
Knowledge of Human Mpox (Monkeypox) and Attitude towards Mpox Vaccination among Male Sex Workers in China: A Cross-Sectional Study
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Participants and Procedures
2.2. Data Collection and Quality Control
2.3. Study Variables
2.4. Data Analysis
3. Results
3.1. Socio-Demographic Characteristic
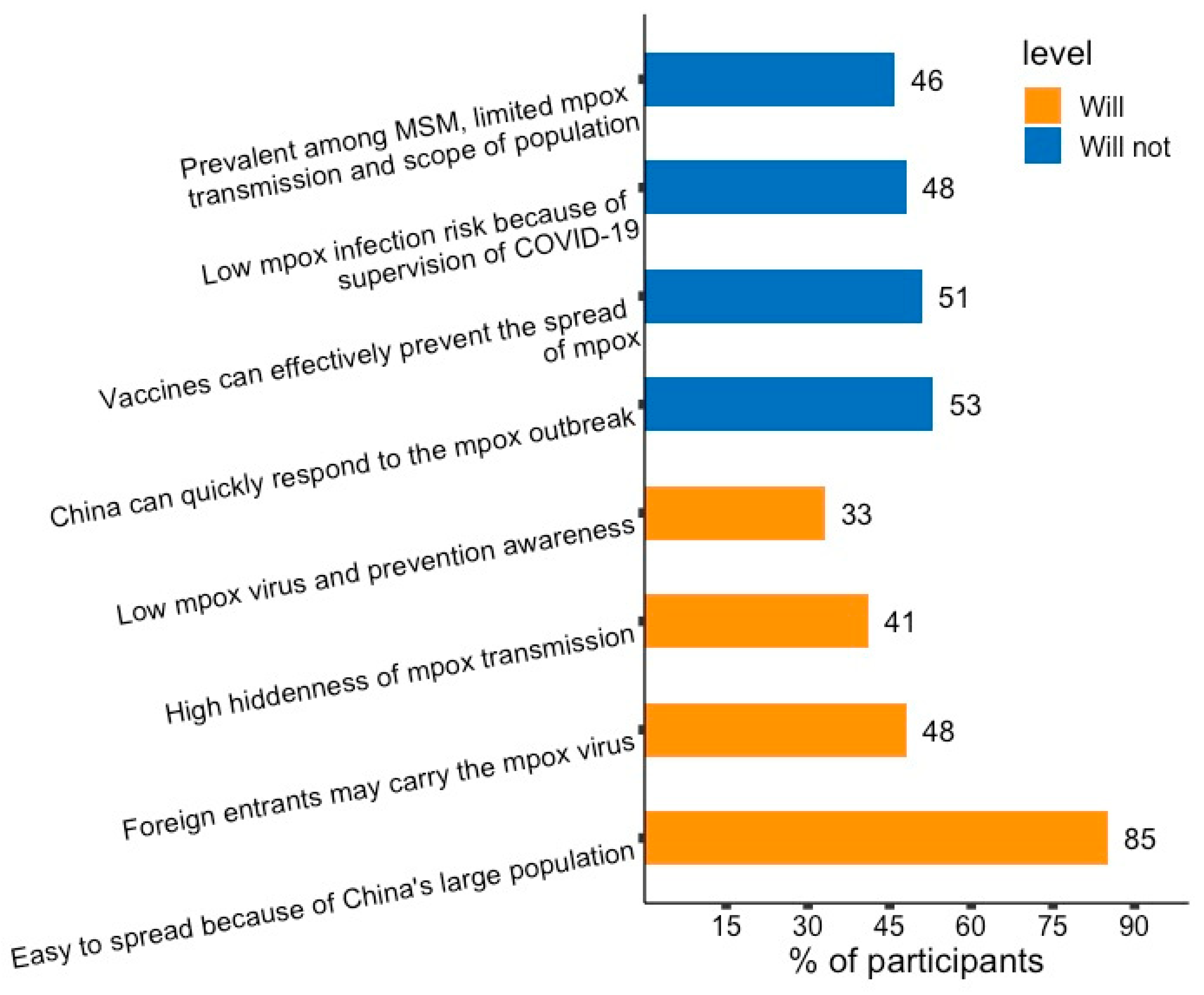
3.2. Whether China Would Become A Mpox Endemic Country
3.3. Factors Associated with Mpox Knowledge Level
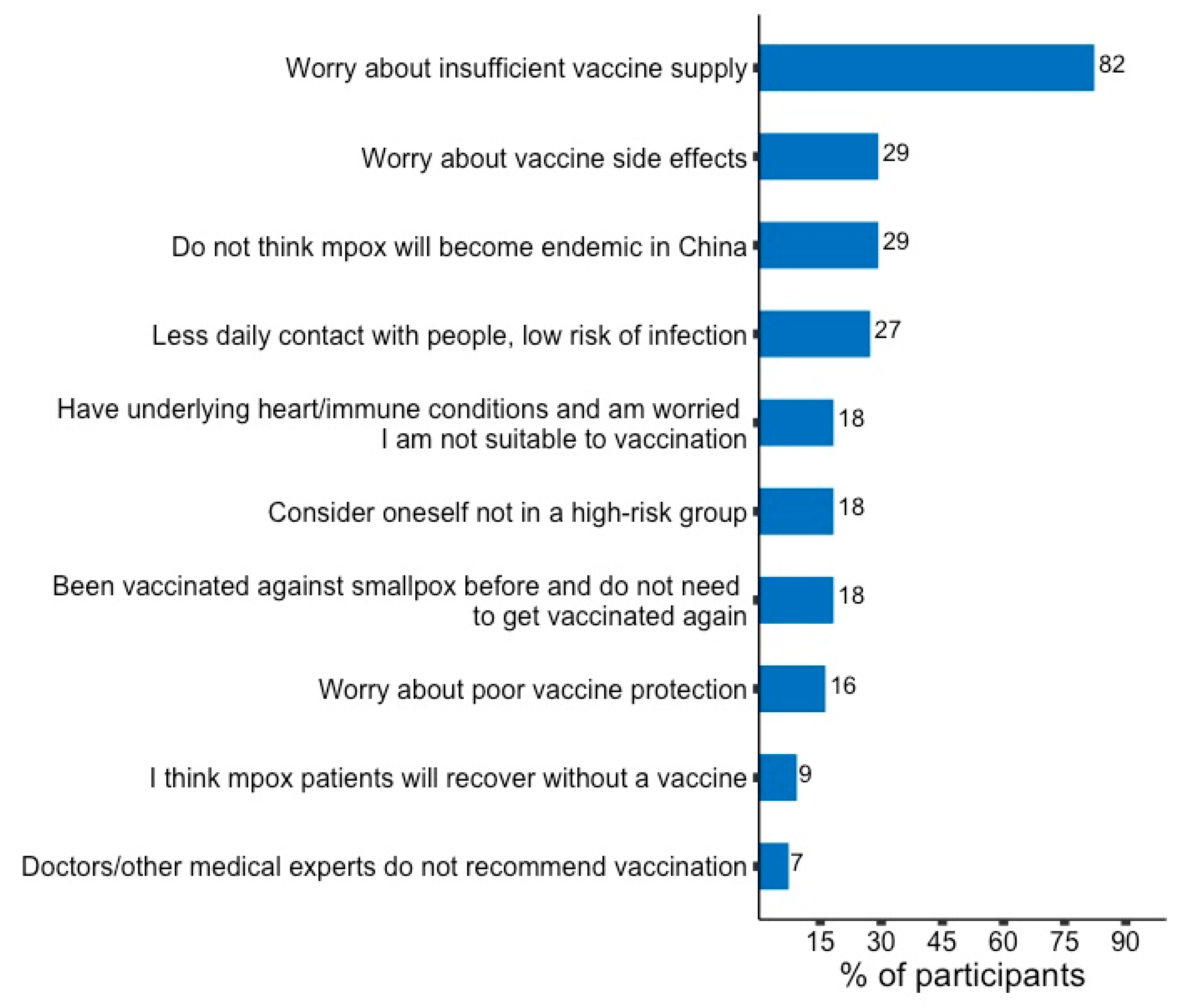
3.4. Attitude towards Mpox Vaccination and Correlates
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Monkeypox. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/monkeypox (accessed on 24 October 2022).
- Liu, Q.; Fu, L.; Wang, B.; Sun, Y.; Wu, X.; Peng, X.; Li, Y.; Lin, Y.F.; Fitzpatrick, T.; Vermund, S.H.; et al. Clinical Characteristics of Human Mpox (Monkeypox) in 2022: A Systematic Review and Meta-Analysis. Pathogens 2023, 12, 146. [Google Scholar] [CrossRef]
- Mccollum, A.M.; Damon, I.K. Human Monkeypox. Clin. Infect. Dis. 2013, 58, 260–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention. 2022 Monkeypox Outbreak Global Map. 2022. Available online: https://www.cdc.gov/poxvirus/monkeypox/response/2022/world-map.html (accessed on 24 October 2022).
- World Health Organization. Director-General Declares the Ongoing Monkeypox Outbreak a Public Health Emergency of In-ternational Concern. 2022. Available online: https://www.who.int/europe/news/item/23-07-2022-who-director-general-declares-the-ongoing-monkeypox-outbreak-a-public-health-event-of-international-concern (accessed on 24 October 2022).
- Petersen, E.; Zumla, A.; Hui, D.; Blumberg, L.; Valdoleiros, S.; Amao, L.; Ntoumi, F.; Asogun, D.; Simonsen, L.; Haider, N.; et al. Vaccination for monkeypox prevention in persons with high-risk sexual behaviours to control on-going outbreak of monkeypox virus clade 3. Int. J. Infect. Dis. 2022, 122, 569–571. [Google Scholar] [CrossRef] [PubMed]
- Philpott, D.; Hughes, C.M.; Alroy, K.A.; Kerins, J.L.; Pavlick, J.; Asbel, L.; Crawley, A.; Newman, A.P.; Spencer, H.; Feldpausch, A.; et al. Epidemiologic and Clinical Characteristics of Monkeypox Cases—United States, May 17–July 22, 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 1018–1022. [Google Scholar] [CrossRef] [PubMed]
- The WHO Europen Region. Joint ECDC- WHO Regional Office for Europe Monkeypox Surveillance Bulletin. 2022. Available online: https://monkeypoxreport.ecdc.europa.eu (accessed on 24 October 2022).
- Liu, X.; Zhu, Z.; He, Y.; Lim, J.W.; Lane, B.; Wang, H.; Peng, Q.; Sun, L.; Lu, H. Monkeypox claims new victims: The outbreak in men who have sex with men. Infect. Dis. Poverty 2022, 11, 84. [Google Scholar] [CrossRef] [PubMed]
- Baral, S.D.; Friedman, M.R.; Geibel, S.; Rebe, K.; Bozhinov, B.; Diouf, D.; Sabin, K.; Holland, C.E.; Chan, R.; Cáceres, C.F. Male sex workers: Practices, contexts, and vulnerabilities for HIV acquisition and transmission. Lancet 2015, 385, 260–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, M.H.; Gong, H.; Jiang, G.H. Prevalence and characteristics of HIV and syphilis among male sex workers in China. Chin. J. AIDS STD 2019, 25, 99–104. [Google Scholar] [CrossRef]
- Rao, A.K.; Petersen, B.W.; Whitehill, F.; Razeq, J.H.; Isaacs, S.N.; Merchlinsky, M.J.; Campos-Outcalt, D.; Morgan, R.L.; Damon, I.; Sánchez, P.J.; et al. Use of JYNNEOS (Smallpox and Monkeypox Vaccine, Live, Nonreplicating) for Preexposure Vaccination of Persons at Risk for Occupational Exposure to Orthopoxviruses: Recommendations of the Advisory Committee on Immunization Practices—United States, 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 734–742. [Google Scholar] [CrossRef]
- Zhao, H.; Wang, W.; Zhao, L.; Ye, S.; Song, J.; Lu, R.; Zong, H.; Wu, C.; Huang, W.; Huang, B.; et al. The First Imported Case of Monkeypox in the Mainland of China—Chongqing Municipality, China, September 16, 2022. CDCC Wkly. 2022, 4, 853–854. [Google Scholar] [CrossRef]
- Keebayoon, A.; Mungmunpuntipantip, R.; Wiwanitkit, V. China and monkeypox: Correspondence. Anim. Model. Exp. Med. 2022, 5, 485–486. [Google Scholar] [CrossRef]
- Wei, Q. Is China ready for monkeypox? Anim. Model. Exp. Med. 2022, 5, 397–398. [Google Scholar] [CrossRef] [PubMed]
- Sadlier, C.; Lynam, A.; O’Dea, S.; Delamere, S.; Quinlan, M.; Clarke, S.; Sheils, O.; Bergin, C. HPV vaccine acceptability in HIV-infected and HIV negative men who have sex with men (MSM) in Ireland. Hum. Vaccines Immunother. 2016, 12, 1536–1541. [Google Scholar] [CrossRef] [Green Version]
- Feleke, B.T.; Wale, M.Z.; Yirsaw, M.T. Knowledge, attitude and preventive practice towards COVID-19 and associated factors among outpatient service visitors at Debre Markos compressive specialized hospital, north-west Ethiopia, 2020. PLoS ONE 2021, 16, e0251708. [Google Scholar] [CrossRef] [PubMed]
- Harapan, H.; Setiawan, A.M.; Yufika, A.; Anwar, S.; Wahyuni, S.; Asrizal, F.W.; Sufri, M.R.; Putra, R.P.; Wijayanti, N.P.; Salwiyadi, S.; et al. Knowledge of human monkeypox viral infection among general practitioners: A cross-sectional study in Indonesia. Ann. Trop. Med. Parasitol. 2020, 114, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.; Pan, P.; Lin, Y.; Ye, L.; Xie, L.; Xie, Y.; Liang, B.; Zheng, F.; Chen, R.; Wen, L.; et al. A Survey on HIV/AIDS-Related Knowledge, Attitudes, Risk Behaviors, and Characteristics of Men Who Have Sex with Men among University Students in Guangxi, China. BioMed Res. Int. 2020, 2020, 7857231. [Google Scholar] [CrossRef]
- Kahle, E.M.; Sullivan, S.; Stephenson, R. Functional Knowledge of Pre-Exposure Prophylaxis for HIV Prevention Among Participants in a Web-Based Survey of Sexually Active Gay, Bisexual, and Other Men Who Have Sex with Men: Cross-Sectional Study. JMIR Public Health Surveill. 2018, 4, e13. [Google Scholar] [CrossRef]
- Wadhera, P.; Evans, J.L.; Stein, E.; Gandhi, M.; Couture, M.-C.; Sansothy, N.; Sichan, K.; Maher, L.; Kaldor, J.; Page, K.; et al. Human papillomavirus knowledge, vaccine acceptance, and vaccine series completion among female entertainment and sex workers in Phnom Penh, Cambodia: The Young Women’s Health Study. Int. J. STD AIDS 2014, 26, 893–902. [Google Scholar] [CrossRef] [Green Version]
- Ousseine, Y.M.; Vaux, S.; Vandentorren, S.; Bonmarin, I.; Champenois, K.; Lydié, N.; Velter, A. Predictors of Uncertainty and Unwillingness to Receive the COVID-19 Vaccine in Men Who Have Sex with Men in France. Int. J. Environ. Res. Public Health 2022, 19, 5372. [Google Scholar] [CrossRef]
- Nadarzynski, T.; Frost, M.; Miller, D.; Wheldon, C.W.; Wiernik, B.M.; Zou, H.; Richardson, D.; Marlow, L.A.; Smith, H.; Jones, C.J.; et al. Vaccine acceptability, uptake and completion amongst men who have sex with men: A systematic review, meta-analysis and theoretical framework. Vaccine 2021, 39, 3565–3581. [Google Scholar] [CrossRef]
- Zheng, W.; Sun, Y.; Li, H.; Zhao, H.; Zhan, Y.; Gao, Y.; Hu, Y.; Li, P.; Lin, Y.-F.; Chen, H.; et al. COVID-19 vaccine uptake and hesitancy among HIV-infected men who have sex with men in mainland China: A cross-sectional survey. Hum. Vaccines Immunother. 2021, 17, 4971–4981. [Google Scholar] [CrossRef]
- Sethi, G.; Holden, B.M.; Greene, L.; Gaffney, J.; Ward, H. Hepatitis B vaccination for male sex workers: The experience of a specialist GUM service. Sex. Transm. Infect. 2006, 82, 84–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riad, A.; Drobov, A.; Rozmarinová, J.; Drapáčová, P.; Klugarová, J.; Dušek, L.; Pokorná, A.; Klugar, M. Monkeypox Knowledge and Vaccine Hesitancy of Czech Healthcare Workers: A Health Belief Model (HBM)-Based Study. Vaccines 2022, 10, 2022. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.-K.; Pan, X.-F.; Wang, S.-M.; Yang, C.-X.; Gao, X.-H.; Wang, Z.-Z.; Li, M.; Ren, Z.-F.; Zhao, F.-H.; Qiao, Y.-L. Perceptions and acceptability of HPV vaccination among parents of young adolescents: A multicenter national survey in China. Vaccine 2013, 31, 3244–3249. [Google Scholar] [CrossRef]
- Brown, B.; Blas, M.M.; Heidari, O.; Carcamo, C.; Halsey, N.A. Reported changes in sexual behaviour and human papillomavirus knowledge in Peruvian female sex workers following participation in a human papillomavirus vaccine trial. Int. J. STD AIDS 2013, 24, 531–535. [Google Scholar] [CrossRef]
- Harapan, H.; Setiawan, A.M.; Yufika, A.; Anwar, S.; Wahyuni, S.; Asrizal, F.W.; Sufri, M.R.; Putra, R.P.; Wijayanti, N.P.; Salwiyadi, S.; et al. Physicians’ willingness to be vaccinated with a smallpox vaccine to prevent monkeypox viral infection: A cross-sectional study in Indonesia. Clin. Epidemiol. Glob. Health 2020, 8, 1259–1263. [Google Scholar] [CrossRef] [PubMed]
- Harapan, H.; Wagner, A.L.; Yufika, A.; Setiawan, A.M.; Anwar, S.; Wahyuni, S.; Asrizal, F.W.; Sufri, M.R.; Putra, R.P.; Wijayanti, N.P.; et al. Acceptance and willingness to pay for a hypothetical vaccine against monkeypox viral infection among frontline physicians: A cross-sectional study in Indonesia. Vaccine 2020, 38, 6800–6806. [Google Scholar] [CrossRef]
- Mutisya, E.M.; Mutua, G.; Nyasani, D.; Nduta, H.; Kabuti, R.W.; Muturi-Kioi, V.; Omosa-Manyonyi, G.; Abaasa, A.; Lindan, K.; Price, M.A.; et al. Willingness to participate in future HIV vaccine trials among men who have sex with men and female sex workers living in Nairobi, Kenya. PLoS ONE 2020, 15, e0238028. [Google Scholar] [CrossRef]
- Delaney, K.P.; Sanchez, T.; Hannah, M.; Edwards, O.W.; Carpino, T.; Agnew-Brune, C.; Renfro, K.; Kachur, R.; Carnes, N.; DiNenno, E.A.; et al. Strategies Adopted by Gay, Bisexual, and Other Men Who Have Sex with Men to Prevent Monkeypox virus Transmission—United States, August 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 1126–1130. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Category | Frequency | Percentage |
|---|---|---|---|
| Gender identity | Cisgender male | 148 | 96.1 |
| Transgender female | 6 | 3.9 | |
| Marital status | Not single | 83 | 53.9 |
| Single | 71 | 46.1 | |
| Sexual orientation | Heterosexual | 91 | 59.1 |
| Non-heterosexual | 63 | 40.9 | |
| Educational level | College or above | 61 | 39.6 |
| High school or below | 93 | 60.4 | |
| Region | Urban | 139 | 90.3 |
| Rural | 15 | 9.7 | |
| Employment | Employed or retired | 140 | 90.9 |
| Unemployed | 14 | 9.1 | |
| Monthly income (CNY) | <5000 | 41 | 26.6 |
| >9990 | 27 | 17.5 | |
| 5000–9999 | 57 | 37.0 | |
| No income | 29 | 18.8 | |
| History of chronic diseases | No | 123 | 79.9 |
| Yes | 31 | 20.1 | |
| Self-reported STD history | No | 9 | 5.8 |
| Yes | 145 | 94.2 | |
| Have anxiety symptoms | No | 139 | 90.3 |
| Yes | 15 | 9.7 | |
| Have depression symptoms | No | 125 | 81.2 |
| Yes | 29 | 18.8 |
| Variables | Category | Poor Knowledge (N = 78) | Good Knowledge (N = 76) | AOR * (Multivariable) |
|---|---|---|---|---|
| Willing to receive mpox vaccination | No | 33 (42.3%) | 24 (31.6%) | |
| Yes | 45 (57.7%) | 52 (68.4%) | 2.51 (1.14–5.54, p = 0.023) | |
| Employment | Employed or retired | 75 (96.2%) | 65 (85.5%) | |
| Unemployed | 3 (3.8%) | 11 (14.5%) | 5.01 (1.21–20.70, p = 0.026) | |
| History of chronic diseases | No | 59 (75.6%) | 64 (84.2%) | |
| Yes | 19 (24.4%) | 12 (15.8%) | 0.43 (0.15–1.29, p = 0.133) | |
| Marital status | Not single | 49 (62.8%) | 34 (44.7%) | |
| Single | 29 (37.2%) | 42 (55.3%) | 2.46 (1.22–4.97, p = 0.012) | |
| Sexual orientation | Heterosexual | 41 (52.6%) | 50 (65.8%) | |
| Non-heterosexual | 37 (47.4%) | 26 (34.2%) | 0.51 (0.21–1.26, p = 0.146) | |
| Gender identity | Cisgender male | 76 (97.4%) | 72 (94.7%) | |
| Transgender female | 2 (2.6%) | 4 (5.3%) | 4.77 (0.73–31.03, p = 0.102) |
| Variables | Category | No (N = 57) | Yes (N = 97) | AOR * (Multivariable) |
|---|---|---|---|---|
| Age | Mean ± SD | 21.8 ± 7.0 | 29.1 ± 10.6 | 1.06 (1.00–1.12, p = 0.035) |
| Educational level | Undergraduate or above | 17 (29.8%) | 44 (45.4%) | |
| High school or below | 40 (70.2%) | 53 (54.6%) | 0.94 (0.40–2.21, p = 0.887) | |
| History of chronic diseases | No | 56 (98.2%) | 67 (69.1%) | |
| Yes | 1 (1.8%) | 30 (30.9%) | 8.53 (1.01–71.68, p = 0.049) | |
| Ever heard of MPXV | No | 30 (52.6%) | 24 (24.7%) | |
| Yes | 27 (47.4%) | 73 (75.3%) | 1.61 (0.22–12.03, p = 0.642) | |
| Paid attention to mpox outbreak information | Never | 37 (64.9%) | 40 (41.2%) | |
| Always | 9 (15.8%) | 17 (17.5%) | 0.65 (0.16–2.71, p = 0.558) | |
| Often | 11 (19.3%) | 40 (41.2%) | 1.30 (0.35–4.80, p = 0.692) | |
| Accessed mpox information from the Internet | No | 33 (57.9%) | 35 (36.1%) | |
| Yes | 24 (42.1%) | 62 (63.9%) | 1.25 (0.22–7.18, p = 0.802) | |
| Accessed mpox information from traditional media | No | 53 (93%) | 69 (71.1%) | |
| Yes | 4 (7%) | 28 (28.9%) | 2.93 (0.75–11.45, p = 0.122) | |
| Belief that China will become a mpox endemic country | No | 52 (91.2%) | 75 (77.3%) | |
| Yes | 5 (8.8%) | 22 (22.7%) | 2.40 (0.71–8.17, p = 0.161) | |
| Belief that high-risk groups should be prioritized if mpox vaccine is in short supply | Disagree | 21 (36.8%) | 13 (13.4%) | |
| Agree | 36 (63.2%) | 84 (86.6%) | 2.57 (1.01–6.54, p = 0.048) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.; Li, Y.; Fu, L.; Zhou, X.; Wu, X.; Wang, B.; Peng, X.; Sun, Y.; Liu, Q.; Lin, Y.-F.; et al. Knowledge of Human Mpox (Monkeypox) and Attitude towards Mpox Vaccination among Male Sex Workers in China: A Cross-Sectional Study. Vaccines 2023, 11, 285. https://doi.org/10.3390/vaccines11020285
Chen Y, Li Y, Fu L, Zhou X, Wu X, Wang B, Peng X, Sun Y, Liu Q, Lin Y-F, et al. Knowledge of Human Mpox (Monkeypox) and Attitude towards Mpox Vaccination among Male Sex Workers in China: A Cross-Sectional Study. Vaccines. 2023; 11(2):285. https://doi.org/10.3390/vaccines11020285
Chicago/Turabian StyleChen, Yuanyi, Yuwei Li, Leiwen Fu, Xinyi Zhou, Xinsheng Wu, Bingyi Wang, Xin Peng, Yinghui Sun, Qi Liu, Yi-Fan Lin, and et al. 2023. "Knowledge of Human Mpox (Monkeypox) and Attitude towards Mpox Vaccination among Male Sex Workers in China: A Cross-Sectional Study" Vaccines 11, no. 2: 285. https://doi.org/10.3390/vaccines11020285