
Adaptation and Validation of a French Version of the Vaccination Attitudes Examination (VAX) Scale


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
The VAX Scale Translation Process
2.3. Experimental Design
2.4. Questionnaires
2.4.1. French Version of the Vaccination Attitudes Examination (VAX) Scale
2.4.2. Vaccination Behaviours and Intentions
2.4.3. Vaccine Conspiracy Beliefs Scale
2.4.4. Beliefs about Medicines Questionnaire
2.4.5. Parent Attitudes about Childhood Vaccines Survey
2.4.6. Survey Validity Check
3. Results
3.1. Statistical Analyses
3.2. Results
3.2.1. Preliminary Analysis
3.2.2. Demographic and Clinical Characteristics
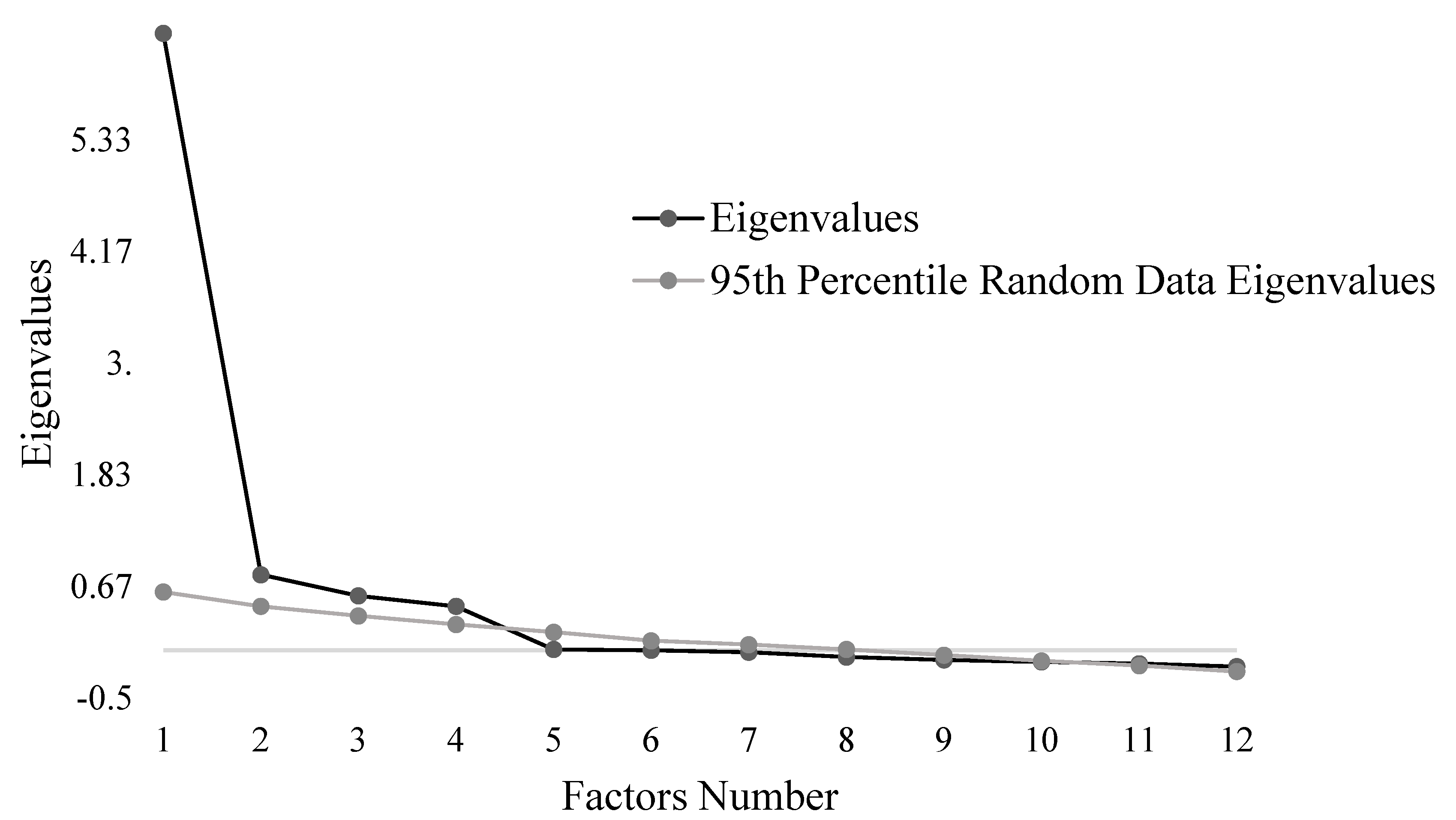
3.2.3. Exploratory Factor Analysis
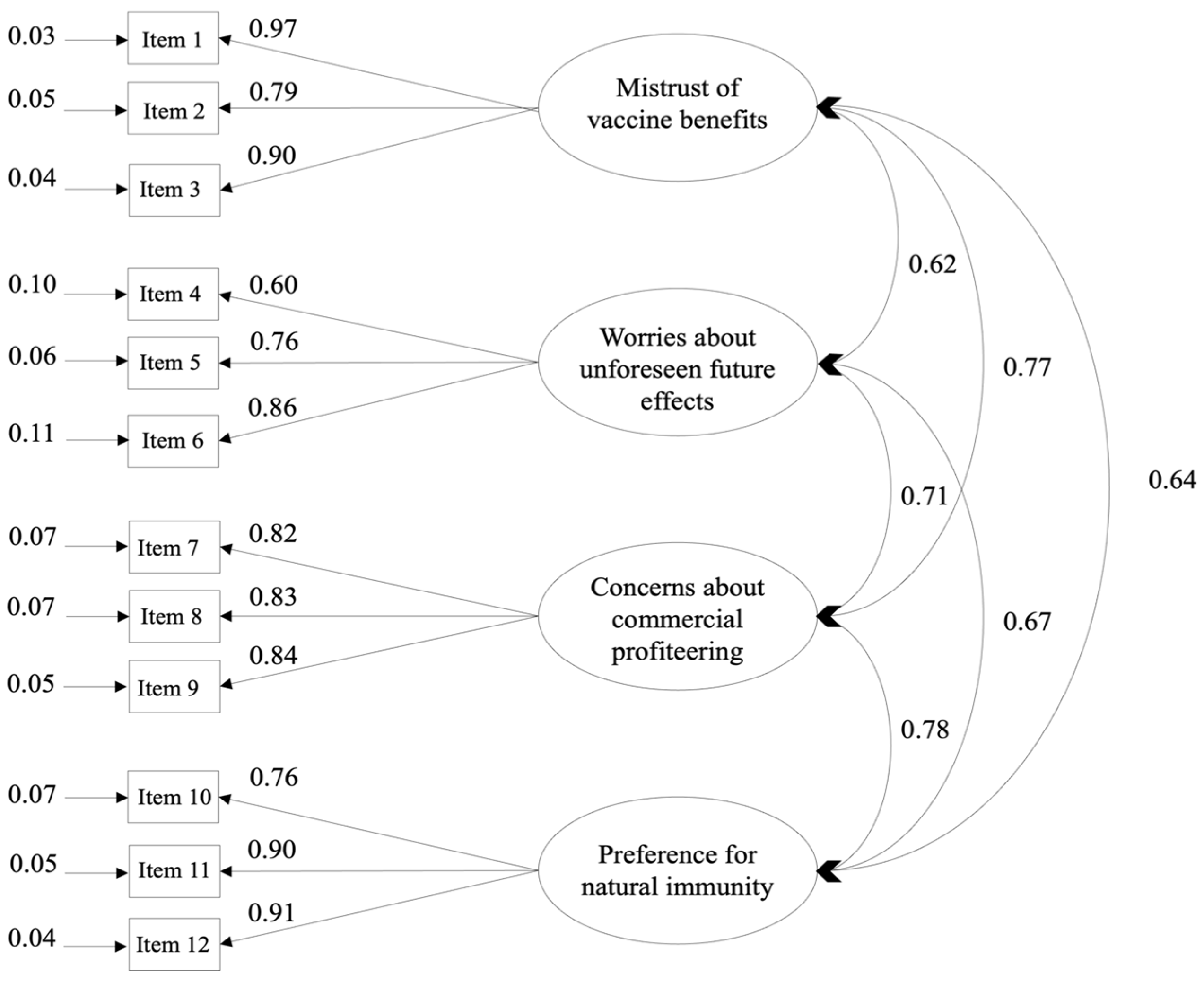
3.2.4. Confirmatory Factor Analysis
3.2.5. Internal Consistency
3.2.6. Convergent Validity
3.2.7. Divergent Validity
3.2.8. Temporal Stability
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Greenwood, B. The contribution of vaccination to global health: Past, present and future. Philos. Trans. R. Soc. B Biol. Sci. 2014, 369, 20130433. [Google Scholar] [CrossRef]
- Andre, F.; Booy, R.; Bock, H.; Clemens, J.; Datta, S.; John, T.; Lee, B.; Lolekha, S.; Peltola, H.; Ruff, T.; et al. Vaccination greatly reduces disease, disability, death and inequity worldwide. Bull. World Health Organ. 2008, 86, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Cassimos, D.C.; Effraimidou, E.; Medic, S.; Konstantinidis, T.; Theodoridou, M.; Maltezou, H.C. Vaccination Programs for Adults in Europe, 2019. Vaccines 2020, 8, 34. [Google Scholar] [CrossRef] [PubMed]
- Nichol, K.L.; Lind, A.; Margolis, K.L.; Murdoch, M.; McFadden, R.; Hauge, M.; Magnan, S.; Drake, M. The Effectiveness of Vaccination against Influenza in Healthy, Working Adults. N. Engl. J. Med. 1995, 333, 889–893. [Google Scholar] [CrossRef] [PubMed]
- Fisk, R.J.; Zhang, Y. Barriers to vaccination for coronavirus disease 2019 (COVID-19) control: Experience from the United States. Glob. Health J. 2021, 5, 51–55. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Larson, H.J.; de Figueiredo, A.; Xiahong, Z.; Schulz, W.S.; Verger, P.; Johnston, I.G.; Cook, A.R.; Jones, N.S. The State of Vaccine Confidence 2016: Global Insights Through a 67-Country Survey. EbioMedicine 2016, 12, 295–301. [Google Scholar] [CrossRef]
- Mueller, J. Les attitudes des Français face à la vaccination: Une évolution préoccupante. Médecine 2017, 13, 171–174. [Google Scholar] [CrossRef]
- Peretti-Watel, P.; Verger, P.; Raude, J.; Constant, A.; Gautier, A.; Jestin, C.; Beck, F. Dramatic change in public attitudes towards vaccination during the 2009 influenza A(H1N1) pandemic in France. Eurosurveillance 2013, 18, 20623. [Google Scholar] [CrossRef]
- Brown, K.F.; Kroll, J.S.; Hudson, M.J.; Ramsay, M.; Green, J.; Long, S.J.; Vincent, C.A.; Fraser, G.; Sevdalis, N. Factors underlying parental decisions about combination childhood vaccinations including MMR: A systematic review. Vaccine 2010, 28, 4235–4248. [Google Scholar] [CrossRef]
- Herzog, R.; Álvarez-Pasquin, M.J.; Díaz, C.; Del Barrio, J.L.; Estrada, J.M.; Gil, Á. Are healthcare workers’ intentions to vaccinate related to their knowledge, beliefs and attitudes? A systematic review. BMC Public Health 2013, 13, 154. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, S.L.; Rupp, R.; Zimet, G.D.; Meza, H.M.; Loza, M.L.; Short, M.B.; Succop, P.A. Uptake of HPV Vaccine: Demographics, Sexual History and Values, Parenting Style, and Vaccine Attitudes. J. Adolesc. Health 2008, 43, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.R.; Nichol, K.L.; Lipczynski, K. Barriers to Adult Immunization. Am. J. Med. 2008, 121, S28–S35. [Google Scholar] [CrossRef]
- Dubé, È.; Ward, J.K.; Verger, P.; MacDonald, N.E. Vaccine Hesitancy, Acceptance, and Anti-Vaccination: Trends and Future Prospects for Public Health. Annu. Rev. Public Health 2021, 42, 175–191. [Google Scholar] [CrossRef]
- Wicker, S.; Maltezou, H.C. Vaccine-preventable diseases in Europe: Where do we stand? Expert Rev. Vaccines 2014, 13, 979–987. [Google Scholar] [CrossRef]
- Parent du Châtelet, I.; Floret, D.; Antona, D.; Lévy-Bruhl, D. Measles resurgence in France in 2008, a preliminary report. Eurosurveillance 2009, 14, 19118. [Google Scholar] [CrossRef]
- Sallam, M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef]
- Qayum, I. Top ten global health threats for 2019: The WHO list. J. Rehman Med. Inst. 2019, 5, 1–2. [Google Scholar]
- de Figueiredo, A.; Simas, C.; Karafillakis, E.; Paterson, P.; Larson, H.J. Mapping global trends in vaccine confidence and investigating barriers to vaccine uptake: A large-scale retrospective temporal modelling study. Lancet 2020, 396, 898–908. [Google Scholar] [CrossRef] [PubMed]
- Opel, D.J.; Mangione-Smith, R.; Taylor, J.A.; Korfiatis, C.; Wiese, C.; Catz, S.; Martin, D.P. Development of a survey to identify vaccine-hesitant parents: The parent attitudes about childhood vaccines survey. Hum. Vaccines 2011, 7, 419–425. [Google Scholar] [CrossRef]
- Sabahelzain, M.M.; Dubé, E.; Moukhyer, M.; Larson, H.J.; van den Borne, B.; Bosma, H. Psychometric properties of the adapted measles vaccine hesitancy scale in Sudan. PLoS ONE 2020, 15, e0237171. [Google Scholar] [CrossRef]
- Martin, L.R.; Petrie, K.J. Understanding the Dimensions of Anti-Vaccination Attitudes: The Vaccination Attitudes Examination (VAX) Scale. Ann. Behav. Med. 2017, 51, 652–660. [Google Scholar] [CrossRef] [PubMed]
- Paredes, B.; Cárdaba, M.Á.; Cuesta, U.; Martinez, L. Validity of the Spanish Version of the Vaccination Attitudes Examination Scale. Vaccines 2021, 9, 1237. [Google Scholar] [CrossRef] [PubMed]
- Wood, L.; Smith, M.; Miller, C.B.; O’Carroll, R.E. The Internal Consistency and Validity of the Vaccination Attitudes Examination Scale: A Replication Study. Ann. Behav. Med. 2019, 53, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Paul, E.; Steptoe, A.; Fancourt, D. Attitudes towards vaccines and intention to vaccinate against COVID-19: Implications for public health communications. Lancet Reg. Health Eur. 2021, 1, 100012. [Google Scholar] [CrossRef]
- Yildiz, E.; Gungormus, Z.; Dayapglu, N. Assessment of Validity and Reliability of the Turkish Version of the Vaccination Attitudes Examination (VAX) Scale. Int. J. Caring Sci. 2021, 14, 261–268. [Google Scholar]
- Huza, G. The Psychometric Properties of a Romanian Version of the Vaccination Attitudes Examination (VAX) Scale. International. J. HIV/AIDS Prev. Educ. Behav. Sci. 2020, 6, 25. [Google Scholar] [CrossRef]
- Badenes-Ribera, L.; Silver, N.C.; Pedroli, E. Editorial: Scale Development and Score Validation. Front. Psychol. 2020, 11, 799. [Google Scholar] [CrossRef]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 6th ed.; international ed.; Pearson: London, UK, 2013. [Google Scholar]
- Beaton, D.E.; Bombardier, C.; Guillemin, F.; Ferraz, M.B. Guidelines for the Process of Cross-Cultural Adaptation of Self-Report Measures. Spine 2000, 25, 3186–3191. [Google Scholar] [CrossRef]
- Johns, R. One Size Doesn’t Fit All: Selecting Response Scales For Attitude Items. J. Elect. Public Opin. Parties 2005, 15, 237–264. [Google Scholar] [CrossRef]
- Taherdoost, H. What Is the Best Response Scale for Survey and Questionnaire Design; Review of Different Lengths of Rating Scale/Attitude Scale/Likert Scale. Int. J. Acad. Res. Manag. 2019, 8, 1–10. [Google Scholar]
- Shapiro, G.K.; Holding, A.; Perez, S.; Amsel, R.; Rosberger, Z. Validation of the vaccine conspiracy beliefs scale. Papillomavirus Res. 2016, 2, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Fall, E.; Gauchet, A.; Izaute, M.; Horne, R.; Chakroun, N. Validation of the French version of the Beliefs about Medicines Questionnaire (BMQ) among diabetes and HIV patients. Eur. Rev. Appl. Psychol. 2014, 64, 335–343. [Google Scholar] [CrossRef]
- Olarewaju, V.O.; Jafflin, K.; Deml, M.J.; Zimmermann, C.; Sonderegger, J.; Preda, T.; Staub, H.; Kwiatkowski, M.; Kloetzer, A.; Huber, B.M.; et al. Application of the Parent Attitudes about Childhood Vaccines (PACV) survey in three national languages in Switzerland: Exploratory factor analysis and Mokken scale analysis. Hum. Vaccines Immunother. 2021, 17, 2652–2660. [Google Scholar] [CrossRef] [PubMed]
- Chandler, J.; Sisso, I.; Shapiro, D. Participant carelessness and fraud: Consequences for clinical research and potential solutions. J. Abnorm. Psychol. 2020, 129, 49–55. [Google Scholar] [CrossRef]
- Curran, P.G. Methods for the detection of carelessly invalid responses in survey data. J. Exp. Soc. Psychol. 2016, 66, 4–19. [Google Scholar] [CrossRef]
- Field, A. Discovering Statistics Using IBM SPSS Statistics, 5th ed.; SAGE Publications: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- Costello, A.B.; Osborne, J. Best practices in exploratory factor analysis: Four recommendations for getting the most from your analysis. Pract. Assess. Res. Eval. 2015, 10, 7. [Google Scholar] [CrossRef]
- Horn, J.L. A rationale and test for the number of factors in factor analysis. Psychometrika 1965, 30, 179–185. [Google Scholar] [CrossRef]
- Kaiser, H.F. The Application of Electronic Computers to Factor Analysis. Educ. Psychol. Meas. 1960, 20, 141–151. [Google Scholar] [CrossRef]
- Navarro, D.J.; Foxcroft, D.R. Learning Statistics with Jamovi: A Tutorial for Psychology Students and Other Beginners; OSF: Peoria, IL, USA, 2018. [Google Scholar] [CrossRef]
- Schermelleh-Engel, K.; Moosbrugger, H.; Müller, H. Evaluating the Fit of Structural Equation Models: Tests of Significance and Descriptive Goodness-of-Fit Measures. Methods Psychol. Res. 2003, 8, 23–74. [Google Scholar]
- McDonald, R.P. Test Theory A Unified Treatment; Taylor and Francis: Oxfordshire, UK, 2013. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: New York, NY, USA, 1988; Available online: https://www.taylorfrancis.com/books/mono/10.4324/9780203771587/statistical-power-analysis-behavioral-sciences-jacob-cohen (accessed on 1 July 1988).
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Schwarzinger, M.; Watson, V.; Arwidson, P.; Alla, F.; Luchini, S. COVID-19 vaccine hesitancy in a representative working-age population in France: A survey experiment based on vaccine characteristics. Lancet Public Health 2021, 6, e210–e221. [Google Scholar] [CrossRef] [PubMed]
- Troiano, G.; Nardi, A. Vaccine hesitancy in the era of COVID-19. Public Health 2021, 194, 245–251. [Google Scholar] [CrossRef]
- Prickett, K.C.; Habibi, H.; Carr, P.A. COVID-19 Vaccine Hesitancy and Acceptance in a Cohort of Diverse New Zealanders. Lancet Reg. Health West. Pac. 2021, 14, 100241. [Google Scholar] [CrossRef]
- Pivetti, M.; Melotti, G.; Bonomo, M.; Hakoköngäs, E. Conspiracy Beliefs and Acceptance of COVID-Vaccine: An Exploratory Study in Italy. Soc. Sci. 2021, 10, 108. [Google Scholar] [CrossRef]
- Ball, H.L. Conducting Online Surveys. J. Hum. Lact. 2019, 35, 413417. [Google Scholar] [CrossRef]
- Bethlehem, J. Selection Bias in Web Surveys: Selection Bias in Web Surveys. Int. Stat. Rev. 2010, 78, 161188. [Google Scholar] [CrossRef]
- Suarez-Balcazar, Y.; Balcazar, F.E.; Taylor-Ritzler, T. Using the Internet to conduct research with culturally diverse populations: Challenges and opportunities. Cult. Divers. Ethn. Minor. Psychol. 2009, 15, 96104. [Google Scholar] [CrossRef]
- Wellman, B. The Three Ages of Internet Studies: Ten, Five and Zero Years Ago. N. Media Soc. 2004, 6, 123129. [Google Scholar] [CrossRef]
- Smith, G. Does Gender Influence Online Survey Participation?: A Record-Linkage Analysis of University Faculty Online Survey Response Behavior; ED 501717; ERIC Document Reproduction Service: Chantilly, VI, USA, 2008. [Google Scholar]
- Kung, F.Y.H.; Kwok, N.; Brown, D.J. Are Attention Check Questions a Threat to Scale Validity?: Attention Checks and Scale Validity. Appl. Psychol. 2018, 67, 264283. [Google Scholar] [CrossRef]
- Meade, A.W.; Craig, S.B. Identifying careless responses in survey data. Psychol. Methods 2012, 17, 437455. [Google Scholar] [CrossRef] [PubMed]
- Jabrayilov, R.; Emons, W.H.M.; Sijtsma, K. Comparison of Classical Test Theory and Item Response Theory in Individual Change Assessment. Appl. Psychol. Meas. 2016, 40, 559572. [Google Scholar] [CrossRef]
- Brouwer, D.; Meijer, R.R.; Zevalkink, J. Measuring individual significant change on the Beck Depression Inventory-II through IRT-based statistics. Psychother. Res. 2013, 23, 489501. [Google Scholar] [CrossRef] [PubMed]
- Sébille, V.; Hardouin, J.-B.; Le Néel, T.; Kubis, G.; Boyer, F.; Guillemin, F.; Falissard, B. Methodological issues regarding power of classical test theory (CTT) and item response theory (IRT)-based approaches for the comparison of patient-reported outcomes in two groups of patients—A simulation study. BMC Med. Res. Methodol. 2010, 10, 24. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Total Sample (n = 450) | Sub-Sample 1 (n = 225) | Sub-Sample 2 (n = 225) | |
|---|---|---|---|
| Experimental modality | - | - | - |
| Qualtrics | 72% | 71% | 72% |
| Paper | 28% | 29% | 28% |
| Demographics | - | - | - |
| Age, years | 32.92 ± 14.16 [18–81] | 33.46 ± 14.64 [18–80] | 32.38 ± 13.66 [18–81] |
| Female | 75% | 74% | 76% |
| Years of scholarship | 15.05 ± 2.28 [9–22] | 15.07 ± 2.28 [9–20] | 15.04 ± 2.29 [9–22] |
| Occupational status | - | - | - |
| Working | 52% | 53% | 51% |
| Student | 35% | 33% | 38% |
| Retired | 6% | 7% | 4% |
| Unemployed | 6% | 6% | 6% |
| Disabled worker or unemployed with disabled status | 1% | 1% | 1% |
| Family life | - | - | - |
| Have at least one child | 29% | 32% | 27% |
| Health | - | - | - |
| Have a chronic disease | 20% | 21% | 18% |
| Take a treatment | 20% | 23% | 18% |
| Past vaccination behaviours | - | - | - |
| Influenza vaccination | - | - | - |
| Yes | 11% | 14% | 8% |
| No | 89% | 86% | 92% |
| COVID-19 vaccination | - | - | - |
| Yes | 77% | 76% | 78% |
| No | 23% | 24% | 22% |
| Vaccination intentions | - | - | - |
| Influenza vaccination | - | - | - |
| Yes | 8% | 9% | 6% |
| No | 72% | 70% | 74% |
| Maybe | 16% | 16% | 16% |
| Already done | 4% | 5% | 4% |
| COVID-19 vaccination | - | - | - |
| Yes | 28% | 29% | 28% |
| No | 17% | 17% | 17% |
| Maybe | 12% | 13% | 10% |
| Already done | 43% | 41% | 45% |
| Items | Mean ± SD | Factor 1 | Factor 2 | Factor 3 | Factor 4 |
|---|---|---|---|---|---|
| 1 | 2.50 ± 1.19 | 0.03 | −0.90 | −0.03 | 0.06 |
| 2 | 1.85 ± 1.01 | 0.19 | −0.52 | 0.18 | −0.12 |
| 3 | 2.35 ± 1.17 | −0.07 | −1.00 | −0.02 | 0.02 |
| 4 | 3.65 ± 1.14 | −0.03 | −0.01 | −0.01 | 0.86 |
| 5 | 3.14 ± 1.18 | 0.19 | −0.05 | 0.26 | 0.46 |
| 6 | 2.70 ± 1.37 | 0.35 | −0.18 | 0.11 | 0.32 |
| 7 | 2.29 ± 1.29 | 0.79 | −0.01 | 0.04 | 0.02 |
| 8 | 2.23 ± 1.36 | 0.95 | −0.002 | −0.11 | 0.04 |
| 9 | 1.79 ± 1.22 | 0.79 | −0.04 | 0.15 | −0.08 |
| 10 | 2.88 ± 1.21 | −0.002 | −0.02 | 0.73 | −0.01 |
| 11 | 2.59 ± 1.34 | −0.03 | −0.05 | 0.86 | 0.01 |
| 12 | 2.31 ± 1.26 | 0.04 | −0.04 | 0.83 | 0.05 |
| % of variance | 55.41 | 9.73 | 8.09 | 7 |
| Mean ± SD [Min–Max] | |
|---|---|
| Vaccination Attitudes Examination Scale α | - |
| Total | 30.68 ± 11.01 [12–60] |
| Mistrust of vaccine benefits | 6.89 ± 3.22 [3–15] |
| Worries about unforeseen future effects | 9.64 ± 3.11 [3–15] |
| Concerns about commercial profiteering | 6.42 ± 3.47 [3–15] |
| Preference for natural immunity | 7.72 ± 3.39 [3–15] |
| Vaccine Conspiracy Belief Scale α | 2.88 ± 1.40 [1–7] |
| Parent Attitudes about Childhood Vaccines Survey β | 9.24 ± 7.93 [0–26] |
| Beliefs about Medicines Questionnaire | - |
| Specific δ | - |
| Perceived necessity for a prescribed treatment | 10.7 ± 3.93 [5–25] |
| Concerns about negative effects | 17.9 ± 4.19 [8–25] |
| General α | - |
| Beliefs about prescribe medicines | 12 ± 3.48 [4–20] |
| Perceived negative effects of treatment | 15.13 ± 3.23 [4–20] |
| Vaccination Attitudes Examination Scale α | |||||
|---|---|---|---|---|---|
| Total | Mistrust of Vaccine Benefit | Worries about Unforeseen Future Effects | Concerns about Commercial Profiteering | Preference for Natural Immunity | |
| Vaccine Conspiracy Belief Scale α | 0.84 ** | 0.71 ** | 0.63 ** | 0.78 ** | −0.68 ** |
| Parent Attitudes about Childhood Vaccines Survey β | 0.84 ** | 0.66 ** | 0.73 ** | 0.78 ** | −0.73 ** |
| Beliefs about Medicines Questionnaire | - | - | - | - | - |
| Specific δ | - | - | - | - | - |
| Perceived necessity for a prescribed treatment | 0.32 ** | −0.23 | −0.27 * | −0.33 ** | −0.28 * |
| Concerns about its negative effects | −0.46 ** | −0.35 * | −0.40 ** | −0.40 ** | −0.42 ** |
| General α | - | - | - | - | - |
| Beliefs about prescribe medicines | 0.58 ** | −0.47 ** | −0.43 ** | −0.54 ** | −0.49 ** |
| Perceived negative effects of treatment | −0.54 ** | −0.41 ** | −0.39 ** | −0.53 * | −0.46 ** |
| Mean ± Standard Deviation | ||
|---|---|---|
| Items | 1st Administration Mean ± SD | 2nd Administration Mean ± SD |
| 1 | 2.40 ± 1.15 | 2.34 ± 1.1 |
| 2 | 1.83 ± 1.01 | 1.79 ± 0.91 |
| 3 | 2.31 ± 1.09 | 2.29 ± 1.02 |
| 4 | 3.47 ± 1.19 | 3.62 ± 1.13 |
| 5 | 3.07 ± 1.11 | 3.04 ± 1.11 |
| 6 | 2.53 ± 1.37 | 2.62 ± 1.29 |
| 7 | 2.24 ± 1.25 | 2.12 ± 1.18 |
| 8 | 2.01 ± 1.29 | 2.12 ± 1.24 |
| 9 | 1.59 ± 1.06 | 1.64 ± 1.08 |
| 10 | 2.62 ± 1.18 | 2.65 ± 1.24 |
| 11 | 2.31 ± 1.25 | 2.36 ± 1.21 |
| 12 | 2.05 ± 1.15 | 2.04 ± 1.16 |
| Total VAX score | 28.45 ± 10.36 | 28.54 ± 10.24 |
| Mistrust of vaccine benefits | 6.54 ± 2.98 | 6.41 ± 2.68 |
| Worries about unforeseen future effects | 9.09 ± 3.10 | 9.28 ± 2.95 |
| Concerns about commercial profiteering | 5.84 ± 3.25 | 5.87 ± 3.15 |
| Preference for natural immunity | 6.97 ± 3.17 | 6.97 ± 3.25 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Eisenblaetter, M.; Madiouni, C.; Laraki, Y.; Capdevielle, D.; Raffard, S. Adaptation and Validation of a French Version of the Vaccination Attitudes Examination (VAX) Scale. Vaccines 2023, 11, 1001. https://doi.org/10.3390/vaccines11051001
Eisenblaetter M, Madiouni C, Laraki Y, Capdevielle D, Raffard S. Adaptation and Validation of a French Version of the Vaccination Attitudes Examination (VAX) Scale. Vaccines. 2023; 11(5):1001. https://doi.org/10.3390/vaccines11051001
Chicago/Turabian StyleEisenblaetter, Margot, Clarisse Madiouni, Yasmine Laraki, Delphine Capdevielle, and Stéphane Raffard. 2023. "Adaptation and Validation of a French Version of the Vaccination Attitudes Examination (VAX) Scale" Vaccines 11, no. 5: 1001. https://doi.org/10.3390/vaccines11051001