032, 0.34215] | 0.32720 [0.24394, 0.41045] | 0.32603 [0.22519, 0.42687] | 0.54310 [0.44715, 0.63904] | |
| 0.00012 [−0.0679, 0.06822] | 0.11758 [0.02434, 0.21083] | 0.64576 [0.83210, 0.96535] | 0.51002 [0.47033, 0.54970] | |
| 0.01583 [−0.0229, 0.05461] | 0.28121 [0.20859, 0.35382] | 0.88343 [0.79233, 0.97452] | 0.87620 [0.78317, 0.96922] | |
| 0.68982 [0.61379, 0.76585] | 0.69391 [0.61708, 0.77070] | 0.89522 [0.77477, 1.01567] | 0.49071 [0.44117, 0.52506] | |
| 0.27906 [0.20984, 0.34828] | 0.59369 [0.52832, 0.65905] | 0.91138 [0.79100, 1.03177] | 0.47209 [0.42120, 0.52289] | |
| 0.19411 [0.12131, 0.26691] | 0.00502 [-0.0760, 0.08605] | 0.85105 [0.75183, 0.95027] | 0.59134 [0.52606, 0.65661] | |
| 0.64782 [0.57741, 0.71824] | 0.21637 [0.13351, 0.29921] | 0.63620 [0.56903, 0.70337] | 0.37854 [0.32847, 0.42861] | |
| 0.00499 [0.00492, 0.00506] | 0.00499 [0.00496, 0.00502] | 0.00006 [−0.0002, 0.00019] | 0.00486 [0.00440, 0.00532] | |
| 0.00067 [0.00063, 0.00072] | 0.00131 [0.00126, 0.00135] | 0.00026 [0.00018, 0.00034] | 0.00139 [0.00129, 0.00149] | |
| 0.00498 [0.00465, 0.00532] | 0.00497 [0.00489, 0.00505] | 0.00027 [−0.00004, 0.0006] | 0.00351 [0.00309, 0.00392] | |
| 0.00395 [0.00371, 0.00419] | 0.00256 [0.00253, 0.00265] | 0.00004 [−0.0003, 0.00040] | 0.00256 [0.00237, 0.00276] | |
| 0.00868 [0.00824, 0.00913] | 0.00839 [0.00829, 0.00851] | 0.00031 [−0.0005, 0.00114] | 0.00862 [0.00792, 0.00933] | |
| 0.00294 [0.00280, 0.00309] | 0.00356 [0.00341, 0.00372] | 0.000004 [−0.0004, 0.0004] | 0.00439 [0.00407, 0.00472] | |
| 0.00029 [0.00028, 0.00031] | 0.19703 [0.17974, 0.00211] | 0.00567 [0.00458, 0.00677] | 0.00197 [0.00183, 0.02114] | |
| 0.00019 [0.00018, 0.00020] | 0.09581 [0.08846, 0.10316] | 0.00015 [−0.0007, 0.00098] | 0.00099 [0.00182, 0.00217] | |
| 0.00040 [0.00038, 0.00042] | 0.19959 [0.17916, 0.22004] | 0.00298 [0.00221, 0.00375] | 0.00199 [0.01899, 0.02094] | |
| 0.00019 [0.00018, 0.00020] | 0.02278 [0.01553, 0.03003] | 0.00382 [0.00308, 0.00457] | 0.00099 [0.00090, 0.00108] |
| Parameter | Rwanda | Algeria | Kenya | DR Congo |
|---|---|---|---|---|
| 0.56684 [0.54223, 0.59140] | 0.79907 [0.74159, 0.85655] | 0.63721 [0.58228, 0.69215] | 0.59252 [0.55302, 0.63202] | |
| 0.32961 [0.28843, 0.37078] | 0.44401 [0.39858, 0.48943] | 0.69956 [0.66150, 0.73763] | 0.25625 [0.18964, 0.32285] | |
| 0.34471 [0.30639, 0.38305] | 0.54705 [0.48178, 0.61232] | 0.49691 [0.46349, 0.53033] | 0.29970 [0.26933, 0.33008] | |
| 0.18714 [0.17146, 0.20282] | 0.05621 [0.05062, 0.06181] | 0.04087 [0.02406, 0.05769] | 0.01336 [0.00516, 0.02154] | |
| 0.49657 [0.45476, 0.53838] | 0.95831 [0.90050, 1.01612] | 0.46168 [0.42345, 0.49992] | 0.99997 [0.94617, 1.05378] | |
| 0.38102 [0.32949, 0.43255] | 0.36306 [0.26965, 0.45647] | 0.24275 [0.21254, 0.27297] | 0.42697 [0.33455, 0.51938] | |
| 0.43582 [0.41439, 0.45727] | 0.22221 [0.11050, 0.33392] | 0.31683 [0.26989, 0.36376] | 0.00335 [−0.0765, 0.08316] | |
| 0.41064 [0.35984, 0.46145] | 0.17918 [0.09015, 0.26821] | 0.08219 [0.03981, 0.12458] | 0.10705 [0.05563, 0.15847] | |
| 0.48203 [0.43416, 0.52992] | 0.23469 [0.15878, 0.31059] | 0.45516 [0.41124, 0.49907] | 0.22848 [0.17245, 0.28450] | |
| 0.49791 [0.44987, 0.54594] | 0.48487 [0.42802, 0.54172] | 0.25320 [0.23014, 0.27626] | 0.01724 [−0.0390, 0.07350] | |
| 0.35278 [0.31528, 0.39029] | 0.62145 [0.55725, 0.68564] | 0.39507 [0.35426, 0.43587] | 0.48985 [ 0.44160, 0.5380] | |
| 0.03734 [0.00201, 0.07265] | 0.73060 [0.65886, 0.80235] | 0.00433 [−0.0367, 0.04540] | 0.40973 [0.35467, 0.4648] | |
| 0.00019 [0.00018, 0.00022] | 0.00163 [0.00109, 0.00215] | 0.00019 [0.00018, 0.00021] | 0.00073 [0.00053, 0.00092] | |
| 0.00010 [0.00009, 0.00011] | 0.00008 [0.00007, 0.00009] | 0.00006 [0.00005, 0.00010] | 0.00028 [0.00020, 0.00035] | |
| 0.00254 [0.00227, 0.00281] | 0.00025 [−0.0003, 0.00079] | 0.00288 [0.00269, 0.00306] | 0.00095 [0.00077, 0.00113] | |
| 0.00189 [0.00170, 0.00208] | 0.00003 [−0.0002, 0.00026] | 0.00199 [0.00185, 0.00213] | 0.00097 [0.00089, 0.00106] | |
| 0.00018 [−0.0003, 0.00064] | 0.00130 [0.00042, 0.00218] | 0.00192 [0.00171, 0.00213] | 0.000009 [−0.0004, 0.0005] | |
| 0.00091 [0.00086, 0.00096] | 0.003461 [0.0031, 0.00387] | 0.00198 [0.00180, 0.00216] | 0.00001 [0.00000, 0.00002] | |
| 0.00023 [0.00020, 0.00025] | 0.00025 [0.00022, 0.00027] | 0.00029 [0.00027, 0.00032] | 0.00026 [0.00023, 0.00028] | |
| 0.00019 [0.00018, 0.00020] | 0.00017 [0.00012, 0.00021] | 0.00012 [0.00010, 0.00013] | 0.000001 [0.0000, 0.00002] | |
| 0.00021 [0.00019, 0.00023] | 0.00052 [0.00048, 0.00056] | 0.00014 [0.00013, 0.00015] | 0.00029 [0.00028, 0.00031] | |
| 0.00019 [0.00019, 0.00021] | 0.00002 [−0.00001, 0.00005] | 0.00006 [0.00005, 0.00010] | 0.00018 [0.00016, 0.00020] |
| Parameter | |||||
|---|---|---|---|---|---|
| Namibia | 0.813 [0.775, 0.851] | 0.011 [0.009, 0.013] | 0.889 [0.851, 0.927] | 1.713 [1.639, 1.788] | 2.569 [2.449, 2.688] |
| South Africa | 0.670 [0.658, 0.683] | 0.002 [0.015, 0.017] | 0.800 [0.786, 0.820] | 1.500 [1.464, 1.515] | 3.131 [3.099, 3.163] |
| Nigeria | 0.777 [0.749, 0.829] | 0.021 [0.019, 0.024] | 0.801 [0.772, 0.829] | 1.599 [1.554, 1.643] | 3.157 [3.049, 3.265] |
| Libya | 0.699 [0.682, 0.716] | 0.010 [0.009, 0.012] | 0.723 [0.707, 0.739] | 1.432 [1.399, 1.464] | 2.586 [2.525, 2.647] |
| DR Congo | 0.841 [0.778, 0.903] | 0.00 [0.000, 0.001] | 0.841 [0.778, 0.903] | 1.682 [1.557, 1.808] | 2.407 [2.228, 2.587] |
| Rwanda | 0.853 [0.841, 0.865] | 0.040 [0.036, 0.044] | 0.912 [0.896, 0.928] | 1.806 [1.781, 1.831] | 2.817 [2.777, 2.856] |
| Algeria | 0.908 [0.805, 1.011] | 0.007 [0.005, 0.009] | 0.987 [0.8797, 1.094] | 1.902 [1.026, 2.237] | 3.640 [2.893, 3.634] |
| Kenya | 0.225 [0.222, 0.227] | 0.836 [0.801, 0.872] | 0.007 [0.004, 0.011] | 1.911 [1.864, 1.986] | 2.438 [2.335, 2.543] |
References
- Niu, Y.; Rui, J.; Wang, Q.; Zhang, W.; Chen, Z.; Xie, F.; Zhao, Z.; Lin, S.; Zhu, Y.; Wang, Y.; et al. Containing the transmission of COVID-19: A modeling study in 160 countries. Front. Med. 2021, 8, 701836. [Google Scholar] [CrossRef]
- Khalifa, S.A.; Swilam, M.M.; El-Wahed, A.A.A.; Du, M.; El-Seedi, H.H.; Kai, G.; Masry, S.H.; Abdel-Daim, M.M.; Zou, X.; Halabi, M.F.; et al. Beyond the Pandemic: COVID-19 Pandemic Changed the Face of Life. Int. J. Environ. Res. Public Health 2021, 18, 5645. [Google Scholar] [CrossRef] [PubMed]
- Spiteri, G.; Fielding, J.; Diercke, M.; Campese, C.; Enouf, V.; Gaymard, A.; Bella, A.; Sognamiglio, P.; Moros, M.J.S.; Riutort, A.N.; et al. First cases of coronavirus disease 2019 (COVID-19) in the WHO European Region, 24 January to 21 February 2020. Eurosurveillance 2020, 25, 2000178. [Google Scholar] [CrossRef] [PubMed]
- Bouba, Y.; Tsinda, E.K.; Fonkou, M.D.M.; Mmbando, G.S.; Bragazzi, N.L.; Kong, J.D. The determinants of the low COVID-19 transmission and mortality rates in Africa: A cross-country analysis. Front. Public Health 2021, 9, 751197. [Google Scholar] [CrossRef]
- WHO. Weekly Bulletin on Outbreak and other Emergencies: Week 12: 14–20 March 2022; Technical documents; World Health Organization. Regional Office for Africa: Brazzaville, Republic of Congo, 2022. [Google Scholar]
- Mendez-Brito, A.; El Bcheraoui, C.; Pozo-Martin, F. Systematic review of empirical studies comparing the effectiveness of non-pharmaceutical interventions against COVID-19. J. Infect. 2021, 83, 281–293. [Google Scholar] [CrossRef] [PubMed]
- Ejigu, B.A.; Asfaw, M.D.; Cavalerie, L.; Abebaw, T.; Nanyingi, M.; Baylis, M. Assessing the impact of non-pharmaceutical interventions (NPI) on the dynamics of COVID-19: A mathematical modelling study of the case of Ethiopia. PLoS ONE 2021, 16, e0259874. [Google Scholar] [CrossRef] [PubMed]
- Cai, C.; Peng, Y.; Shen, E.; Huang, Q.; Chen, Y.; Liu, P.; Guo, C.; Feng, Z.; Gao, L.; Zhang, X.; et al. A comprehensive analysis of the efficacy and safety of COVID-19 vaccines. Mol. Ther. 2021, 29, 2794–2805. [Google Scholar] [CrossRef]
- Ngonghala, C.N.; Iboi, E.; Eikenberry, S.; Scotch, M.; MacIntyre, C.R.; Bonds, M.H.; Gumel, A.B. Mathematical assessment of the impact of non-pharmaceutical interventions on curtailing the 2019 novel Coronavirus. Math. Biosci. 2020, 325, 108364. [Google Scholar] [CrossRef]
- Wang, R.; Zhang, Q.; Ge, J.; Ren, W.; Zhang, R.; Lan, J.; Ju, B.; Su, B.; Yu, F.; Chen, P.; et al. Analysis of SARS-CoV-2 variant mutations reveals neutralization escape mechanisms and the ability to use ACE2 receptors from additional species. Immunity 2021, 54, 1611–1621. [Google Scholar] [CrossRef]
- Shattock, A.J.; Le Rutte, E.A.; Dünner, R.P.; Sen, S.; Kelly, S.L.; Chitnis, N.; Penny, M.A. Impact of vaccination and non-pharmaceutical interventions on SARS-CoV-2 dynamics in Switzerland. Epidemics 2022, 38, 100535. [Google Scholar] [CrossRef]
- Yang, B.; Yu, Z.; Cai, Y. The impact of vaccination on the spread of COVID-19: Studying by a mathematical model. Phys. A Stat. Mech. Its Appl. 2022, 590, 126717. [Google Scholar] [CrossRef]
- Randolph, H.E.; Barreiro, L.B. Herd immunity: Understanding COVID-19. Immunity 2020, 52, 737–741. [Google Scholar] [CrossRef] [PubMed]
- Knoll, M.D.; Wonodi, C. Oxford–AstraZeneca COVID-19 vaccine efficacy. Lancet 2021, 397, 72–74. [Google Scholar] [CrossRef] [PubMed]
- Loembé, M.M.; Nkengasong, J.N. COVID-19 vaccine access in Africa: Global distribution, vaccine platforms, and challenges ahead. Immunity 2021, 54, 1353–1362. [Google Scholar] [CrossRef]
- COVID-19 Vaccination Rate in Africa 2022, by Country. Available online: https://www.statista.com/statistics/1221298/covid-19-vaccination-rate-in-african-countries. (accessed on 26 August 2022).
- Nachega, J.B.; Sam-Agudu, N.A.; Masekela, R.; van der Zalm, M.M.; Nsanzimana, S.; Condo, J.; Ntoumi, F.; Rabie, H.; Kruger, M.; Wiysonge, C.S.; et al. Addressing challenges to rolling out COVID-19 vaccines in African countries. Lancet Glob. Health 2021, 9, e746–e748. [Google Scholar] [CrossRef] [PubMed]
- Al-Kassim Hassan, M.; Adam Bala, A.; Jatau, A.I. Low rate of COVID-19 vaccination in Africa: A cause for concern. Ther. Adv. Vaccines Immunother. 2022, 10, 25151355221088159. [Google Scholar] [CrossRef] [PubMed]
- Bernal, J.L.; Andrews, N.; Gower, C.; Gallagher, E.; Simmons, R.; Thelwall, S.; Stowe, J.; Tessier, E.; Groves, N.; Dabrera, G.; et al. Effectiveness of COVID-19 vaccines against the B. 1.617. 2 (Delta) variant. N. Engl. J. Med. 2021, 385, 585–594. [Google Scholar] [CrossRef]
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA COVID-19 vaccine in a nationwide mass vaccination setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef]
- Hagan, L.M.; McCormick, D.W.; Lee, C.; Sleweon, S.; Nicolae, L.; Dixon, T.; Banta, R.; Ogle, I.; Young, C.; Dusseau, C.; et al. Outbreak of SARS-CoV-2 B. 1.617. 2 (Delta) variant infections among incarcerated persons in a federal prison—Texas, July–August 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 1349. [Google Scholar] [CrossRef]
- MacIntyre, C.R.; Costantino, V.; Trent, M. Modelling of COVID-19 vaccination strategies and herd immunity, in scenarios of limited and full vaccine supply in NSW, Australia. Vaccine 2021, 40, 2506–2513. [Google Scholar] [CrossRef]
- Jentsch, P.C.; Anand, M.; Bauch, C.T. Prioritising COVID-19 vaccination in changing social and epidemiological landscapes: A mathematical modelling study. Lancet Infect. Dis. 2021, 21, 1097–1106. [Google Scholar] [CrossRef] [PubMed]
- McNamara, L.A.; Wiegand, R.E.; Burke, R.M.; Sharma, A.J.; Sheppard, M.; Adjemian, J.; Ahmad, F.B.; Anderson, R.N.; Barbour, K.E.; Binder, A.M.; et al. Estimating the early impact of the US COVID-19 vaccination programme on COVID-19 cases, emergency department visits, hospital admissions, and deaths among adults aged 65 years and older: An ecological analysis of national surveillance data. Lancet 2022, 399, 152–160. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.; Kim, J.S.; Kim, J.E.; Choi, H.; Lee, C.H. Vaccination prioritization strategies for COVID-19 in Korea: A mathematical modeling approach. Int. J. Environ. Res. Public Health 2021, 18, 4240. [Google Scholar] [CrossRef] [PubMed]
- Iboi, E.A.; Ngonghala, C.N.; Gumel, A.B. Will an imperfect vaccine curtail the COVID-19 pandemic in the US? Infect. Dis. Model. 2020, 5, 510–524. [Google Scholar] [PubMed]
- Machado, B.; Antunes, L.; Caetano, C.; Pereira, J.F.; Nunes, B.; Patrício, P.; Morgado, M.L. The impact of vaccination on the evolution of COVID-19 in Portugal. Math. Biosci. Eng. 2022, 19, 936–952. [Google Scholar] [CrossRef]
- Fisman, D.N.; Amoako, A.; Tuite, A.R. Impact of population mixing between vaccinated and unvaccinated subpopulations on infectious disease dynamics: Implications for SARS-CoV-2 transmission. CMAJ 2022, 194, E573–E580. [Google Scholar] [CrossRef]
- Taboe, H.B.; Asare-Baah, M.; Yesmin, A.; Ngonghala, C.N. The impact of age structure and vaccine prioritization on COVID-19 in West Africa. Infect. Dis. Model. 2022, 7, 709–727. [Google Scholar] [CrossRef]
- Zuo, C.; Meng, Z.; Zhu, F.; Zheng, Y.; Ling, Y. Assessing vaccination prioritization strategies for COVID-19 in south africa based on age-specific compartment model. Front. Public Health 2022, 10, 876551. [Google Scholar] [CrossRef]
- Yang, C.; Yang, Y.; Li, Y. Assessing vaccination priorities for different ages and age-specific vaccination strategies of COVID-19 using an SEIR modelling approach. PLoS ONE 2021, 16, e0261236. [Google Scholar] [CrossRef]
- Ackah, B.B.; Woo, M.; Stallwood, L.; Fazal, Z.A.; Okpani, A.; Ukah, U.V.; Adu, P.A. COVID-19 vaccine hesitancy in Africa: A scoping review. Glob. Health Res. Policy 2022, 7, 1–20. [Google Scholar] [CrossRef]
- Mutombo, P.N.; Fallah, M.P.; Munodawafa, D.; Kabel, A.; Houeto, D.; Goronga, T.; Mweemba, O.; Balance, G.; Onya, H.; Kamba, R.S.; et al. COVID-19 vaccine hesitancy in Africa: A call to action. Lancet Glob. Health 2022, 10, e320–e321. [Google Scholar] [CrossRef] [PubMed]
- Kanyanda, S.; Markhof, Y.; Wollburg, P.; Zezza, A. Acceptance of COVID-19 vaccines in sub-Saharan Africa: Evidence from six national phone surveys. BMJ Open 2021, 11, e055159. [Google Scholar] [CrossRef] [PubMed]
- Clemens, J.; Aziz, A.B.; Tadesse, B.T.; Kang, S.; Marks, F.; Kim, J. Evaluation of protection by COVID-19 vaccines after deployment in low and lower-middle income countries. EClinicalMedicine 2022, 43, 101253. [Google Scholar] [CrossRef] [PubMed]
- Rabiu, M.; Iyaniwura, S.A. Assessing the potential impact of immunity waning on the dynamics of COVID-19 in South Africa: An endemic model of COVID-19. Nonlinear Dyn. 2022, 109, 203–223. [Google Scholar] [CrossRef]
- Choe, P.G.; Kang, C.K.; Suh, H.J.; Jung, J.; Song, K.H.; Bang, J.H.; Kim, E.S.; Kim, H.B.; Park, S.W.; Kim, N.J.; et al. Waning antibody responses in asymptomatic and symptomatic SARS-CoV-2 infection. Emerg. Infect. Dis. 2021, 27, 327. [Google Scholar] [CrossRef]
- Goldberg, Y.; Mandel, M.; Bar-On, Y.M.; Bodenheimer, O.; Freedman, L.; Haas, E.J.; Milo, R.; Alroy-Preis, S.; Ash, N.; Huppert, A. Waning immunity after the BNT162b2 vaccine in Israel. N. Engl. J. Med. 2021, 385, e85. [Google Scholar] [CrossRef]
- Tovissodé, C.F.; Doumatè, J.T.; Glèlè Kakaï, R. A Hybrid Modeling Technique of Epidemic Outbreaks with Application to COVID-19 Dynamics in West Africa. Biology 2021, 10, 365. [Google Scholar] [CrossRef] [PubMed]
- Diekmann, O.; Heesterbeek, J.A.P.; Metz, J.A. On the definition and the computation of the basic reproduction ratio R 0 in models for infectious diseases in heterogeneous populations. J. Math. Biol. 1990, 28, 365–382. [Google Scholar] [CrossRef]
- As, V.S.; Gribben, C.; Bishop, J.; Hanlon, P.; Caldwell, D.; Wood, R.; Reid, M.; McMenamin, J.; Goldberg, D.; Stockton, D.; et al. Effect of vaccination on transmission of COVID-19: An observational study in healthcare workers and their households. N. Engl. J. Med. 2021, 21, 2021-03. [Google Scholar]
- Marks, M.; Millat-Martinez, P.; Ouchi, D.; h Roberts, C.; Alemany, A.; Corbacho-Monné, M.; Ubals, M.; Tobias, A.; Tebé, C.; Ballana, E.; et al. Transmission of COVID-19 in 282 clusters in Catalonia, Spain: A cohort study. Lancet Infect. Dis. 2021, 21, 629–636. [Google Scholar] [CrossRef]
- Wang, Y.; Zheng, K.; Gao, W.; Lv, J.; Yu, C.; Wang, L.; Wang, Z.; Wang, B.; Liao, C.; Li, L. Asymptomatic and pre-symptomatic infection in Coronavirus Disease 2019 pandemic. Med Rev. 2022, 2, 66–88. [Google Scholar] [CrossRef]
- Chen, X.; Huang, Z.; Wang, J.; Zhao, S.; Wong, M.C.S.; Chong, K.C.; He, D.; Li, J. Ratio of asymptomatic COVID-19 cases among ascertained SARS-CoV-2 infections in different regions and population groups in 2020: A systematic review and meta-analysis including 130, 123 infections from 241 studies. BMJ Open 2021, 11, e049752. [Google Scholar] [CrossRef] [PubMed]
- Sobczak, M.; Pawliczak, R. COVID-19 vaccination efficacy in numbers including SARS-CoV-2 variants and age comparison: A meta-analysis of randomized clinical trials. Ann. Clin. Microbiol. Antimicrob. 2022, 21, 1–12. [Google Scholar] [CrossRef]
- Jabłońska, K.; Aballéa, S.; Toumi, M. The real-life impact of vaccination on COVID-19 mortality in Europe and Israel. Public Health 2021, 198, 230–237. [Google Scholar] [CrossRef]
- Musa, S.S.; Wang, X.; Zhao, S.; Li, S.; Hussaini, N.; Wang, W.; He, D. The heterogeneous severity of COVID-19 in African countries: A modeling approach. Bull. Math. Biol. 2022, 84, 1–16. [Google Scholar] [CrossRef]
- COVID-19 Vaccination—Africa CDC. Available online: https://www.cdc.gov/media/releases/2021/s1119-booster-shots.html (accessed on 26 August 2021).
- Onigbinde, O.A.; Ajagbe, A.O. COVID-19 vaccination and herd immunity In Africa: An incentive-based approach could be the game-changer to vaccine hesitancy. Public Health Pract. 2022, 4, 100282. [Google Scholar] [CrossRef]
- Townsend, J.P.; Hassler, H.B.; Sah, P.; Galvani, A.P.; Dornburg, A. The durability of natural infection and vaccine-induced immunity against future infection by SARS-CoV-2. Proc. Natl. Acad. Sci. USA 2022, 119, e2204336119. [Google Scholar] [CrossRef]
- Dan, J.M.; Mateus, J.; Kato, Y.; Hastie, K.M.; Yu, E.D.; Faliti, C.E.; Grifoni, A.; Ramirez, S.I.; Haupt, S.; Frazier, A.; et al. Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection. Science 2021, 371, eabf4063. [Google Scholar] [CrossRef]
- Curley, B. How long does immunity from COVID-19 vaccination last? Healthline. 2021. Available online: https://www.healthline.com/health-news/how-long-does-immunity-from-covid-19-vaccination-last (accessed on 25 July 2021).
- Xin, H.; Li, Y.; Wu, P.; Li, Z.; Lau, E.H.; Qin, Y.; Wang, L.; Cowling, B.J.; Tsang, T.; Li, Z. Estimating the latent period of coronavirus disease 2019 (COVID-19). Clin. Infect. Dis. 2021, 74, 1678–1681. [Google Scholar] [CrossRef] [PubMed]
- Mancuso, M.; Eikenberry, S.E.; Gumel, A.B. Will vaccine-derived protective immunity curtail COVID-19 variants in the US? Infect. Dis. Model. 2021, 6, 1110–1134. [Google Scholar] [CrossRef] [PubMed]
- Parry, H.; Tut, G.; Bruton, R.; Faustini, S.; Stephens, C.; Saunders, P.; Bentley, C.; Hilyard, K.; Brown, K.; Amirthalingam, G.; et al. mRNA vaccination in people over 80 years of age induces strong humoral immune responses against SARS-CoV-2 with cross neutralization of P. 1 Brazilian variant. Elife 2021, 10, e69375. [Google Scholar] [CrossRef] [PubMed]




| State Variable | Description |
|---|---|
| Susceptible unvaccinated (vaccinated) population | |
| Exposed unvaccinated (vaccinated) population | |
| Pre-symptomatic infectious unvaccinated (vaccinated) population | |
| Asymptomatic infectious unvaccinated (vaccinated) population | |
| Symptomatic infectious unvaccinated (vaccinated) population | |
| Confirmed infectious unvaccinated (vaccinated) population | |
| Recovered unvaccinated (vaccinated) population | |
| COVID-deceased unvaccinated (vaccinated) population |
| Parameter | Description | Unit |
|---|---|---|
| Recruitment rate | Individual | |
| Natural death rate | ||
| Vaccination rate | ||
| Vaccine-derived immunity rate | ||
| Latent period | days | |
| Pre-symptomatic period | days | |
| () | Rate at which recovered unvaccinated (vaccinated) individuals from COVID-19 lose acquired immunity | |
| Proportion of pre-symptomatic infectious unvaccinated (vaccinated), who develop COVID-19 symptoms | dimensionless | |
| Infection probability of a susceptible individual in class i by an infectious individual in class j, for | dimensionless | |
| COVID-19 death rate of symptomatic infectious unvaccinated (vaccinated) individuals | ||
| COVID-19 death rate of confirmed infectious unvaccinated (vaccinated) individuals | ||
| Recovery rate of asymptomatic unvaccinated (vaccinated) individuals | ||
| Recovery rate of symptomatic unvaccinated (vaccinated) individuals | ||
| Recovery rate of symptomatic unvaccinated (vaccinated) individuals | ||
| Relative infectiousness of unvaccinated pre-symptomatic (asymptomatic, symptomatic, confirmed) individuals | dimensionless | |
| Relative infectiousness of unvaccinated pre-symptomatic (asymptomatic, symptomatic, confirmed) individuals | dimensionless | |
| Per capita rate at which unvaccinated individuals from the pre-symptomatic (asymptomatic, symptomatic) infectious class test positive | ||
| Per capita rate at which vaccinated individuals from the pre-symptomatic (asymptomatic, symptomatic) infectious class test positive | ||
| COVID-19 induced death rate of unvaccinated (vaccinated) symptomatic infectious individuals | ||
| COVID-19 induced death rate of unvaccinated (vaccinated) confirmed infectious individuals |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montcho, Y.; Nalwanga, R.; Azokpota, P.; Doumatè, J.T.; Lokonon, B.E.; Salako, V.K.; Wolkewitz, M.; Glèlè Kakaï, R. Assessing the Impact of Vaccination on the Dynamics of COVID-19 in Africa: A Mathematical Modeling Study. Vaccines 2023, 11, 857. https://doi.org/10.3390/vaccines11040857
Montcho Y, Nalwanga R, Azokpota P, Doumatè JT, Lokonon BE, Salako VK, Wolkewitz M, Glèlè Kakaï R. Assessing the Impact of Vaccination on the Dynamics of COVID-19 in Africa: A Mathematical Modeling Study. Vaccines. 2023; 11(4):857. https://doi.org/10.3390/vaccines11040857
Chicago/Turabian StyleMontcho, Yvette, Robinah Nalwanga, Paustella Azokpota, Jonas Têlé Doumatè, Bruno Enagnon Lokonon, Valère Kolawole Salako, Martin Wolkewitz, and Romain Glèlè Kakaï. 2023. "Assessing the Impact of Vaccination on the Dynamics of COVID-19 in Africa: A Mathematical Modeling Study" Vaccines 11, no. 4: 857. https://doi.org/10.3390/vaccines11040857