SARS-CoV-2 Antibody Dynamics in Healthcare Workers after mRNA Vaccination

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Recruitment, and Participants
2.2. Laboratory Methods
2.3. Clinical Assessment
2.4. Aims
2.5. Statistical Methods
3. Results
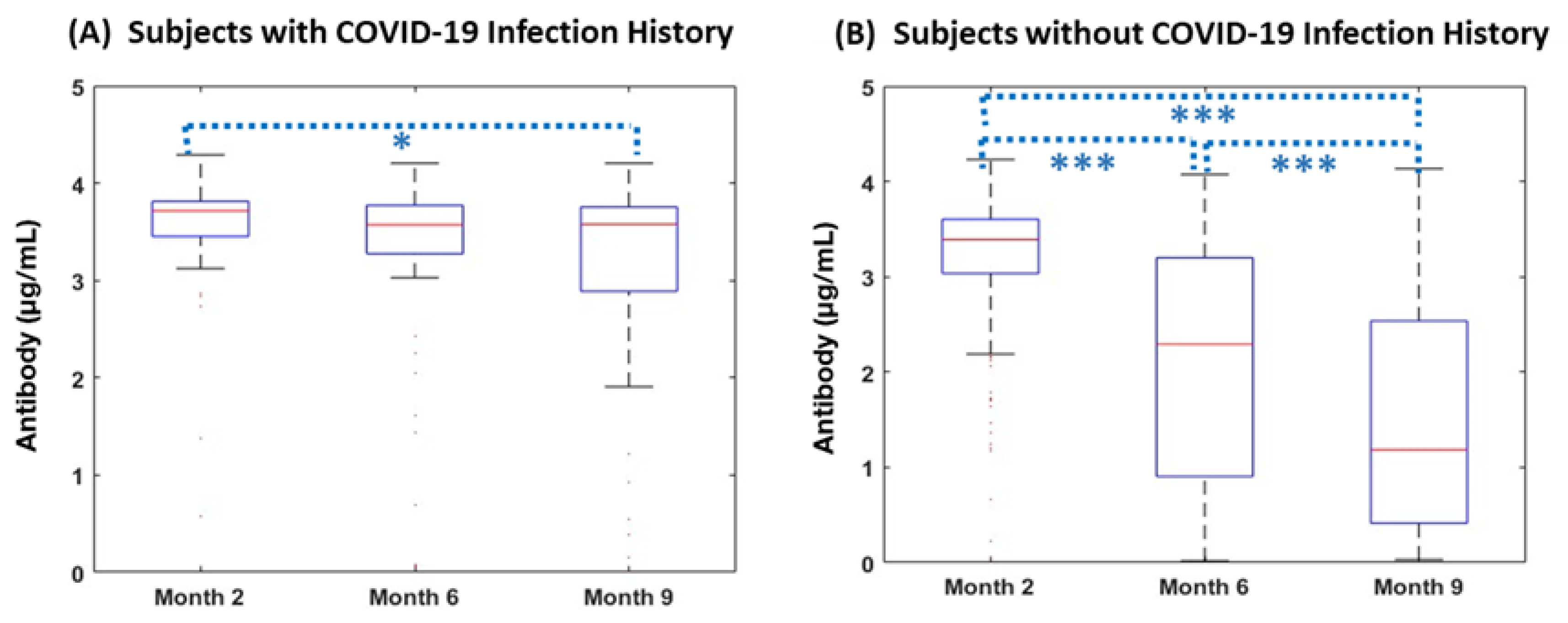
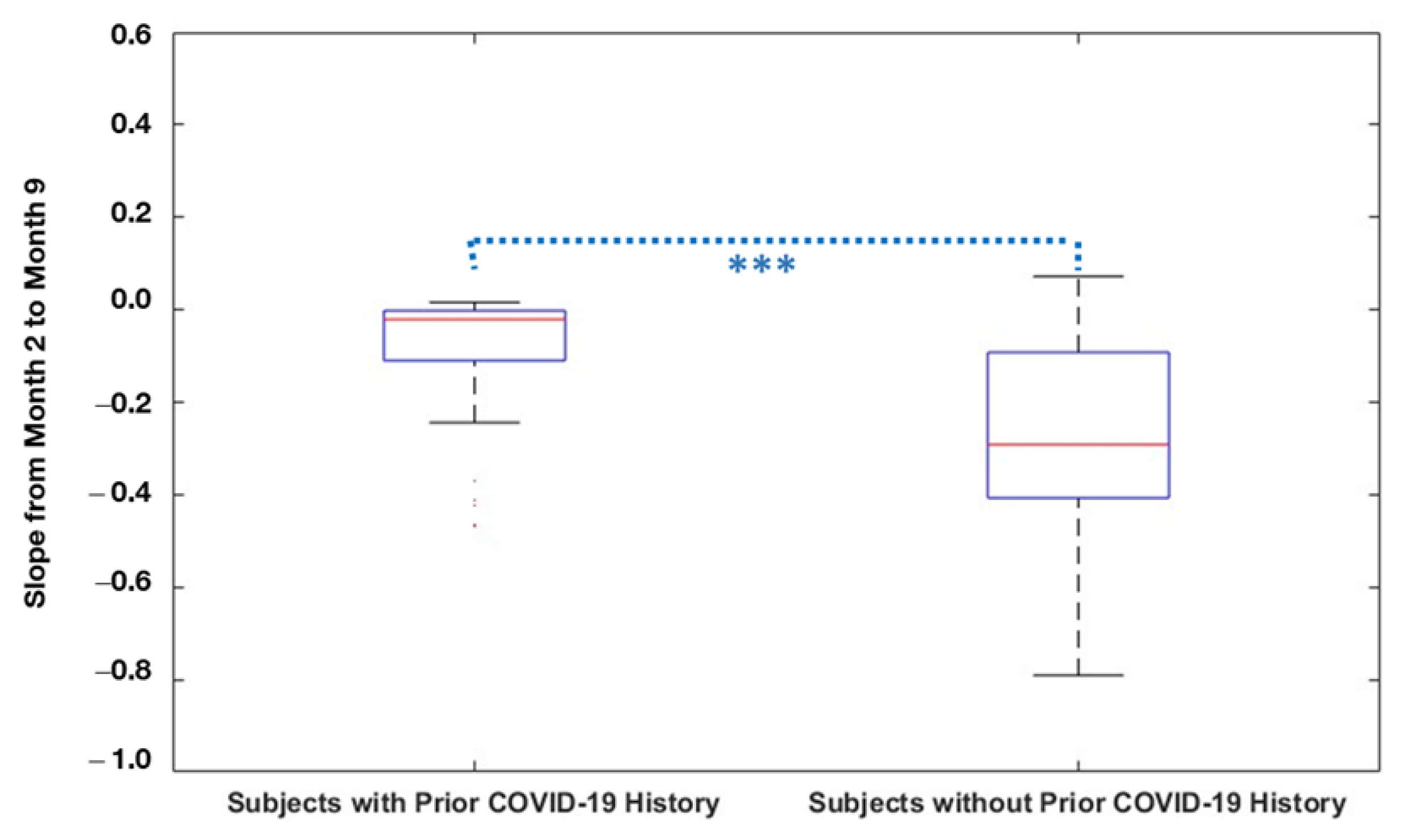
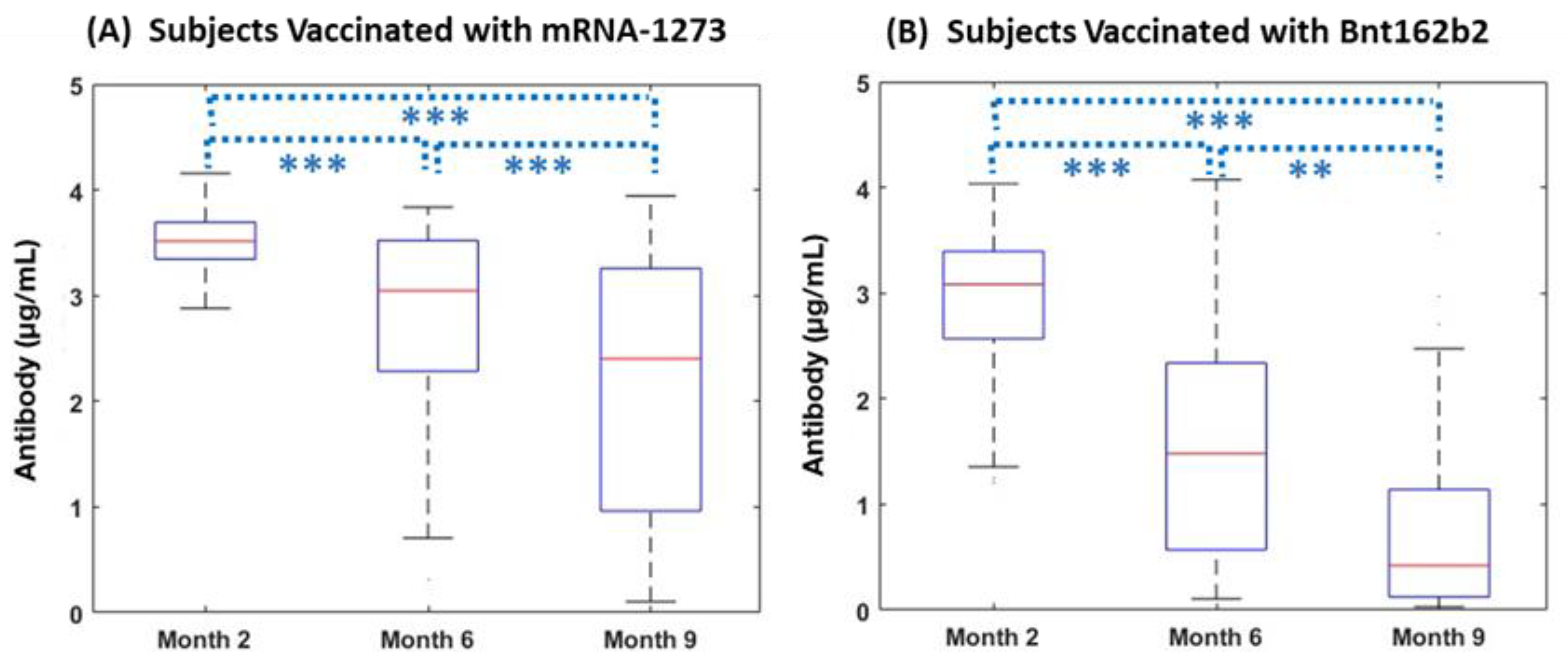
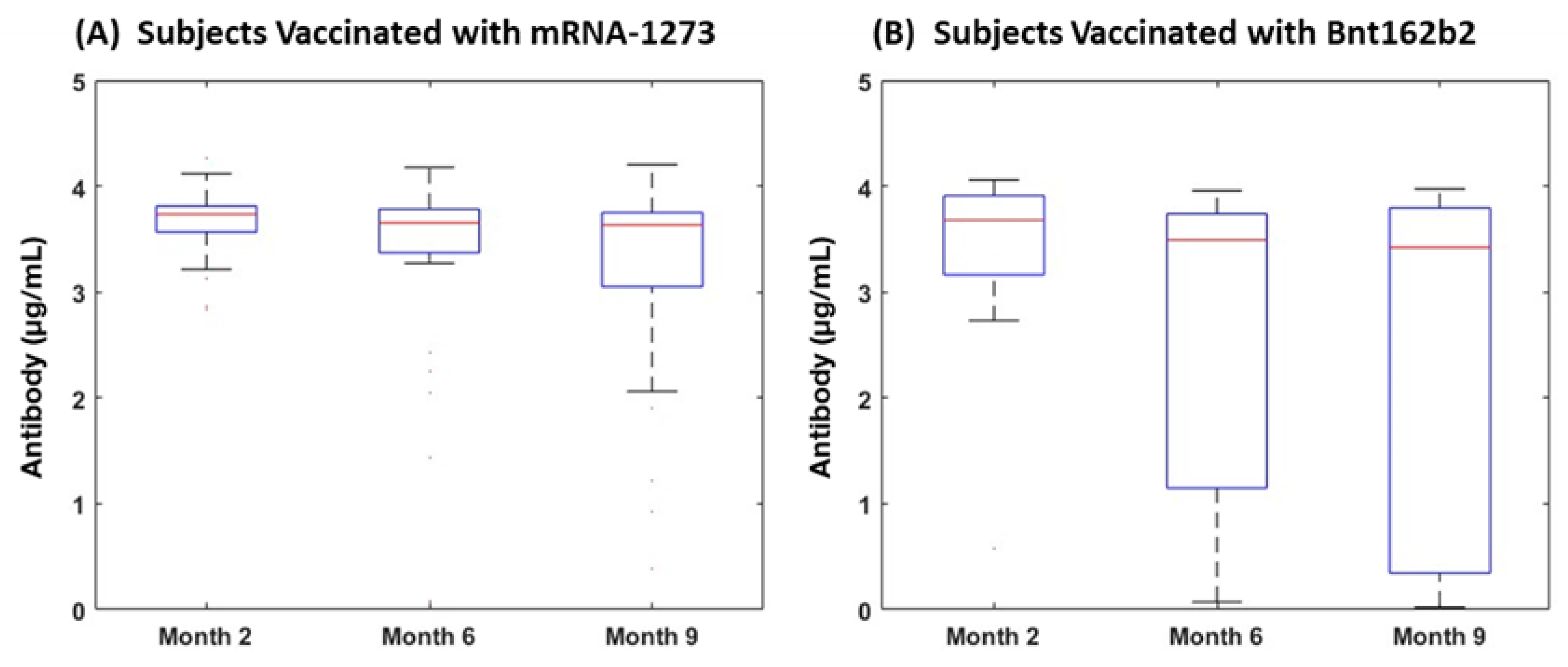
3.1. Antibody Dynamics
3.2. Subjects without Pre-Vaccination COVID-19 Infection History
3.3. Subjects with COVID-19 Infection History
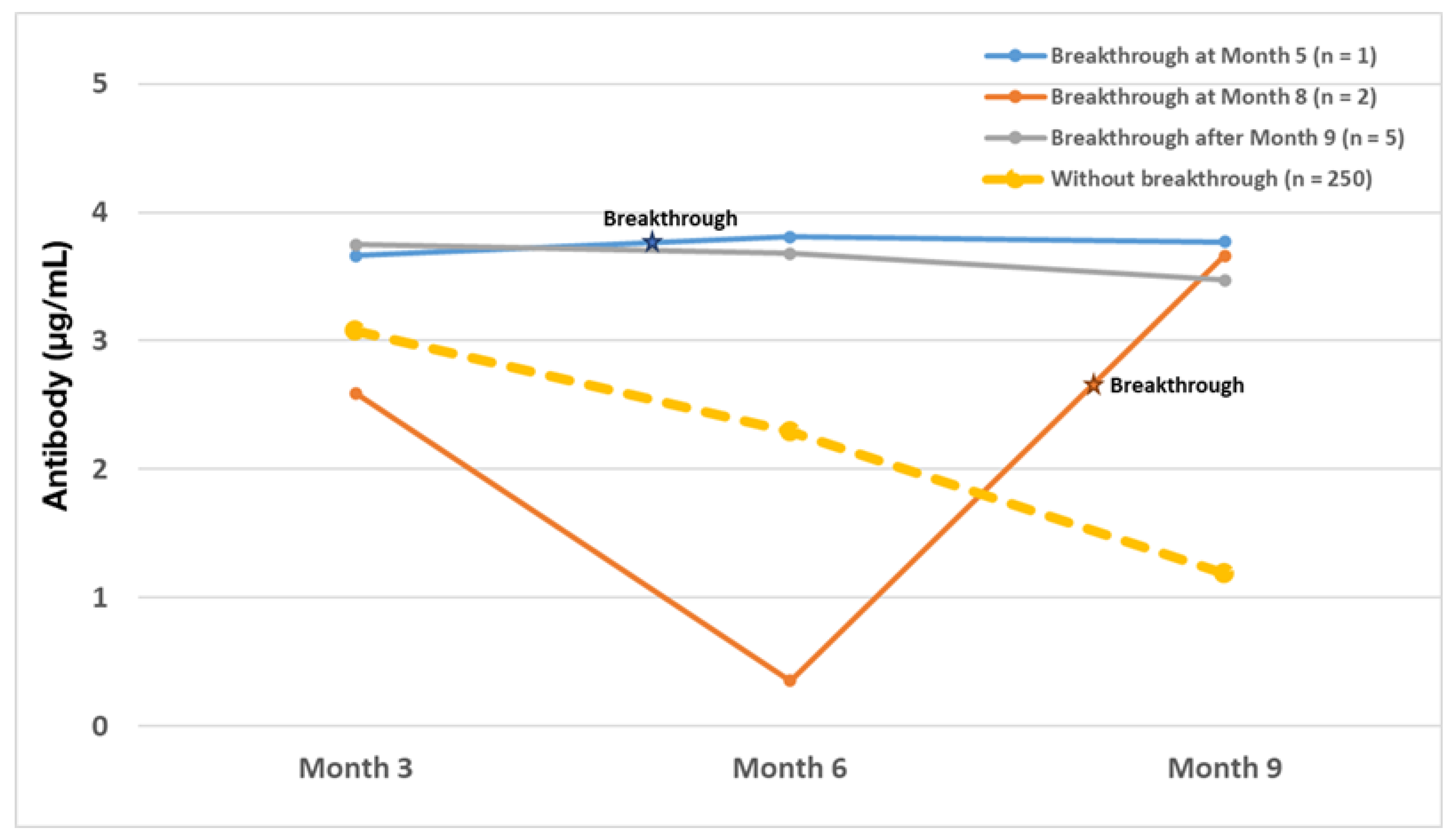
3.4. Clinical Infections after Vaccination
3.5. Vaccine-Associated Adverse Events
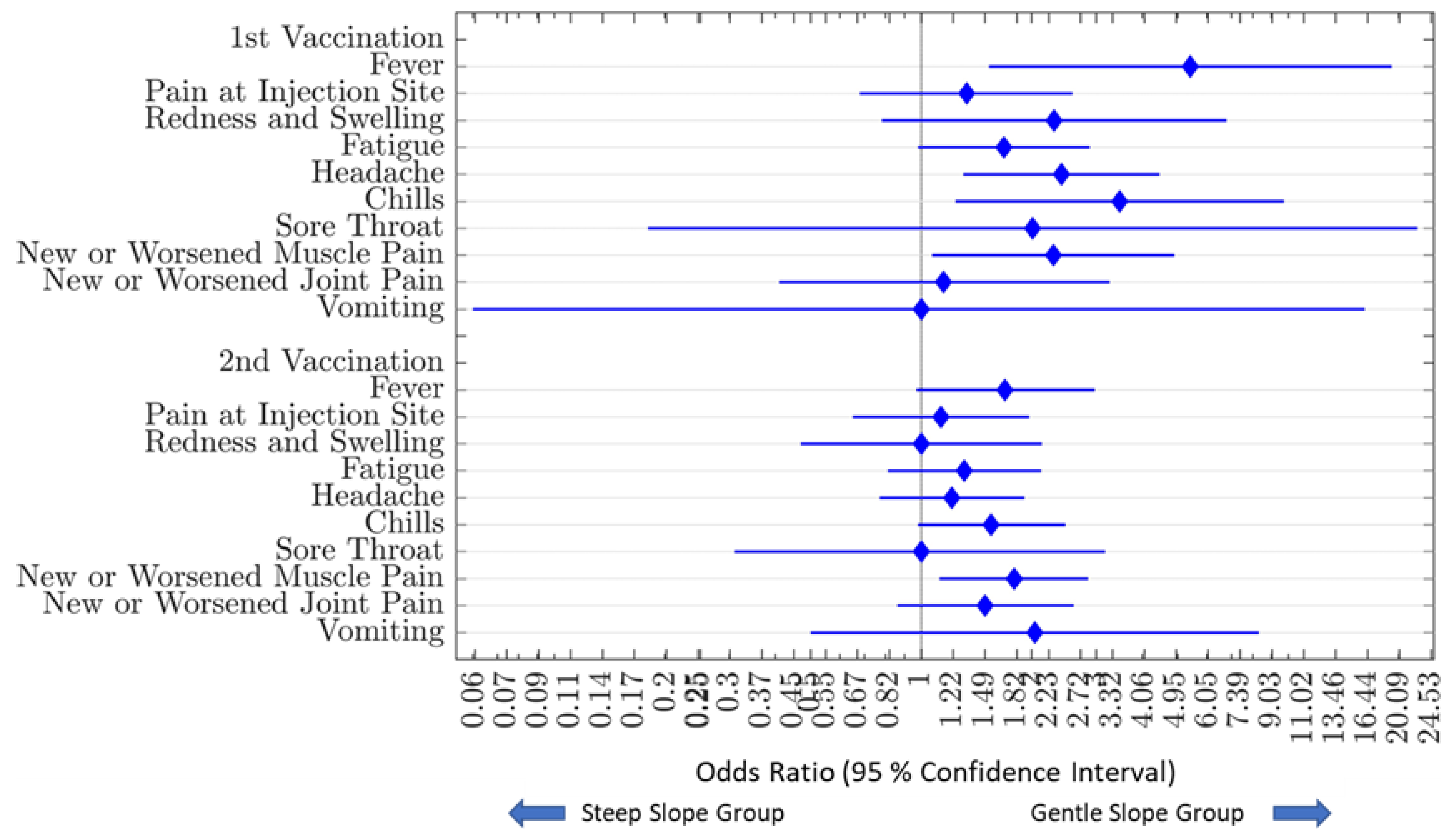
3.5.1. Relationship of Vaccine-Associated Adverse Events and Antibody Decay Characteristics
3.5.2. Impact of Prior COVID Illness on Adverse Events and Antibody Dynamics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. WHO Coronavirus Dashboard. Available online: https://covid19.who.int/ (accessed on 15 July 2022).
- Department, H.W. The Impact of COVID-19 on Health and Care Workers: A Closer Look at Deaths; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Woon, Y.L.; Lee, Y.L.; Chong, Y.M.; Ayub, N.A.; Krishnabahawan, S.L.; Lau, J.F.W.; Subramaniam-Kalianan, R.; Sam, I.C.; Chan, Y.F.; Sevalingam, R.K.; et al. Serology surveillance of SARS-CoV-2 antibodies among healthcare workers in COVID-19 designated facilities in Malaysia. Lancet Reg. Health-West. Pac. 2021, 9, 100123. [Google Scholar] [CrossRef] [PubMed]
- Talbot, L.R.; Romeiser, J.L.; Spitzer, E.D.; Gan, T.J.; Singh, S.M.; Fries, B.C.; Bennett-Guerrero, E. Prevalence of IgM and IgG antibodies to SARS-CoV-2 in health care workers at a tertiary care New York hospital during the Spring COVID-19 surge. Perioper. Med. 2021, 10, 7. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.K.; Minn, D.; Song, D.Y.; Lee, C.H.; Ryoo, N.H.; Jeon, C.H.; Song, K.E.; Suh, J.S.; Chang, S.H. Prevalence of SARS-CoV-2 Antibody in 2,935 Healthcare Workers at 6 Major Hospitals, Daegu, Korea. J. Korean Med. Sci. 2021, 36, e294. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Basteiro, A.L.; Moncunill, G.; Tortajada, M.; Vidal, M.; Guinovart, C.; Jimenez, A.; Santano, R.; Sanz, S.; Mendez, S.; Llupia, A.; et al. Seroprevalence of antibodies against SARS-CoV-2 among health care workers in a large Spanish reference hospital. Nat. Commun. 2020, 11, 3500. [Google Scholar] [CrossRef] [PubMed]
- Mishra, B.; Behera, B.; Singh, A.K.; Mohapatra, P.R.; Patro, B.K.; Panigrahi, M.K.; Pillai, J.S.K.; Barik, S.; Mahapatra, A.; Mohanty, S.; et al. Seroprevalence of SARS-CoV-2 antibodies among healthcare workers in a teaching hospital in Eastern India. J. Fam. Med. Prim. Care 2021, 10, 2974–2979. [Google Scholar] [CrossRef] [PubMed]
- Milazzo, L.; Lai, A.; Pezzati, L.; Oreni, L.; Bergna, A.; Conti, F.; Meroni, C.; Minisci, D.; Galli, M.; Corbellino, M.; et al. Dynamics of the seroprevalence of SARS-CoV-2 antibodies among healthcare workers at a COVID-19 referral hospital in Milan, Italy. Occup. Environ. Med. 2021, 78, 541–547. [Google Scholar] [CrossRef]
- Larribere, L.; Gordejeva, J.; Kuhnhenn, L.; Kurscheidt, M.; Pobiruchin, M.; Vladimirova, D.; Martin, M.; Roser, M.; Schramm, W.; Martens, U.M.; et al. Assessment of SARS-CoV-2 Infection among Healthcare Workers of a German COVID-19 Treatment Center. Int. J. Environ. Res. Public Health 2021, 18, 7057. [Google Scholar] [CrossRef] [PubMed]
- Bueno-Hernandez, N.; Carrillo-Ruiz, J.D.; Mendez-Garcia, L.A.; Rizo-Tellez, S.A.; Viurcos-Sanabria, R.; Santoyo-Chavez, A.; Marquez-Franco, R.; Aguado-Garcia, A.; Baltazar-Lopez, N.; Tomita-Cruz, Y.; et al. High Incidence Rate of SARS-CoV-2 Infection in Health Care Workers at a Dedicated COVID-19 Hospital: Experiences of the Pandemic from a Large Mexican Hospital. Healthcare 2022, 10, 896. [Google Scholar] [CrossRef]
- Allen, N.; Riain, U.N.; Conlon, N.; Ferenczi, A.; Carrion Martin, A.I.; Domegan, L.; Walsh, C.; Doherty, L.; O’Farrelly, C.; Higgins, E.; et al. Prevalence of antibodies to SARS-CoV-2 in Irish hospital healthcare workers. Epidemiol. Infect. 2021, 149, e157. [Google Scholar] [CrossRef]
- Wilkins, J.T.; Gray, E.L.; Wallia, A.; Hirschhorn, L.R.; Zembower, T.R.; Ho, J.; Kalume, N.; Agbo, O.; Zhu, A.; Rasmussen-Torvik, L.J.; et al. Seroprevalence and Correlates of SARS-CoV-2 Antibodies in Health Care Workers in Chicago. Open Forum. Infect. Dis. 2021, 8, ofaa582. [Google Scholar] [CrossRef]
- Kantele, A.; Laaveri, T.; Kareinen, L.; Pakkanen, S.H.; Blomgren, K.; Mero, S.; Patjas, A.; Virtanen, J.; Uusitalo, R.; Lappalainen, M.; et al. SARS-CoV-2 infections among healthcare workers at Helsinki University Hospital, Finland, spring 2020: Serosurvey, symptoms and risk factors. Travel Med. Infect. Dis. 2021, 39, 101949. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, L.; Ferrari, P.; Piumatti, G.; Jovic, S.; Rodriguez, B.F.; Mele, F.; Giacchetto-Sasselli, I.; Terrot, T.; Silacci-Fregni, C.; Cameroni, E.; et al. Risk assessment and seroprevalence of SARS-CoV-2 infection in healthcare workers of COVID-19 and non-COVID-19 hospitals in Southern Switzerland. Lancet Reg. Health-Eur. 2021, 1, 100013. [Google Scholar] [CrossRef] [PubMed]
- Smallwood, N.; Harrex, W.; Rees, M.; Willis, K.; Bennett, C.M. COVID-19 infection and the broader impacts of the pandemic on healthcare workers. Respirology 2022, 27, 411–426. [Google Scholar] [CrossRef]
- Malipiero, G.; D’Agaro, P.; Segat, L.; Moratto, A.; Villalta, D. Long-term decay of anti-RBD IgG titers after BNT162b2 vaccination is not mirrored by loss of neutralizing bioactivity against SARS-CoV-2. Clin. Chim. Acta 2022, 524, 11–17. [Google Scholar] [CrossRef]
- Salazar, E.; Kuchipudi, S.V.; Christensen, P.A.; Eagar, T.; Yi, X.; Zhao, P.; Jin, Z.; Long, S.W.; Olsen, R.J.; Chen, J.; et al. Convalescent plasma anti-SARS-CoV-2 spike protein ectodomain and receptor-binding domain IgG correlate with virus neutralization. J. Clin. Investig. 2020, 130, 6728–6738. [Google Scholar] [CrossRef] [PubMed]
- Naaber, P.; Tserel, L.; Kangro, K.; Sepp, E.; Jurjenson, V.; Adamson, A.; Haljasmagi, L.; Rumm, A.P.; Maruste, R.; Karner, J.; et al. Dynamics of antibody response to BNT162b2 vaccine after six months: A longitudinal prospective study. Lancet Reg. Health-Eur. 2021, 10, 100208. [Google Scholar] [CrossRef]
- Pilishvili, T.; Gierke, R.; Fleming-Dutra, K.E.; Farrar, J.L.; Mohr, N.M.; Talan, D.A.; Krishnadasan, A.; Harland, K.K.; Smithline, H.A.; Hou, P.C.; et al. Effectiveness of mRNA Covid-19 Vaccine among U.S. Health Care Personnel. N. Engl. J. Med. 2021, 385, e90. [Google Scholar] [CrossRef] [PubMed]
- Rivelli, A.; Fitzpatrick, V.; Blair, C.; Copeland, K.; Richards, J. Incidence of COVID-19 reinfection among Midwestern healthcare employees. PLoS ONE 2022, 17, e0262164. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services. Common Terminology Criteria for Adverse Events (CTCAE) Version 4.0; National Institutes of Health: Bethesda, MD, USA, 2009.
- COVID-19: Your Health: People with Certain Medical Conditions. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html#immunocompromised (accessed on 4 September 2022).
- Campo, F.; Venuti, A.; Pimpinelli, F.; Abril, E.; Blandino, G.; Conti, L.; De Virgilio, A.; De Marco, F.; Di Noia, V.; Di Domenico, E.G.; et al. Antibody Persistence 6 Months Post-Vaccination with BNT162b2 among Health Care Workers. Vaccines 2021, 9, 1125. [Google Scholar] [CrossRef]
- Kiefer, M.K.; Allen, K.D.; Russo, J.R.; Ma’ayeh, M.; Gee, S.E.; Kniss, D.; Cackovic, M.; Costantine, M.M.; Rood, K.M. Decline in Sars-CoV-2 antibodies over 6-month follow-up in obstetrical healthcare workers. Am. J. Reprod. Immunol. 2021, 86, e13490. [Google Scholar] [CrossRef]
- Marot, S.; Malet, I.; Leducq, V.; Zafilaza, K.; Sterlin, D.; Planas, D.; Gothland, A.; Jary, A.; Dorgham, K.; Bruel, T.; et al. Rapid decline of neutralizing antibodies against SARS-CoV-2 among infected healthcare workers. Nat. Commun. 2021, 12, 844. [Google Scholar] [CrossRef] [PubMed]
- Worsley, C.M.; van der Mescht, M.A.; Hoffmann, D.; Meyer, P.W.A.; Ueckermann, V.; Rossouw, T.M. Decline in antibody responses to SARS-CoV-2 post-vaccination poses a risk to health care workers. J. Infect. 2022, 85, 334–363. [Google Scholar] [CrossRef] [PubMed]
- Bajema, K.L.; Dahl, R.M.; Evener, S.L.; Prill, M.M.; Rodriguez-Barradas, M.C.; Marconi, V.C.; Beenhouwer, D.O.; Holodniy, M.; Lucero-Obusan, C.; Brown, S.T.; et al. Comparative Effectiveness and Antibody Responses to Moderna and Pfizer-BioNTech COVID-19 Vaccines among Hospitalized Veterans—Five Veterans Affairs Medical Centers, United States, February 1-September 30, 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 1700–1705. [Google Scholar] [CrossRef] [PubMed]
- Steensels, D.; Pierlet, N.; Penders, J.; Mesotten, D.; Heylen, L. Comparison of SARS-CoV-2 Antibody Response Following Vaccination With BNT162b2 and mRNA-1273. J. Am. Med. Assoc. 2021, 326, 1533–1535. [Google Scholar] [CrossRef]
- Decru, B.; Van Elslande, J.; Steels, S.; Van Pottelbergh, G.; Godderis, L.; Van Holm, B.; Bossuyt, X.; Van Weyenbergh, J.; Maes, P.; Vermeersch, P. IgG Anti-Spike Antibodies and Surrogate Neutralizing Antibody Levels Decline Faster 3 to 10 Months After BNT162b2 Vaccination Than After SARS-CoV-2 Infection in Healthcare Workers. Front. Immunol. 2022, 13, 909910. [Google Scholar] [CrossRef]
- Buonfrate, D.; Piubelli, C.; Gobbi, F.; Martini, D.; Bertoli, G.; Ursini, T.; Moro, L.; Ronzoni, N.; Angheben, A.; Rodari, P.; et al. Antibody response induced by the BNT162b2 mRNA COVID-19 vaccine in a cohort of health-care workers, with or without prior SARS-CoV-2 infection: A prospective study. Clin. Microbiol. Infect. 2021, 27, 1845–1850. [Google Scholar] [CrossRef]
- Hall, V.J.; Foulkes, S.; Charlett, A.; Atti, A.; Monk, E.J.M.; Simmons, R.; Wellington, E.; Cole, M.J.; Saei, A.; Oguti, B.; et al. SARS-CoV-2 infection rates of antibody-positive compared with antibody-negative health-care workers in England: A large, multicentre, prospective cohort study (SIREN). Lancet 2021, 397, 1459–1469. [Google Scholar] [CrossRef]
- Padoan, A.; Cosma, C.; Della Rocca, F.; Barbaro, F.; Santarossa, C.; Dall’Olmo, L.; Galla, L.; Cattelan, A.; Cianci, V.; Basso, D.; et al. A cohort analysis of SARS-CoV-2 anti-spike protein receptor binding domain (RBD) IgG levels and neutralizing antibodies in fully vaccinated healthcare workers. Clin. Chem. Lab. Med. 2022, 60, 1110–1115. [Google Scholar] [CrossRef]
- Vicenti, I.; Basso, M.; Gatti, F.; Scaggiante, R.; Boccuto, A.; Zago, D.; Modolo, E.; Dragoni, F.; Parisi, S.G.; Zazzi, M. Faster decay of neutralizing antibodies in never infected than previously infected healthcare workers three months after the second BNT162b2 mRNA COVID-19 vaccine dose. Int. J. Infect. Dis. 2021, 112, 40–44. [Google Scholar] [CrossRef]
- Raw, R.K.; Rees, J.; Kelly, C.A.; Wroe, C.; Chadwick, D.R. Prior COVID-19 infection is associated with increased Adverse Events (AEs) after the first, but not the second, dose of the BNT162b2/Pfizer vaccine. Vaccine 2022, 40, 418–423. [Google Scholar] [CrossRef]
- Van Elslande, J.; Weemaes, M.; Godderis, L.; Van Pottelbergh, G.; Bossuyt, X.; Vermeersch, P. IgG anti-spike antibody levels in healthcare workers with and without prior COVID-19 up to 3 months after BNT162b2 vaccination. Diagn. Microbiol. Infect. Dis. 2022, 102, 115638. [Google Scholar] [CrossRef]
- Vassallo, A.; Shajahan, S.; Harris, K.; Hallam, L.; Hockham, C.; Womersley, K.; Woodward, M.; Sheel, M. Sex and Gender in COVID-19 Vaccine Research: Substantial Evidence Gaps Remain. Front. Glob. Women’s Health 2021, 2, 761511. [Google Scholar] [CrossRef] [PubMed]
- Izak, M.; Stoyanov, E.; Dezuraev, K.; Shinar, E. Correlation of Anti-SARS-CoV-2 S1-specificIgG antibody levels and adverse events following vaccination with BNT162b2 mRNA COVID-19 vaccine in healthcare workers. Vaccine 2022, 40, 428–431. [Google Scholar] [CrossRef] [PubMed]
- Hermann, E.A.; Lee, B.; Balte, P.P.; Xanthakis, V.; Kirkpatrick, B.D.; Cushman, M.; Oelsner, E. Association of Symptoms After COVID-19 Vaccination With Anti-SARS-CoV-2 Antibody Response in the Framingham Heart Study. J. Am. Med. Assoc. Netw. Open 2022, 5, e2237908. [Google Scholar] [CrossRef] [PubMed]
- Rieke, G.J.; van Bremen, K.; Bischoff, J.; ToVinh, M.; Monin, M.B.; Schlabe, S.; Raabe, J.; Kaiser, K.M.; Finnemann, C.; Odainic, A.; et al. Natural Killer Cell-Mediated Antibody-Dependent Cellular Cytotoxicity Against SARS-CoV-2 After Natural Infection Is More Potent Than After Vaccination. J. Infect. Dis. 2022, 225, 1688–1693. [Google Scholar] [CrossRef]
- Agrati, C.; Castilletti, C.; Goletti, D.; Sacchi, A.; Bordoni, V.; Mariotti, D.; Notari, S.; Matusali, G.; Meschi, S.; Petrone, L.; et al. Persistent Spike-specific T cell immunity despite antibody reduction after 3 months from SARS-CoV-2 BNT162b2-mRNA vaccine. Sci. Rep. 2022, 12, 6687. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Breakthrough Infection (n = 8) | Non-Breakthrough Infection (n = 288) | All (n = 296) | |||
|---|---|---|---|---|---|
| Baseline PCR Negative (n = 5) | Baseline PCR Positive (n = 3) | Baseline PCR Negative (n = 245) | Baseline PCR Positive (n = 43) | ||
| Female | 2 (40%) | 1 (33%) | 201 (82%) | 33 (75%) | 237 (80%) |
| Age (years) | 38.4 ± 10.7 | 35.3 ± 6.1 | 44.2 ± 12.3 | 41.9 ± 11.9 | 43.7 ± 12.2 |
| Ethnicity | |||||
| African American | 5 (2%) | 5 (2%) | |||
| Asian | 16 (7%) | 1 (2%) | 17 (6%) | ||
| Caucasian | 5 (100%) | 3 (100%) | 203 (83%) | 37 (86%) | 248 (83%) |
| Hispanic | 15 (6%) | 5 (11%) | 20 (7%) | ||
| Vaccine Product | |||||
| mRNA-1273 | 3 (60%) | 3 (100%) | 105 (43%) | 26 (60%) | 137 (46%) |
| bnt162b2 | 2 (40%) | 140 (57%) | 17 (40%) | 159 (54%) | |
| Heart Disease | 4 (2%) | 1 (2%) | 5 (2%) | ||
| Lung Disease | 2 (1%) | 2 (1%) | |||
| Diabetes | 5 (2%) | 5 (2%) | |||
| Obesity | 9 (4%) | 9 (3%) | |||
| Lifetime Smoking or Vaping history | 9 (4%) | 2 (5%) | 11 (4%) | ||
| Pregnancy | 1 (0%) | 1 (0%) | |||
| Moderate or Severe Immunocompromise | 8 (3%) | 8 (3%) | |||
| N (%) | Subjects without Prior COVID-19 History | Subjects with Prior COVID-19 History | Total |
|---|---|---|---|
| Slope with Gentle Decline | 108 (44%) | 39 (85%) | 147 (50%) |
| Slope with Steep Decline | 139 (56%) | 7 (15%) | 146 (50%) |
| Grand Total | 247 | 46 | 293 |
| N (%) | mRNA-1273 | Bnt162b2 | Total |
|---|---|---|---|
| Slope with Gentle Decline | 64 (60%) | 44 (31%) | 108 (44%) |
| Slope with Steep Decline | 43 (40%) | 96 (69%) | 139 (56%) |
| Total (%) | 107 | 140 | 247 |
| N (%) | mRNA-1273 | Bnt162b2 | Total |
|---|---|---|---|
| Gentle Decline | 24 (83%) | 15 (88%) | 39 (85%) |
| Steep Decline | 5 (17%) | 2 (12%) | 7 (15%) |
| Total (%) | 29 | 17 | 46 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dieckhaus, K.D.; Kim, M.-J.; Shen, J.-B.; Liang, T.S.; Kleinberg, M.J.; Siedlarz, K.M.; Banach, D.B.; Metersky, M.L.; Fuller, R.P.; Mortensen, E.M.; et al. SARS-CoV-2 Antibody Dynamics in Healthcare Workers after mRNA Vaccination. Vaccines 2023, 11, 358. https://doi.org/10.3390/vaccines11020358
Dieckhaus KD, Kim M-J, Shen J-B, Liang TS, Kleinberg MJ, Siedlarz KM, Banach DB, Metersky ML, Fuller RP, Mortensen EM, et al. SARS-CoV-2 Antibody Dynamics in Healthcare Workers after mRNA Vaccination. Vaccines. 2023; 11(2):358. https://doi.org/10.3390/vaccines11020358
Chicago/Turabian StyleDieckhaus, Kevin D., Min-Jung Kim, Jian-Bing Shen, Tina S. Liang, Michael J. Kleinberg, Kristen M. Siedlarz, David B. Banach, Mark L. Metersky, Rob P. Fuller, Eric M. Mortensen, and et al. 2023. "SARS-CoV-2 Antibody Dynamics in Healthcare Workers after mRNA Vaccination" Vaccines 11, no. 2: 358. https://doi.org/10.3390/vaccines11020358