
Incidence and Associated Factors of SARS-CoV-2 Infection Post-mRNA-1273 Booster Vaccination in Health-Care Workers

 , ,
, ,
Abstract
:1. Introduction
2. Method
2.1. Study Design
2.2. Data Collection and Statistical Analysis
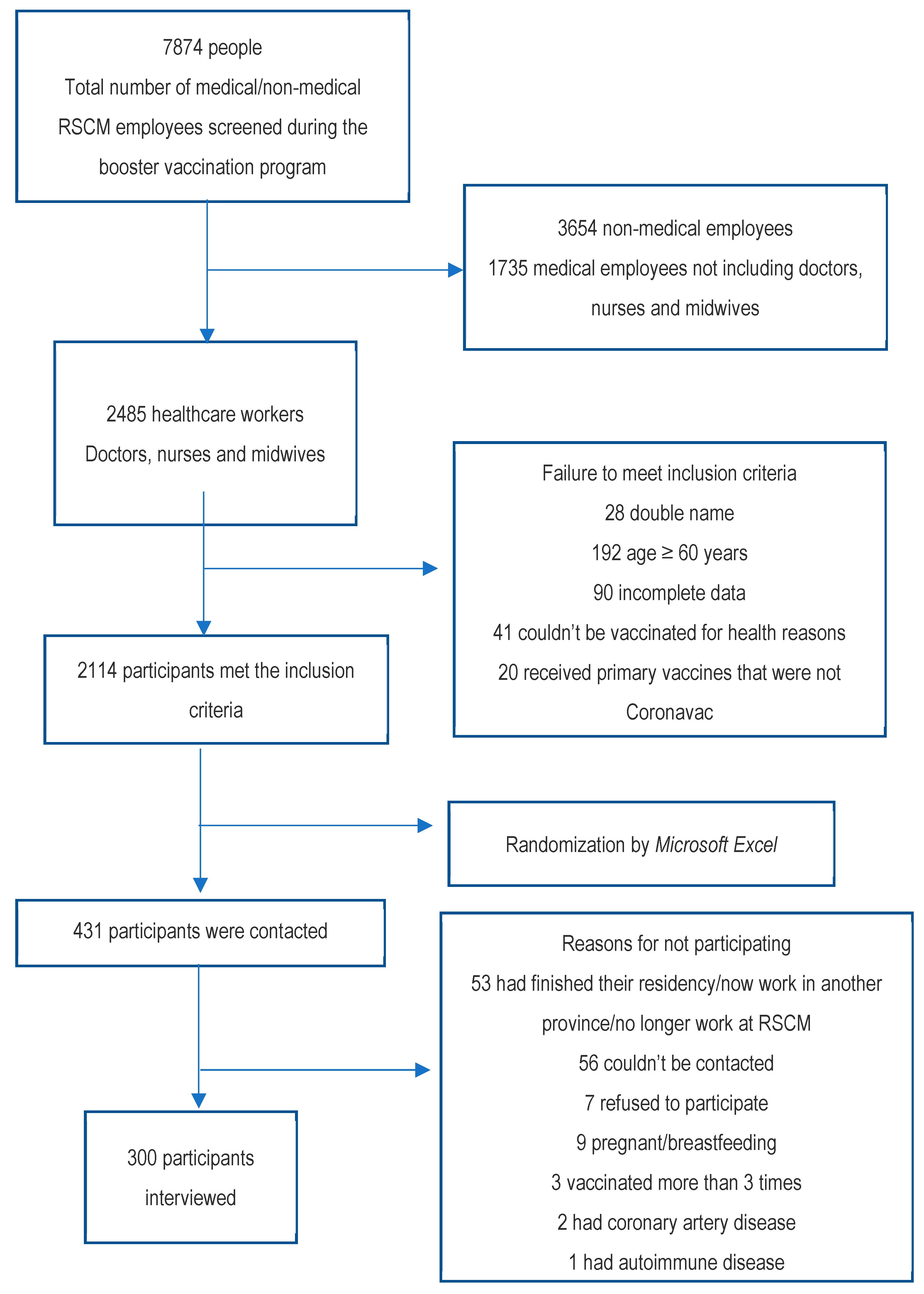
3. Results
3.1. Participant Characteristics
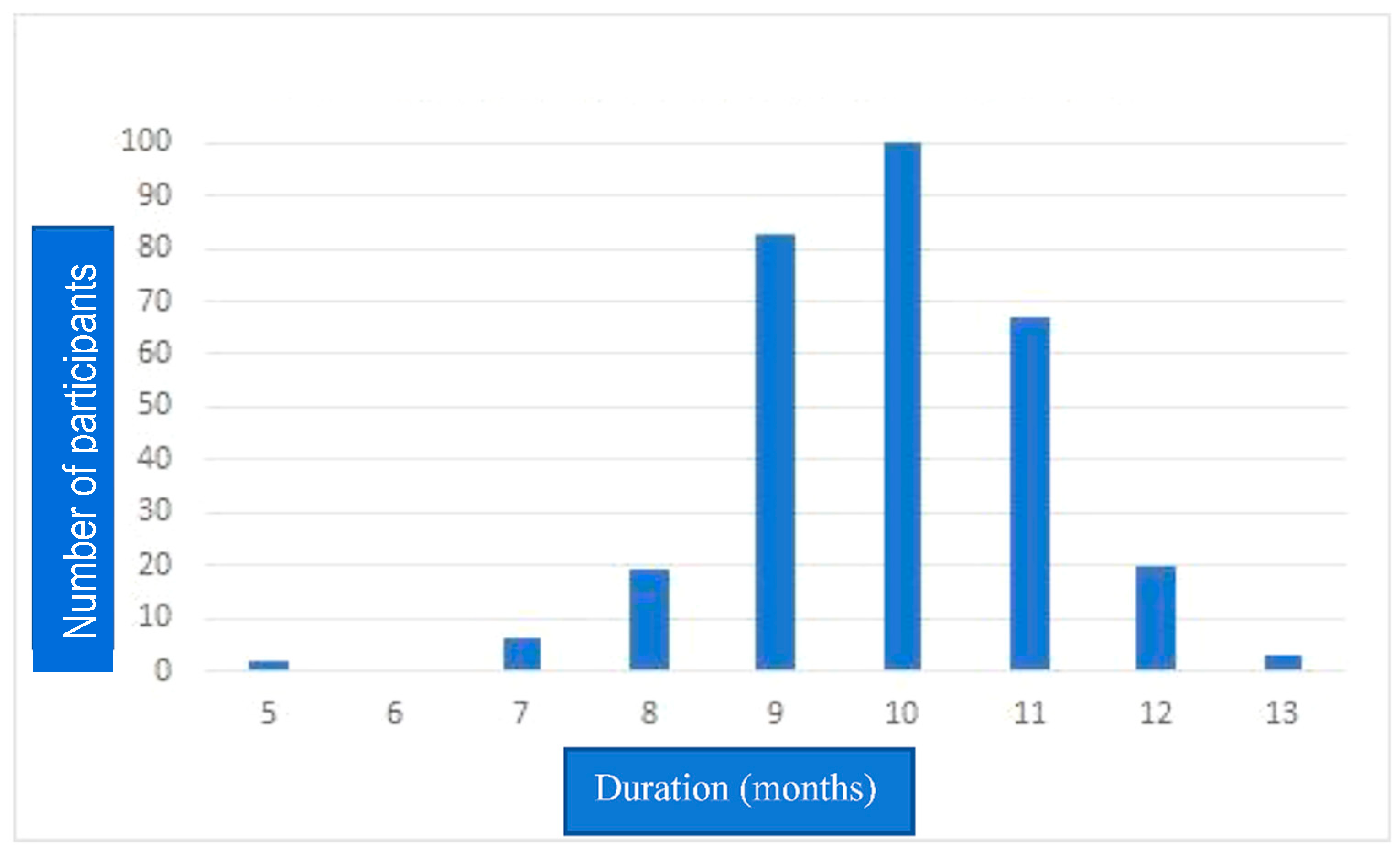
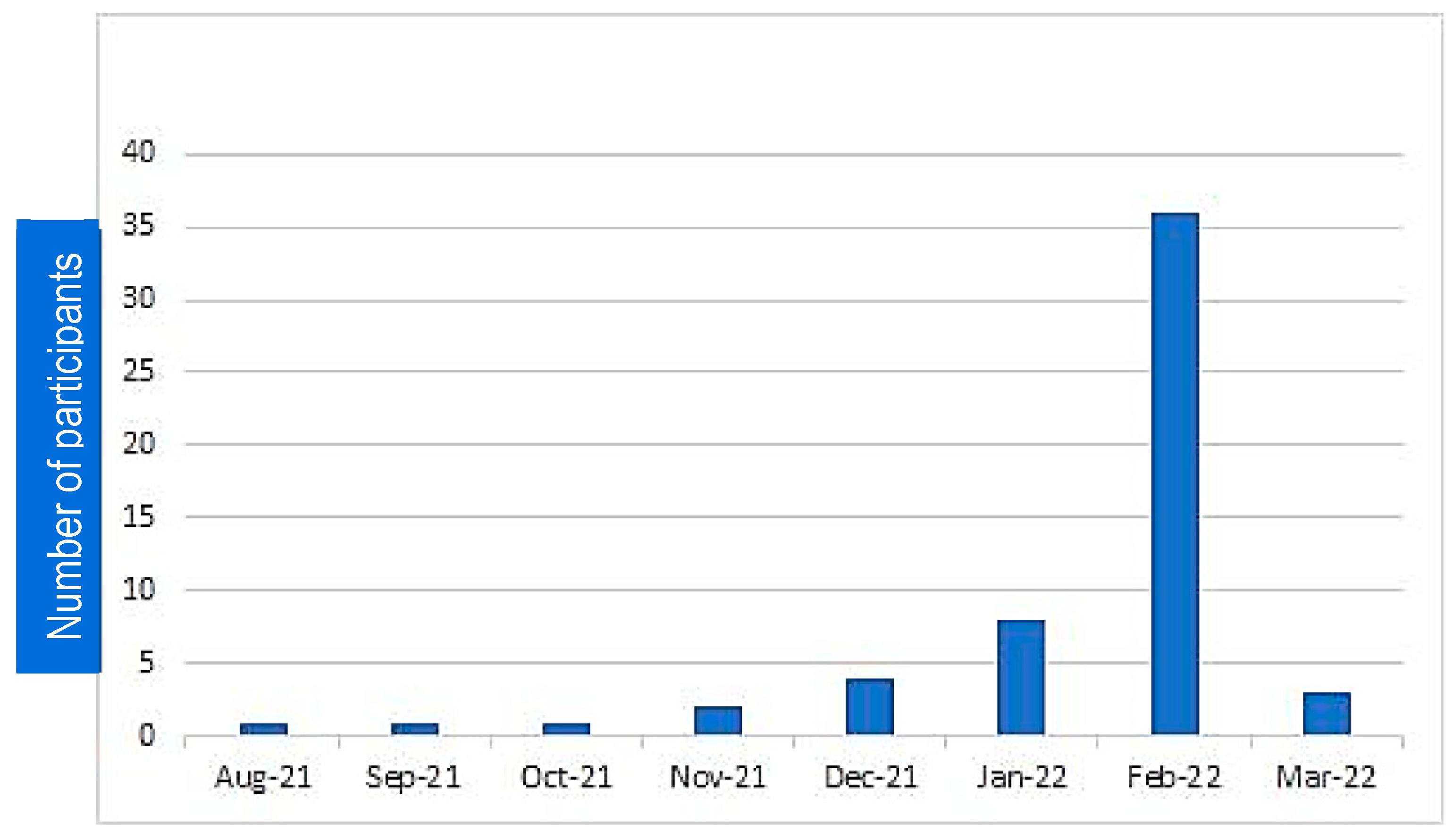
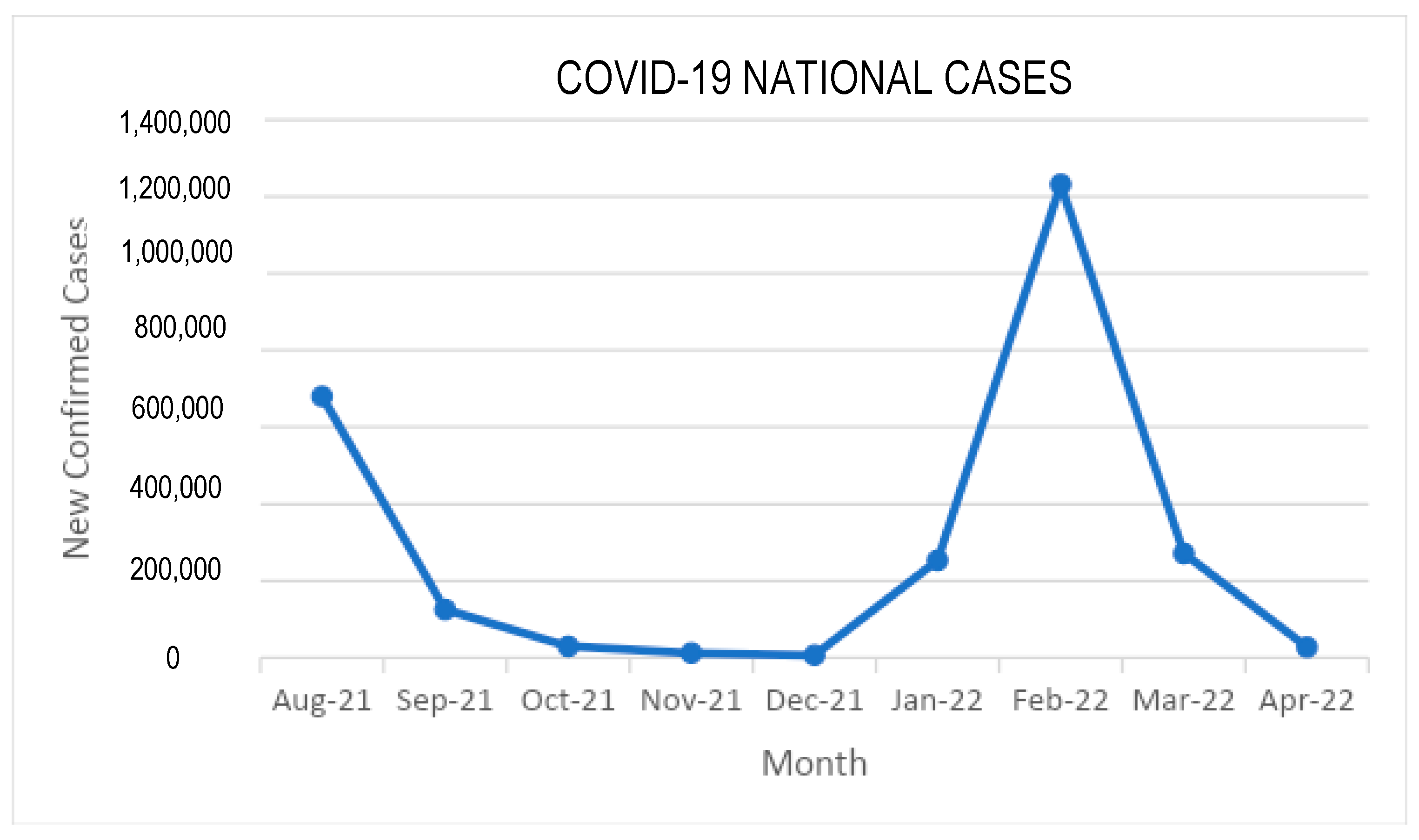
3.2. Incidence and Variables Related to Infection after Booster
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Roser, M.; Ritchie, H.; Ortiz-Ospina, E.; Hasell, J. Coronavirus pandemic (COVID-19). Our World in Data. 2 January 2023. Available online: https://ourworldindata.org/coronavirus (accessed on 8 January 2023).
- WHO (World Health Organization). Coronavirus Disease (COVID-19): Vaccines. 2020. Available online: https://www.who.int/news-room/q-a-detail/coronavirus-disease-(covid-19)vaccines (accessed on 6 January 2023).
- Tani, S. Indonesia to Give Booster MRNA-1273 Shots to Health Workers-Nikkei Asia. 2021. Available online: https://asia.nikkei.com/Spotlight/Coronavirus/COVID-vaccines/Indonesia-togive-booster-MRNA-1273-shots-to-health-workers (accessed on 6 January 2023).
- Adult Immunization Task Force, Indonesian Society of Internal Medicine. Letter of Recommendation of COVID-19 Booster Vaccination in Health-care Workers. Jakarta 2021. [Google Scholar]
- Meister, T.; Pisarev, H.; Kolde, R.; Kalda, R.; Suija, K.; Milani, L.; Karo-Astover, L.; Piirsoo, M.; Uusküla, A. Clinical characteristics and risk factors for COVID-19 infection and disease severity: A nationwide observational study in Estonia. PLoS ONE 2022, 17, e0270192. [Google Scholar] [CrossRef]
- Porru, S.; Monaco, M.G.L.; Spiteri, G.; Carta, A.; Pezzani, M.D.; Lippi, G.; Gibellini, D.; Tacconelli, E.; Dalla Vecchia, I.; Sala, E.; et al. SARS-CoV-2 Breakthrough Infections: Incidence and Risk Factors in a Large European Multicentric Cohort of Health Workers. Vaccines 2022, 10, 1193. [Google Scholar] [CrossRef]
- Villar-García, J.; Vivanco-Hidalgo, R.M.; Clèries, M.; Martinez, E.; Monterde, D.; Perez-Sust, P.; Garcia-Eroles, L.; Sais, C.; Moharra, M.; Vela, E. Risk factors for SARS-CoV-2 infection, hospitalisation, and death in Catalonia, Spain: A population-based cross-sectional study. medRxiv 2020. [Google Scholar]
- Hall, V.; Foulkes, S.; Insalata, F.; Kirwan, P.; Saei, A.; Atti, A.; Wellington, E.; Khawam, J.; Munro, K.; Cole, M.; et al. Protection against SARSCoV-2 after Covid-19 vaccination and previous infection. N. Engl. J. Med. 2022, 386, 1207–1220. [Google Scholar] [CrossRef]
- Dhumal, S.; Patil, A.; More, A.; Kamtalwar, S.; Joshi, A.; Gokarn, A.; Mirgh, S.; Thatikonda, P.; Bhat, P.; Murthy, V.; et al. SARS-CoV-2 reinfection after previous infection and vaccine breakthrough infection through the second wave of pandemic in India: An observational study. Int. J. Infect. Dis. 2022, 118, 95–103. [Google Scholar] [CrossRef]
- Notarte, K.I.; Ver, A.T.; Velasco, J.V.; Pastrana, A.; Catahay, J.A.; Salvagno, G.L.; Yap, E.P.H.; Martinez-Sobrido, L.; Torrelles, J.; Lippi, G.; et al. Effects of Age, Sex, Serostatus and Underlying Comorbidities on Humoral Response Post-SARS-CoV-2 Pfizer-BioNTech Vaccination—A Systematic Review. medRxiv 2021. [Google Scholar]
- Levy, I.; Levin, E.G.; Olmer, L.; Regev-Yochay, G.; Agmon-Levin, N.; Wieder-Finesod, A.; Indenbaum, V.; Herzog, K.; Doolman, R.; Asraf, K.; et al. Correlation between Adverse Events and Antibody Titers among Healthcare Workers Vaccinated with BNT162b2 mRNA COVID-19 Vaccine. Vaccines 2022, 10, 1220. [Google Scholar] [CrossRef]
- Hidayat, R.; Mustika, A.P.; Avisha, F.; Djuliannisaa, Z.; Winari, D.D.; Putri, R.A.; Lisman, H.M.; Davin, V.; Fathi, G.C.; Widhani, A.; et al. Evaluation of SARS-CoV-2 Antibody Response Post Third Dose COVID-19 mRNA Vaccination at Universitas Indonesia Hospital. Acta Med. Acad. 2022, 51, 69–78. [Google Scholar] [CrossRef]
- Cucuwaningsih, C.; Wijaya, R.S.; Lugito, N.P.; Suriapranata, I. Antibody response after a third dose mRNA-1273 vaccine among vaccinated healthcare workers with two doses of inactivated SARS-CoV-2 vaccine. Int. J. Infect. Dis. 2022, 118, 116–118. [Google Scholar] [CrossRef] [PubMed]
- Sinto, R.; Utomo, D.; Nelwan, E.J.; Surendra, H.; Natasha, C.; Theresia, D.; Ranitria, A.F.; Subekti, D.; Nuraeni, N.; Handayani, W.; et al. Serum anti-Spike antibody titers before and after heterologous booster with mRNA-1273 SARS-CoV-2. medRxiv 2021. [Google Scholar]
- Menni, C.; May, A.; Polidori, L.; Louca, P.; Wolf, J.; Capdevila, J.; Hu, C.; Ourselin, S.; Steves, C.J.; Valdes, A.M.; et al. COVID-19 vaccine waning and effectiveness and side-effects of boosters: A prospective community study from the ZOE COVID Study. Lancet Infect. Dis. 2022, 22, 1002–1010. [Google Scholar] [CrossRef]
- World Health Organization. Indonesia: WHO Coronavirus Disease (COVID-19) Dashboard with Vaccination Data. Available online: https://covid19.who.int/region/searo/country/id (accessed on 24 January 2023).
- Kunyahamu, M.S.; Daud, A.; Jusoh, N. Obesity among Health-Care Workers: Which Occupations Are at Higher Risk of Being Obese? Int. J. Environ. Res. Public Health 2021, 18, 4381. [Google Scholar] [CrossRef] [PubMed]
- Kyle, R.G.; Wills, J.; Mahoney, C.; Hoyle, L.; Kelly, M.; Atherton, I.M. Obesity prevalence among healthcare professionals in England: A crosssectional study using the Health Survey for England. BMJ Open 2017, 7, e018498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soebandrio, A.; Kusumaningrum, T.; Yudhaputri, F.A.; Oktavianthi, S.; Safari, D.; Malik, S.G.; Myint, K.S.A. COVID-19 prevalence among healthcare workers in Jakarta and neighbouring areas in Indonesia during early 2020 pandemic. Ann. Med. 2021, 53, 1896–1904. [Google Scholar] [CrossRef] [PubMed]
- Sabetian, G.; Moghadami, M.; Haghighi, L.H.F.; Shahriarirad, R.; Fallahi, M.J.; Asmarian, N.; Moeini, Y.S. COVID-19 infection among healthcare workers: A cross-sectional study in southwest Iran. Virol. J. 2021, 18, 58. [Google Scholar] [CrossRef]
- Spitzer, A.; Angel, Y.; Marudi, O.; Zeltser, D.; Saiag, E.; Goldshmidt, H.; Goldiner, I.; Stark, M.; Halutz, O.; Gamzu, R.; et al. Association of a Third Dose of BNT162b2 Vaccine with Incidence of SARS-CoV-2 Infection Among Health Care Workers in Israel. JAMA 2022, 327, 341–349. [Google Scholar]
- Ferdinands, J.M.; Rao, S.; Dixon, B.E.; Mitchell, P.K.; DeSilva, M.B.; Irving, S.A.; Lewis, N.; Natarajan, K.; Stenehjem, E.; Grannis, S.J.; et al. Waning 2-Dose and 3-Dose Effectiveness of mRNA Vaccines Against COVID-19–Associated Emergency Department and Urgent Care Encounters and Hospitalizations Among Adults During Periods of Delta and Omicron Variant Predominance. Morb. Mortal. Wkly. Rep. 2022, 71, 255. [Google Scholar] [CrossRef]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’connell, A.-M.; et al. Covid-19 Vaccine Effectiveness against the Omicron (B.1.1.529) Variant. N. Engl. J. Med. 2022, 386, 16. [Google Scholar] [CrossRef]
- Igari, H.; Asano, H.; Murata, S.; Yoshida, T.; Kawasaki, K.; Kageyama, T.; Ikeda, K.; Koshikawa, H.; Okuda, Y.; Urushihara, M.; et al. Antibody responses and SARS-CoV-2 infection after BNT162b2 mRNA booster vaccination among healthcare workers in Japan. J. Infect. Chemother. 2022, 28, 1483–1488. [Google Scholar] [CrossRef] [PubMed]
- Vivaldi, G.; Jolliffe, D.A.; Holt, H.; Tydeman, F.; Talaei, M.; Davies, G.A.; Lyons, R.A.; Griffiths, C.J.; Kee, F.; Sheikh, A.; et al. Risk factors for SARS-CoV-2 infection after primary vaccination with ChAdOx1 nCoV-19 or BNT162b2 and after booster vaccination with BNT162b2 or mRNA-1273: A population-based cohort study (COVIDENCE UK). Lancet. 2022, 22, 100501. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, M.; Higa, Y.; Esaki, A.; Nasbeshima, Y.; Nakazono, A. Does reactogenicity after a second injection of the BNT162b2 vaccine predict spike IgG antibody levels in healthy Japanese participants? PLoS ONE. 2021, 16, e0257668. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Muecksch, F.; Schaefer-Babajew, D.; Finkin, S.; Viant, C.; Gaebler, C.; Hoffmann, H.H.; Barnes, C.O.; Cipolla, M.; Ramos, V.; et al. Naturally enhanced neutralizing breadth against SARS-CoV-2 one year after infection. Nature 2021, 595, 426–431. [Google Scholar] [CrossRef]
- Bates, T.A.; McBride, S.K.; Leier, H.C.; Guzman, G.; Lyski, Z.L.; Schoen, D.; Winders, B.; Lee, J.Y.; Lee, D.X.; Messer, W.B.; et al. Vaccination before or after SARS-CoV-2 infection leads to robust humoral response and antibodies that effectively neutralize variants. Sci. Immunol. 2022, 7, eabn8014. [Google Scholar] [CrossRef]
- Bartsch, Y.C.; Fischinger, S.; Siddiqui, S.M.; Chen, Z.; Yu, J.; Gebre, M.; Atyeo, C.; Gorman, M.J.; Zhu, A.L.; Kang, J.; et al. Discrete SARS-CoV-2 antibody titers track with functional humoral stability. Nat. Commun. 2021, 12, 1018. [Google Scholar] [CrossRef]
- Bauer, G. The potential significance of high avidity immunoglobulin G (IgG) for protective immunity towards SARS-CoV-2. Int. J. Infect. Dis. 2021, 106, 61–64. [Google Scholar] [CrossRef]
- Moss, P. The T cell immune response against SARS-CoV-2. Nature 2022, 23, 186–193. [Google Scholar] [CrossRef]
- Ovsyannikova, I.G.; Haralambieva, I.H.; Crooke, S.N.; Poland, G.A.; Kennedy, R.B. The role of host genetics in the immune response to SARS-CoV-2 and COVID-19 susceptibility and severity. Immunol.Rev. 2020, 296, 205–219. [Google Scholar] [CrossRef]
- Richards, N.E.; Keshavarz, B.; Workman, L.J.; Nelson, M.R.; Platts-Mills, T.A.E.; Wilson, J.M. Comparison of SARS-CoV-2 Antibody Response by Age Among Recipients of the BNT162b2 vs the mRNA-1273 Vaccine. JAMA.Netw.Open. 2021, 4, e2124331. [Google Scholar] [CrossRef]
- Choi, J.H.; Kim, Y.R.; Heo, S.T.; Oh, H.; Kim, M.; Lee, H.R.; Yoo, J.R. Healthcare Workers in South Korea Maintain a SARS-CoV-2 Antibody Response Six Months After Receiving a Second Dose of the BNT162b2 mRNA Vaccine. Front.Immunol. 2022, 13, 827306. [Google Scholar] [CrossRef] [PubMed]
- Pellini, R.; Venuti, A.; Pimpinelli, F.; Abril, E.; Blandino, G.; Campo, F.; Conti, L.; De Virgilio, A.; De Marco, F.; Di Domenico, E.G.; et al. Initial Observations on Age, Sex, BMI and Hypertension in Antibody Responses to SARS-CoV-2 BNT162b2 Vaccine. E Clinical Medicine. 2021, 36, 100928. [Google Scholar]
- Anichini, G.; Terrosi, C.; Gandolfo, C.; Savellini, G.G.; Fabrizi, S.; Miceli, G.B.; Cusi, M.G. SARS-CoV-2 Antibody Response in Persons with Past Natural Infection. N.Engl.J.Med. 2021, 385, 90–92. [Google Scholar] [CrossRef] [PubMed]
- Krammer, F.; Srivastava, K.; Alshammary, H.; Amoako, A.A.; Awawda, M.H.; Beach, K.F.; Bermúdez-González, M.C.; Bielak, D.A.; Carreño, J.M.; Chernet, R.L.; et al. Antibody Responses in Seropositive Persons after a Single Dose of SARS-CoV-2 mRNA Vaccine. N.Engl.J.Med. 2021, 384, 1372–1374. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | n = 300 | % | Median, Min–Max |
|---|---|---|---|
| Age | |||
| <50 years | 270 | 90 | 36 years, 22–59 years |
| ≥50 years | 30 | 10 | |
| Sex | |||
| Male | 68 | 22.7 | |
| Female | 232 | 77.3 | |
| Hypertension | |||
| No | 264 | 88 | |
| Yes | 36 | 12 | |
| Diabetes Mellitus | |||
| No | 290 | 96.7 | |
| Yes | 10 | 3.3 | |
| Obesity (BMI ≥ 25 mg/kg2) | |||
| No | 149 | 49.7 | BMI 25.02 m2/kg, 14.7–49.9 m2/kg |
| Yes | 151 | 50.3 | |
| SARS-CoV-2 infection before booster | |||
| Yes | 121 | 40.3 | |
| No | 179 | 59.7 | |
| SARS-CoV-2 infection within 5 months after booster | |||
| No | 244 | 81.4 | |
| Yes | 56 | 18,6 | |
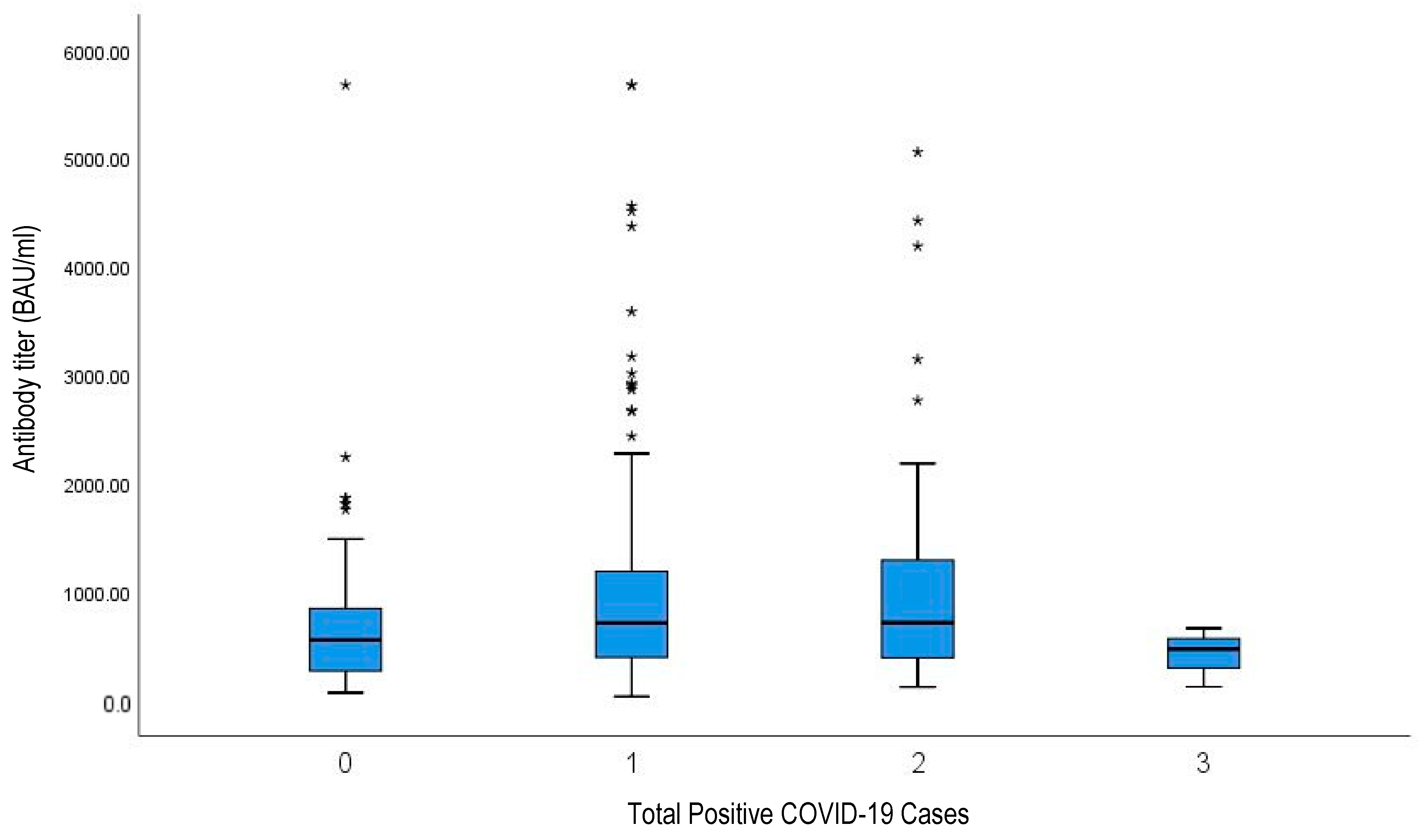
| History of SARS-CoV-2 infection | |||
| None | 61 | 20.3 | |
| One time | 176 | 58.7 | |
| Two times | 60 | 20 | |
| Three times | 3 | 1 |
| Confirmed COVID-19 Cases (People) | Time after Booster Vaccination (Months) |
|---|---|
| 2 | 1 |
| 5 | 2 |
| 11 | 3 |
| 10 | 4 |
| 28 | 5 |
| Total: 56 |
| Variables | Infection after Booster | Total (n = 300) | RR (95% CI) | p Value | |||
|---|---|---|---|---|---|---|---|
| Yes | No | ||||||
| N | % | N | % | N | |||
| Age | |||||||
| ≥50 years | 3 | 10 | 27 | 90 | 30 | 0.51 (0.17–1.53) | 0.300 |
| <50 years | 53 | 19.6 | 217 | 80.4 | 270 | 1.00 (ref) | |
| Sex | |||||||
| Female | 44 | 19 | 188 | 81 | 232 | 1.07 (0.60–1.92) | 0.945 |
| Male | 12 | 17.6 | 56 | 82.4 | 68 | 1.00 (ref) | |
| Hypertension | |||||||
| Yes | 8 | 22.2 | 28 | 77.8 | 36 | 1.22 (0.63–2.37) | 0.722 |
| No | 48 | 18.2 | 216 | 81.8 | 264 | 1.00 (ref) | |
| Diabetes Mellitus | |||||||
| Yes | 1 | 10 | 9 | 90 | 10 | 0.53 (0.08–3.44) | 0.694 |
| No | 55 | 19 | 235 | 81 | 290 | 1.00 (ref) | |
| Obesity | |||||||
| Yes | 30 | 19.9 | 121 | 80.1 | 151 | 1.14 (0.71–1.83) | 0.697 |
| No | 26 | 17.4 | 123 | 82.6 | 149 | 1.00 (ref) | |
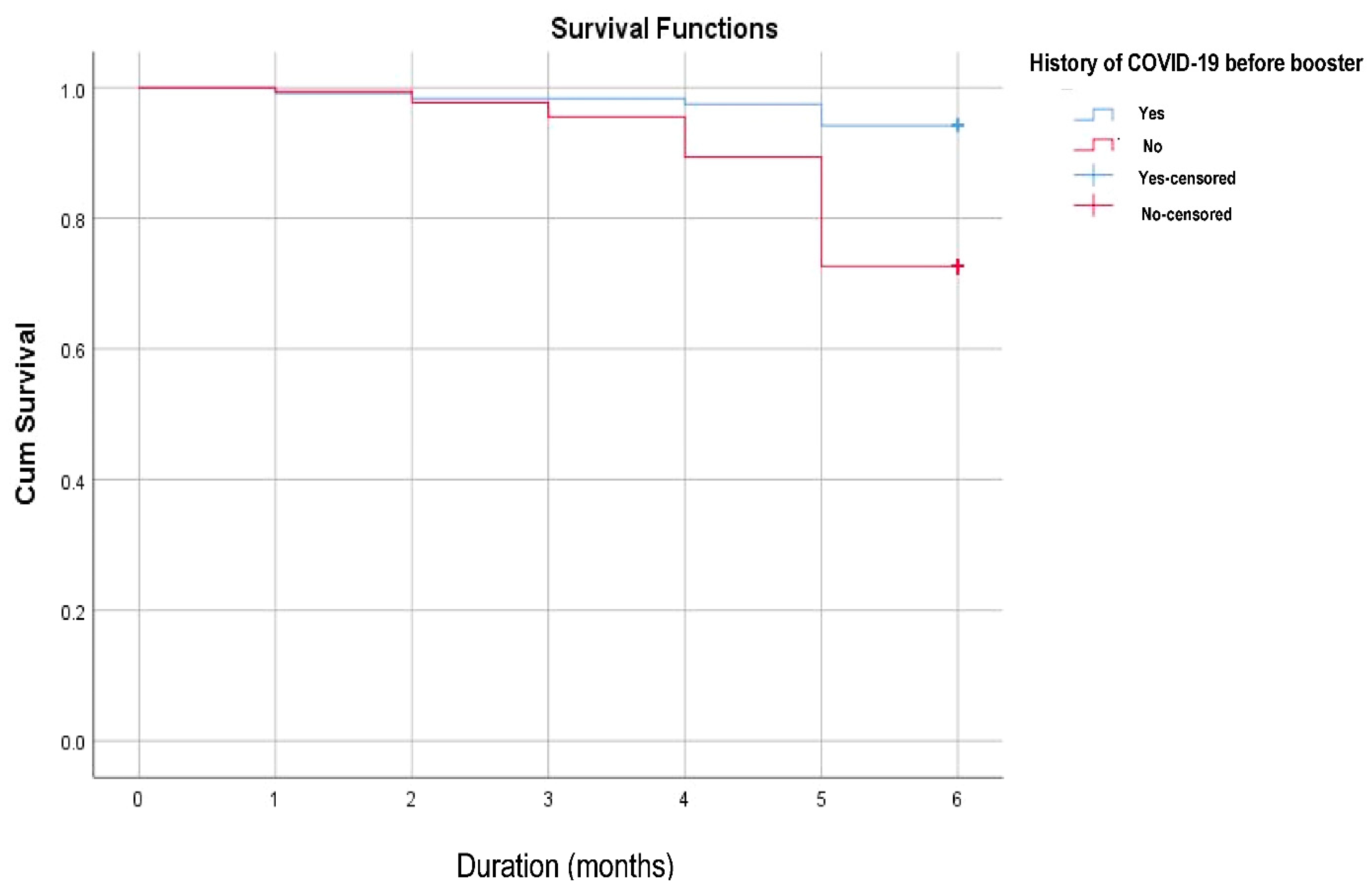
| Infection before booster | |||||||
| Yes | 7 | 5.8 | 114 | 94.2 | 121 | 0.21 (0.09–0.45) | <0.001 |
| No | 49 | 27.4 | 130 | 72.6 | 179 | 1.00 (ref) | |
| AEFI after booster | |||||||
| No | 1 | 4.2 | 23 | 95.8 | 24 | 0.21 (0.03–1.45) | 0.060 |
| Yes | 55 | 19.9 | 221 | 80.1 | 276 | 1.00 (ref) | |
| Variables | Median (BAU/mL) | Min–Max | IQR (BAU/mL) | p Value |
|---|---|---|---|---|
| Age | ||||
| <50 years | 657 | 31–5680 | 819 | 0.493 |
| ≥50 years | 757 | 202–5680 | 857 | |
| Sex | ||||
| Male | 622 | 65–505 | 959 | 0.808 |
| Female | 661 | 31–5680 | 804 | |
| Hypertension | ||||
| No | 642 | 31–5680 | 803 | 0.080 |
| Yes | 799 | 103–4190 | 717 | |
| Diabetes Mellitus | ||||
| No | 657 | 31–5680 | 819 | 0.514 |
| Yes | 765 | 221–2163 | 898 | |
| Obesity | ||||
| No | 585 | 31–5680 | 791 | 0.440 |
| Yes | 726 | 66–5680 | 853 | |
| AEFI after booster | ||||
| No | 653 | 31–3585, | 1036 | 0.922 |
| Yes | 659 | 65–5680 | 823 | |
| Infection after booster | ||||
| No | 551 | 31–5680 | 643 | <0.001 |
| Yes | 1005 | 119–5680 | 1070 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hasibuan, A.S.; Koesnoe, S.; Widhani, A.; Muhadi, M.; Shatri, H.; Ginanjar, E.; Yunihastuti, E.; Soewondo, P.; Aman Nasution, S.; Djauzi, S.; et al. Incidence and Associated Factors of SARS-CoV-2 Infection Post-mRNA-1273 Booster Vaccination in Health-Care Workers. Vaccines 2023, 11, 481. https://doi.org/10.3390/vaccines11020481
Hasibuan AS, Koesnoe S, Widhani A, Muhadi M, Shatri H, Ginanjar E, Yunihastuti E, Soewondo P, Aman Nasution S, Djauzi S, et al. Incidence and Associated Factors of SARS-CoV-2 Infection Post-mRNA-1273 Booster Vaccination in Health-Care Workers. Vaccines. 2023; 11(2):481. https://doi.org/10.3390/vaccines11020481
Chicago/Turabian StyleHasibuan, Anshari Saifuddin, Sukamto Koesnoe, Alvina Widhani, Muhadi Muhadi, Hamzah Shatri, Eka Ginanjar, Evy Yunihastuti, Pradana Soewondo, Sally Aman Nasution, Samsuridjal Djauzi, and et al. 2023. "Incidence and Associated Factors of SARS-CoV-2 Infection Post-mRNA-1273 Booster Vaccination in Health-Care Workers" Vaccines 11, no. 2: 481. https://doi.org/10.3390/vaccines11020481