
Safety Following COVID-19 Booster Vaccine with BNT162b2 Compared to mRNA-1273 in Solid Cancer Patients Previously Vaccinated with ChAdOx1 or CoronaVac
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Outcomes
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Vaccine Safety
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yang, L.; Chai, P.; Yu, J.; Fan, X. Effects of cancer on patients with COVID-19: A systematic review and meta-analysis of 63,019 participants. Cancer Biol. Med. 2021, 18, 298–307. [Google Scholar] [CrossRef] [PubMed]
- Kuderer, N.M.; Choueiri, T.K.; Shah, D.P.; Shyr, Y.; Rubinstein, S.M.; Rivera, D.R.; Shete, S.; Hsu, C.-Y.; Desai, A.; de Lima Lopes, G., Jr.; et al. Clinical impact of COVID-19 on patients with cancer (CCC19): A cohort study. Lancet 2020, 395, 1907–1918. [Google Scholar] [CrossRef] [PubMed]
- Liang, W.; Guan, W.; Chen, R.; Wang, W.; Li, J.; Xu, K.; Li, C.; Ai, Q.; Lu, W.; Liang, H.; et al. Cancer patients in SARS-CoV-2 infection: A nationwide analysis in China. Lancet Oncol. 2020, 21, 335–337. [Google Scholar] [CrossRef] [PubMed]
- Giannakoulis, V.G.; Papoutsi, E.; Siempos, I.I. Effect of Cancer on Clinical Outcomes of Patients With COVID-19: A Meta-Analysis of Patient Data. JCO Glob. Oncol. 2020, 6, 799–808. [Google Scholar] [CrossRef]
- Sheikh, A.; McMenamin, J.; Taylor, B.; Robertson, C. SARS-CoV-2 Delta VOC in Scotland: Demographics, risk of hospital admission, and vaccine effectiveness. Lancet 2021, 397, 2461–2462. [Google Scholar] [CrossRef]
- Dejnirattisai, W.; Huo, J.; Zhou, D.; Zahradník, J.; Supasa, P.; Liu, C.; Duyvesteyn, H.M.E.; Ginn, H.M.; Mentzer, A.J.; Tuekprakhon, A.; et al. SARS-CoV-2 Omicron-B.1.1.529 leads to widespread escape from neutralizing antibody responses. Cell 2022, 185, 467–484.e415. [Google Scholar] [CrossRef]
- Thomas, S.J.; Moreira, E.D., Jr.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Polack, F.P.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine through 6 Months. N. Engl. J. Med. 2021, 385, 1761–1773. [Google Scholar] [CrossRef]
- Chemaitelly, H.; Tang, P.; Hasan, M.R.; AlMukdad, S.; Yassine, H.M.; Benslimane, F.M.; Al Khatib, H.A.; Coyle, P.; Ayoub, H.H.; Al Kanaani, Z.; et al. Waning of BNT162b2 Vaccine Protection against SARS-CoV-2 Infection in Qatar. N. Engl. J. Med. 2021, 385, e83. [Google Scholar] [CrossRef]
- Goldberg, Y.; Mandel, M.; Bar-On, Y.M.; Bodenheimer, O.; Freedman, L.; Haas, E.J.; Milo, R.; Alroy-Preis, S.; Ash, N.; Huppert, A. Waning Immunity after the BNT162b2 Vaccine in Israel. N. Engl. J. Med. 2021, 385, e85. [Google Scholar] [CrossRef]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.-M.; et al. COVID-19 Vaccine Effectiveness against the Omicron (B.1.1.529) Variant. N. Engl. J. Med. 2022, 386, 1532–1546. [Google Scholar] [CrossRef]
- Bruxvoort, K.J.; Sy, L.S.; Qian, L.; Ackerson, B.K.; Luo, Y.; Lee, G.S.; Tian, Y.; Florea, A.; Aragones, M.; Tubert, J.E.; et al. Effectiveness of mRNA-1273 against delta, mu, and other emerging variants of SARS-CoV-2: Test negative case-control study. BMJ 2021, 375, e068848. [Google Scholar] [CrossRef] [PubMed]
- Abu-Raddad, L.J.; Chemaitelly, H.; Ayoub, H.H.; AlMukdad, S.; Yassine, H.M.; Al-Khatib, H.A.; Smatti, M.K.; Tang, P.; Hasan, M.R.; Coyle, P.; et al. Effect of mRNA Vaccine Boosters against SARS-CoV-2 Omicron Infection in Qatar. N. Engl. J. Med. 2022, 386, 1804–1816. [Google Scholar] [CrossRef] [PubMed]
- Butt, A.A.; Talisa, V.B.; Shaikh, O.S.; Omer, S.B.; Mayr, F.B. Relative Vaccine SARS-CoV-2 RNA Vaccine Booster Dose Against the Omicron Variant. Clin. Infect. Dis. 2022, 75, 2161–2168. [Google Scholar] [CrossRef] [PubMed]
- Arbel, R.; Hammerman, A.; Sergienko, R.; Friger, M.; Peretz, A.; Netzer, D.; Yaron, S. BNT162b2 Vaccine Booster and Mortality Due to COVID-19. N. Engl. J. Med. 2021, 385, 2413–2420. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. COVID-19 Vaccine Boosters. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/booster-shot.html (accessed on 1 October 2021).
- Lasagna, A.; Bergami, F.; Lilleri, D.; Percivalle, E.; Quaccini, M.; Alessio, N.; Comolli, G.; Sarasini, A.; Sammartino, J.C.; Ferrari, A.; et al. Immunogenicity and safety after the third dose of BNT162b2 anti-SARS-CoV-2 vaccine in patients with solid tumors on active treatment: A prospective cohort study. ESMO Open 2022, 7, 100458. [Google Scholar] [CrossRef]
- Ligumsky, H.; Dor, H.; Etan, T.; Golomb, I.; Nikolaevski-Berlin, A.; Greenberg, I.; Halperin, T.; Angel, Y.; Henig, O.; Spitzer, A.; et al. Immunogenicity and safety of BNT162b2 mRNA vaccine booster in actively treated patients with cancer. Lancet Oncol. 2022, 23, 193–195. [Google Scholar] [CrossRef]
- Auster, O.; Finkel, U.; Dagan, N.; Barda, N.; Laufer, A.; Balicer, R.D.; Ben-Shachar, S. Short-term Adverse Events After the Third Dose of the BNT162b2 mRNA COVID-19 Vaccine in Adults 60 Years or Older. JAMA Netw. Open 2022, 5, e227657. [Google Scholar] [CrossRef]
- Luangdilok, S.; Wanchaijiraboon, P.; Pakvisal, N.; Susiriwatananont, T.; Zungsontiporn, N.; Sriuranpong, V.; Sainamthip, P.; Suntronwong, N.; Vichaiwattana, P.; Wanlapakorn, N.; et al. Immunogenicity after a Third COVID-19 mRNA Booster in Solid Cancer Patients Who Previously Received the Primary Heterologous CoronaVac/ChAdOx1 Vaccine. Vaccines 2022, 10, 1613. [Google Scholar] [CrossRef]
- Luangdilok, S.; Wanchaijiraboon, P.; Pakvisal, N.; Susiriwatananont, T.; Zungsontiporn, N.; Sriuranpong, V.; Namkanisorn, T.; Sainamthip, P.; Suntronwong, N.; Vichaiwattana, P.; et al. Immunogenicity and Omicron Neutralization Following a Third COVID-19 Vaccination in Solid Cancer Patients Previously Primed with Two Doses of Chadox1 Vaccine: A Prospective Cohort Study. Lancet 2022. [Google Scholar] [CrossRef]
- Teeyapun, N.; Luangdilok, S.; Pakvisal, N.; Sainamthip, P.; Mingmalairak, S.; Poovorawan, N.; Sitthideatphaiboon, P.; Parinyanitikul, N.; Sriuranpong, V.; Namkanisorn, T.; et al. Immunogenicity of ChAdOx1-nCoV-19 vaccine in solid malignancy patients by treatment regimen versus healthy controls: A prospective, multicenter observational study. Eclinicalmedicine 2022, 52, 101608. [Google Scholar] [CrossRef]
- Wanchaijiraboon, P.; Teeyapun, N.; Pakvisal, N.; Sainamthip, P.; Susiriwatananont, T.; Zungsontiporn, N.; Suntronwong, N.; Vichaiwattana, P.; Klinsawat, W.; Wanlapakorn, N.; et al. Durability of Immune Response to ChAdOx1-nCoV-19 Vaccine in Solid Cancer Patients Undergoing Anticancer Treatment. Vaccines 2022, 10, 1662. [Google Scholar] [CrossRef] [PubMed]
- FDA US. Toxicity Grading Scale for Healthy Adult and Adolescent Volunteers Enrolled in Preventive Vaccine Clinical Trials, Guidance for Industry. Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/toxicity-grading-scale-healthy-adult-and-adolescent-volunteers-enrolled-preventive-vaccine-clinical (accessed on 1 October 2021).
- Munro, A.P.S.; Janani, L.; Cornelius, V.; Aley, P.K.; Babbage, G.; Baxter, D.; Bula, M.; Cathie, K.; Chatterjee, K.; Dodd, K.; et al. Safety and immunogenicity of seven COVID-19 vaccines as a third dose (booster) following two doses of ChAdOx1 nCov-19 or BNT162b2 in the UK (COV-BOOST): A blinded, multicentre, randomised, controlled, phase 2 trial. Lancet 2021, 398, 2258–2276. [Google Scholar] [CrossRef] [PubMed]
- Beatty, A.L.; Peyser, N.D.; Butcher, X.E.; Cocohoba, J.M.; Lin, F.; Olgin, J.E.; Pletcher, M.J.; Marcus, G.M. Analysis of COVID-19 Vaccine Type and Adverse Effects Following Vaccination. JAMA Netw. Open 2021, 4, e2140364. [Google Scholar] [CrossRef]
- Nachtigall, I.; Bonsignore, M.; Hohenstein, S.; Bollmann, A.; Günther, R.; Kodde, C.; Englisch, M.; Ahmad-Nejad, P.; Schröder, A.; Glenz, C.; et al. Effect of gender, age and vaccine on reactogenicity and incapacity to work after COVID-19 vaccination: A survey among health care workers. BMC Infect. Dis. 2022, 22, 291. [Google Scholar] [CrossRef]
- Rolfes, L.; Härmark, L.; Kant, A.; van Balveren, L.; Hilgersom, W.; van Hunsel, F. COVID-19 vaccine reactogenicity—A cohort event monitoring study in the Netherlands using patient reported outcomes. Vaccine 2022, 40, 970–976. [Google Scholar] [CrossRef]
- Mehta, N.; Sales, R.M.; Babagbemi, K.; Levy, A.D.; McGrath, A.L.; Drotman, M.; Dodelzon, K. Unilateral axillary Adenopathy in the setting of COVID-19 vaccine. Clin. Imaging 2021, 75, 12–15. [Google Scholar] [CrossRef]
- Lehman, C.D.; D’Alessandro, H.A.; Mendoza, D.P.; Succi, M.D.; Kambadakone, A.; Lamb, L.R. Unilateral Lymphadenopathy After COVID-19 Vaccination: A Practical Management Plan for Radiologists Across Specialties. J. Am. Coll. Radiol. 2021, 18, 843–852. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Özütemiz, C.; Potter, D.A.; Özütemiz, A.; Steinberger, D. Lymphadenopathy after the Third COVID-19 Vaccine. Curr. Probl. Cancer Case Rep. 2021, 4, 100127. [Google Scholar] [CrossRef]
- So, A.C.P.; McGrath, H.; Ting, J.; Srikandarajah, K.; Germanou, S.; Moss, C.; Russell, B.; Monroy-Iglesias, M.; Dolly, S.; Irshad, S.; et al. COVID-19 Vaccine Safety in Cancer Patients: A Single Centre Experience. Cancers 2021, 13, 3573. [Google Scholar] [CrossRef] [PubMed]
- Pakvisal, N.; Sainamthip, P.; Teeyapun, N.; Luangdilok, S.; Wanlapakorn, N.; Yorsaeng, R.; Poovorawan, Y.; Pakvisal, P.; Susiriwatananont, T.; Zungsontiporn, N.; et al. Vaccine-Related adverse events following AZD1222 (ChAdOx1-nCoV-19) COVID-19 vaccine in solid malignancy patients receiving cancer treatment, as compared to age-matched healthy controls. Hum. Vaccines Immunother. 2022, 18, 2094149. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | All Patients n = 370 | BNT162b2 n = 172 | mRNA-1273 n = 198 | p-Value |
|---|---|---|---|---|
| Age, mean +/− SD <65 years, n (%) ≥65 years, n (%) | 59.61 +/− 12.3 229 (61.9) 141 (38.1) | 61.12 +/− 11.9 98 (57) 74 (43) | 58.30 +/− 12.5 131 (66.2) 67 (33.8) | 0.027 0.070 |
| Female, n (%) | 213 (57.6) | 108 (62.8) | 105 (53) | 0.058 |
| ECOG PS, n (%) 0–1 2 | 335 (90.5) 35 (9.5) | 156 (90.7) 16 (9.3) | 179 (90.4) 19 (9.6) | 0.923 |
| BMI, n (%) <18.5 (underweight) ≥18.5 | 46 (12.4) 324 (87.6) | 19 (11) 153 (89) | 27 (13.6) 171 (86.4) | 0.451 |
| Comorbidity No Hypertension Dyslipidemia Diabetes Chronic liver disease Cerebrovascular disease Chronic obstructive pulmonary disease Chronic kidney disease Coronary heart disease Gout Autoimmune disease | 175 (47.3) 128 (34.6) 81 (21.9) 66 (17.8) 19 (5.1) 12 (3.2) 7 (1.9) 6 (1.6) 5 (1.4) 5 (1.4) 3 (0.8) | 66 (38.4) 67 (39) 46 (26.7) 40 (23.3) 11 (6.4) 7 (4.1) 1 (0.6) 6 (3.5) 3 (1.7) 1 (0.6) 3 (1.7) | 109 (55.1) 61 (30.8) 35 (17.7) 26 (13.1) 8 (4) 5 (2.5) 6 (3) 0 2 (1) 4 (2) 0 | 0.001 0.100 0.041 0.012 0.311 0.400 0.088 0.008 0.542 0.231 0.059 |
| Current disease status, n (%) Early Locally advanced Metastasis | 111 (30) 51 (13.8) 208 (56.2) | 41 (23.8) 13 (7.6) 118 (68.6) | 70 (35.4) 38 (19.2) 90 (45.4) | <0.001 |
| Cancer type, n (%) Breast Colorectal Lung Head neck Hepatocellular carcinoma Gastrointestinal stromal tumor Pancreaticobiliary Esophagus Gastric Prostate Bladder Melanoma Renal cell carcinoma Other | 123 (33.2) 79 (21.4) 73 (19.7) 17 (4.5) 15 (4.1) 11 (3) 10 (2.7) 7 (1.9) 5 (1.4) 5 (1.4) 5 (1.4) 5 (1.4) 4 (1.1) 11 (3) | 47 (27.3) 29 (16.9) 54 (31.4) 6 (3.4) 8 (4.7) 10 (5.8) 3 (1.7) 0 1 (0.6) 1 (0.6) 1 (0.6) 3 (1.7) 4 (2.3) 5 (2.9) | 76 (38.4) 50 (25.3) 19 (9.6) 11 (5.5) 7 (3.5) 1 (0.5) 7 (3.5) 7 (3.5) 4 (2) 4 (2) 4 (2) 2 (1) 0 6 (3) | <0.001 |
| Cancer treatment, n (%) No treatment Targeted therapy/Hormonal therapy Chemotherapy Immunotherapy Radiation | 63 (17) 157 (42.4) 124 (33.5) 26 (7) 18 (4.9) | 23 (13.4) 89 (51.7) 42 (24.4) 18 (10.5) 5 (2.9) | 40 (20.2) 68 (34.3) 82 (41.4) 8 (4) 13 (6.6) | <0.001 0.103 |
| Corticosteroid use, n (%) No Yes | 261 (70.5) 109 (29.5) | 133 (77.3) 39 (22.7) | 128 (64.6) 70 (35.4) | 0.008 |
| Type of primary vaccine, n (%) ChAdOx1/ChAdOx1 CoronaVac/ChAdOx1 | 326 (88.1) 44 (11.9) | 152 (88.4) 20 (11.6) | 174 (87.9) 24 (12.1) | 0.884 |
| Interval between 2nd to 3rd vaccine, n (%) 3 months >3–6 months | 30 (8.1) 340 (91.9) | 6 (3.5) 166 (96.5) | 24 (12.1) 174 (87.9) | 0.002 |
| Adverse Events | All Patients n = 370 | BNT162b2 n = 172 | mRNA-1273 n = 198 | p-Value |
|---|---|---|---|---|
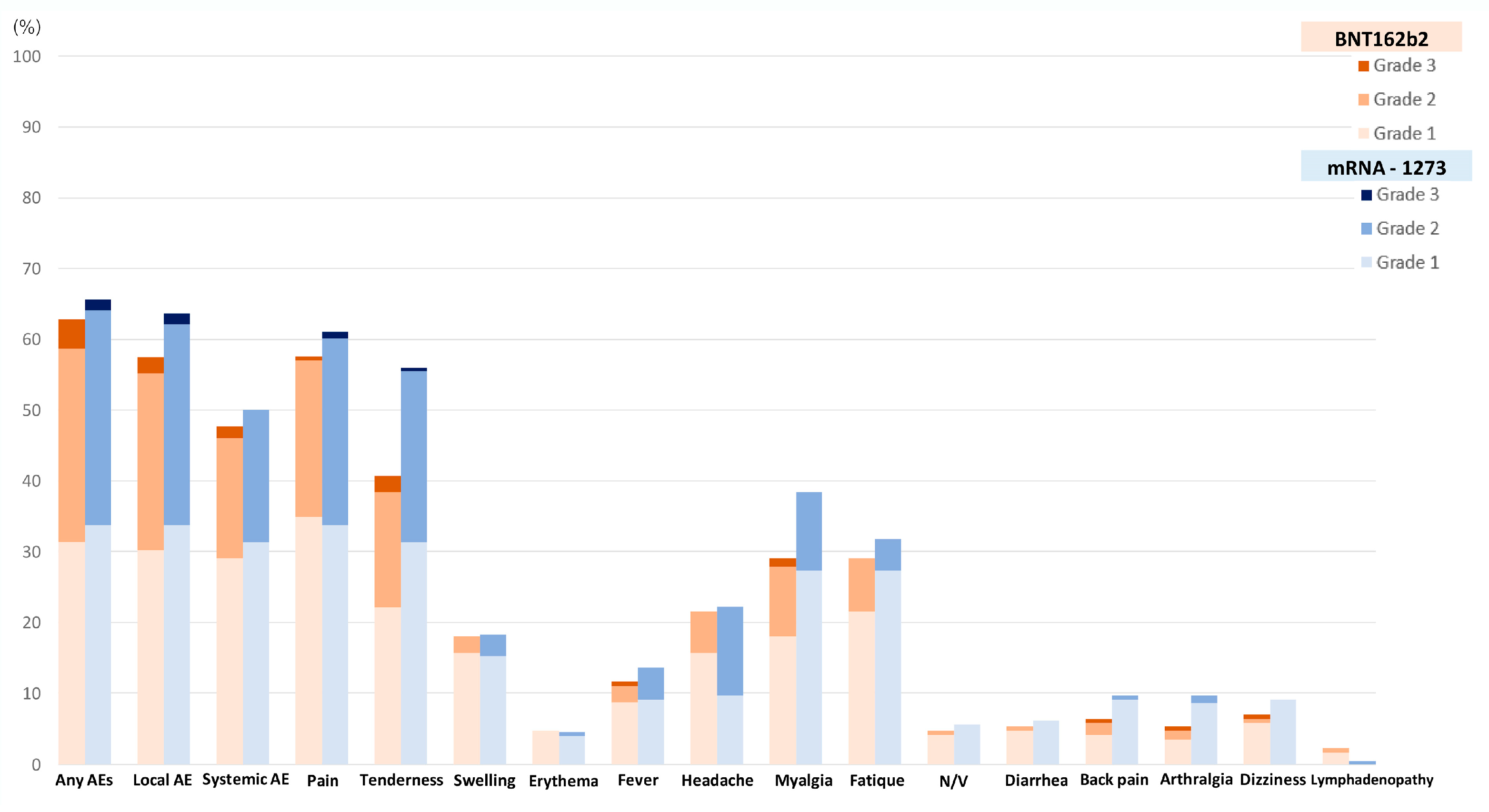
| Any AE, n a (%) Grade 1/2/3 | 238 (64.3) 121/107/10 (50.8/45/4.2) | 108 (62.8) 54/47/7 (50/43.5/6.5) | 130 (65.7) 67/60/3 (51.5/46.2/2.3) | 0.566 0.410 |
| Local AE, n a (%) Grade 1/2/3 | 225 (60.8) 119/99/7 (52.9/44/3.1) | 99 (57.6) 52/43/4 (52.5/43.4/4.1) | 126 (63.6) 67/56/3 (53.2/44.4/2.4) | 0.232 0.587 |
| Pain, n a (%) Grade 1/2/3 | 220 (59.5) 127/90/3 (57.7/40.9/1.4) | 99 (57.6) 60/38/1 (60.6/38.4/1) | 121 (61.1) 67/52/2 (55.4/43/1.7) | 0.488 0.703 |
| Tenderness, n a (%) Grade 1/2/3 | 181 (48.9) 100/76/5 (55.2/42/2.8) | 70 (40.7) 38/28/4 (54.3/40/5.7) | 111 (56.1) 62/48/1 (55.9/43.2/0.9) | 0.003 0.155 |
| Swelling, n a (%) Grade 1/2/3 | 67 (18.1) 57/10/0 (85.1/14.9/0) | 31 (18) 27/4/0 (87.1/12.9/0) | 36 (18.2) 30/6/0 (83.3/16.7/0) | 0.968 0.666 |
| Erythema, n a (%) Grade 1/2/3 | 17 (4.6) 16/1/0 (94.1/5.9/0) | 8 (4.7) 8/0/0 (100/0/0) | 9 (4.5) 8/1/0 (88.9/11.1/0) | 0.961 0.331 |
| Systemic AE, n a (%) Grade 1/2/3 | 181 (48.9) 112/66/3 (61.9/36.4/1.7) | 82 (47.7) 50/29/3 (61/35.4/3.6) | 99 (50) 62/37/0 (62.6/37.4/0) | 0.655 0.275 |
| Fever, n a (%) Grade 1/2/3 | 47 (12.7) 33/13/1 (70.2/27.7/2.1) | 20 (11.6) 15/4/1 (75/20/5) | 27 (13.6) 18/9/0 (66.7/33.3/0) | 0.563 0.333 |
| Headache, n a (%) Grade 1/2/3 | 81 (21.9) 46/35/0 (56.8/43.2/0) | 37 (21.5) 27/10/0 (73/27/0) | 44 (22.2) 19/25/0 (43.2/56.8/0) | 0.869 0.007 |
| Myalgia, n a (%) Grade 1/2/3 | 126 (34.1) 85/39/2 (67.5/31/1.6) | 50 (29.1) 31/17/2 (62/34/4) | 76 (38.4) 54/22/0 (71.1/28.9/0) | 0.059 0.161 |
| Fatigue, n a (%) Grade 1/2/3 | 113 (30.5) 91/22/0 (80.5/19.5/0) | 50 (29.1) 37/13/0 (74/26/0) | 63 (31.8) 54/9/0 (85.7/14.3/0) | 0.567 0.118 |
| Nausea/Vomiting, n a (%) Grade 1/2/3 | 19 (5.1) 18/1/0 (94.7/5.3/0) | 8 (4.7) 7/1/0 (87.5/12.5/0) | 11 (5.6) 11/0/0 (100/0/0) | 0.694 0.228 |
| Diarrhea, n a (%) Grade 1/2/3 | 21 (5.7) 20/1/0 (95.2/4.8/0) | 9 (5.2) 8/1/0 (88.9/11.1/0) | 12 (6.1) 12/0/0 (100/0/0) | 0.731 0.237 |
| Arthralgia, n a (%) Grade 1/2/3 | 30 (8.1) 25/4/1 (83.3/13.3/3.3) | 11 (6.4) 7/3/1 (63.6/27.3/9.1) | 19 (9.6) 18/1/0 (94.7/5.3/0) | 0.261 0.079 |
| Back pain, n a (%) Grade 1/2/3 | 28 (7.6) 23/4/1 (82.1/14.3/3.6) | 9 (5.2) 6/2/1 (66.7/22.2/11.1) | 19 (9.6) 17/2/0 (89.5/10.5/0) | 0.113 0.214 |
| Dizziness, n a (%) Grade 1/2/3 | 30 (8.1) 28/1/1 (93.3/3.3/1) | 12 (7) 10/1/1 (83.3/8.3/8.3) | 18 (9.1) 18/0/0 (100/0/0) | 0.457 0.200 |
| Lymphadenopathy, n a (%) Grade 1/2/3 | 5 (1.4) 3/2/0 (60/40/0) | 4 (2.3) 3/1/0 75/25/0 | 1 (0.5) 0/1/0 0/100/0 | 0.130 0.171 |
| Factors | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| Odds Ratio (95% CI) | p-Value | Odds Ratio (95% CI) | p-Value | |
| Age * (years) | ||||
| ≥65 | Ref | |||
| <65 | 1.97 (1.27–3.04) | 0.002 | 1.87 (1.19–2.94) | 0.007 |
| Sex * | ||||
| Male | Ref | |||
| Female | 2.06 (1.34–3.17) | 0.001 | 1.82 (1.16–2.88) | 0.010 |
| BMI | ||||
| ≥18.5 | Ref | |||
| Underweight (<18.5) | 0.69 (0.37–1.29) | 0.240 | NA | |
| Comorbidity | ||||
| No | Ref | |||
| Yes | 0.74 (0.48–1.13) | 0.163 | NA | |
| ECOG PS | ||||
| 0–1 | Ref | |||
| 2 | 0.82 (0.40–1.66) | 0.575 | NA | |
| Staging | ||||
| Non-metastasis | Ref | |||
| Metastasis stage | 0.87 (0.57–1.34) | 0.541 | NA | |
| Type of treatment | ||||
| No treatment | Ref | |||
| Targeted/Endocrine therapy | 1.52 (0.82–2.83) | 0.184 | NA | |
| Chemotherapy | 0.70 (0.37–1.30) | 0.258 | NA | |
| Immunotherapy | 0.92 (0.36–2.36) | 0.862 | NA | |
| Radiation | ||||
| No | Ref | |||
| Yes | 0.54 (0.21–1.39) | 0.200 | NA | |
| Concurrent steroid use * | ||||
| No | Ref | |||
| Yes | 0.54 (0.34–0.86) | 0.009 | 0.66 (0.40–1.09) | 0.112 |
| Type of primary vaccine * | ||||
| ChAdOx1/ChAdOx1 | Ref | |||
| CoronaVac/ChAdOx1 | 0.46 (0.24–0.88) | 0.018 | 0.49 (0.24–0.97) | 0.042 |
| Interval between 2nd to 3rd vaccine | ||||
| 3 months | Ref | |||
| >3 months | 0.63 (0.27–1.47) | 0.286 | NA | |
| Type of mRNA vaccine * | ||||
| BNT162b2 | Ref | |||
| mRNA-1273 | 1.13 (0.74–1.74) | 0.566 | 1.22 (0.78–1.92) | 0.381 |
| Factors | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| Odds Ratio (95% CI) | p-Value | Odds Ratio (95% CI) | p-Value | |
| Age * (years) | ||||
| ≥65 | Ref | |||
| <65 | 2.34 (1.52–3.61) | <0.001 | 2.05 (1.29–3.27) | 0.002 |
| Sex * | ||||
| Male | Ref | |||
| Female | 2.05 (1.34–3.14) | <0.001 | 1.78 (1.14–2.80) | 0.011 |
| BMI | ||||
| ≥18.5 | Ref | |||
| Underweight (<18.5) | 0.74 (0.40–1.38) | 0.339 | NA | |
| Comorbidity * | ||||
| No | Ref | |||
| Yes | 0.62 (0.40–0.94) | 0.024 | 0.72 (0.44–1.17) | 0.186 |
| ECOG | ||||
| 0–1 | Ref | |||
| 2 | 0.58 (0.29–1.16) | 0.122 | NA | |
| Staging | ||||
| Non-metastasis | Ref | |||
| Metastasis stage | 0.85 (0.56–1.30) | 0.454 | NA | |
| Type of treatment | ||||
| No treatment | Ref | |||
| Targeted/Endocrine therapy | 1.60 (0.87–2.92) | 0.130 | NA | |
| Chemotherapy | 0.75 (0.41–1.38) | 0.357 | NA | |
| Immunotherapy | 0.96 (0.38–2.42) | 0.928 | NA | |
| Radiation | ||||
| No | Ref | |||
| Yes | 0.50 (0.19–1.29) | 0.152 | NA | |
| Concurrent steroid use * | ||||
| No | Ref | |||
| Yes | 0.52 (0.33–0.81) | 0.004 | 0.59 (0.36–0.97) | 0.042 |
| Type of primary vaccine * | ||||
| ChAdOx1/ChAdOx1 | Ref | |||
| CoronaVac/ChAdOx1 | 0.55 (0.29–1.04) | 0.066 | 0.58 (0.29–1.17) | 0.129 |
| Interval between 2nd to 3rd vaccine | ||||
| 3 months | Ref | |||
| >3 months | 0.76 (0.35–1.67) | 0.494 | NA | |
| Type of mRNA vaccine * | ||||
| BNT162b2 | Ref | |||
| mRNA-1273 | 1.29 (0.85–1.96) | 0.123 | 1.36 (0.86–2.13) | 0.197 |
| Factors | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| Odds Ratio (95% CI) | p-Value | Odds Ratio (95% CI) | p-Value | |
| Age * (years) | ||||
| ≥65 | Ref | |||
| <65 | 2.00 (1.31–3.08) | 0.001 | 1.94 (1.24–3.04) | 0.004 |
| Sex * | ||||
| Male | Ref | |||
| Female | 2.03 (1.33–3.09) | <0.001 | 1.85 (1.18–2.88) | 0.007 |
| BMI | ||||
| ≥18.5 | Ref | |||
| Underweight (<18.5) | 0.86 (0.46–1.60) | 0.636 | NA | |
| Comorbidity | ||||
| No | Ref | |||
| Yes | 0.86 (0.57–1.30) | 0.480 | NA | |
| ECOG | ||||
| 0–1 | Ref | |||
| 2 | 0.67 (0.29–1.16) | 0.120 | NA | |
| Staging | ||||
| Non-metastasis | Ref | |||
| Metastasis stage | 0.85 (0.33–1.36) | 0.271 | NA | |
| Type of treatment | ||||
| No treatment | Ref | |||
| Targeted/Endocrine therapy | 1.24 (0.69–2.22) | 0.479 | NA | |
| Chemotherapy | 0.66 (0.36–1.21) | 0.174 | NA | |
| Immunotherapy | 0.71 (0.28–1.79) | 0.467 | NA | |
| Radiation * | ||||
| No | Ref | |||
| Yes | 0.28 (0.09–0.86) | 0.028 | 0.29 (0.09–0.92) | 0.045 |
| Concurrent steroid use * | ||||
| No | Ref | |||
| Yes | 0.68 (0.43–1.07) | 0.096 | 0.88 (0.54–1.45) | 0.631 |
| Type of primary vaccine * | ||||
| ChAdOx1/ChAdOx1 | Ref | |||
| CoronaVac/ChAdOx1 | 0.43 (0.21–0.85) | 0.015 | 0.41 (0.20–0.86) | 0.018 |
| Interval between 2nd to 3rd vaccine | ||||
| 3 months | Ref | |||
| >3 months | 0.83 (0.39–1.74) | 0.614 | NA | |
| Type of mRNA vaccine * | ||||
| BNT162b2 | Ref | |||
| mRNA-1273 | 1.10 (0.73–1.65) | 0.655 | 1.16 (0.75–1.80) | 0.501 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wanchaijiraboon, P.; Sainamthip, P.; Teeyapun, N.; Luangdilok, S.; Poovorawan, Y.; Wanlapakorn, N.; Tanasanvimon, S.; Sriuranpong, V.; Susiriwatananont, T.; Zungsontiporn, N.; et al. Safety Following COVID-19 Booster Vaccine with BNT162b2 Compared to mRNA-1273 in Solid Cancer Patients Previously Vaccinated with ChAdOx1 or CoronaVac. Vaccines 2023, 11, 356. https://doi.org/10.3390/vaccines11020356
Wanchaijiraboon P, Sainamthip P, Teeyapun N, Luangdilok S, Poovorawan Y, Wanlapakorn N, Tanasanvimon S, Sriuranpong V, Susiriwatananont T, Zungsontiporn N, et al. Safety Following COVID-19 Booster Vaccine with BNT162b2 Compared to mRNA-1273 in Solid Cancer Patients Previously Vaccinated with ChAdOx1 or CoronaVac. Vaccines. 2023; 11(2):356. https://doi.org/10.3390/vaccines11020356
Chicago/Turabian StyleWanchaijiraboon, Passakorn, Panot Sainamthip, Nattaya Teeyapun, Sutima Luangdilok, Yong Poovorawan, Nasamon Wanlapakorn, Suebpong Tanasanvimon, Virote Sriuranpong, Thiti Susiriwatananont, Nicha Zungsontiporn, and et al. 2023. "Safety Following COVID-19 Booster Vaccine with BNT162b2 Compared to mRNA-1273 in Solid Cancer Patients Previously Vaccinated with ChAdOx1 or CoronaVac" Vaccines 11, no. 2: 356. https://doi.org/10.3390/vaccines11020356