
A Qualitative Study Exploring Motivators and Barriers to COVID-19 Vaccine Uptake among Adults in South Africa and Zimbabwe
 , , , and
, , , and
Abstract
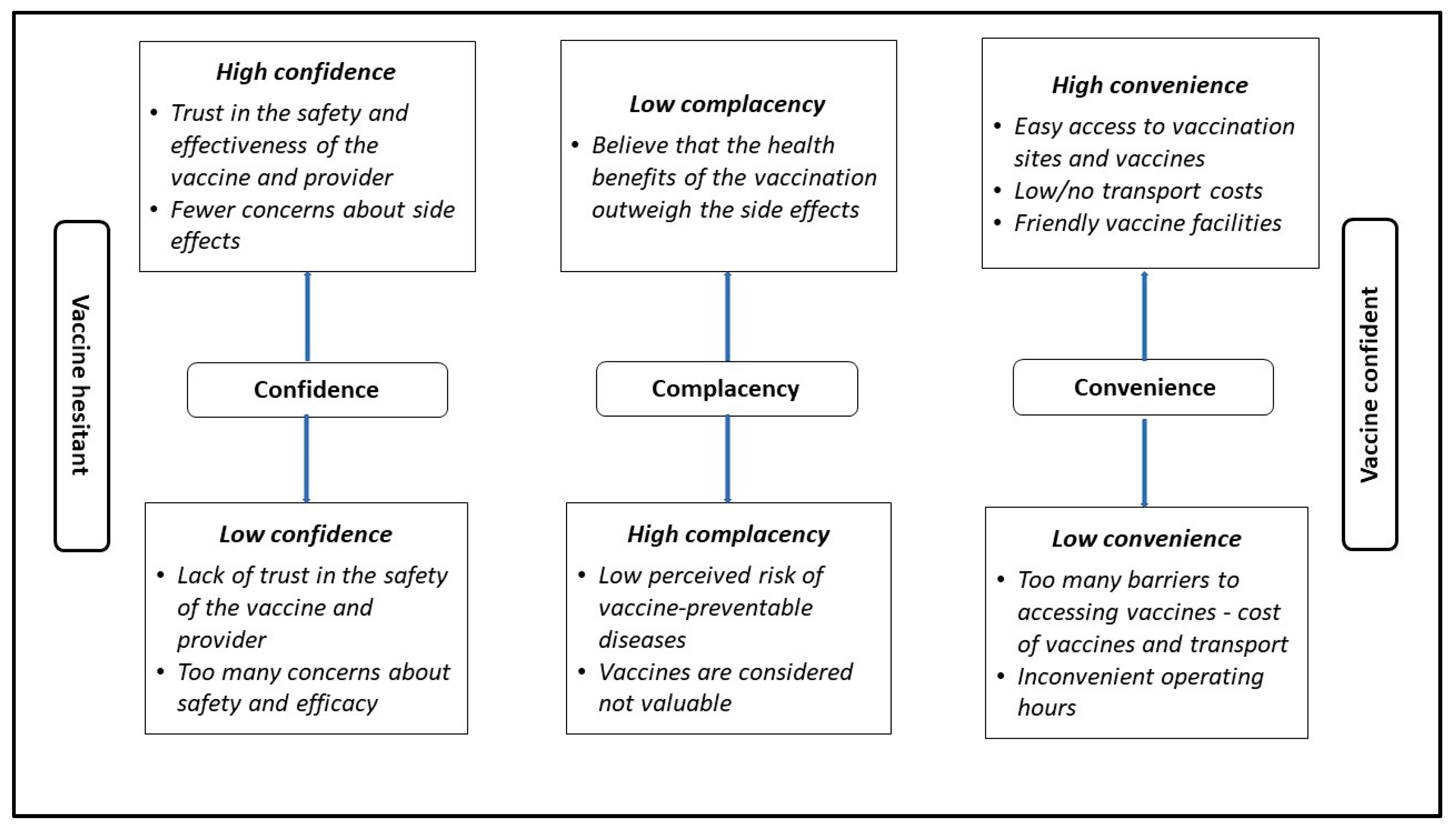
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Setting
2.3. Sampling
2.4. Procedures
2.5. Measures
2.6. Data Analysis
2.7. Ethical Considerations
3. Results
3.1. Participants’ Sociodemographics

{kind=link}
{kind=link}
| Variables | South Africa (n = 81) | Zimbabwe (n = 48) | Total (n = 129) |
|---|---|---|---|
| Gender | |||
| Female | 56 (69.1%) | 29 (60.4%) | 85 (65.9) |
| Male | 25 (30.9%) | 19 (39.6%) | 44 (34.1) |
| Median age (IQR): | 40 (23) | 39.5 (19) | 40 (22) |
| Race | |||
| Black | 65 (80.2) | 48 (100) | 113 (87.6) |
| Colored | 16 (19.8) | 16 (12.4) | |
| HIV status Negative Positive | * Not assessed | 40 (83.3) 8 (16.7) | N/A |
| Education | |||
| Primary | 9 (11.1) | 3 (6.2) | 12 (9.3) |
| Secondary | 61 (75.3) | 9 (18.8) | 70 (54.3) |
| O level | – | 32 (66.7) | 32 (24.8) |
| A level | – | 3 (6.2) | 3 (2.3) |
| Post matric diploma | 9 (11.1) | 1 (2.1) | 10 (7.8) |
| Bachelor’s degree | 2 (2.5) | – | 2 (1.6) |
| Employment | |||
| Unemployed | 63 (77.8) | 14 (29.2) | 77 (59.7) |
| Self-employed | 2 (2.5) | 22 (45.8) | 24 (18.6) |
| Employed part time | 3 (3.7) | 2 (4.2) | 5 (3.9) |
| Volunteer work | 7 (8.6) | 1 (2.1) | 8 (6.2) |
| Employed full time | 6 (7.4) | 8 (16.6) | 14 (10.9) |
| Pensioner | – | 1 (2.1) | 1 (0.7) |
| Vaccination status | |||
| Unvaccinated | 37 (45.7) | 24 (50) | 61 (49.3) |
| Vaccinated | 44 (54.3) | 24 (50) | 68 (52.7) |
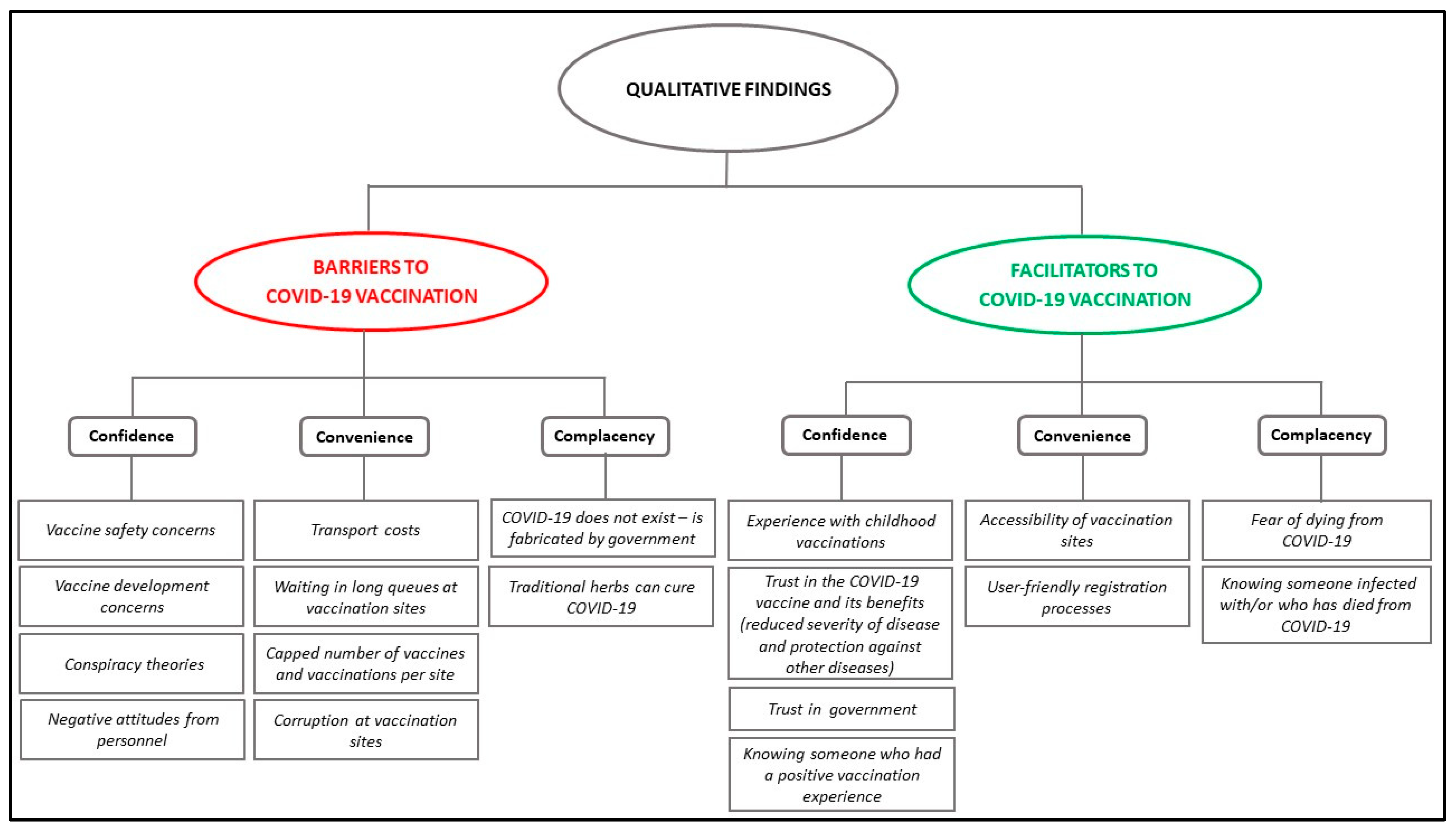
3.2. Barriers to COVID-19 Vaccination
3.2.1. Lack of Convenience as Barrier
“At clinics it [will] be full, that made people not to go. It would be too full.”(V_50+ GP)
“If there’s a line, so most of the people isn’t going because no one wants to stand in the line.”(UV_18–35_WC)
“There were a lot of people at the vaccination site to an extent that someone wakes up around 4 am but could not get the number to be vaccinated. It’s true there were now many people who knew they now needed to be vaccinated. Without blaming the nurses, some people lost interest and eventually stayed at home.”(V_45+_ZIM)
“I just think what’s preventing people… in fact, from the time you enter through the gate here going to the point where they vaccinate you, maybe I’m expecting to spend 30 min. After spending the 1 h here, I will also tell people back home that I almost died of hunger there at the hospital whilst they linger and vaccinate us at their own pace, so the ones I tell will hesitate to come.”(V_45+_ZIM)
“… Imagine waking up early in the morning, feeling cold for 2 days and you don’t get the vaccine because their number is enough for that particular day. When it happened to some people, they lost interest and stayed at home forever.”(V_45+_ZIM)
“… But when I returned for the second time, the challenge was [that] there were only two of us, so we had to wait for an additional four people to come so that they could open a batch of vaccines and inject us. We came in early, and we had to wait close to an hour, waiting for people trickling in. That one was also the challenge.”(V_50+_GP)
“Some people said, ‘we don’t get the vaccine; we buy vaccination cards’. So, I feel like the whole system was bad.”(V_45+_ZIM)
“Some would come and stand at the gate with money on a paper and hand it to someone … That discouraged me because I will have come in time. The person who would’ve come will just hand over money and do not get vaccinated and leave you in the queue pretending as if they have been vaccinated.”(V_18-44_ZIM)
3.2.2. Low Confidence as a Barrier
“We also discovered on the news that when the first batch arrived—I think it’s Johnson & Johnson or Pfizer—they told us that the vaccines expired, so I think a lot of people got skeptical from that point, because how can they order things [vaccines] that are expired?”(UV_18–35_GP)
“But this thing, COVID, only just arrived but it already has a vaccine, which doesn’t make sense.”(UV_35–49_SA)
“… Cancer and HIV have always been here but now there is COVID-19 and they managed to get the vaccine so quick. When did they do the research? So quick there is vaccine, and they collect it from the airport. When did they manufacture the vaccine? There is this disease, but already they manufactured this. When did they mix the medications and see how they function? They cannot get the cure for HIV/AIDS, cancer, high blood, and sugar [diabetes].”(V_35–49_11_GP)
“Even now there are those who say the government sees that there are a lot of us, and this is the way to kill us.”(V_50+_GP)
“… But people are saying we are going to change in 2 or 3 years and become zombies, all those who are vaccinated. I am so scared to be vaccinated and I am not ready yet.”(UV_35–49_WC)
“So, this is why we couldn’t get vaccinated because of what we heard in the community—people saying ‘Ahh, this vaccine was brought to clear [reduce] the population, it’s clearing and it’s killing’.”(UV_18–44_ZIM)
“… we [participants in the FGD] take ART, so with the news that you may die, the vaccine will destroy all the drugs you are taking, so the vaccine is too powerful, so we said, ‘let’s wait’… plus we are on ART, and in some other times we have challenges with the ART… so when I have problems after getting vaccinated, people will start blaming the vaccine, but I may have been terminally ill for long.”(UV_R_18–44_ZIM)
3.2.3. High Complacency as a Barrier
“I have never heard that a Nyaope [type of drug] addict is sick with COVID.”(UV_18–26 _GP)
“I am also not concerned because the COVID symptoms are just in your head, and if you tell yourself that you have COVID, that’s when you’ll see symptoms; otherwise, you have to treat yourself.”(UV_18–26_GP)
“[The] same thing that *Kim [Pseudonym used] said that she tested positive [for COVID-19], and I also tested positive before her and we took our herbs and quarantined, and we didn’t get sick. They called me after [a] month that I tested positive, and I did not vaccinate, but I was drinking the herbs, so I will not vaccinate.”(UV_18–26_GP)
“No, you will use your tablets or homemade medication like garlic and olive leaves. I still have garlic in my refrigerator. I don’t want to be vaccinated; I am healthy.”(UV_50+_WC)
“Here I support what they are saying, that I can be vaccinated but I am safe if I get zumbani or whatever and just drink.”(UV_45+_ZIM)
3.3. Motivators for COVID-19 Vaccine Uptake
3.3.1. Convenience as a Motivator
“I stay close to the clinic, and they would ask about where you stay and if you are able to come, and if not then they would tell you that on this particular day, they will be vaccinating at this particular place, which will be closer to where you stay, meaning you can get it easily.”(V_18–44_ZIM)
“Yes, because we have many vaccination sites that side, so it was not difficult at all.”(V_18–35_GP)
“It is easy, because you go there—even if you are not registered online, you go there, and they register you at the table. It is an easy process.”(V_36–49_GP)
3.3.2. Confidence as a Motivator
“I am supporting [participant] number 46 and I personally felt that there’s no Ministry which brings a vaccine to kill us but for our survival because the nation will perish, so I did not.”(V_18-44_ZIM)
“The reason I got vaccinated is that I trust the government will not kill the people. I am still alive… the government and the department of health will not kill [the] people. If they say there is a disease, and they say we should vaccinate, surely they want us to live.”(V_50+_GP)
“What really made me to get vaccinated is I heard that if you are vaccinated, it prevents the severity of COVID disease, and you experience less pain when it affects you because our immunity… they attack each other. Even my sister got COVID, and she had minor symptoms because she was vaccinated. Because of this, I decided to get vaccinated.”(V_45+_ZIM)
“The other reason is we grew up having these vaccines, and we just know that, whenever something like this is introduced, it is beneficial in life.”(V_45+_ZIM)
3.3.3. Low Complacency as a Motivator
“I vaccinated because I survived two times from Corona. I had Corona, so I saw a need to vaccinate since they said there will be [a] fourth wave, maybe I will not survive this time. So, I decided to get vaccinated to help myself because I nearly died as I had Corona two times. Yeah, I only wanted to stay alive.”(V_36–49_GP)
“What forced me to be vaccinated was I was afraid of dying and being crippled. I was scared, [and] that’s why I was vaccinated.”(V_18-44_ZIM)
“I saw a person who was ill with COVID. He had difficulty in breathing, and you could feel pity for him. So, it made me realize that getting vaccinated is the best, and that’s what pushed me to get vaccinated.”(V_18–44_ZIM)
“I vaccinated because I survived two times from Corona. I had Corona, so I saw a need to vaccinate. Since they said there will be a fourth wave, maybe I will not survive this time. So, I decided to get vaccinated to help myself because I nearly died as I had Corona two times, I only wanted to stay alive.”-(Participant 15, VIN_FGD_V_36-49 years_11-MAR-2022 GP)
4. Discussion
4.1. Confidence as a Barrier and Motivator
4.2. Convenience as a Barrier and Motivator
4.3. Complacency as a Barrier and Motivator
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, C.; Wang, Z.; Wang, G.; Lau, J.Y.; Zhang, K.; Li, W. COVID-19 in early 2021: Current status and looking forward. Signal Transduct. Target. Ther. 2021, 6, 114. [Google Scholar] [CrossRef]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 16 January 2023).
- World Health Organization. WHO Coronavirus (COVID-19) South Africa. Available online: https://covid19.who.int/region/afro/country/za (accessed on 16 January 2023).
- World Health Organization. WHO Coronavirus (COVID-19) Zimbabwe. Available online: https://covid19.who.int/region/afro/country/zw (accessed on 16 January 2023).
- Dzinamarira, T.; Nachipo, B.; Phiri, B.; Musuka, G. COVID-19 Vaccine Roll-Out in South Africa and Zimbabwe: Urgent Need to Address Community Preparedness, Fears and Hesitancy. Vaccines 2021, 9, 250. [Google Scholar] [CrossRef] [PubMed]
- Makadzange, A.T.; Gundidza, P.; Lau, C.; Dietrich, J.; Beta, N.; Myburgh, N.; Elose, N.; Ndhlovu, C.; James, W.; Stanberry, L. Attitudes to Vaccine Mandates among Late Adopters of COVID-19 Vaccines in Zimbabwe. Vaccines 2022, 10, 1090. [Google Scholar] [CrossRef]
- European Medicines Agency. COVID-19 Vaccines: Authorised. Available online: https://www.ema.europa.eu/en/human-regulatory/overview/public-health-threats/coronavirus-disease-covid-19/treatments-vaccines/vaccines-covid-19/covid-19-vaccines-authorised (accessed on 16 February 2023).
- World Health Organization. Status of COVID-19 Vaccines within WHO EUL/PQ Evaluation Process. Available online: https://extranet.who.int/pqweb/sites/default/files/documents/Status_COVID_VAX_12January2023.pdf (accessed on 16 February 2023).
- Larson, H.J.; Jarrett, C.; Eckersberger, E.; Smith, D.M.; Paterson, P. Understanding vaccine hesitancy around vaccines and vaccination from a global perspective: A systematic review of published literature, 2007–2012. Vaccine 2014, 32, 2150–2159. [Google Scholar] [CrossRef] [PubMed]
- The Strategic Advisory Group of Experts (SAGE). Report of the SAGE Working Group on Vaccine Hesitancy. Available online: https://www.asset-scienceinsociety.eu/sites/default/files/sage_working_group_revised_report_vaccine_hesitancy.pdf (accessed on 21 March 2023).
- Wismans, A.; Thurik, R.; Baptista, R.; Dejardin, M.; Janssen, F.; Franken, I. Psychological characteristics and the mediating role of the 5C model in explaining students’ COVID-19 vaccination intention. PLoS ONE 2021, 16, e0255382. [Google Scholar] [CrossRef]
- Geiger, M.; Rees, F.; Lilleholt, L.; Santana, A.P.; Zettler, I.; Wilhelm, O.; Betsch, C.; Böhm, R. Measuring the 7Cs of vaccination readiness. Eur. J. Psychol. Assess. 2022, 38, 261–269. [Google Scholar] [CrossRef]
- National Department of Health. Coronavirus COVID-19 Alert Level 1. Available online: https://www.gov.za/covid-19/about/coronavirus-covid-19-alert-level-1 (accessed on 28 September 2022).
- Gerretsen, P.; Kim, J.; Caravaggio, F.; Quilty, L.; Sanches, M.; Wells, S.; Brown, E.E.; Agic, B.; Pollock, B.G.; Graff-Guerrero, A. Individual determinants of COVID-19 vaccine hesitancy. PLoS ONE 2021, 16, e0258462. [Google Scholar] [CrossRef]
- COVID-19 Law Lab. Statutory Instrument. SI 2022-067 Public Health (COVID-19 Prevention, Containment and Treatment) (National Lockdown) (No. 2) (Amendment) Order, 2022 (No. 41), Zimbabwean Government: Harare, Zimbabwe, 2022.
- Department of Health Republic of South Africa. South Africa COVID-19 and Vaccine Social Listening Report 30 May 2022, Report 51; Department of Health Republic of South Africa: Pretoria, South Africa, 30 May 2022.
- Burger, R.; Köhler, T.; Golos, A.M.; Buttenheim, A.M.; English, R.; Tameris, M.; Maughan-Brown, B. Longitudinal changes in COVID-19 vaccination intent among South African adults: Evidence from the NIDS-CRAM panel survey, February to May 2021. BMC Public Health 2022, 22, 422. [Google Scholar] [CrossRef] [PubMed]
- Campbell, S.; Greenwood, M.; Prior, S.; Shearer, T.; Walkem, K.; Young, S.; Bywaters, D.; Walker, K. Purposive sampling: Complex or simple? Research case examples. J. Res. Nurs. 2020, 25, 652–661. [Google Scholar] [CrossRef]
- Penrod, J.; Preston, D.B.; Cain, R.E.; Starks, M.T. A discussion of chain referral as a method of sampling hard-to-reach populations. J. Transcult. Nurs. 2003, 14, 100–107. [Google Scholar] [CrossRef]
- Schurink, E. Designing qualitative research. In Research at Grass Roots: A Primer for the Caring Professions; de Vos, A., Ed.; Van Schaik: Pretoria, South Africa, 1998; pp. 252–276. [Google Scholar]
- Nyumba, T.O.; Wilson, K.; Derrick, C.J.; Mukherjee, N. The use of focus group discussion methodology: Insights from two decades of application in conservation. Methods Ecol. Evol. 2018, 9, 20–32. [Google Scholar] [CrossRef] [Green Version]
- Srivastava, A.; Thomson, S.B. Framework analysis: A qualitative methodology for applied policy research. Adm. Gov. 2009, 4, 72–79. [Google Scholar]
- Brown, K. Coloured and black relations in South Africa: The burden of racialized hierarchy. Macalester Int. 2000, 9, 198–207. [Google Scholar]
- Adhikari, M. ‘God made the white man, God made the black man…’: Popular racial stereotyping of Coloured people in apartheid South Africa. S. Afr. Hist. J. 2006, 55, 142–164. [Google Scholar] [CrossRef]
- Belli, S.; Broncano, F. Narratives of trust: Sharing knowledge as a second-order emotion. Hum. Aff. 2017, 27, 241–251. [Google Scholar] [CrossRef]
- Gewirtz-Meydan, A.; Mitchell, K.; Shlomo, Y.; Heller, O.; Grinstein-Weiss, M. COVID-19 among youth in Israel: Correlates of decisions to vaccinate and reasons for refusal. J. Adolesc. Health 2022, 70, 396–402. [Google Scholar] [CrossRef] [PubMed]
- Bates, B.R.; Villegas-Botero, A.; Costales, J.A.; Moncayo, A.L.; Tami, A.; Carvajal, A.; Grijalva, M.J. COVID-19 vaccine hesitancy in three Latin American countries: Reasons given for not becoming vaccinated in Colombia, Ecuador, and Venezuela. Health Commun. 2022, 37, 1465–1475. [Google Scholar] [CrossRef] [PubMed]
- Barrall, A.L.; Hoff, N.A.; Nkamba, D.M.; Musene, K.; Ida, N.; Bratcher, A.; Dzogang, C.; Tangney, S.; Beia, M.; Nzaji, M.K.; et al. Hesitancy to receive the novel coronavirus vaccine and potential influences on vaccination among a cohort of healthcare workers in the Democratic Republic of the Congo. Vaccine 2022, 40, 4998–5009. [Google Scholar] [CrossRef]
- Pugliese-Garcia, M.; Heyerdahl, L.W.; Mwamba, C.; Nkwemu, S.; Chilengi, R.; Demolis, R.; Guillermet, E.; Sharma, A. Factors influencing vaccine acceptance and hesitancy in three informal settlements in Lusaka, Zambia. Vaccine 2018, 36, 5617–5624. [Google Scholar] [CrossRef]
- Magadmi, R.M.; Kamel, F.O. Beliefs and barriers associated with COVID-19 vaccination among the general population in Saudi Arabia. BMC Public Health 2021, 21, 1438. [Google Scholar] [CrossRef]
- Cascini, F.; Pantovic, A.; Al-Ajlouni, Y.; Failla, G.; Ricciardi, W. Attitudes, acceptance and hesitancy among the general population worldwide to receive the COVID-19 vaccines and their contributing factors: A systematic review. EClinicalMedicine 2021, 40, 101113. [Google Scholar] [CrossRef] [PubMed]
- Crawshaw, J.; Konnyu, K.; Castillo, G.; van Allen, Z.; Grimshaw, J.M.; Presseau, J. Behavioural determinants of COVID-19 vaccination acceptance among healthcare workers: A rapid review. Public Health 2022, 210, 123–133. [Google Scholar] [CrossRef] [PubMed]
- Sherman, S.M.; Smith, L.E.; Sim, J.; Amlôt, R.; Cutts, M.; Dasch, H.; Rubin, G.J.; Sevdalis, N. COVID-19 vaccination intention in the UK: Results from the COVID-19 vaccination acceptability study (CoVAccS), a nationally representative cross-sectional survey. Hum. Vaccin. Immunother. 2021, 17, 1612–1621. [Google Scholar] [CrossRef] [PubMed]
- Usher, K.; Bhullar, N.; Durkin, J.; Gyamfi, N.; Jackson, D. Family violence and COVID-19: Increased vulnerability and reduced options for support. Int. J. Ment. Health Nurs. 2020, 29, 549–552. [Google Scholar] [CrossRef] [Green Version]
- Wynen, J.; Op de Beeck, S.; Verhoest, K.; Glavina, M.; Six, F.; Van Damme, P.; Beutels, P.; Hendrickx, G.; Pepermans, K. Taking a COVID-19 Vaccine or Not? Do Trust in Government and Trust in Experts Help Us to Understand Vaccination Intention? Adm. Soc. 2022, 54, 1875–1901. [Google Scholar] [CrossRef]
- Mokgobi, M.G. Understanding traditional African healing. Afr. J. Phys. Health Educ. Recreat. Danc. 2014, 20, 24–34. [Google Scholar]
- Krah, E.; de Kruijf, J.; Ragno, L. Integrating Traditional Healers into the Health Care System: Challenges and Opportunities in Rural Northern Ghana. J. Community Health 2018, 43, 157–163. [Google Scholar] [CrossRef] [Green Version]
- Audet, C.M.; Clemens, E.M.; Ngobeni, S.; Mkansi, M.; Sack, D.E.; Wagner, R.G. Throwing the bones to diagnose HIV: Views of rural South African traditional healers on undertaking HIV counselling and testing. AIDS Care 2021, 33, 1316–1320. [Google Scholar] [CrossRef]
- Kwedi Nolna, S.; Ntonè, R.; Fouda Mbarga, N.; Mbainda, S.; Mutangala, W.; Boua, B.; Niba, M.; Okoko, A. Integration of traditional healers in human African trypanosomiasis case finding in Central Africa: A quasi-experimental study. Trop. Med. Infect. Dis. 2020, 5, 172. [Google Scholar] [CrossRef]
- Lessard, D.; Ortiz-Paredes, D.; Park, H.; Varsaneux, O.; Worthington, J.; Basta, N.E.; MacDonald, S.E.; Lebouché, B.; Cox, J.; Ismail, S.J.; et al. Barriers and facilitators to COVID-19 vaccine acceptability among people incarcerated in Canadian federal prisons: A qualitative study. Vaccine X 2022, 10, 100150. [Google Scholar] [CrossRef]
- Klassen, A.C.; Milliron, B.-J.; Reynolds, L.; Bakhtibekova, Z.; Mamadraimov, S.; Bahruddinov, M.; Shokamolova, S.; Shuster, M.; Mukhtar, S.; Gafurova, M.; et al. Formative research to address vaccine hesitancy in Tajikistan. Vaccine 2021, 39, 1516–1527. [Google Scholar] [CrossRef] [PubMed]


| Age | South Africa | Zimbabwe | Total |
|---|---|---|---|
| (Years) | n (%) | n (%) | n (%) |
| 18–19 | – | 6 (12.5) | 6 (4.7) |
| 20–29 | 22 (27.2) | 8 (16.7) | 30 (23.2) |
| 30–39 | 18 (22.2) | 10 (20.8) | 28 (21.7) |
| 40–49 | 13 (16.0) | 17 (35.4) | 30 (23.2) |
| 50–59 | 22 (27.2) | 3 (6.3) | 25 (19.4) |
| 60+ | 6 (7.4) | 4 (8.3) | 10 (7.8) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Myburgh, N.; Mulaudzi, M.; Tshabalala, G.; Beta, N.; Gutu, K.; Vermaak, S.; Lau, C.; Hill, C.; Stanberry, L.; James, W.; et al. A Qualitative Study Exploring Motivators and Barriers to COVID-19 Vaccine Uptake among Adults in South Africa and Zimbabwe. Vaccines 2023, 11, 729. https://doi.org/10.3390/vaccines11040729
Myburgh N, Mulaudzi M, Tshabalala G, Beta N, Gutu K, Vermaak S, Lau C, Hill C, Stanberry L, James W, et al. A Qualitative Study Exploring Motivators and Barriers to COVID-19 Vaccine Uptake among Adults in South Africa and Zimbabwe. Vaccines. 2023; 11(4):729. https://doi.org/10.3390/vaccines11040729
Chicago/Turabian StyleMyburgh, Nellie, Mamakiri Mulaudzi, Gugulethu Tshabalala, Norest Beta, Kimberley Gutu, Stefanie Vermaak, Charles Lau, Catherine Hill, Lawrence Stanberry, Wilmot James, and et al. 2023. "A Qualitative Study Exploring Motivators and Barriers to COVID-19 Vaccine Uptake among Adults in South Africa and Zimbabwe" Vaccines 11, no. 4: 729. https://doi.org/10.3390/vaccines11040729