

Evaluation of the Approach towards Vaccination against COVID-19 among the Polish Population—In Relation to Sociodemographic Factors and Physical and Mental Health

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Explanatory Variables
2.3. Measures
2.4. Statistics
3. Results
3.1. Study Group
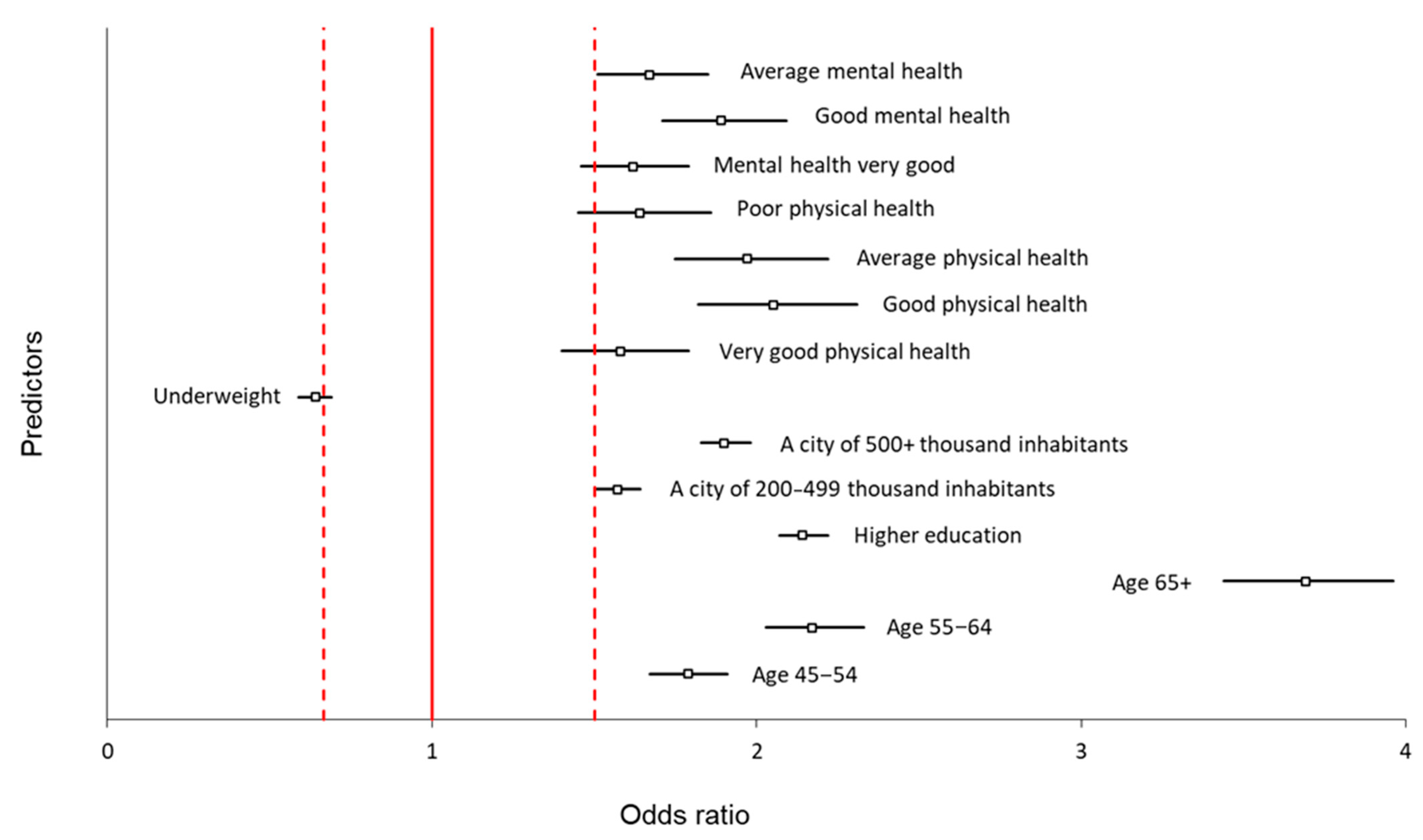
3.2. Predictors of a Positive Attitude toward COVID-19 Vaccination
3.3. Predictors of Negative Attitude toward COVID-19 Vaccination
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hopkins, J. COVID-19 Map—Johns Hopkins Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/map.html%0Ahttps://coronavirus.jhu.edu/data/mortality%0Ahttps://coronavirus.jhu.edu/map.html (accessed on 27 September 2022).
- WHO Director General’s Speeches. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 28 January 2023).
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Rahimmanesh, I.; Shariati, L.; Dana, N.; Esmaeili, Y.; Vaseghi, G.; Haghjooy Javanmard, S. Cancer Occurrence as the Upcoming Complications of COVID-19. Front. Mol. Biosci. 2022, 8, 1361. [Google Scholar] [CrossRef]
- Jdiaa, S.S.; Mansour, R.; El Alayli, A.; Gautam, A.; Thomas, P.; Mustafa, R.A. COVID–19 and chronic kidney disease: An updated overview of reviews. J. Nephrol. 2022, 35, 69–85. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Byrne, C.D.; Zheng, M.H.; Targher, G. Diabetes as a risk factor for greater COVID-19 severity and in-hospital death: A meta-analysis of observational studies. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 1236–1248. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Wu, Y.; He, Y.; Liu, X.; Liu, M.; Tang, Y.; Li, X.; Yang, G.; Liang, G.; Xu, S.; et al. Age-Related Risk Factors and Complications of Patients with COVID-19: A Population-Based Retrospective Study. Front. Med. 2022, 8, 757459. [Google Scholar] [CrossRef]
- Ayling, K.; Jia, R.; Coupland, C.; Chalder, T.; Massey, A.; Broadbent, E.; Vedhara, K. Psychological Predictors of Self-reported COVID-19 Outcomes: Results from a Prospective Cohort Study. Ann. Behav. Med. 2022, 56, 484–497. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, S.; Rathor, R.; Singh, S.; Kumar, B.; Suryakumar, G. Obesity: A Risk Factor for COVID-19. Adv. Exp. Med. Biol. 2021, 1352, 195–210. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.M.; Vegvari, C.; Truscott, J.; Collyer, B.S. Challenges in creating herd immunity to SARS-CoV-2 infection by mass vaccination. Lancet 2020, 396, 1614–1616. [Google Scholar] [CrossRef]
- WHO/Samuel Aranda WHO. Ten Threats to Global Health in 2019. Available online: https://www.who.int/emergencies/ten-threats-to-global-health-in-2019 (accessed on 28 January 2023).
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Poland: Attitude towards vaccine for coronavirus (COVID-19) 2021 | Statista. Available online: https://www.statista.com/statistics/1111564/poland-attitude-towards-vaccine-for-the-coronavirus-covid-19/ (accessed on 8 March 2023).
- Evans, R. European Centre for Disease Prevention and Control. Available online: https://vaccinetracker.ecdc.europa.eu/public/extensions/COVID-19/vaccine-tracker.html#uptake-tab (accessed on 28 January 2023).
- Ruszają szczepienia osób 70+. Ponad 60% Polaków jest na „tak”— Szczepienie przeciwko COVID-19—Portal Gov.pl. Available online: https://www.gov.pl/web/szczepimysie/ruszaja-szczepienia-osob-70-ponad-60-polakow-jest-na-tak (accessed on 8 March 2023).
- Sowa, P.; Kiszkiel, Ł.; Laskowski, P.P.; Alimowski, M.; Szczerbiński, Ł.; Paniczko, M.; Moniuszko-Malinowska, A.; Kamiński, K. Covid-19 vaccine hesitancy in poland—Multifactorial impact trajectories. Vaccines 2021, 9, 876. [Google Scholar] [CrossRef]
- Stasiuk, K.; Maciuszek, J.; Polak, M.; Doliński, D. Profiles of Vaccine Hesitancy: The Relation between Personal Experience with Vaccines, Attitude towards Mandatory Vaccination, and Support for Anti-Vaccine Arguments among Vaccine Hesitant Individuals. Soc. Psychol. Bull. 2021, 16, 1–20. [Google Scholar] [CrossRef]
- Walkowiak, M.P.; Walkowiak, D. Predictors of COVID-19 Vaccination Campaign Success: Lessons Learnt from the Pan-demic So Far. A Case Study from Poland. Vaccines 2021, 9, 1153. [Google Scholar] [CrossRef]
- Raciborski, F.; Samel-Kowalik, P.; Gujski, M.; Pinkas, J.; Arcimowicz, M.; Jankowski, M. Factors associated with a lack of willingness to vaccinate against covid-19 in poland: A 2021 nationwide cross-sectional survey. Vaccines 2021, 9, 1000. [Google Scholar] [CrossRef]
- Szychowska, A.; Zimny-Zając, A.; Dziankowska-Zaborszczyk, E.; Grodzicki, T.; Drygas, W.; Zdrojewski, T. Physical Activity versus Selected Health Behaviors, Subjective Physical and Psychological Health and Multimorbidity in a Large Cohort of Polish Seniors during the COVID-19 Pandemic (Results of the National Test for Poles’ Health). Int. J. Environ. Res. Public Health 2023, 20, 556. [Google Scholar] [CrossRef]
- Onet—Narodowy Test Zdrowia. Available online: https://narodowytestzdrowia.medonet.pl/ (accessed on 28 January 2023).
- Sallam, M. COVID-19 vaccine hesitancy worldwide: A concise systematic review of vaccine acceptance rates. Vaccines 2021, 9, 160. [Google Scholar] [CrossRef] [PubMed]
- Zanettini, C.; Omar, M.; Dinalankara, W.; Imada, E.L.; Colantuoni, E.; Parmigiani, G.; Marchionni, L. Influenza vaccination and covid-19 mortality in the usa: An ecological study. Vaccines 2021, 9, 427. [Google Scholar] [CrossRef]
- Kwok, K.O.; Li, K.K.; WEI, W.I.; Tang, A.; Wong, S.Y.S.; Lee, S.S. Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: A survey. Int. J. Nurs. Stud. 2021, 114, 103854. [Google Scholar] [CrossRef]
- AlHajri, B.; Alenezi, D.; Alfouzan, H.; Altamimi, S.; Alzalzalah, S.; Almansouri, W.; Alqudeimat, Y.; Almokhaizeem, Z.; Ziyab, A.H. Willingness of parents to vaccinate their children against influenza and the novel coronavirus disease-2019. J. Pediatr. 2021, 231, 298–299. [Google Scholar] [CrossRef]
- Goldman, R.D.; McGregor, S.; Marneni, S.R.; Katsuta, T.; Griffiths, M.A.; Hall, J.E.; Seiler, M.; Klein, E.J.; Cotanda, C.P.; Gelernter, R.; et al. Willingness to Vaccinate Children against Influenza after the Coronavirus Disease 2019 Pandemic. J. Pediatr. 2021, 228, 87–93.e2. [Google Scholar] [CrossRef]
- Zaprutko, T.; Kremin, Y.; Michalak, M.; Bernatoniene, J.; Zaprutko, L.; Hudz, N.; Stolecka, A.; Cynar, J.; Niewczas, K.; Sprawka, J.; et al. Social Attitude to COVID-19 and Influenza Vaccinations after the Influenza Vaccination Season and between the Second and Third COVID-19 Wave in Poland, Lithuania, and Ukraine. Int. J. Environ. Res. Public Health 2022, 19, 2042. [Google Scholar] [CrossRef] [PubMed]
- Del Riccio, M.; Lina, B.; Caini, S.; Staadegaard, L.; Wiegersma, S.; Kynčl, J.; Combadière, B.; MacIntyre, C.R.; Paget, J. Letter to the editor: Increase of influenza vaccination coverage rates during the COVID-19 pandemic and implications for the upcoming influenza season in northern hemisphere countries and Australia. Eurosurveillance 2021, 26, 2101143. [Google Scholar] [CrossRef]
- Raport: Sytuacja zdrowotna ludności Polski i jej uwarunkowania—NIZP PZH—PIB. Available online: https://www.pzh.gov.pl/raport-sytuacja-zdrowotna-ludnosci-polski-i-jej-uwarunkowania/ (accessed on 14 March 2023).
- Ministerio de Sanidad—Profesionales—Salud pública—Prevención de la salud—Vacunaciones—Programa vacunación—Coberturas de Vacunación. Dartos Estadísticos. Available online: https://www.sanidad.gob.es/profesionales/saludPublica/prevPromocion/vacunaciones/calendario-y-coberturas/coberturas/home.htm (accessed on 14 March 2023).
- Caserotti, M.; Girardi, P.; Rubaltelli, E.; Tasso, A.; Lotto, L.; Gavaruzzi, T. Associations of COVID-19 risk perception with vaccine hesitancy over time for Italian residents. Soc. Sci. Med. 2021, 272, 113688. [Google Scholar] [CrossRef]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef]
- Conlon, A.; Ashur, C.; Washer, L.; Eagle, K.A.; Hofmann Bowman, M.A. Impact of the influenza vaccine on COVID-19 infection rates and severity. Am. J. Infect. Control 2021, 49, 694–700. [Google Scholar] [CrossRef]
- Wang, K.; Wong, E.L.Y.; Ho, K.F.; Cheung, A.W.L.; Chan, E.Y.Y.; Yeoh, E.K.; Wong, S.Y.S. Intention of nurses to accept coronavirus disease 2019 vaccination and change of intention to accept seasonal influenza vaccination during the coronavirus disease 2019 pandemic: A cross-sectional survey. Vaccine 2020, 38, 7049–7056. [Google Scholar] [CrossRef]
- Nguyen, K.H.; Srivastav, A.; Razzaghi, H.; Williams, W.; Lindley, M.C.; Jorgensen, C.; Abad, N.; Singleton, J.A. COVID-19 vaccination intent, perceptions, and reasons for not vaccinating among groups prioritized for early vaccination—United States, September and December 2020. Am. J. Transplant. 2021, 21, 1650–1656. [Google Scholar] [CrossRef]
- Thomson, A.; Watson, M. Vaccine hesitancy: A vade mecum v1.0. Vaccine 2016, 34, 1989–1992. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rashid, H.; Yin, J.K.; Ward, K.; King, C.; Seale, H.; Booy, R. Assessing interventions to improve influenza vaccine uptake among health care workers. Health Aff. 2016, 35, 284–292. [Google Scholar] [CrossRef] [PubMed]
- Verger, P.; Scronias, D.; Dauby, N.; Adedzi, K.A.; Gobert, C.; Bergeat, M.; Gagneur, A.; Dubé, E. Attitudes of healthcare workers towards COVID-19 vaccination: A survey in France and French-speaking parts of Belgium and Canada, 2020. Eurosurveillance 2021, 26, 2002047. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of COVID-19 vaccination during the covid-19 pandemic in china. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef]
- Freeman, D.; Loe, B.S.; Chadwick, A.; Vaccari, C.; Waite, F.; Rosebrock, L.; Jenner, L.; Petit, A.; Lewandowsky, S.; Vanderslott, S.; et al. COVID-19 vaccine hesitancy in the UK: The Oxford coronavirus explanations, attitudes, and narratives survey (Oceans) II. Psychol. Med. 2022, 52, 3127–3141. [Google Scholar] [CrossRef] [PubMed]
- Bhartiya, S.; Kumar, N.; Singh, T.; Murugan, S.; Rajavel, S.; Wadhwani, M. Knowledge, attitude and practice towards COVID-19 vaccination acceptance in West India. Int. J. Community Med. Public Health 2021, 8, 1170–1176. [Google Scholar] [CrossRef]
- Hoque, A.M.; Buckus, S.; Hoque, M.; Hoque, M.E.; Van Hal, G. COVID-19 Vaccine Acceptability Among Pregnant Women at a Primary Health Care Facility in Durban, South Africa. Eur. J. Med. Health Sci. 2020, 2. [Google Scholar] [CrossRef]
- Kilic, M.; Ustundag Ocal, N.; Uslukilic, G. The relationship of Covid-19 vaccine attitude with life satisfaction, religious attitude and Covid-19 avoidance in Turkey. Hum. Vaccines Immunother. 2021, 17, 3384–3398. [Google Scholar] [CrossRef]
- Sherman, S.M.; Smith, L.E.; Sim, J.; Amlôt, R.; Cutts, M.; Dasch, H.; Rubin, G.J.; Sevdalis, N. COVID-19 vaccination intention in the UK: Results from the COVID-19 vaccination acceptability study (CoVAccS), a nationally representative cross-sectional survey. Hum. Vaccines Immunother. 2021, 17, 1612–1621. [Google Scholar] [CrossRef]
- Thorneloe, R.; Wilcockson, H.E.; Lamb, M.; Jordan, C.; Arden, M. Willingness to receive a COVID-19 vaccine among adults at high-risk of COVID-19: A UK-wide survey. Health Psychol. 2020, 18, 1–15. [Google Scholar]
- Al-Mohaithef, M.; Padhi, B.K. Determinants of covid-19 vaccine acceptance in saudi arabia: A web-based national survey. J. Multidiscip. Healthc. 2020, 13, 1657–1663. [Google Scholar] [CrossRef]
- Abebe, H.; Shitu, S.; Mose, A. Understanding of COVID-19 vaccine knowledge, attitude, acceptance, and determinates of COVID-19 vaccine acceptance among adult population in Ethiopia. Infect. Drug Resist. 2021, 14, 2015–2025. [Google Scholar] [CrossRef]
- Zintel, S.; Flock, C.; Arbogast, A.L.; Forster, A.; von Wagner, C.; Sieverding, M. Gender differences in the intention to get vaccinated against COVID-19: A systematic review and meta-analysis. J. Public Health 2022, 1–25. [Google Scholar] [CrossRef]
- Biswas, N.; Mustapha, T.; Khubchandani, J.; Price, J.H. The Nature and Extent of COVID-19 Vaccination Hesitancy in Healthcare Workers. J. Community Health 2021, 46, 1244–1251. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, L.C.; Soveri, A.; Lewandowsky, S.; Karlsson, L.; Karlsson, H.; Nolvi, S.; Karukivi, M.; Lindfelt, M.; Antfolk, J. Fearing the disease or the vaccine: The case of COVID-19. Pers. Individ. Dif. 2021, 172, 110590. [Google Scholar] [CrossRef] [PubMed]
- Harrison, E.A.; Wu, J.W. Vaccine confidence in the time of COVID-19. Eur. J. Epidemiol. 2020, 35, 325–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Feature (Variable) | n | Percentage |
|---|---|---|
| Gender | ||
| Men | 119,169 | 59.6% |
| Women | 80,831 | 40.4% |
| Age (years old) | ||
| 18–24 | 5011 | 2.5% |
| 25–34 | 19,005 | 9.5% |
| 35–44 | 36,333 | 18.2% |
| 45–54 | 43,265 | 21.6% |
| 55–64 | 43,624 | 21.8% |
| 65+ | 52,765 | 26.4% |
| Education | ||
| Primary | 27,154 | 13.6% |
| Secondary | 59,384 | 29.7% |
| Higher | 112,462 | 56.2% |
| Place of residence | ||
| Village | 44,232 | 22.1% |
| Town less than 19,000 inhabitants | 23,824 | 11.9% |
| Town between 20,000 to 49,000 inhabitants | 30,729 | 15.6% |
| Town between 50,000 to 99,000 inhabitants | 23,293 | 11.6% |
| Town between 100,000 to 199,000 inhabitants | 22,047 | 11.0% |
| Town between 200,000 to 499,000 inhabitants | 21,203 | 10.6% |
| Town more than 500,000 inhabitants | 34,672 | 17.4% |
| Region in Poland | ||
| South | 45,452 | 22.7% |
| Northwest | 32,348 | 16.2% |
| Southwest | 22,008 | 11.0% |
| North | 28,000 | 14.0% |
| Central | 17,817 | 8.9% |
| East | 22,866 | 11.4% |
| Masovian voivodeship | 31,508 | 15.7% |
| BMI | ||
| Underweight | 3408 | 1.7% |
| In norm | 68,471 | 34.2% |
| Overweight | 77,630 | 38.8% |
| Obesity | 50,489 | 25.2% |
| Physical health | ||
| Very good | 27,606 | 3.8% |
| Good | 80,417 | 40.2% |
| Normal | 76,259 | 38.2% |
| Bad | 14,285 | 7.1% |
| Very bad | 1433 | 0.7% |
| Mental health | ||
| Very good | 45,221 | 22.6% |
| Good | 83,660 | 41.8% |
| Normal | 52,354 | 26.2% |
| Bad | 16,642 | 8.3% |
| Very bad | 2123 | 1.1% |
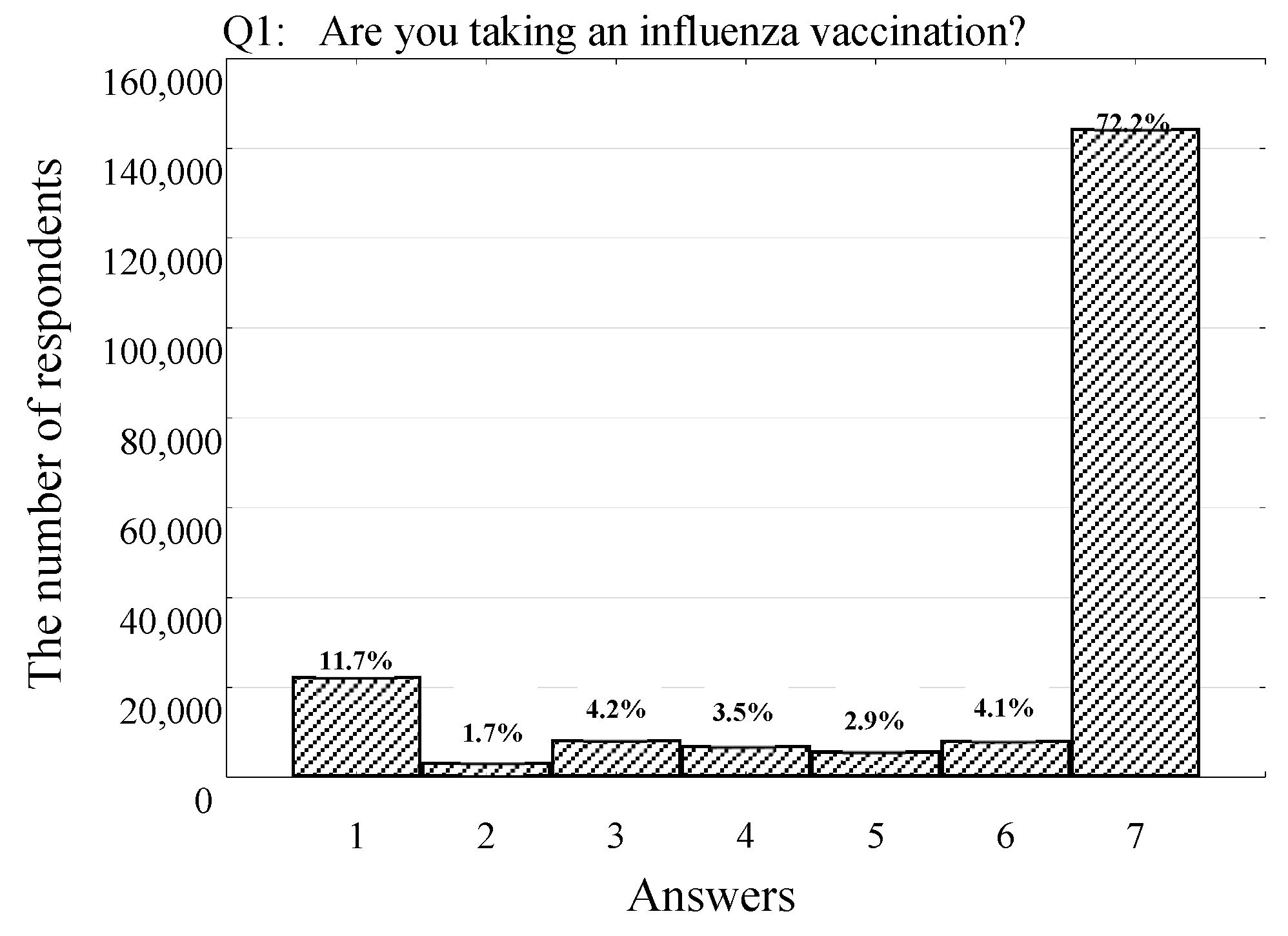
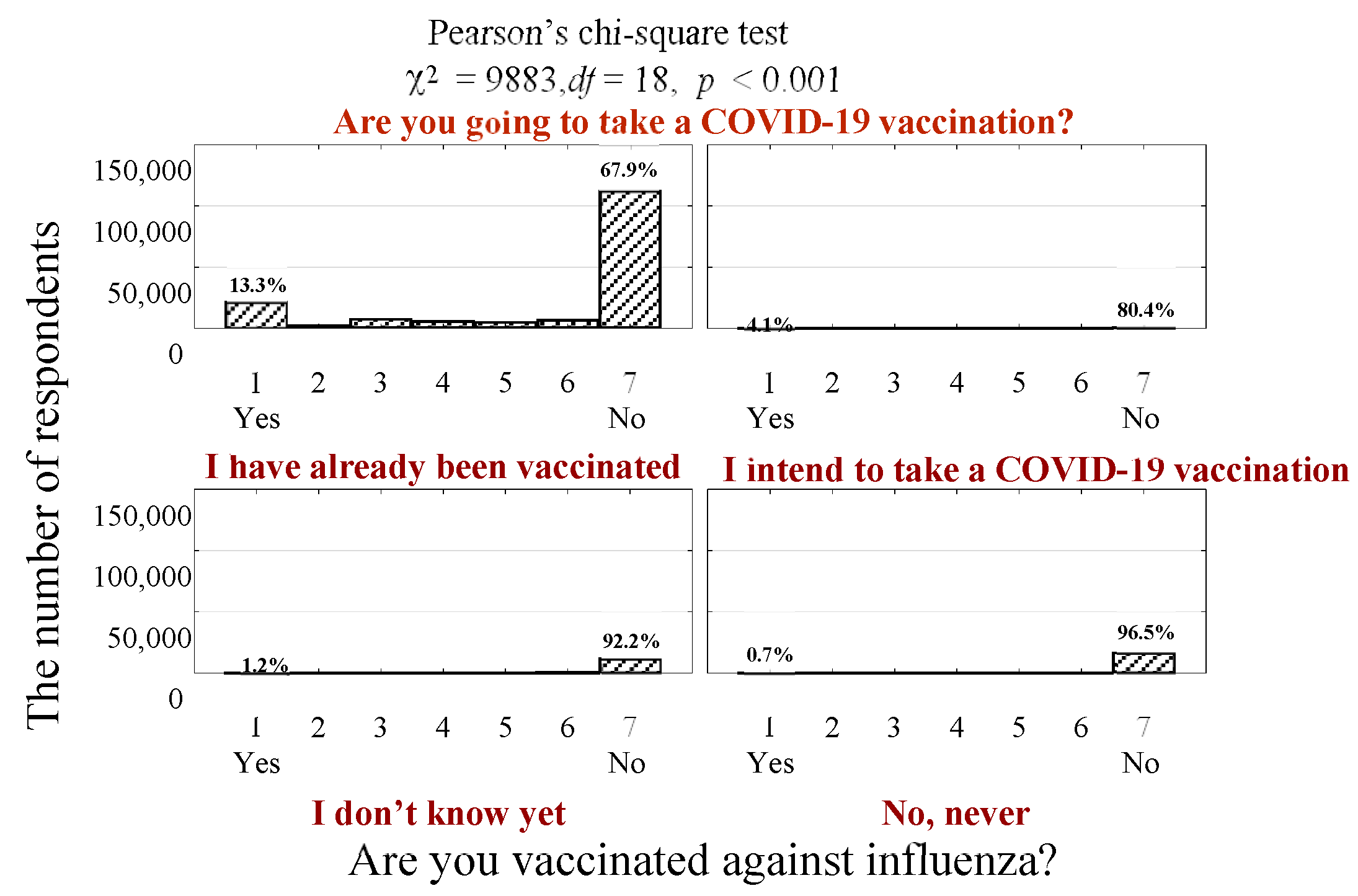
| Q1: Are you vaccinated against influenza? | n | (%) |
| 1—Yes, every year, including in 2022 | 22,512 | 11.3 |
| 2—Yes, every year, but I couldn’t take an influenza vaccination in 2022 due to the lack of its availability | 3413 | 1.7 |
| 3—Yes, but not every year. I got the influenza vaccine in 2022 | 8431 | 4.2 |
| 4—Yes, but not every year. I wanted to get a vaccine in 2022, but I couldn’t due to the lack of its availability | 7069 | 3.5 |
| 5—Usually not, but I got the influenza vaccine in 2022 | 5873 | 2.9 |
| 6—Usually not. I wanted to get a vaccine in 2022, but I couldn’t due to the lack of its availability | 8233 | 4.1 |
| 7—No, never | 144,469 | 72.2 |
| Q2: Are you going to take a vaccine against COVID-19? | n | (%) |
| 1—Yes, I have already been vaccinated | 166,445 | 83.2 |
| 2—Yes, I intend to take a COVID-19 vaccination | 2217 | 1.1 |
| 3—I don’t know yet | 13,471 | 6.7 |
| 4—No, never | 17,867 | 8.9 |
| Q3: Why won’t you take a COVID-19 vaccination? | n | (%) |
| 1—I have concerns about the safety of the COVID-19 vaccine | 9966 | 5.0 |
| 2—I am afraid of post-vaccination complications | 11,913 | 6.0 |
| 3—I can’t get vaccinated due to medical reasons | 4372 | 2.2 |
| 4—I am against vaccination in general | 5087 | 2.5 |
| Predictors of Positive Attitudes toward COVID-19 Vaccination | Attitude to Vaccination | p | OR (95%) | |||
|---|---|---|---|---|---|---|
| Positive | Negative | |||||
| n | (%) | n | (%) | |||
| Gender: | ||||||
| Men | 69,364 | 41.1% | 11,467 | 36.6% | <0.001 | 1.21 (1.18–1.24) |
| Women | 99,298 | 58.9% | 19,871 | 63.4% | 1.00 (ref.) | |
| Age (years old): | <0.001 | |||||
| 18–24 | 3727 | 2.2% | 1284 | 4.1% | 1.00 (ref.) | |
| 25–34 | 14,243 | 8.4% | 4762 | 15.2% | 1.03 (0.96–1.11) | |
| 35–44 | 28,504 | 16.9% | 7829 | 25.0% | 1.25 (1.17–1.34) | |
| 45–54 | 36,275 | 21.5% | 6990 | 22.3% | 1.79 (1.67–1.91) | |
| 55–64 | 37,650 | 22.3% | 5971 | 19.1% | 2.17 (2.03–2.33) | |
| 65+ | 48,263 | 28.6% | 4502 | 14.4% | 3.69 (3.44–3.96) | |
| Education: | <0.001 | |||||
| Primary | 20,736 | 12.3% | 6418 | 20.5% | 1.00 (ref.) | |
| Secondary | 48,778 | 28.9% | 10,606 | 33.8% | 1.42 (1.37–1.47) | |
| Higher | 99,148 | 58.8% | 14,314 | 45.7% | 2.14 (2.07–2.22) | |
| Place of residence: | <0.001 | |||||
| Village | 35,382 | 21.0% | 8850 | 28.2% | 1.00 (ref.) | |
| Town less than 19,000 inhabitants | 20,132 | 11.9% | 3692 | 11.8% | 1.36 (1.31–1.42) | |
| Town between 20,000 to 49,000 inhabitants | 25,790 | 15.3% | 4939 | 15.8% | 1.31 (1.26–1.36) | |
| Town between 50,000 to 99,000 inhabitants | 19,606 | 11.6% | 3687 | 11.8% | 1.33 (1.28–1.39) | |
| Town between 100,000 to 199,000 inhabitants | 18,825 | 11.2% | 3222 | 10.3% | 1.46 (1.40–1.53) | |
| Town between 200,000 to 499,000 inhabitants | 18,288 | 10.8% | 2915 | 9.3% | 1.57 (1.50–1.64) | |
| Town more than 500,000 inhabitants | 30,639 | 18.2% | 4033 | 12.9% | 1.90 (1.83–1.98) | |
| Region in Poland: | <0.001 | |||||
| South | 37,854 | 22.4% | 7598 | 24.2% | 1.00 (ref.) | |
| Northwest | 27,852 | 16.5% | 4494 | 14.3% | 1.24 (1.20–1.29) | |
| Southwest | 18,463 | 10.9% | 3545 | 11.3% | 1.05 (1.00–1.09) | |
| North | 24,199 | 14.3% | 3801 | 12.1% | 1.28 (1.23–1.33) | |
| Central | 14,974 | 8.9% | 2843 | 9.1% | 1.06 (1.01–1.11) | |
| East | 17,867 | 10.6% | 5002 | 16.0% | 0.72 (0.69–0.75) | |
| Masovian voivodeship | 27,453 | 16.3% | 4055 | 12.9% | 1.36 (1.30–1.42) | |
| BMI | <0.001 | |||||
| Underweight | 2553 | 1.5% | 855 | 2.7% | 0.64 (0.59–0.69) | |
| In norm | 564,56 | 33.5% | 12,015 | 38.3% | 1.00 (ref.) | |
| Overweight | 66,544 | 39.5% | 11,086 | 35.4% | 1.28 (1.24–1.31) | |
| Obesity | 43,109 | 25.6% | 7382 | 23.6% | 1.24 (1.20–1.28) | |
| Physical health | <0.001 | |||||
| Very good | 22,568 | 13.4% | 5038 | 16.1% | 1.58 (1.40–1.79) | |
| Good | 68,601 | 40.7% | 11,816 | 37.7% | 2.05 (1.82–2.31) | |
| Normal | 64,680 | 38.3% | 11,579 | 36.9% | 1.97 (1.75–2.22) | |
| Bad | 11,754 | 7.0% | 2531 | 8.1% | 1.64 (1.45–1.86) | |
| Very bad | 1059 | 0.6% | 374 | 1.2% | 1.00 (ref.) | |
| Mental health | <0.001 | |||||
| Very good | 37,790 | 22.4% | 7431 | 23.7% | 1.62 (1.46–1.79) | |
| Good | 71,630 | 42.5% | 12,030 | 38.4% | 1.89 (1.71–2.09) | |
| Normal | 44,002 | 26.1% | 8352 | 26.7% | 1.67 (1.51–1.85) | |
| Bad | 13,629 | 8.1% | 3013 | 9.6% | 1.44 (1.29–1.60) | |
| Very bad | 1611 | 1.0% | 512 | 1.6% | 1.00 (ref.) | |
| Predictors of Negative Attitude to COVID-19 Vaccination | Respondents against Vaccination | p | OR (95%) | |||
|---|---|---|---|---|---|---|
| Yes | No | |||||
| n | (%) | n | (%) | |||
| Gender: | ||||||
| Men | 2673 | 52.5% | 8794 | 33.5% | <0.001 | 2.20 (2.07–2.34) |
| Women | 2414 | 47.5% | 17,457 | 66.5% | 1.00 (ref.) | |
| Age (years old): | <0.001 | |||||
| 18–24 | 269 | 5.3% | 1015 | 3.9% | 1.36 (1.16–1.59) | |
| 25–34 | 832 | 16.4% | 3930 | 15.0% | 1.09 (0.97–1.21) | |
| 35–44 | 1306 | 25.7% | 6523 | 24.8% | 1.03 (0.93–1.13) | |
| 45–54 | 1058 | 20.8% | 5932 | 22.6% | 0.92 (0.83–1.01) | |
| 55–64 | 888 | 17.5% | 5083 | 19.4% | 0.90 (0.81–1.00) | |
| 65+ | 734 | 14.4% | 3768 | 14.4% | 1.00 (ref.) | |
| Education level: | <0.001 | |||||
| Primary | 1427 | 28.1% | 4991 | 19.0% | 2.01 (1.86–2.17) | |
| Secondary | 1879 | 36.9% | 8727 | 33.2% | 1.52 (1.41–1.63) | |
| Higher | 1781 | 35.0% | 12,533 | 47.7% | 1.00 (ref.) | |
| Place of residence: | 0.061 | |||||
| Village | 1446 | 28.4% | 7404 | 28.2% | 1.00 (ref.) | |
| Town less than 19,000 inhabitants | 607 | 11.9% | 3085 | 11.8% | 1.01 (0.91–1.12) | |
| Town between 20,000 to 49,000 inhabitants | 763 | 15.0% | 4176 | 15.9% | 0.94 (0.85–1.03) | |
| Town between 50,000 to 99,000 inhabitants | 653 | 12.8% | 3034 | 11.6% | 1.10 (1.00–1.22) | |
| Town between 100,000 to 199,000 inhabitants | 524 | 10.3% | 2698 | 10.3% | 0.99 (0.89–1.11) | |
| Town between 200,000 to 499,000 inhabitants | 435 | 8.6% | 2480 | 9.4% | 0.90 (0.80–1.01) | |
| Town more than 500,000 inhabitants | 659 | 13.0% | 3374 | 12.9% | 1.00 (0.90–1.11) | |
| Region in Poland: | 0.213 | |||||
| South | 1225 | 24.1% | 6373 | 24.3% | 1.00 (ref.) | |
| Northwest | 711 | 14.0% | 3783 | 14.4% | 0.98 (0.88–1.08) | |
| Southwest | 612 | 12.0% | 2933 | 11.2% | 1.09 (0.98–1.21) | |
| North | 647 | 12.7% | 3154 | 12.0% | 1.07 (0.96–1.18) | |
| Central | 440 | 8.6% | 2403 | 9.2% | 0.95 (0.85–1.07) | |
| East | 825 | 16.2% | 4177 | 15.9% | 1.03 (0.93–1.13) | |
| Masovian voivodeship | 627 | 12.3% | 3428 | 13.1% | 0.95 (0.86–1.06) | |
| BMI | 0.196 | |||||
| Underweight | 145 | 2.9% | 710 | 2.7% | 1.09 (0.90–1.31) | |
| In norm | 1900 | 37.4% | 10,115 | 38.5% | 1.00 (ref.) | |
| Overweight | 1861 | 36.6% | 9225 | 35.1% | 1.07 (1.00–1.15) | |
| Obesity | 1181 | 23.2% | 6201 | 23.6% | 1.01 (0.94–1.10) | |
| Physical health | <0.001 | |||||
| Very good | 1215 | 23.9% | 3823 | 14.6% | 1.51 (1.15–1.99) | |
| Good | 1987 | 39.1% | 9829 | 37.4% | 0.96 (0.73–1.26) | |
| Normal | 1517 | 29.8% | 10,062 | 38.3% | 0.72 (0.55–0.94) | |
| Bad | 303 | 6.0% | 2228 | 8.5% | 0.65 (0.48–0.87) | |
| Very bad | 65 | 1.3% | 309 | 1.2% | 1.00 (ref.) | |
| Mental health | <0.001 | |||||
| Very good | 1583 | 31.1% | 5848 | 22.3% | 1.34 (1.06–1.70) | |
| Good | 1878 | 36.9% | 10,152 | 38.7% | 0.92 (0.72–1.16) | |
| Normal | 1145 | 22.5% | 7207 | 27.5% | 0.79 (0.62–1.00) | |
| Bad | 395 | 7.8% | 2618 | 10.0% | 0.75 (0.58–0.96) | |
| Very bad | 86 | 1.7% | 426 | 1.6% | 1.00 (ref.) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gołębiowska, J.; Zimny-Zając, A.; Dróżdż, M.; Makuch, S.; Dudek, K.; Mazur, G.; Agrawal, S. Evaluation of the Approach towards Vaccination against COVID-19 among the Polish Population—In Relation to Sociodemographic Factors and Physical and Mental Health. Vaccines 2023, 11, 700. https://doi.org/10.3390/vaccines11030700
Gołębiowska J, Zimny-Zając A, Dróżdż M, Makuch S, Dudek K, Mazur G, Agrawal S. Evaluation of the Approach towards Vaccination against COVID-19 among the Polish Population—In Relation to Sociodemographic Factors and Physical and Mental Health. Vaccines. 2023; 11(3):700. https://doi.org/10.3390/vaccines11030700
Chicago/Turabian StyleGołębiowska, Justyna, Anna Zimny-Zając, Mateusz Dróżdż, Sebastian Makuch, Krzysztof Dudek, Grzegorz Mazur, and Siddarth Agrawal. 2023. "Evaluation of the Approach towards Vaccination against COVID-19 among the Polish Population—In Relation to Sociodemographic Factors and Physical and Mental Health" Vaccines 11, no. 3: 700. https://doi.org/10.3390/vaccines11030700