

Determinants Influenced by COVID-19 Vaccine: Employing the Health Action Process Approach and the Belief in Conspiracy Theories


Abstract
:1. Introduction
2. Theoretical Background
2.1. HAPA Model
2.2. Belief in Conspiracy Theories and COVID-19 Vaccination
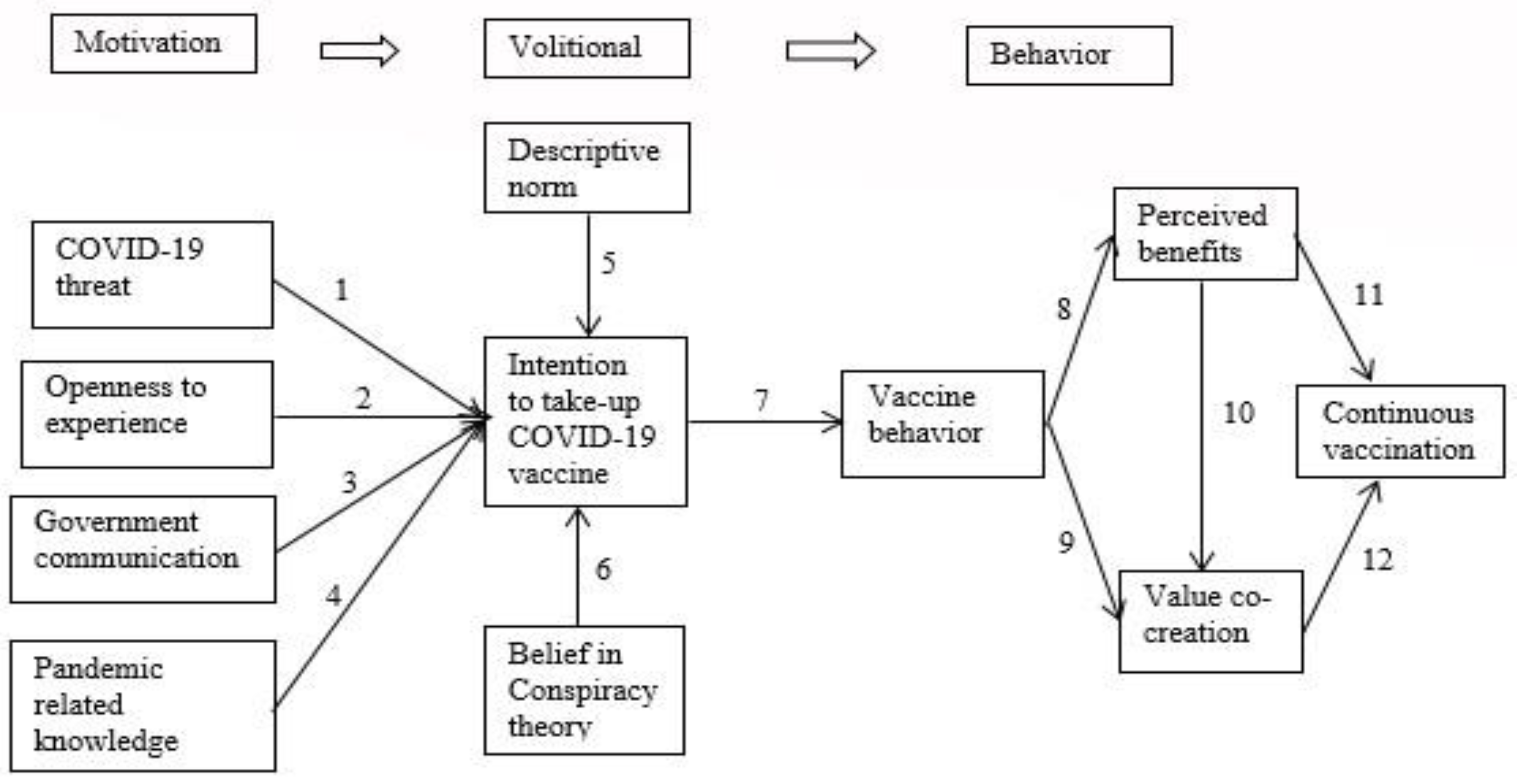
3. Hypotheses Development
4. Materials and Methods
4.1. Designing Measurements and Surveys
4.2. The Delphi Method
4.3. IRR Index
4.4. Data Collection
4.5. Sampling Distribution
4.6. Data Investigation
4.7. IRB
5. Results
5.1. Demographic Data
5.2. Reliability and Convergent Validity
5.3. Convergent Validity
5.4. Discriminant Validity
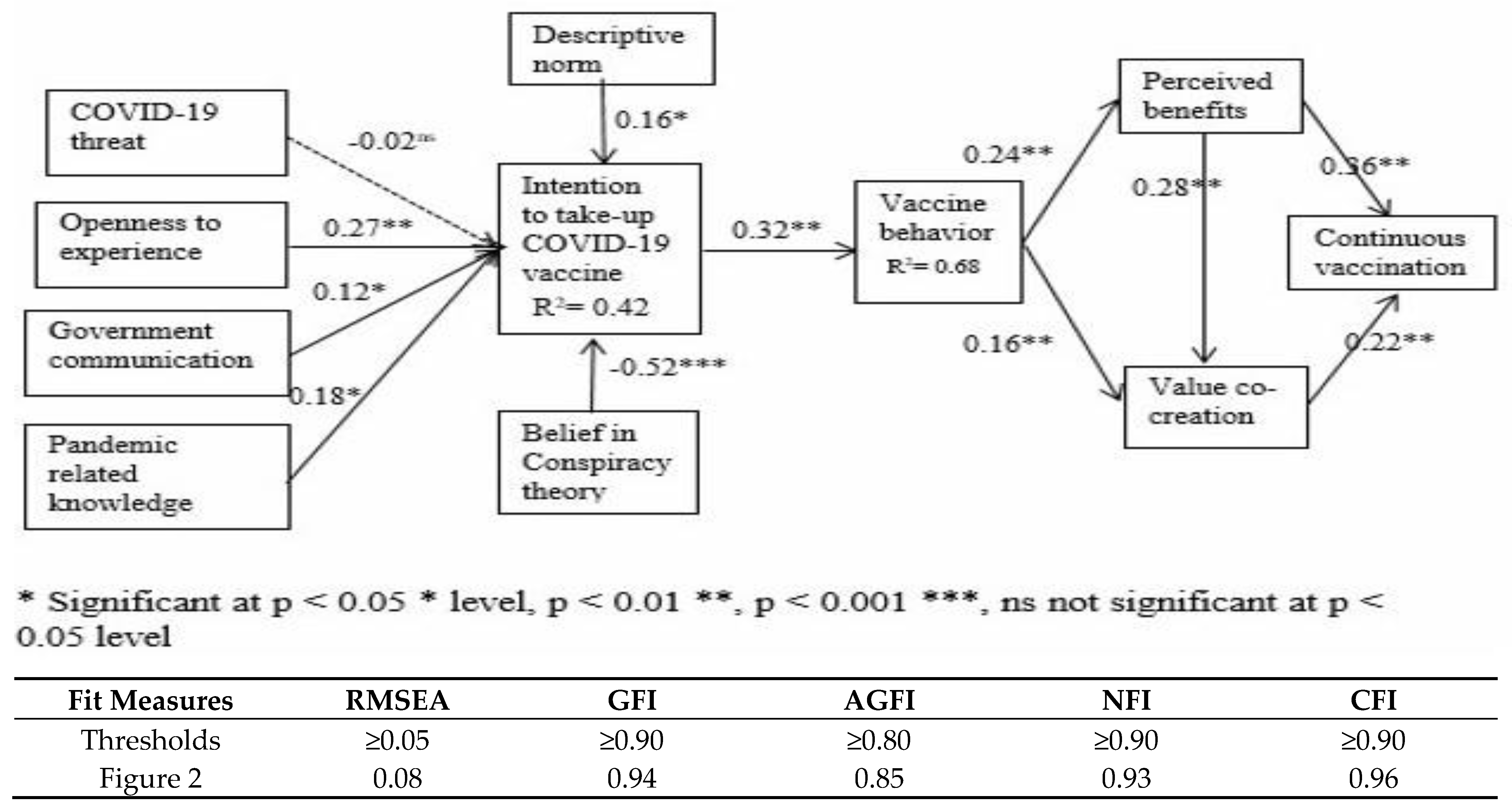
5.5. Tests of the Structural Model
5.6. The Structural Model’s Tests
6. Discussion and Implications
7. Limitations and Future Study
8. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kumar, A.; Singh, R.; Kaur, J.; Pandey, S.; Sharma, V.; Thakur, L.; Sati, S.; Mani, S.; Asthana, S.; Sharma, T.K.; et al. Wuhan to World: The COVID-19 Pandemic. Front. Cell. Infect. Microbiol. 2021, 11, 596201. [Google Scholar] [CrossRef]
- WHO. Coronavirus Disease (COVID-19) Pandemic. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019?gclid=EAIaIQobChMI7dXri7j36gIVWCUrCh2lLg2TEAAYASAAEgKwIvD_BwE (accessed on 22 April 2022).
- Onyeaka, H.; Anumudu, C.K.; Al-Sharify, Z.T.; Egele-Godswill, E.; Mbaegbu, P. COVID-19 pandemic: A review of the global lockdown and its far-reaching effects. Sci. Prog. 2021, 104, 1–18. [Google Scholar] [CrossRef]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 22 April 2022).
- Suthar, A.B.; Wang, J.; Seffren, V.; Wiegand, R.E.; Griffing, S.; Zel, E. Public health impact of covid-19 vaccines in the United States: Observational study. BMJ 2022, 377, e069317. [Google Scholar] [CrossRef]
- Hall, V.J.; Foulkes, S.; Saei, A.; Andrews, N.; Oguti, B.; Charlett, A.; Wellington, E.; Stowe, J.; Gillson, N.; Atti, A.; et al. SIREN Study Group. COVID-19 vaccine coverage in health-care workers in England and effectiveness of BNT162b2 mRNA vaccine against infection (SIREN): A prospective, multicentre, cohort study. Lancet 2021, 397, 1725–1735. [Google Scholar] [CrossRef] [PubMed]
- Ung, C.O.L.; Hu, Y.; Hu, H.; Bian, Y. Investigating the intention to receive the COVID-19 vaccination in Macao: Implications for vaccination strategies. BMC Infect. Dis. 2022, 22, 218. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Marks, F.; Clemens, J.D. Looking beyond COVID-19 vaccine phase 3 trials. Nat. Med. 2021, 27, 205–211. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Lists Additional COVID-19 Vaccine for Emergency Use and Issues Interim Policy Recommendations. 2021. Available online: https://www.who.int/news/item/07-05-2021-who-lists-additional-covid-19-vaccine-for-emergency-use-and-issues-interim-policy-recommendations (accessed on 26 April 2022).
- Dinleyici, E.C.; Borrow, R.; Safadi, M.A.P.; van Damme, P.; Munoz, F. M Vaccines and routine immunization strategies during the COVID-19 Pandemic. Hum. Vaccines Immunother. 2021, 17, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Al-Qerem, W.A.; Jarab, A.S. COVID-19 vaccination acceptance and its associated factors among a Middle Eastern population. Front. Public Health 2021, 9, 632914. [Google Scholar] [CrossRef] [PubMed]
- Kwok, K.O.; Li, K.K.; Wei, W.I.; Tang, A.; Wong, S.Y.S.; Lee, S.S. Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: A survey. Int. J. Nurs. Stud. 2021, 114, 103854. [Google Scholar] [CrossRef]
- Pertwee, E.; Simas, C.; Larson, H.J. An epidemic of uncertainty: Rumors, conspiracy theories and vaccine hesitancy. Nat. Med. 2022, 28, 456–459. [Google Scholar] [CrossRef]
- Zhu, W.; Zou, H.; Song, Y.; Ren, L.; Xu, Y. Understanding the continuous vaccination of the COVID-19 vaccine: An empirical study from China. Hum. Vaccines Immunother. 2021, 17, 4954–4963. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Qu, S.; Fang, Y.; Ip, M.; Wang, Z. Behavioral intention to perform risk compensation behaviors after receiving HPV vaccination among men who have sex with men in China. Hum. Vaccines Immunother. 2019, 15, 1737–1744. [Google Scholar] [CrossRef]
- Hamilton, K.; Smith, S.R.; Keech, J.J.; Moyers, S.A.; Hagger, M.S. Application of the health action process approach to social distancing behavior during covid-19. Appl. Psychol.-Health Well Being 2020, 12, 1244–1269. [Google Scholar] [CrossRef] [PubMed]
- Akther, T.; Nur, T. A model of factors influencing COVID-19 vaccine acceptance: A synthesis of the theory of reasoned action, conspiracy theory belief, awareness, perceived usefulness, and perceived ease of use. PLoS ONE 2022, 17, e0261869. [Google Scholar] [CrossRef]
- Seddig, D.; Maskileyson, D.; Davidov, E.; Ajzen, I.; Schmidt, P. Correlates of COVID-19 vaccination intentions: Attitudes, institutional trust, fear, conspiracy beliefs, and vaccine skepticism. Soc. Sci. Med. 2022, 302, 114981. [Google Scholar] [CrossRef]
- Xin, M.; Luo, S.; She, R.; Yu, Y.; Li, L.; Wang, S.; Ma, L.; Tao, F.; Zhang, J.; Zhao, J.; et al. Negative cognitive and psychological correlates of mandatory quarantine during the initial COVID-19 outbreak in China. Am. Psychol. 2020, 75, 607–617. [Google Scholar] [CrossRef]
- Villani, L.; Pastorino, R.; Molinari, E.; Anelli, F.; Ricciardi, W.; Graffigna, G.; Boccia, S. Impact of the COVID-19 Pandemic on psychological well-being of students in an Italian university: A web-based cross-sectional survey. Glob. Health 2021, 17, 39. [Google Scholar] [CrossRef]
- Duan, L.; Zhu, G. Psychological interventions for people affected by the COVID-19 epidemic. Lancet Psychiatry 2020, 7, 300–302. [Google Scholar] [CrossRef]
- Frazier, P.; Gabriel, A.; Merians, A.; Lust, K. Understanding stress as an impediment to academic performance. J. Am. Coll. Health 2019, 67, 562–570. [Google Scholar] [CrossRef]
- Rogers, E.M. Diffusion of Innovations, 5th ed.; Free Press: New York, NY, USA, 2003. [Google Scholar]
- Patterson, F.; Zibarras, L.D. Selecting for creativity and innovation potential: Implications for practice in healthcare education. Adv. Health Sci. Educ. Theory Pract. 2017, 22, 417–428. [Google Scholar] [CrossRef]
- Skavronskaya, L.; Moyle, B.; Scott, N. The Experience of Novelty and the Novelty of Experience. Front. Psychol. 2020, 11, 322. [Google Scholar] [CrossRef]
- Su, L.; Du, J.; Du, Z. Government Communication, Perceptions of COVID-19, and Vaccination Intention: A Multi-Group Comparison in China. Front. Psychol. 2022, 12, 783374. [Google Scholar] [CrossRef] [PubMed]
- Duan, T.; Jiang, H.; Deng, X.; Zhang, Q.; Wang, F. Government Intervention, Risk Perception, and the Adoption of Protective Action Recommendations: Evidence from the COVID-19 Prevention and Control Experience of China. Int. J. Environ. Res. Public Health 2020, 17, 3387. [Google Scholar] [CrossRef] [PubMed]
- Gabryelczyk, R. Has COVID-19 Accelerated Digital Transformation? Initial Lessons Learned for Public Administrations. Inf. Syst. Manag. 2020, 37, 303–309. [Google Scholar] [CrossRef]
- Aldalaykeh, M.; Al-Hammouri, M.M.; Rababah, J.; Al-Dwaikat, T. COVID-19 Help-Seeking Behaviors: Application of the Theory of Planned Behavior. Psychol. Belg. 2021, 61, 391–400. [Google Scholar] [CrossRef]
- Aerts, C.; Revilla, M.; Duval, L.; Paaijmans, K.; Chandrabose, J.; Cox, H.; Sicuri, E. Understanding the role of disease knowledge and risk perception in shaping preventive behavior for selected vectorborne diseases in Guyana. PLoS Negl. Trop. Dis. 2020, 14, e0008149. [Google Scholar] [CrossRef] [Green Version]
- Sherman, S.M.; Smith, L.E.; Sim, J.; Amlôt, R.; Cutts, M.; Dasch, H.; Rubin, G.J.; Sevdalis, N. COVID-19 vaccination intention in the UK: Results from the COVID-19 vaccination acceptability study (CoVAccS), a nationally representative cross-sectional survey. Hum. Vaccines Immunother. 2020, 17, 1612–1621. [Google Scholar] [CrossRef]
- Graupensperger, S.; Abdallah, D.A.; Lee, C.M. Social norms and vaccine uptake: College students’ COVID vaccination intentions, attitudes, and estimated peer norms and comparisons with influenza vaccine. Vaccine 2021, 39, 2060–2067. [Google Scholar] [CrossRef]
- Graupensperger, S.; Lee, C.; Larimer, M. Young adults underestimate how well peers adhere to COVID-19 preventive behavioral guidelines. J. Prim. Prev. 2021. ahead of print. [Google Scholar] [CrossRef]
- Dutta, B.; Peng, M.-H.; Sun, S.-L. Modeling the adoption of personal health record (PHR) among individual: The effect of health-care technology self-efficacy and gender concern. Libyan J. Med. 2018, 13, 1500349. [Google Scholar] [CrossRef] [Green Version]
- Dutta, B.; Hwang, H.G. The adoption of electronic medical record by physicians: A PRISMA-compliant systematic review. Medicine 2020, 99, e19290. [Google Scholar] [CrossRef]
- Bhatti, W.A.; Glowik, M.; Arslan, A. Knowledge sharing motives and value cocreation behavior of the consumers in physiotherapy services: A cross-cultural study. J. Knowl. Manag. 2020, 25, 1128–1145. [Google Scholar] [CrossRef]
- Kuo, C.-S.; Hsu, C.-C. Continuance Intention to Use and Perceived Net Benefits as Perceived by Streaming Platform Users: An Application of the Updated IS Success. Model. Behav. Sci. 2022, 12, 124. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Li, D. What motivates audience comments on live streaming platforms? PLoS ONE 2020, 15, e0231255. [Google Scholar] [CrossRef] [Green Version]
- Caputo, F.; Garcia-Perez, A.; Cillo, V.; Giacosa, E. A knowledge-based view of people and technology: Directions for a value co-creation-based learning organization. J. Knowl. Manag. 2019, 23, 1314–1334. [Google Scholar] [CrossRef] [Green Version]
- Kamali, M.; Zarea, H.; Su, Z.; Soltani, S. The influence of value cocreation on customer loyalty, behavioural intention, and customer satisfaction in emerging markets. AD-Minister 2021, 39, 5–24. [Google Scholar] [CrossRef]
- Al-kumaim, N.H.; Alhazmi, A.K.; Ramayah, T.; Shabbir, M.S.; Gazem, N.A. Sustaining Continuous Engagement in Value Co-creation Among Individuals in Universities Using Online Platforms: Role of Knowledge Self-Efficacy, Commitment and Perceived Benefits. Front. Psychol. 2021, 12, 637808. [Google Scholar] [CrossRef]
- Hair, J.F.; Anderson, R.E.; Tatham, R.L.; William, B. Multivariate Data Analysis, 5th ed.; Prentice Hall: Upper Saddle River, NJ, USA, 1998. [Google Scholar]
- Barbounak, S.G.; Gourounti, K.; Sarantaki, A. Advances of Sentiment Analysis Applications in Obstetrics/Gynecology and Midwifery. Mater. Socio-Med. 2021, 33, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.L. Statistical Analysis and Practice of Questionnaire-SPSS Operation and Application; Chongqing University Press: Chongqing, China, 2010; pp. 100–125. [Google Scholar]
- Busetto, L.; Wick, W.; Gumbinger, G. How to use and assess qualitative research methods. Neurol. Res. Pr. 2020, 2, 14. [Google Scholar] [CrossRef] [PubMed]
- Nduneseokwu, C.K.; Qu, Y.; Appolloni, A. Factors Influencing Consumers’ Intentions to Participate in a Formal E-Waste Collection System: A Case Study of Onitsha, Nigeria. Sustainability 2017, 9, 881. [Google Scholar] [CrossRef] [Green Version]
- Anderson, J.C.; Gerbing, D.W. Structural equation modeling in practice: A review and recommended two step approach. Psychol. Bull. 1998, 103, 411–423. [Google Scholar] [CrossRef]
- Taiwan Demographics. Available online: https://www.worldometers.info/demographics/taiwan-demographics/ (accessed on 28 April 2022).
- Bagozzi, R.P.; Yi, Y. On the evaluation of structural equation models. J. Acad. Marking Sci. 1988, 16, 74–94. [Google Scholar] [CrossRef]
- Fornell, C.; Larcker, D.F. Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Taiwan Centers for Disease Control. Available online: https://www.cdc.gov.tw/En/Category/NewsPage/tov1jahKUv8RGSbvmzLwFg (accessed on 8 May 2022).



{kind=link}
{kind=link}
| Value | Asymp. Std. Error a | Approx. T b | Approx. Sig. | |
|---|---|---|---|---|
| Measure of Agreement Kappa | 0.718 | 0.088 | 7.992 | 0.000 |
| N valid for cases | 390 |
| Item | Option | Count | Percentage % |
|---|---|---|---|
| Gender | Male | 200 | 51.39 |
| Female | 190 | 48.61 | |
| Age | 18–29 | 149 | 38.33 |
| 30–39 | 103 | 26.39 | |
| 40–49 | 74 | 18.89 | |
| 50–59 | 40 | 10.28 | |
| ≥60 | 24 | 6.11 | |
| Education Level | Elementary/Junior high school | 13 | 3.33 |
| Senior high school | 28 | 7.22 | |
| College | 246 | 63.06 | |
| Master’s or above | 103 | 26.39 | |
| Living area in Taiwan | North | 134 | 34.36 |
| Central | 99 | 25.38 | |
| West | 12 | 3.07 | |
| South | 117 | 30.00 | |
| East | 28 | 7.19 |
| Construct | Cronbach’s Alpha | Composite Reliability (CR) | Average Variance Extracted |
|---|---|---|---|
| PT | 0.820 | 0.950 | 0.866 |
| OE | 0.823 | 0.981 | 0.891 |
| GC | 0.869 | 0.976 | 0.829 |
| PK | 0.867 | 0.968 | 0.911 |
| DN | 0.822 | 0.951 | 0.867 |
| BCT | 0.878 | 0.985 | 0.858 |
| INT | 0.805 | 0.938 | 0.874 |
| VB | 0.847 | 0.974 | 0.865 |
| PB | 0.884 | 0.942 | 0.862 |
| VC | 0.817 | 0.956 | 0.878 |
| CVN | 0.868 | 0.916 | 0.867 |
| PT | OE | GC | PK | DN | BCT | INT | VB | PB | VC | CVN | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| PT | 0.930 | ||||||||||
| OE | 0.679 ** | 0.943 | |||||||||
| GC | 0.521 ** | −0.16 ** | 0.910 | ||||||||
| PK | 0.543 * | −0.13 ** | 0.478 * | 0.954 | |||||||
| DN | 0.446 ** | −0.21 ** | 0.521 ** | 0.692 ** | 0.931 | ||||||
| BCT | 0.451 * | −0.27 ** | 0.442 ** | 0.541 * | 0.494 ** | 0.926 | |||||
| INT | 0.559 * | −0.25 ** | −0.12 ** | −0.14 ** | −0.10 ** | −0.18 ** | 0.934 | ||||
| VB | 0.479 * | −0.31 ** | 0.188 * | 0.186 ** | 0.378 * | 0.256 * | 0.478 * | 0.930 | |||
| PB | 0.364 ** | −0.33 ** | 0.194 ** | 0.126 ** | 0.218 * | 0.267 ** | 0.512 * | 0.468 * | 0.928 | ||
| VC | 0.261 ** | −0.17 ** | 0.218 ** | 0.154 ** | 0.312 ** | 0.186 ** | 0.342 ** | 0.278 ** | 0.352 ** | 0.937 | |
| CVN | 0.376 * | −0.41 ** | 0.234 * | 0.138 ** | 0.426 * | 0.242 * | 0.298 * | 0.126 ** | 0.156 ** | 0.286 ** | 0.931 |
| Hypothesis | Proposed Hypothesis Relationship | Path Coefficients | t-Statistics | Hypothesis Test Results |
|---|---|---|---|---|
| H1 | PT → INT | −0.02 | 1.127 | Rejected |
| H2 | OE → INT | 0.27 | 2.562 | Supported |
| H3 | GC → INT | 0.12 | 4.934 | Supported |
| H4 | PK → INT | 0.18 | 4.864 | Supported |
| H5 | DN → INT | 0.16 | 4.216 | Supported |
| H6 | BCT → INT | −0.52 | 4.825 | Supported |
| H7 | INT → VB | 0.32 | 2.956 | Supported |
| H8 | VB → PB | 0.24 | 2.341 | Supported |
| H9 | VB → VC | 0.16 | 2.162 | Supported |
| H10 | PB → VC | 0.28 | 2.786 | Supported |
| H11 | PB → CVN | 0.36 | 3.264 | Supported |
| H12 | PV → CVN | 0.22 | 2.452 | Supported |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dutta, B. Determinants Influenced by COVID-19 Vaccine: Employing the Health Action Process Approach and the Belief in Conspiracy Theories. Vaccines 2023, 11, 730. https://doi.org/10.3390/vaccines11040730
Dutta B. Determinants Influenced by COVID-19 Vaccine: Employing the Health Action Process Approach and the Belief in Conspiracy Theories. Vaccines. 2023; 11(4):730. https://doi.org/10.3390/vaccines11040730
Chicago/Turabian StyleDutta, Bireswar. 2023. "Determinants Influenced by COVID-19 Vaccine: Employing the Health Action Process Approach and the Belief in Conspiracy Theories" Vaccines 11, no. 4: 730. https://doi.org/10.3390/vaccines11040730