
SARS-CoV-2 Infection-Blocking Immunity Post Natural Infection: The Role of Vitamin D
Abstract
:1. Introduction
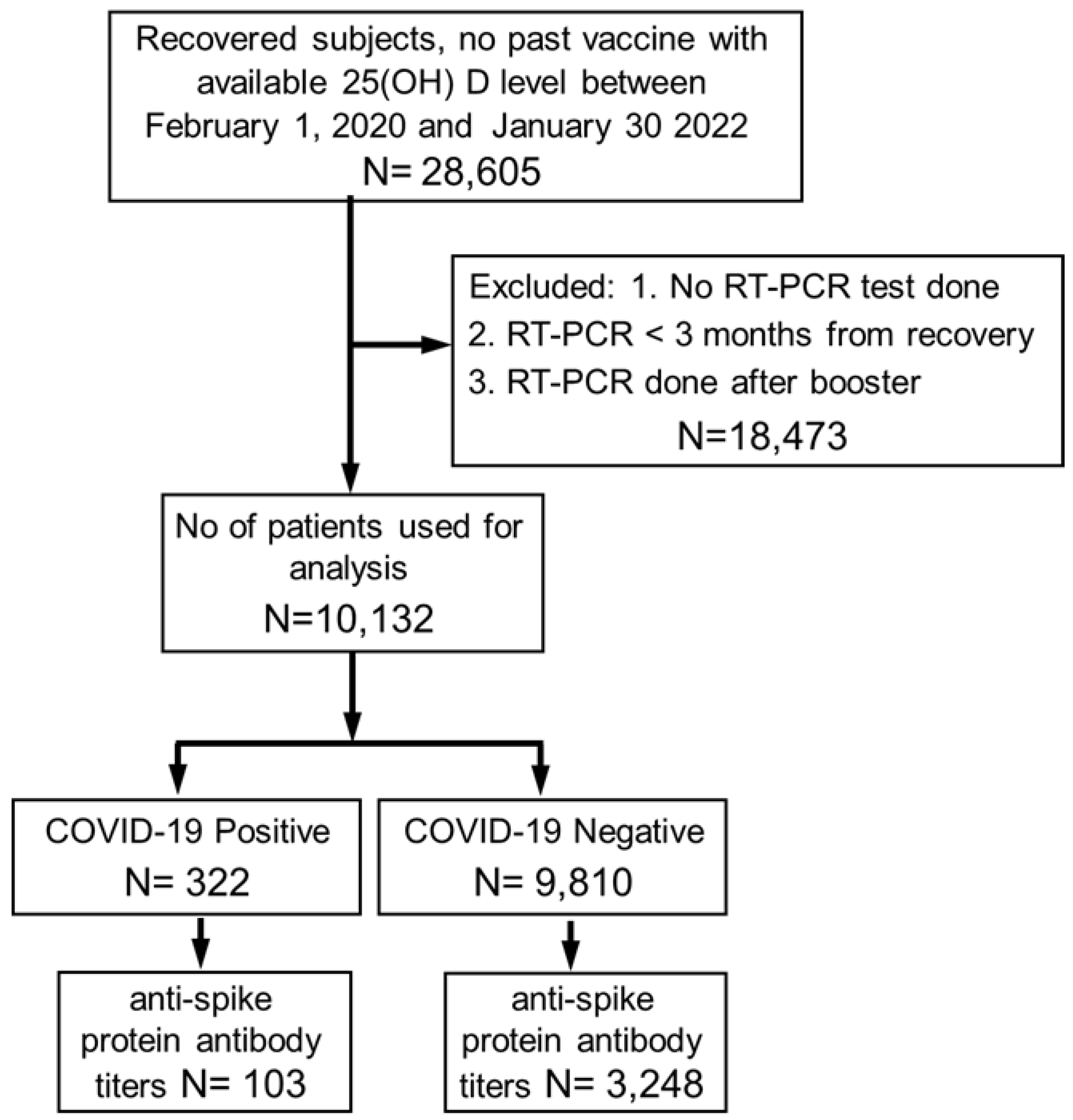
2. Methods and Patients
Statistical Analysis
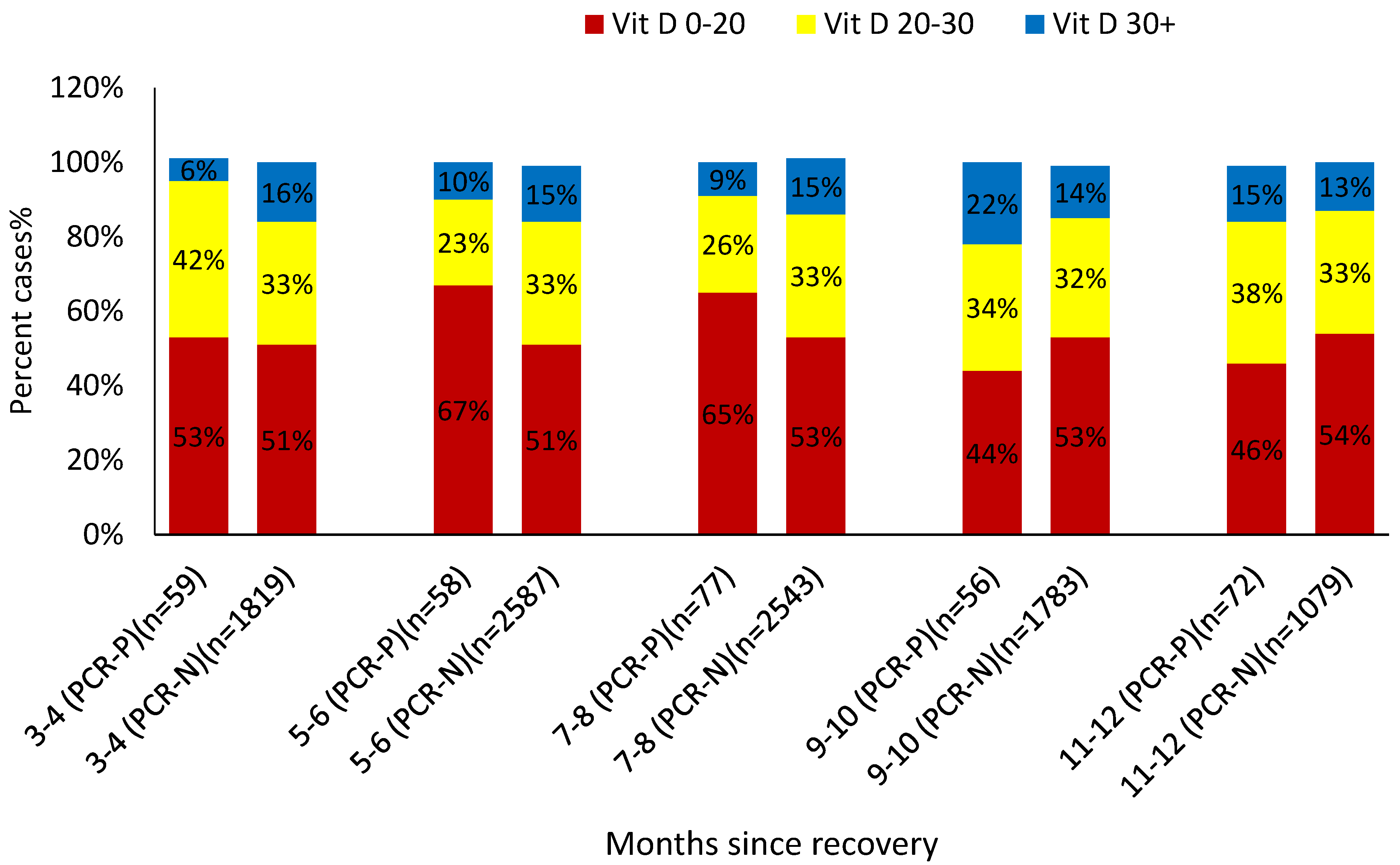
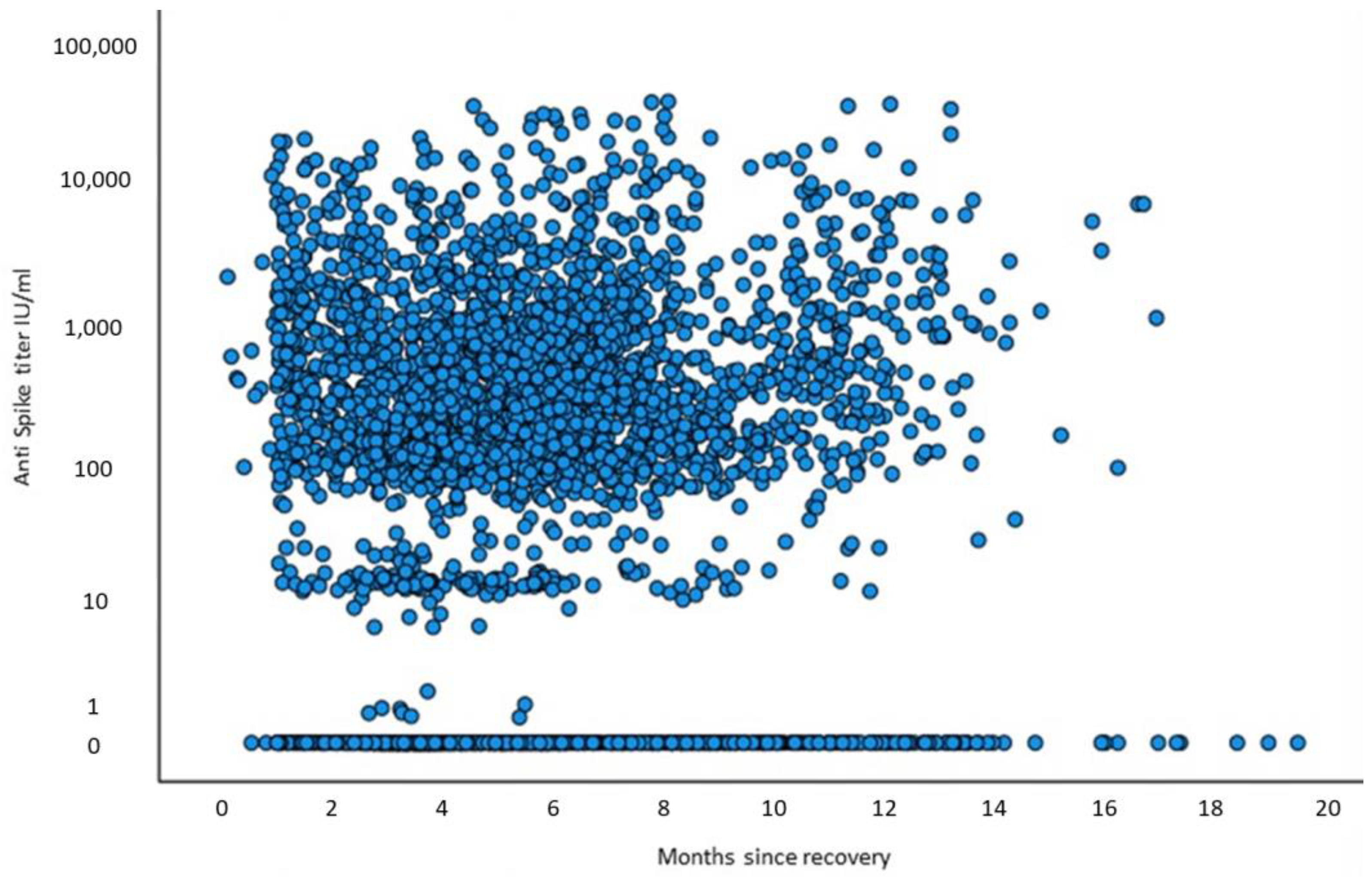
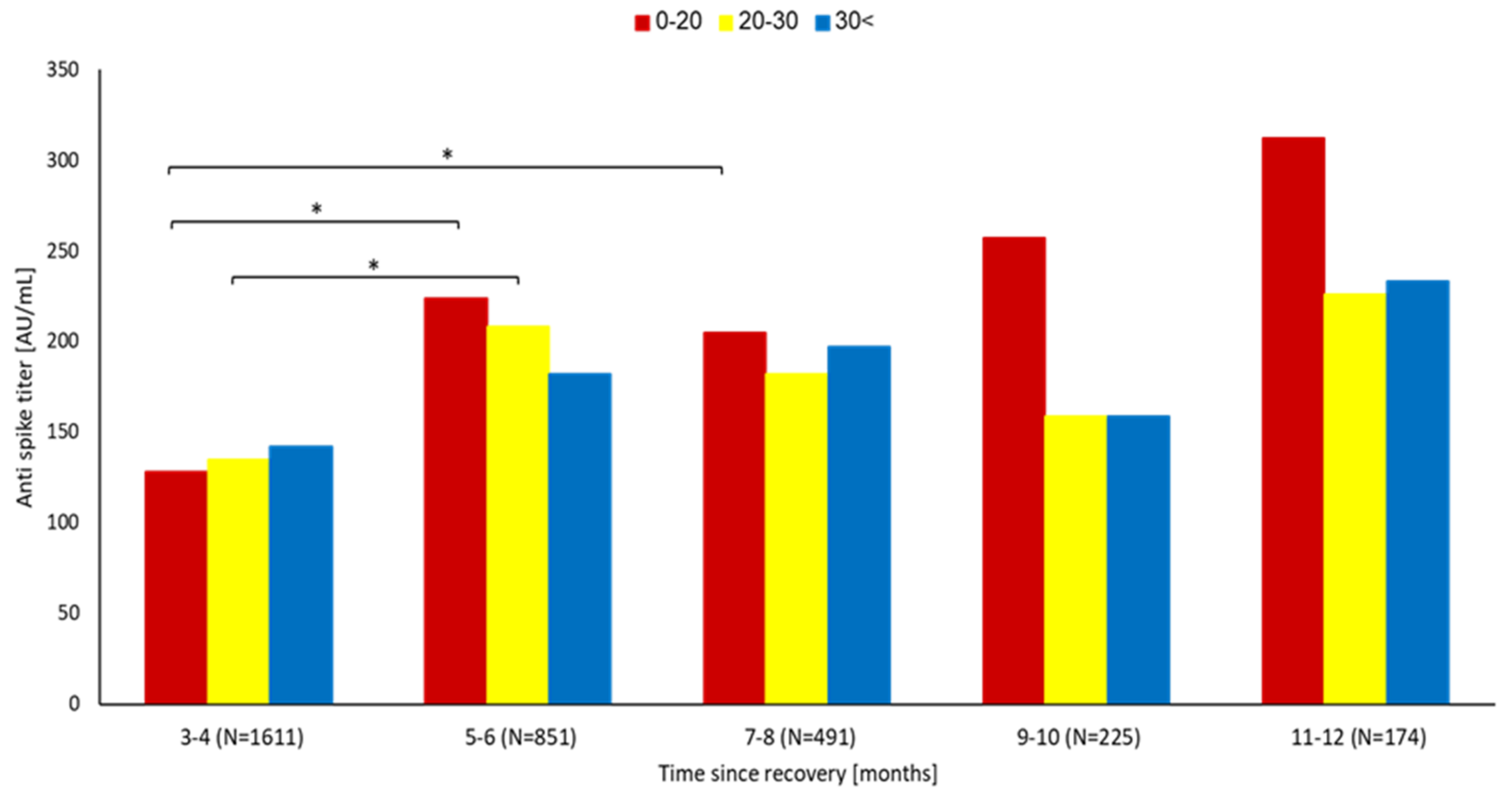
3. Results
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dan, J.M.; Mateus, J.; Kato, Y.; Hastie, K.M.; Yu, E.D.; Faliti, C.E.; Grifoni, A.; Ramirez, S.I.; Haupt, S.; Frazier, A.; et al. Immunological memory to SARS-CoV-2 assessed for up to 8 months after infection. Science 2021, 371, eabf4063. [Google Scholar] [CrossRef]
- Kuxdorf-Alkirata, N.; Maus, G.; Brückmann, D. Efficient calibration for robust indoor localization based on low-cost BLE sensors. In Proceedings of the 2019 IEEE 62nd International Midwest Symposium on Circuits and Systems (MWSCAS), Dallas, TX, USA, 4–7 August 2019; IEEE: Piscataway, NJ, USA, 2019; pp. 702–705. [Google Scholar]
- Wu, F.; Liu, M.; Wang, A.; Lu, L.; Wang, Q.; Gu, C.; Chen, J.; Wu, Y.; Xia, S.; Ling, Y.; et al. Evaluating the association of clinical characteristics with neutralizing antibody levels in patients who have recovered from mild COVID-19 in Shanghai, China. JAMA Intern. Med. 2020, 180, 1356–1362. [Google Scholar] [CrossRef]
- Seow, J.; Graham, C.; Merrick, B.; Acors, S.; Pickering, S.; Steel, K.J.; Hemmings, O.; O’Byrne, A.; Kouphou, N.; Galao, R.P.; et al. Longitudinal observation and decline of neutralizing antibody responses in the three months following SARS-CoV-2 infection in humans. Nat. Microbiol. 2020, 5, 1598–1607. [Google Scholar] [CrossRef]
- Long, Q.-X.; Jia, Y.-J.; Wang, X.; Deng, H.-J.; Cao, X.-X.; Yuan, J.; Fang, L.; Cheng, X.-R.; Luo, C.; He, A.-R.; et al. Immune memory in convalescent patients with asymptomatic or mild COVID-19. Cell Discov. 2021, 7, 18. [Google Scholar] [CrossRef] [PubMed]
- Shenai, M.B.; Rahme, R.; Noorchashm, H. Equivalency of protection from natural immunity in COVID-19 recovered versus fully vaccinated persons: A systematic review and pooled analysis. Cureus 2021, 13, e19102. [Google Scholar] [CrossRef] [PubMed]
- Leidi, A.; Koegler, F.; Dumont, R.; Dubos, R.; Zaballa, M.E.; Piumatti, G.; Coen, M.; Berner, A.; Farhoumand, P.D.; Vetter, P.; et al. Risk of reinfection after seroconversion to SARS-CoV-2: A population-based propensity-score matched cohort study. MedRxiv 2021. [Google Scholar] [CrossRef]
- Sheehan, M.M.; Reddy, A.J.; Rothberg, M.B. Reinfection rates among patients who previously tested positive for coronavirus disease 2019: A retrospective cohort study. Clin. Infect. Dis. 2021, 73, 1882–1886. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, Y.; Mandel, M.; Woodbridge, Y.; Fluss, R.; Novikov, I.; Yaari, R.; Ziv, A.; Freedman, L.; Huppert, A. Protection of previous SARS-CoV-2 infection is similar to that of BNT162b2 vaccine protection: A three-month nationwide experience from Israel. MedRxiv 2021. [Google Scholar] [CrossRef]
- Lumley, S.F.; Rodger, G.; Constantinides, B.; Sanderson, N.; Chau, K.K.; Street, T.L.; O’Donnell, D.; Howarth, A.; Hatch, S.B.; Marsden, B.D.; et al. An observational cohort study on the incidence of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection and B. 1.1. 7 variant infection in healthcare workers by antibody and vaccination status. Clin. Infect. Dis. 2022, 74, 1208–1219. [Google Scholar] [CrossRef] [PubMed]
- Gazit, S.; Shlezinger, R.; Perez, G.; Lotan, R.; Peretz, A.; Ben-Tov, A.; Cohen, D.; Muhsen, K.; Chodick, G.; Patalon, T. Comparing SARS-CoV-2 natural immunity to vaccine-induced immunity: Reinfections versus breakthrough infections. MedRxiv 2021. [Google Scholar] [CrossRef]
- Sabarathinam, C.; Mohan Viswanathan, P.; Senapathi, V.; Karuppannan, S.; Samayamanthula, D.R.; Gopalakrishnan, G.; Alagappan, R.; Bhattacharya, P. SARS-CoV-2 phase I transmission and mutability linked to the interplay of climatic variables: A global observation on the pandemic spread. Environ. Sci. Pollut. Res. 2022, 29, 72366–72383. [Google Scholar] [CrossRef]
- Pulendran, B.; Arunachalam, P.S.; O’Hagan, D.T. Emerging concepts in the science of vaccine adjuvants. Nat. Rev. Drug Discov. 2021, 20, 454–475. [Google Scholar] [CrossRef] [PubMed]
- Jude, E.B.; Ling, S.F.; Allcock, R.; Yeap, B.X.; Pappachan, J.M. Vitamin D deficiency is associated with higher hospitalization risk from COVID-19: A retrospective case-control study. J. Clin. Endocrinol. Metab. 2021, 106, e4708–e4715. [Google Scholar] [CrossRef] [PubMed]
- Campi, I.; Gennari, L.; Merlotti, D.; Mingiano, C.; Frosali, A.; Giovanelli, L.; Torlasco, C.; Pengo, M.F.; Heilbron, F.; Soranna, D.; et al. Vitamin D and COVID-19 severity and related mortality: A prospective study in Italy. BMC Infect. Dis. 2021, 21, 566. [Google Scholar] [CrossRef] [PubMed]
- Jaun, F.; Boesing, M.; Lüthi-Corridori, G.; Abig, K.; Makhdoomi, A.; Bloch, N.; Lins, C.; Raess, A.; Grillmayr, V.; Haas, P.; et al. High-dose vitamin D substitution in patients with COVID-19: Study protocol for a randomized, double-blind, placebo-controlled, multi-center study—VitCov Trial. Trials 2022, 23, 114. [Google Scholar] [CrossRef] [PubMed]
- Gönen, M.S.; Alaylıoğlu, M.; Durcan, E.; Özdemir, Y.; Şahin, S.; Konukoğlu, D.; Nohut, O.K.; Ürkmez, S.; Küçükece, B.; Balkan, İ.İ.; et al. Rapid and effective vitamin D supplementation may present better clinical outcomes in COVID-19 (SARS-CoV-2) patients by altering serum INOS1, IL1B, IFNg, cathelicidin-LL37, and ICAM1. Nutrients 2021, 13, 4047. [Google Scholar] [CrossRef]
- Murai, I.H.; Fernandes, A.L.; Sales, L.P.; Pinto, A.J.; Goessler, K.F.; Duran, C.S.; Silva, C.B.R.; Franco, A.S.; Macedo, M.B.; Dalmolin, H.H.H.; et al. Effect of a single high dose of vitamin D3 on hospital length of stay in patients with moderate to severe COVID-19: A randomized clinical trial. JAMA 2021, 325, 1053–1060. [Google Scholar] [CrossRef]
- Jolliffe, D.A.; Vivaldi, G.; Chambers, E.S.; Cai, W.; Li, W.; Faustini, S.E.; Gibbons, J.M.; Pade, C.; Coussens, A.K.; Richter, A.G.; et al. Vitamin D Supplementation Does Not Influence SARS-CoV-2 Vaccine Efficacy or Immunogenicity: Sub-Studies Nested within the CORONAVIT Randomised Controlled Trial. Nutrients 2022, 14, 3821. [Google Scholar] [CrossRef]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using Open SAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef]
- Grupel, D.; Gazit, S.; Schreiber, L.; Nadler, V.; Wolf, T.; Lazar, R.; Supino-Rosin, L.; Perez, G.; Peretz, A.; Ben Tov, A.; et al. Kinetics of SARS-CoV-2 anti-S IgG after BNT162b2 vaccination. Vaccine 2021, 39, 5337–5340. [Google Scholar] [CrossRef]
- French, D.; Gorgi, A.W.; Ihenetu, K.U.; Weeks, M.A.; Lynch, K.L.; Wu, A.H. Vitamin D status of county hospital patients assessed by the DiaSorin LIAISON® 25-hydroxyvitamin D assay. Clin. Chim. Acta 2011, 412, 258–262. [Google Scholar] [CrossRef]
- Rosecrans, R.; Dohnal, J.C. Seasonal vitamin D changes and the impact on health risk assessment. Clin. Biochem. 2014, 47, 670–672. [Google Scholar] [CrossRef]
- Moure, Z.; Rando-Segura, A.; Gimferrer, L.; Roig, G.; Pumarola, T.; Rodriguez-Garrido, V. Evaluation of the novel DiaSorin LIAISON. Enferm. Infecc. Microbiol. Clin. 2018, 36, 293–295. [Google Scholar] [CrossRef] [PubMed]
- Thuzar, M.; Young, K.; Ahmed, A.H.; Ward, G.; Wolley, M.; Guo, Z.; Gordon, R.D.; McWhinney, B.C.; Ungerer, J.P.; Stowasser, M. Diagnosis of primary aldosteronism by seated saline suppression test-variability between immunoassay and HPLC-MS/MS. J. Clin. Endocrinol. Metab. 2020, 105, e477–e483. [Google Scholar] [CrossRef] [PubMed]
- Hosseini, B.; Tremblay, C.L.; Longo, C.; Golchi, S.; White, J.; Quach, C.; Ste-Mari, L.-G.; Plat, R.; Ducharme, F. PRevention of COVID-19 with Oral Vitamin D supplemental Therapy in Essential healthCare Teams (PROTECT): Ancillary study of a randomised controlled trial. Trials 2022, 16, 1019. [Google Scholar]
- Israel, A.; Merzon, E.; Schäffer, A.A.; Shenhar, Y.; Green, I.; Golan-Cohen, A.; Ruppin, E.; Magen, E.; Vinker, S. Elapsed time since BNT162b2 vaccine and risk of SARS-CoV-2 infection: Test negative design study. BMJ 2021, 375, e067873. [Google Scholar] [CrossRef]
- Apanga, P.A.; Kumbeni, M.T. Adherence to COVID-19 preventive measures and associated factors among pregnant women in Ghana. Trop. Med. Int. Health 2021, 26, 656–663. [Google Scholar] [CrossRef]
- Chen, Y.H.; Wang, W.M.; Kao, T.W.; Chiang, C.P.; Hung, C.T.; Chen, W.L. Inverse relationship between serum vitamin D level and measles antibody titer: A cross-sectional analysis of NHANES, 2001–2004. PLoS ONE 2018, 13, e0207798. [Google Scholar] [CrossRef] [Green Version]
- Linder, N.; Abudi, Y.; Abdalla, W.; Badir, M.; Amitai, Y.; Samuels, J.; Mendelson, E.; Levy, I. Effect of season of inoculation on immune response to rubella vaccine in children. J. Trop. Pediatr. 2011, 57, 299–302. [Google Scholar] [CrossRef]
- Zimmerman, R.K.; Lin, C.J.; Raviotta, J.M.; Nowalk, M.P. Do vitamin D levels affect antibody titers produced in response to HPV vaccine? Hum. Vaccines Immunother. 2015, 11, 2345–2349. [Google Scholar] [CrossRef] [Green Version]
- Hewison, M.; Freeman, L.; Hughes, S.V.; Evans, K.N.; Bland, R.; Eliopoulos, A.G.; Kilby, M.D.; Moss, P.A.H.; Chakraverty, R. Differential regulation of vitamin D receptor and its ligand in human monocyte-derived dendritic cells. J. Immunol. 2003, 170, 5382–5390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alroy, I.; Towers, T.L.; Freedman, L.P. Transcriptional repression of the interleukin-2 gene by vitamin D3: Direct inhibition of NFATp/AP-1 complex formation by a nuclear hormone receptor. Mol. Cell. Biol. 1995, 15, 5789–5799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahon, B.D.; Wittke, A.; Weaver, V.; Cantorna, M.T. The targets of vitamin D depend on the differentiation and activation status of CD4 positive T cells. J. Cell. Biochem. 2003, 89, 922–932. [Google Scholar] [CrossRef]
- Chen, S.; Sims, G.P.; Chen, X.X.; Gu, Y.Y.; Chen, S.; Lipsky, P.E. Modulatory effects of 1, 25-dihydroxyvitamin D3 on human B cell differentiation. J. Immunol. 2007, 179, 1634–1647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Logue, J.K.; Franko, N.M.; McCulloch, D.J.; McDonald, D.; Magedson, A.; Wolf, C.R.; Chu, H.Y. Sequelae in adults at 6 months after COVID-19 infection. JAMA Netw. Open 2021, 4, e210830. [Google Scholar] [CrossRef] [PubMed]
- Gaebler, C.; Wang, Z.; Lorenzi, J.C.; Muecksch, F.; Finkin, S.; Tokuyama, M.; Cho, A.; Jankovic, M.; Schaefer-Babajew, D.; Oliveira, T.Y.; et al. Evolution of antibody immunity to SARS-CoV-2. Nature 2021, 591, 639–644. [Google Scholar] [CrossRef]
- Abu Fanne, R.; Lidawi, G.; Maraga, E.; Moed, M.; Roguin, A.; Meisel, S.R. Correlation between Baseline 25 (OH) Vitamin D Levels and Both Humoral Immunity and Breakthrough Infection Post-COVID-19 Vaccination. Vaccines 2022, 10, 2116. [Google Scholar] [CrossRef]
- Tan, L.; Wang, Q.; Zhang, D.; Ding, J.; Huang, Q.; Tang, Y.-Q.; Wang, Q.; Miao, H. Lymphopenia predicts disease severity of COVID-19: A descriptive and predictive study. Signal Transduct. Target. Ther. 2020, 5, 33. [Google Scholar] [CrossRef]
- Tarke, A.; Sidney, J.; Kidd, C.K.; Dan, J.M.; Ramirez, S.I.; Yu, E.D.; Mateus, J.; da Silva Antunes, R.; Moore, E.; Rubiro, P.; et al. Comprehensive analysis of T cell immunodominance and immunoprevalence of SARS-CoV-2 epitopes in COVID-19 cases. Cell Rep. Med. 2021, 2, 100204. [Google Scholar] [CrossRef]
- Saini, S.K.; Hersby, D.S.; Tamhane, T.; Povlsen, H.R.; Hernandez, S.P.A.; Nielsen, M.; Gang, A.O.; Hadrup, S.R. SARS-CoV-2 genome-wide T cell epitope mapping reveals immunodominance and substantial CD8+ T cell activation in COVID-19 patients. Sci. Immunol. 2021, 6, eabf7550. [Google Scholar] [CrossRef]
- Robbiani, D.F.; Gaebler, C.; Muecksch, F.; Lorenzi, J.C.C.; Wang, Z.; Cho, A.; Agudelo, M.; Barnes, C.O.; Gazumyan, A.; Finkin, S.; et al. Convergent antibody responses to SARS-CoV-2 in convalescent individuals. Nature 2020, 584, 437–442. [Google Scholar] [CrossRef] [PubMed]
- Muecksch, F.; Wise, H.; Batchelor, B.; Squires, M.; Semple, E.; Richardson, C.; McGuire, J.; Clearly, S.; Furrie, E.; Greig, N.; et al. Longitudinal Serological Analysis and Neutralizing Antibody Levels in Coronavirus Disease 2019 Convalescent Patients. J. Infect. Dis. 2021, 223, 389–398. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PCR Negative (n = 9810) | PCR Positive (n = 322) | p-Value | |
|---|---|---|---|
| Age | 40.9 ± 19.1 | 33.06 ± 16.56 | p < 0.0001 |
| Gender Male Female | (35.5%) (64.5%) | (34.5%) (65.5%) | p = 0.72 |
| Ethnicity Arab Orthodox Jewish Other | (34%) (22%) (44%) | (56.5%) (11.5%) (32%) | p < 0.0001 |
| 25(OH) D levels 10–20 20–30 >30 | (52%) (33%) (15%) | (55%) (33%) (12%) | p = 0.36 |
| Anxiety | (38%) | (40%) | p = 0.65 |
| Schizophrenia | (3%) | (6%) | p = 0.057 |
| Depression | (24%) | (27%) | p = 0.53 |
| Dementia | (3.7%) | (1.6%) | p = 0.33 |
| Nephrotic syndrome | (0.4%) | (0.8%) | p = 0.43 |
| Chronic Renal failure | (5.1%) | (4.7%) | p = 1.00 |
| CVA | (4.4%) | (0.8%) | p = 0.045 |
| CHF | (3.6%) | (2.4%) | p = 0.63 |
| PVD | (3.3%) | (0.8%) | p = 0.13 |
| IHD | (7.6%) | (5.5%) | p = 0.49 |
| Hyperlipidemia | (49%) | (31.5%) | p < 0.001 |
| HTN | (1.5%) | (0.8%) | p = 1.00 |
| DM | (11%) | (6.3%) | p = 0.11 |
| COPD | (7.3%) | (5.5%) | p = 0.60 |
| Asthma | (19.7%) | (28.3%) | p = 0.018 |
| SES 1–10 10–20 | (67%) (33%) | (76%) (24%) | p < 0.001 |
| Smoking status Active smoker Non smoker Former smoker | (11%) (88%) (1%) | (13%) (86%) (1%) | p = 0.43 |
| Anti-spike antibody titer <50 ≥50 | (30.5%) (69.5%) | (40%) (60%) | p = 0.051 |
| BMI <18.5 18.5–25 25–29.9 30+ | (5%) (35%) (31%) (29%) | (9%) (39%) (28%) (24%) | p = 0.004 |
| (25(OH)D) > 30 | (25(OH)D) 20–30 | (25(OH)D) < 20 | Overall | |
|---|---|---|---|---|
| 3–4 months | 1.20% | 3.96% | 3.26% | 3.1% |
| 5–6 months | 1.47% | 1.54% | 2.86% | 2.2% |
| 7–8 months | 1.78% | 2.33% | 3.58% | 2.9% |
| 9–10 months | 4.70% | 3.23% | 2.54% | 3.1% |
| 11–12 months | 7.15% | 7.14% | 5.38% | 6.2% |
| 3–12 months | 2.64% | 3.14% | 3.36% | 3.2% |
| 3–8 months | 1.53% | 2.54% | 3.34% | 2.7% |
| 9–12 months | 5.39% | 4.50% | 3.39% | 4.3% |
| Anti-Spike Antibody < 50 (n = 1006) | Anti-Spike Antibody ≥ 50 (n = 2345) | Total (n = 3351) | p-Value | |
|---|---|---|---|---|
| Age | 44.9 ± 19.0 | 43.7 ± 17.6 | 44.05 ± 18.1 | 0.071 |
| Gender Male Female | (35.1%) (64.9%) | (34.0%) (66.0%) | (34.4%) (65.6%) | 0.55 |
| Ethnicity Arab Orthodox Jewish Other | (34.6%) (14.9%) (50.5%) | (36.6%) (15.4%) (48.1%) | (36.0%) (15.2%) (48.8%) | 0.43 |
| 25(OH)D level 0–20 20–30 >30 | (46.0%) (37.2%) (16.8%) | (50.2%) (34.4%) (15.4%) | (48.9%) (35.2%) (15.8%) | 0.093 |
| PCR positive | (4.5%) | (2.5%) | (3.1%) | 0.02 |
| Anxiety | (38.6%) | (41.3%) | (40.4%) | 0.26 |
| Schizophrenia | (1.4%) | (2.6%) | (2.2%) | 0.11 |
| Depression | (22.2%) | (23.0%) | (22.7%) | 0.73 |
| Dementia | (1.2%) | (1.8%) | (1.6%) | 0.45 |
| Nephrotic syndrome | (0.8%) | (0.5%) | (0.6%) | 0.53 |
| Chronic Renal failure | (5.4%) | (4.5%) | (4.8%) | 0.38 |
| CVA | (3.0%) | (4.1%) | (3.8%) | 0.21 |
| CHF | (2.3%) | (2.5%) | (2.4%) | 1.00 |
| PVD | (3.4%) | (3.5%) | (3.5%) | 1.00 |
| IHD | (7.8%) | (6.5%) | (6.9%) | 0.30 |
| Hyperlipidemia | (53.0%) | (51.3%) | (51.9%) | 0.50 |
| HTN | (1.1%) | (1.4%) | (1.3%) | 0.68 |
| DM | (12.1%) | (10.2%) | (10.8%) | 0.19 |
| COPD | (7.5%) | (6.9%) | (7.1%) | 0.64 |
| Asthma | (20.2%) | (17.9%) | (18.7%) | 0.22 |
| SES 1–10 10–20 | (59.5%) (40.5%) | (62.7%) (37.3%) | (61.7%) (38.3%) | 0.10 |
| Smoking status Active smoker Nonsmoker Former smoker | (9.9%) (88.5%) (1.5%) | (8.5%) (90.1%) (1.4%) | (8.9%) (89.7%) (1.4%) | 0.44 |
| BMI 16.5–18.5 18.5–24.9 25–29.9 30+ | (3.7%) (31.1%) (35.1%) (30.1%) | (3.1%) (35.3%) (31.9%) (29.7%) | (3.3%) (34.0%) (32.8%) (29.8%) | 0.11 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abu Fanne, R.; Moed, M.; Kedem, A.; Lidawi, G.; Maraga, E.; Mohsen, F.; Roguin, A.; Meisel, S.-R. SARS-CoV-2 Infection-Blocking Immunity Post Natural Infection: The Role of Vitamin D. Vaccines 2023, 11, 475. https://doi.org/10.3390/vaccines11020475
Abu Fanne R, Moed M, Kedem A, Lidawi G, Maraga E, Mohsen F, Roguin A, Meisel S-R. SARS-CoV-2 Infection-Blocking Immunity Post Natural Infection: The Role of Vitamin D. Vaccines. 2023; 11(2):475. https://doi.org/10.3390/vaccines11020475
Chicago/Turabian StyleAbu Fanne, Rami, Mahmud Moed, Aviv Kedem, Ghalib Lidawi, Emad Maraga, Fady Mohsen, Ariel Roguin, and Simcha-Ron Meisel. 2023. "SARS-CoV-2 Infection-Blocking Immunity Post Natural Infection: The Role of Vitamin D" Vaccines 11, no. 2: 475. https://doi.org/10.3390/vaccines11020475