
One-Year Post-Vaccination Longitudinal Follow-Up of Quantitative SARS-CoV-2 Anti-Spike Total Antibodies in Health Care Professionals and Evaluation of Correlation with Surrogate Neutralization Test

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
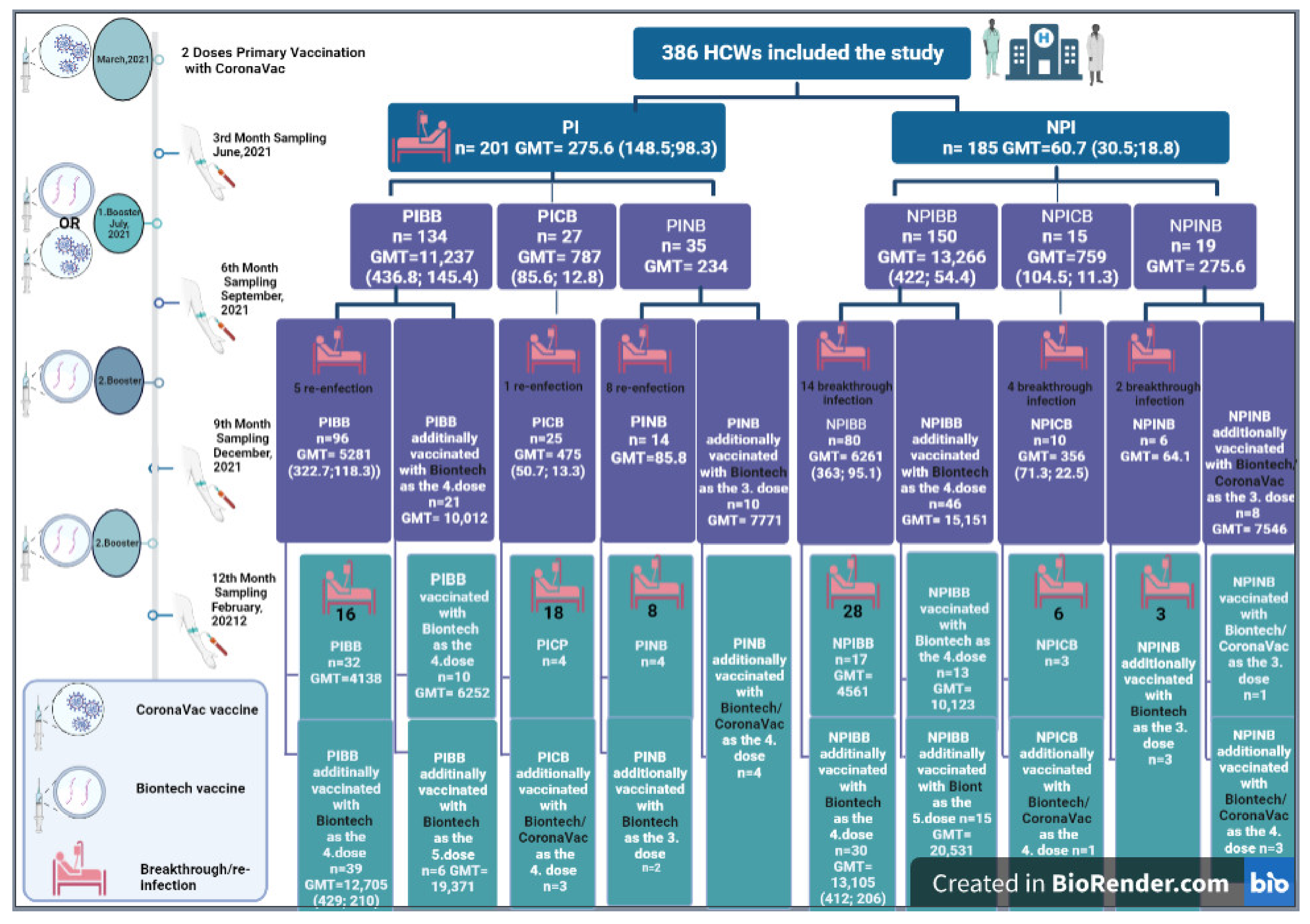
2.1. Participants and Study Design
2.2. Demographics and Clinical Data
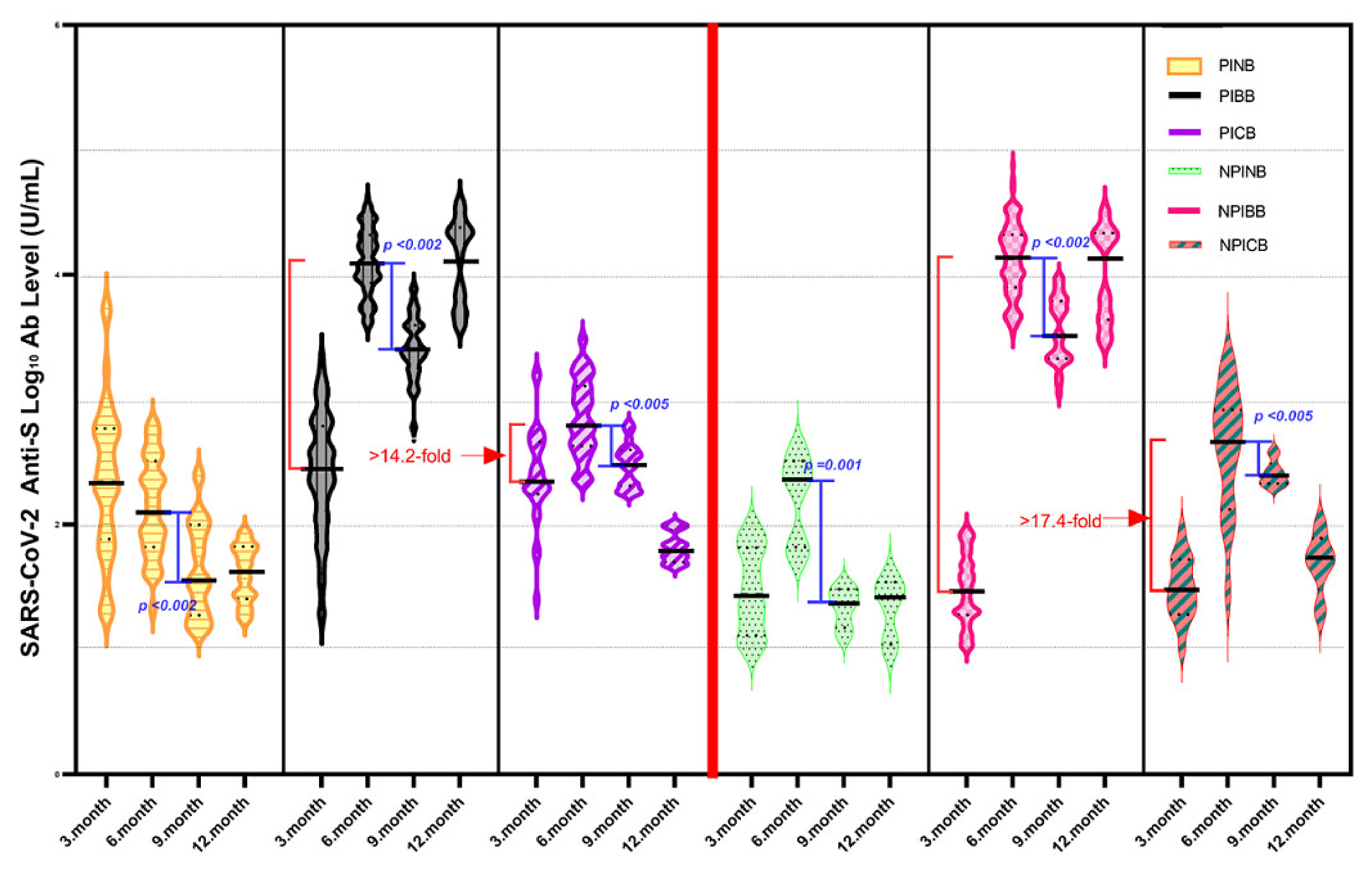
2.3. Assessment of Anti-SARS-CoV-2 Spike Total Antibodies
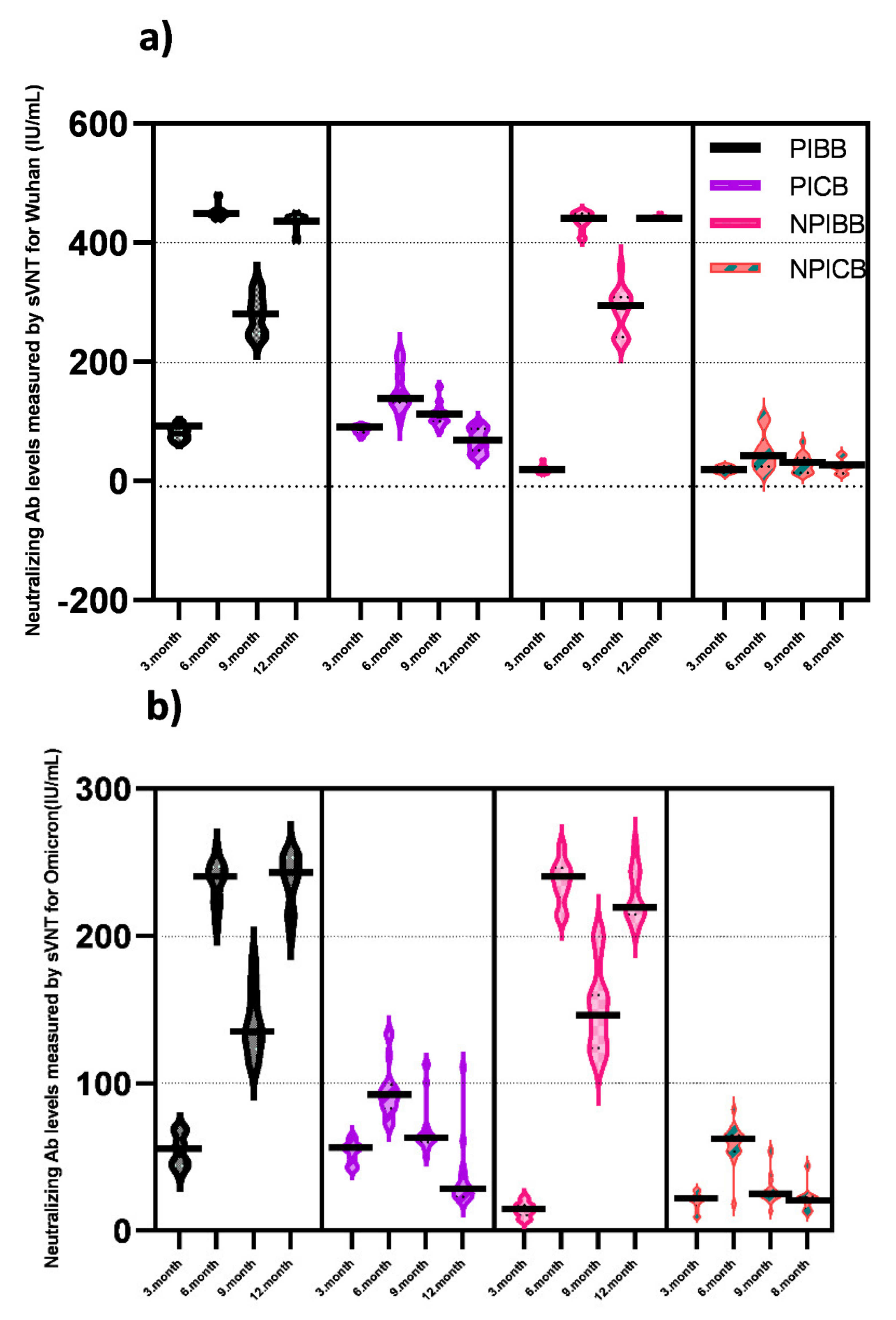
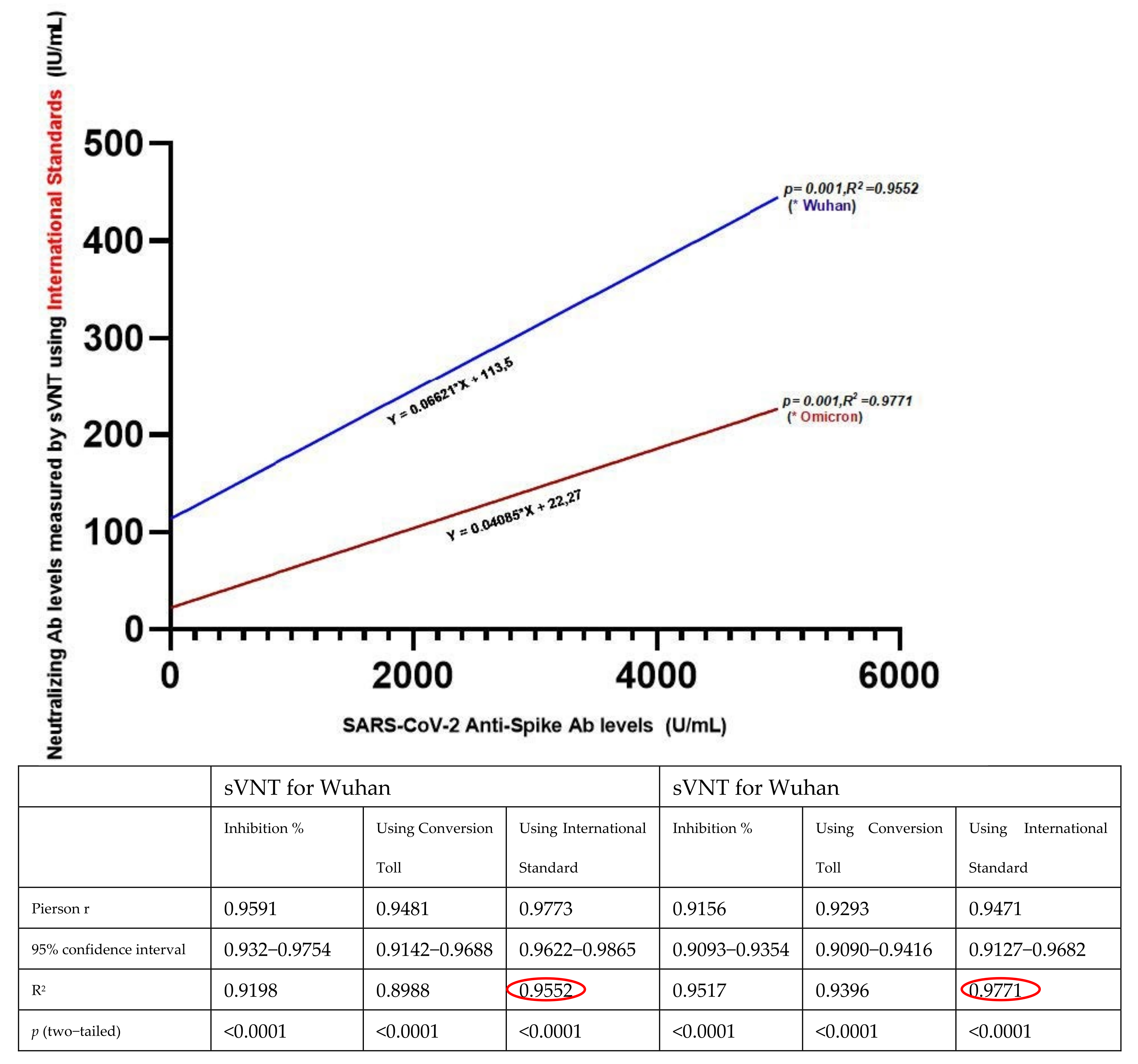
2.4. Assessment of SARS-CoV-2 Neutralizing Antibodies to the Ancestral Wuhan and Omicron Variant
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Park, J.; Lee, H. Delivery Routes for COVID-19 Vaccines. Vaccines 2021, 9, 524. [Google Scholar] [CrossRef]
- Zhao, Q.; Gao, Y.; Xiao, M.; Huang, X.; Wu, X. Synthesis and immunological evaluation of synthetic peptide based anti-SARS-CoV-2 vaccine candidates. Chem. Commun. 2021, 57, 1474–1477. [Google Scholar] [CrossRef]
- Mallapaty, S. WHO approval of Chinese CoronaVac COVID vaccine will be crucial to curbing pandemic. Nature 2021, 594, 161–162. [Google Scholar] [CrossRef]
- Gao, Q.; Bao, L.; Mao, H.; Lin, W.; Kangwei, X.; Minnan, Y.; Yajing, L.; Ling, Z.; Nan, W.; Zhe, L.; et al. Development of an inactivated vaccine candidate for SARS-CoV-2. Science 2020, 369, 77–81. [Google Scholar] [CrossRef]
- Melo-González, F.; Soto, J.A.; González, L.A.; Fernández, J.; Duarte, L.F.; Schultz, B.M.; Gálvez, N.M.S.; Pacheco, G.A.; Ríos, M.; Vázquez, Y.; et al. Recognition of Variants of Concern by Antibodies and T Cells Induced by a SARS-CoV-2 Inactivated Vaccine. Front. Immunol. 2021, 12, 747830. [Google Scholar] [CrossRef]
- Werner, M.; Pervan, P.; Glück, V.; Zeman, F.; Koller, M.; Burkhardt, R.; Glück, T.; Wenzel, J.; Schmidt, B.; Gessner, A.; et al. Evaluation of a broad panel of SARS-CoV-2 serological tests for diagnostic use. J. Clin. Med. 2021, 10, 1580. [Google Scholar] [CrossRef] [PubMed]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- Sauré, D.; O’Ryan, M.; Torres, J.P.; Zuniga, M.; Santelices, E.; Basso, L.J. Dynamic IgG seropositivity after rollout of CoronaVac and BNT162b2 COVID-19 vaccines in Chile: A sentinel surveillance study. Lancet Infect. Dis. 2022, 22, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Zeng, G.; Wu, Q.; Pan, H.; Li, M.; Yang, J.; Wang, L.; Wu, Z.; Jiang, D.; Deng, X.; Chu, K.; et al. Immunogenicity and safety of a third dose of CoronaVac, and immune persistence of a two-dose schedule, in healthy adults: Interim results from two single-centre, double-blind, randomised, placebo-controlled phase 2 clinical trials. Lancet Infect. Dis. 2022, 22, 483–495. [Google Scholar] [CrossRef]
- Cao, Y.; Yisimayi, A.; Bai, Y.; Huang, W.; Li, X.; Zhang, Z.; Yuan, T.; An, R.; Wang, J.; Xiao, T.; et al. Humoral immune response to circulating SARS-CoV-2 variants elicited by inactivated and RBD-subunit vaccines. Cell Res. 2021, 31, 732–741. [Google Scholar] [CrossRef] [PubMed]
- Pieri, M.; Infantino, M.; Manfredi, M.; Nuccetelli, M.; Grossi, V.; Lari, B.; Tomassetti, F.; Sarubbi, S.; Russo, E.; Amedei, A.; et al. Performance evaluation of four surrogate Virus Neutralization Tests (sVNTs) in comparison to the in vivo gold standard test. Front. Biosci. 2022, 27, 74. [Google Scholar] [CrossRef] [PubMed]
- de la Torre, J.C.G.; Cáceres-DelAguila, J.A.; Muro-Rojo, C.; De La Cruz-Escurra, N.; Copaja-Corzo, C.; Hueda-Zavaleta, M.; Siles, D.A.; A Benites-Zapata, V. Humoral Immune Response Induced by the BBIBP-CorV Vaccine (Sinopharm) in Healthcare Workers: A Cohort Study. Trop. Med. Infect. Dis. 2022, 7, 66. [Google Scholar] [CrossRef] [PubMed]
- Nanjing GenScript Diagnostics Technology Co., Ltd. CPass SARS-CoV-2 Neutralization Antibody Detection Kit Instructions for Use; Nanjing GenScript Diagnostics Technology Co., Ltd.: Nanjing, China, 2022. [Google Scholar]
- Mattiuzzo, G.; Bentley, E.M.; Hassall, M.; Routley, S. Establishment of the WHO International Standard and Reference Panel for Anti-SARS-CoV-2 Antibody. World Health Organization. 2020. Available online: https://www.who.int/publications/m/item/WHO-BS-2020.2403 (accessed on 5 May 2021).
- CPass-IU-Conversion-Tool-20210804. 2021. Available online: https://github.com/Lelouchzhu/cPass-to-IU_Conversion/blob/main/cPass-IU-Conversion-tool-20210804.xlsx (accessed on 14 September 2021).
- Zhu, F.; Althaus, T.; Tan, C.W.; Costantini, A.; Ni Chia, W.; Chau, N.V.V.; Van Tan, L.; Mattiuzzo, G.; Rose, N.J.; Voiglio, E.; et al. WHO international standard for SARS-CoV-2 antibodies to determine markers of protection. Lancet Microbe 2022, 3, e81–e82. [Google Scholar] [CrossRef]
- Xia, S.; Zhang, Y.; Wang, Y.; Wang, H.; Yang, Y.; Gao, G.F.; Tan, W.; Wu, G.; Xu, M.; Lou, Z.; et al. Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBIBP-CorV: A randomised, double-blind, placebo-controlled, phase 1/2 trial. Lancet Infect. Dis. 2021, 21, 39–51. [Google Scholar] [CrossRef]
- Lijeskić, O.; Klun, I.; Djaković, M.S.; Gligorić, N.; Štajner, T.; Srbljanović, J.; Djurković-Djaković, O. Prospective cohort study of the kinetics of specific antibodies to SARS-CoV-2 infection and to four SARS-CoV-2 vaccines available in serbia, and vaccine effectiveness: A 3-month interim report. Vaccines 2021, 9, 1031. [Google Scholar] [CrossRef] [PubMed]
- Ebinger, J.E.; Fert-Bober, J.; Printsev, I.; Wu, M.; Sun, N.; Prostko, J.C.; Frias, E.C.; Stewart, J.L.; Van Eyk, J.E.; Braun, J.G.; et al. Antibody responses to the BNT162b2 mRNA vaccine in individuals previously infected with SARS-CoV-2. Nat. Med. 2021, 27, 981–984. [Google Scholar] [CrossRef]
- Liu, Y.; Zeng, Q.; Deng, C.; Li, M.; Li, L.; Liu, D.; Liu, M.; Ruan, X.; Mei, J.; Mo, R.; et al. Robust induction of B cell and T cell responses by a third dose of inactivated SARS-CoV-2 vaccine. Cell Discov. 2022, 8, 10. [Google Scholar] [CrossRef]
- Moghnieh, R.; Mekdashi, R.; El-Hassan, S.; Abdallah, D.; Jisr, T.; Bader, M.; Jizi, I.; Sayegh, M.H.; Bizri, A.R. Immunogenicity and reactogenicity of BNT162b2 booster in BBIBP-CorV-vaccinated individuals compared with homologous BNT162b2 vaccination: Results of a pilot prospective cohort study from Lebanon. Vaccine 2021, 39, 6713–6719. [Google Scholar] [CrossRef]
- Clemens, S.A.C.; Weckx, L.; Clemens, R.; Mendes, A.V.A.; Souza, A.R.; Silveira, M.B.V.; da Guarda, S.N.F.; de Nobrega, M.M.; Pinto, M.I.D.M.; Gonzalez, I.G.S.; et al. Heterologous versus homologous COVID-19 booster vaccination in previous recipients of two doses of CoronaVac COVID-19 vaccine in Brazil (RHH-001): A phase 4, non-inferiority, single blind, randomised study. Lancet 2022, 399, 521–529. [Google Scholar] [CrossRef]
- Vályi-Nagy, I.; Matula, Z.; Gönczi, M.; Tasnády, S.; Bekő, G.; Réti, M.; Ajzner, É.; Uher, F. Comparison of antibody and T cell responses elicited by BBIBP-CorV (Sinopharm) and BNT162b2 (Pfizer-BioNTech) vaccines against SARS-CoV-2 in healthy adult humans. GeroScience 2021, 43, 2321–2331. [Google Scholar] [CrossRef]
- Arbel, R.; Hammerman, A.; Sergienko, R.; Friger, M.; Peretz, A.; Netzer, D.; Yaron, S. BNT162b2 Vaccine Booster and Mortality Due to COVID-19. N. Engl. J. Med. 2021, 385, 2413–2420. [Google Scholar] [CrossRef] [PubMed]
- Saciuk, Y.; Kertes, J.; Stein, N.S.; Zohar, A.E. Effectiveness of a Third Dose of BNT162b2 mRNA Vaccine. J. Infect. Dis. 2022, 225, 30–33. [Google Scholar] [CrossRef] [PubMed]
- Jantarabenjakul, W.; Sodsai, P.; Chantasrisawad, N.; Jitsatja, A.; Ninwattana, S.; Thippamom, N.; Ruenjaiman, V.; Tan, C.W.; Pradit, R.; Sophonphan, J.; et al. Dynamics of Neutralizing Antibody and T-Cell Responses to SARS-CoV-2 and Variants of Concern after Primary Immunization with CoronaVac and Booster with BNT162b2 or ChAdOx1 in Health Care Workers. Vaccines 2022, 10, 639. [Google Scholar] [CrossRef]
- Hueda-Zavaleta, M.; de la Torre, J.C.G.; Aguila, J.A.C.-D.; Muro-Rojo, C.; De La Cruz-Escurra, N.; Siles, D.A.; Minchón-Vizconde, D.; Copaja-Corzo, C.; Bardales-Silva, F.; Benites-Zapata, V.A.; et al. Evaluation of the Humoral Immune Response of a Heterologous Vaccination between BBIBP-CorV and BNT162b2 with a Temporal Separation of 7 Months, in Peruvian Healthcare Workers with and without a History of SARS-CoV-2 Infection. Vaccines 2022, 10, 502. [Google Scholar] [CrossRef]
- Munro, A.P.S.; Janani, L.; Cornelius, V.; Aley, P.K.; Babbage, G.; Baxter, D.; Bula, M.; Cathie, K.; Chatterjee, K.; Dodd, K.; et al. Safety and immunogenicity of seven COVID-19 vaccines as a third dose (booster) following two doses of ChAdOx1 nCov-19 or BNT162b2 in the UK (COV-BOOST): A blinded, multicentre, randomised, controlled, phase 2 trial. Lancet 2021, 398, 2258–2276. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.-T.; Gong, Y.-N.; Huang, C.-G.; Huang, P.-N.; Yu, K.-Y.; Lee, H.-C.; Lee, S.-C.; Chiang, H.-J.; Kung, Y.-A.; Lin, Y.-T.; et al. Quantifying Neutralizing Antibodies in Patients with COVID-19 by a Two-Variable Generalized Additive Model. MSphere 2022, 7, e00883-21. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Previously Infected (n = 201) | Non-Previously Infected (n = 185) | p Value | |
|---|---|---|---|
| Age (years, mean ±Std) | 36.53 ± 8.41 | 37.59 ± 9.03 | 0.39 |
| Gender (n) | 114 female/87 male | 110 female/75 male | 0.48 |
| Risky Medical Condition (n) | 56 (28.1%) | 36 (19.7%) | <0.05 * |
| Smoking (n) | 65 (32.3%) | 40 (21.6%) | <0.02 * |
| BMI (>30) (n) | 26 (12.9%) | 26 (14%) | <0.05 * |
| Comorbidities | |||
| 4 (1.9%) | 4 (2.1%) | 0.32 |
| 16 (7.9%) | 15 (8.1%) | 0.34 |
| 9 (4.4%) | 1 (0.5%) | <0.05 * |
| 4 (1.9%) | 0 (0%) | <0.05 * |
| Sampling Time | Previously Infected Group (n = 201) | Non–Previously Infected Group (n = 185) | p Value | ||||
|---|---|---|---|---|---|---|---|
| Anti-SARS-CoV-2 spike total Ab (U/mL) | |||||||
| (1) 3rd month | 275.6 (102.4–1057.9) | 60.7 (9.8–76.3) | <0.001 * | ||||
| PIBB | PICB | PINB | NPIBB | NPICB | NPINB | ||
| (2) 6th month | 11,237 (2246–39,588) | 787.2 (271.5–916.3) | 234.0 (10.1–627.4) | 13,266 (1879–35,352) | 759.1 (144.8–831.2) | 275.6 (55.6–672.5) | |
| (3) 9th month | 5281 (3732–7739) | 475.4 (248.7–734.8) | 85.8 (23.1–96.7) | 6261 (4568–11,214) | 356.2 (224.2–515.9) | 64.1 (22.5–82.1) | |
| (4) 12th month | 4138 (3266.7–6394)/ † 12,705 (4874–4216) | 91.1 (77.2–103.0) | 80.5 (69.9–93.6) | 4561 (3822–7411)/ † 13,105 (8634–8103) | 86.2 (14.2–101.2) | 68.3 (16.5–99.7) | |
| Anti–SARS–CoV–2 neutralizing antibodies–NabWuhan, NabOmicron (95% CI) (IU/mL) | |||||||
| (1) 3rd month | 148.5 (58.6–135.4), 98.3 (96.2–101.3) | 30.5 (18.6–30.45), 18.8 (14.6–24.2) | <0.001 * | ||||
| PIBB | PICB | PINB | NPIBB | NPICB | NPINB | ||
| (2) 6th month | 436.8 (426.2–445.1), 145.4 (134.0–156.5) | 85.6 (78.8–89.1), 12.8 (11.4–24.5) | NA | 422.5 (412.8–433.2), 54.4 (41.26–63.3) | 104.5 (97.6–104.0), 11.3 (8.6–27.1) | NA | |
| (3) 9th month | 322.7 (317.5–331.9), 118.3 (106.6–155.2) | 50.7 (46.6–57.4), 13.3 (9.6–30.5) | NA | 363.6 (17.8–44.0, 95.1 (92.2–111.7) | 71.3 (65.1–77.2), 22.5 (20.1–25.6 | NA | |
| (4) 12th month | † 429.3(426.2–444.1), † 210.9 (202.0–223.5) | 21.5 (17.7–26.1), 11.2 (6.3–18.6) | NA | † 412.4 (410.3–416.8), † 206.2 (202.5–211.9) | 23.6 (19.8–26.5), 10.8 (8.4–13.7) | NA | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tuyji Tok, Y.; Can Sarinoglu, R.; Ordekci, S.; Yilmaz, S.; Ozcolpan, G.; Bayram, A.; Nohut, O.K.; Kocer, I.; Hasdemir, U.; Kuskucu, M.A.; et al. One-Year Post-Vaccination Longitudinal Follow-Up of Quantitative SARS-CoV-2 Anti-Spike Total Antibodies in Health Care Professionals and Evaluation of Correlation with Surrogate Neutralization Test. Vaccines 2023, 11, 355. https://doi.org/10.3390/vaccines11020355
Tuyji Tok Y, Can Sarinoglu R, Ordekci S, Yilmaz S, Ozcolpan G, Bayram A, Nohut OK, Kocer I, Hasdemir U, Kuskucu MA, et al. One-Year Post-Vaccination Longitudinal Follow-Up of Quantitative SARS-CoV-2 Anti-Spike Total Antibodies in Health Care Professionals and Evaluation of Correlation with Surrogate Neutralization Test. Vaccines. 2023; 11(2):355. https://doi.org/10.3390/vaccines11020355
Chicago/Turabian StyleTuyji Tok, Yesim, Rabia Can Sarinoglu, Seyhan Ordekci, Serife Yilmaz, Gunes Ozcolpan, Aysen Bayram, Okan Kadir Nohut, Ipek Kocer, Ufuk Hasdemir, Mert Ahmet Kuskucu, and et al. 2023. "One-Year Post-Vaccination Longitudinal Follow-Up of Quantitative SARS-CoV-2 Anti-Spike Total Antibodies in Health Care Professionals and Evaluation of Correlation with Surrogate Neutralization Test" Vaccines 11, no. 2: 355. https://doi.org/10.3390/vaccines11020355