
The Impact of Rotavirus Vaccination on Discharges for Pediatric Gastroenteritis in Italy: An Eleven Year (2009–2019) Nationwide Analysis
 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Design and Data Sources
2.3. Statistical Analysis
3. Results
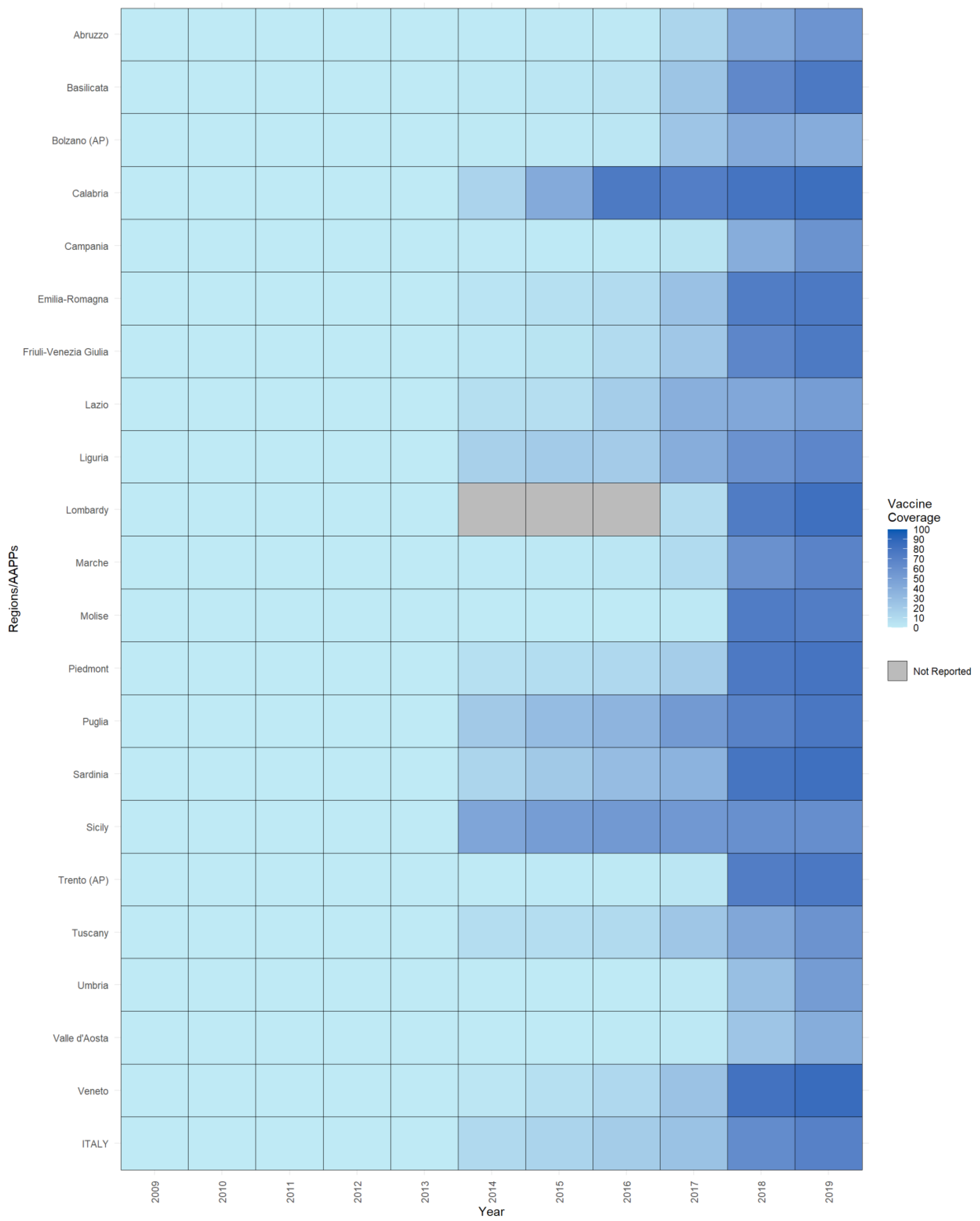
3.1. Vaccination Implementation

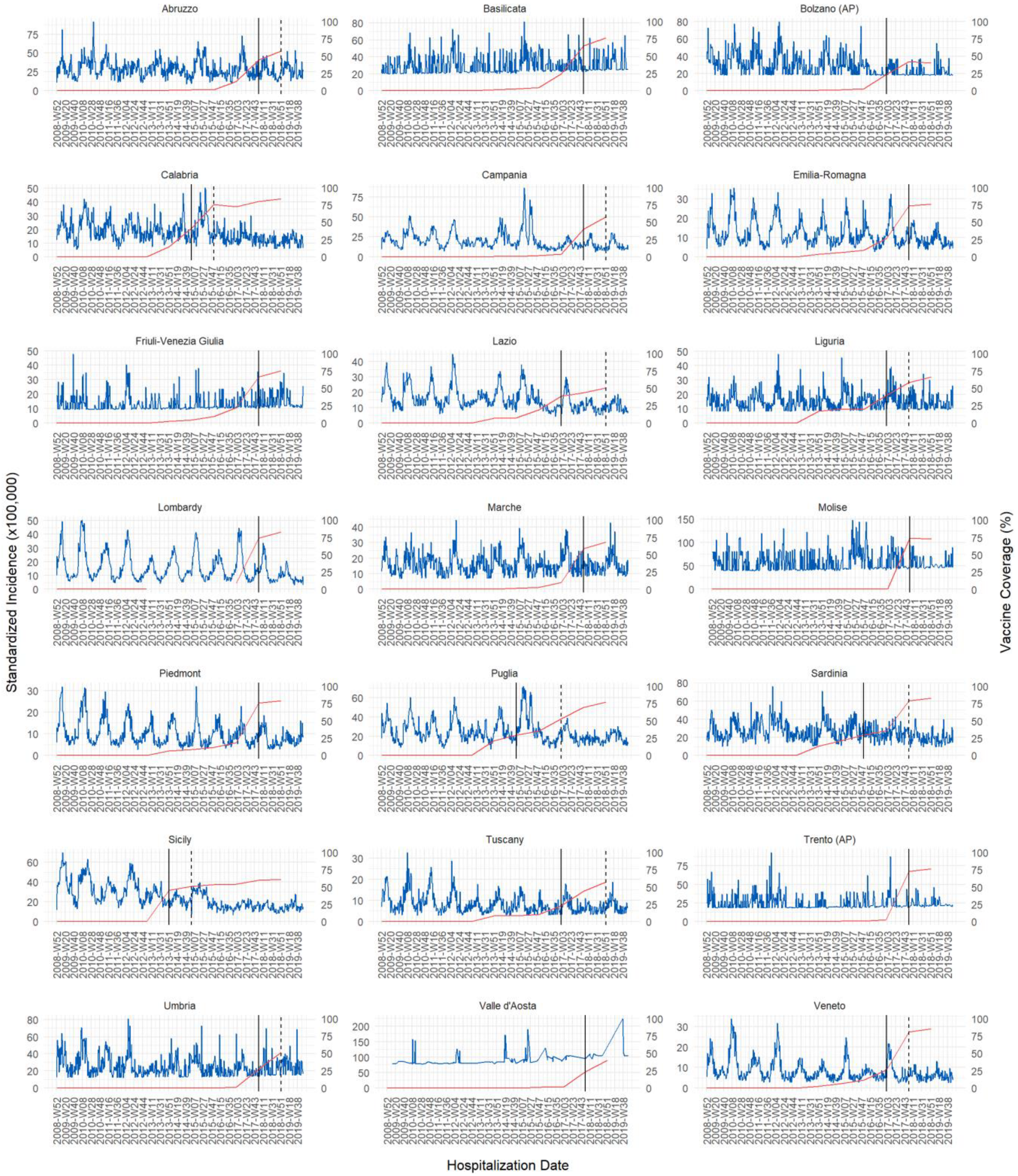
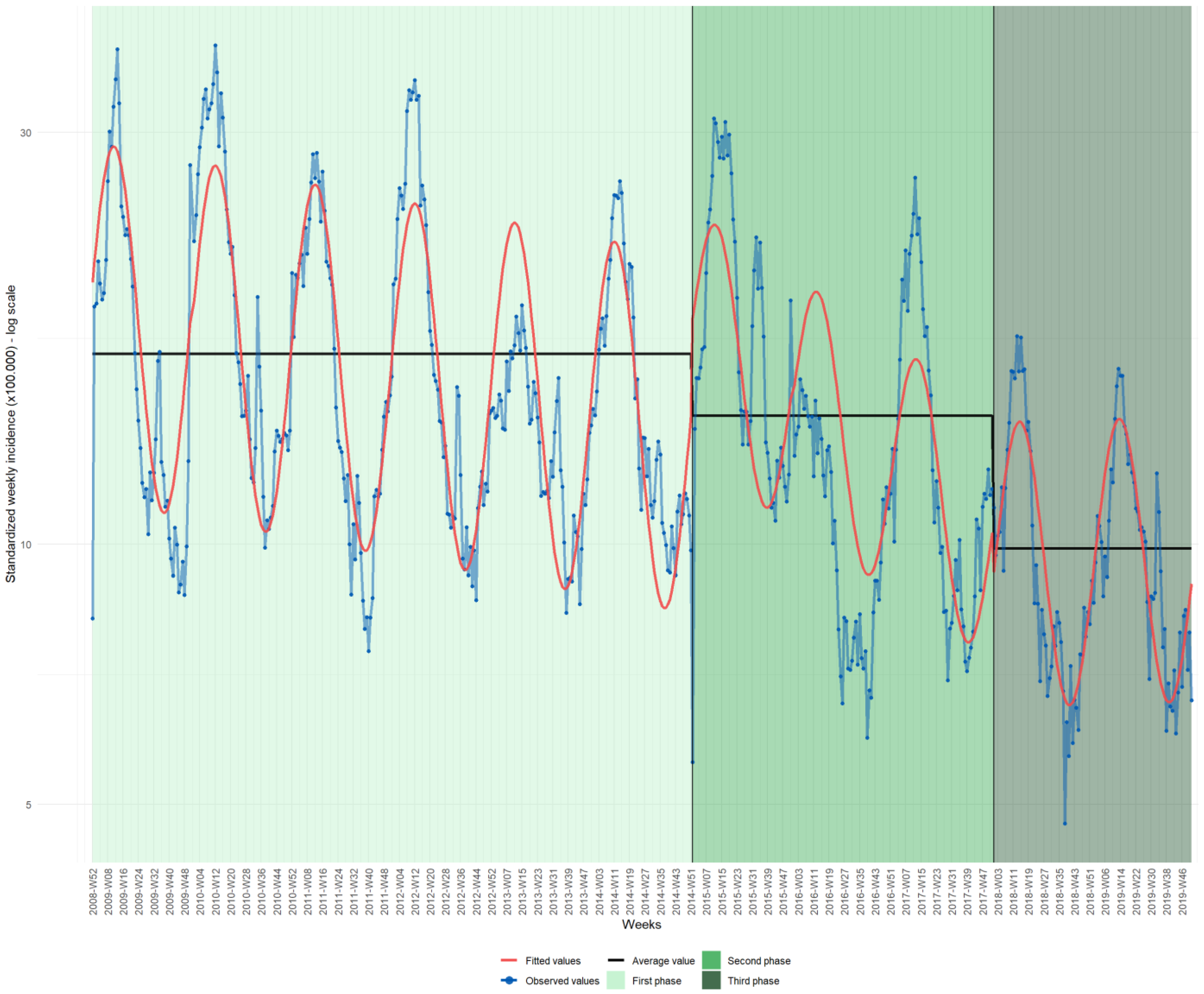
3.2. Hospital Discharges
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tate, J.E.; Burton, A.H.; Boschi-Pinto, C.; Parashar, U.D.; Agocs, M.; Serhan, F.; De Oliveira, L.; Mwenda, J.M.; Mihigo, R.; Ranjan Wijesinghe, P.; et al. Global, Regional, and National Estimates of Rotavirus Mortality in Children <5 Years of Age, 2000–2013. Clin. Infect. Dis. 2016, 62, S96–S105. [Google Scholar] [CrossRef]
- Troeger, C.; Khalil, I.A.; Rao, P.C.; Cao, S.; Blacker, B.F.; Ahmed, T.; Armah, G.; Bines, J.E.; Brewer, T.G.; Colombara, D.V.; et al. Rotavirus Vaccination and the Global Burden of Rotavirus Diarrhea among Children Younger Than 5 Years. JAMA Pediatr. 2018, 172, 958–965. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Rotavirus. Available online: https://www.who.int/teams/health-product-policy-and-standards/standards-and-specifications/vaccines-quality/rotavirus (accessed on 11 December 2022).
- Verberk, J.D.M.; van Dongen, J.A.P.; van de Kassteele, J.; Andrews, N.J.; van Gaalen, R.D.; Hahné, S.J.M.; Vennema, H.; Ramsay, M.; Braeckman, T.; Ladhani, S.; et al. Impact analysis of rotavirus vaccination in various geographic regions in Western Europe. Vaccine 2021, 39, 6671–6681. [Google Scholar] [CrossRef] [PubMed]
- Camilloni, B.; Alunno, A.; Nunzi, E.; Sarnari, L.; Ianiro, G.; Monini, M. Hospital-acquired rotavirus acute gastroenteritis in 10 consecutive seasons in Umbria (Italy). J. Med. Virol. 2020, 92, 3202–3208. [Google Scholar] [CrossRef] [PubMed]
- Pan American Health Organizazion (PAHO). Rotavirus. Available online: https://www.paho.org/en/topics/rotavirus (accessed on 11 December 2022).
- Dennehy, P.H. Rotavirus Infection. An Update on Management and Prevention. Adv. Pediatr. 2012, 59, 47–74. [Google Scholar] [CrossRef]
- Dennehy, P.H. Treatment and prevention of rotavirus infection in children. Curr. Infect. Dis. Rep. 2013, 15, 242–250. [Google Scholar] [CrossRef]
- Jonesteller, C.L.; Burnett, E.; Yen, C.; Tate, J.E.; Parashar, U.D. Effectiveness of rotavirus vaccination: A systematic review of the first decade of global postlicensure data, 2006–2016. Clin. Infect. Dis. 2017, 65, 840–850. [Google Scholar] [CrossRef]
- Kozawa, K.; Higashimoto, Y.; Kawamura, Y.; Miura, H.; Negishi, T.; Hattori, F.; Ihira, M.; Komoto, S.; Taniguchi, K.; Yoshikawa, T. Rotavirus genotypes and clinical outcome of natural infection based on vaccination status in the post-vaccine era. Hum. Vaccines Immunother. 2022, 18, 2037983. [Google Scholar] [CrossRef]
- Bergman, H.; Henschke, N.; Hungerford, D.; Pitan, F.; Ndwandwe, D.; Cunliffe, N.; Soares-Weiser, K. Vaccines for preventing rotavirus diarrhoea: Vaccines in use. Cochrane Database Syst. Rev. 2021, 11, 17. [Google Scholar] [CrossRef]
- Burnett, E.; Parashar, U.; Tate, J. Rotavirus Vaccines: Effectiveness, Safety, and Future Directions. Pediatr. Drugs 2018, 20, 223–233. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Global Use of Rotavirus Vaccines Recommended. Available online: https://apps.who.int/mediacentre/news/releases/2009/rotavirus_vaccines_20090605/en/index.html (accessed on 11 December 2022).
- Aliabadi, N.; Antoni, S.; Mwenda, J.M.; Weldegebriel, G.; Biey, J.N.M.; Cheikh, D.; Fahmy, K.; Teleb, N.; Ashmony, H.A.; Ahmed, H.; et al. AL Global impact of rotavirus vaccine introduction on rotavirus hospitalisations among children under 5 years of age, 2008–2016: Findings from the Global Rotavirus Surveillance Network. Lancet Glob. Health 2019, 7, 678–687. [Google Scholar] [CrossRef]
- de Hoog, M.L.A.; Vesikari, T.; Giaquinto, C.; Huppertz, H.I.; Martinon-Torres, F.; Bruijning-Verhagen, P. Report of the 5th European expert meeting on rotavirus vaccination (EEROVAC). Hum. Vaccines Immunother. 2018, 14, 1027–1034. [Google Scholar] [CrossRef] [PubMed]
- Costantino, C.; Restivo, V.; Tramuto, F.; Casuccio, A.; Vitale, F. Universal rotavirus vaccination program in Sicily: Reduction in health burden and cost despite low vaccination coverage. Hum. Vaccines Immunother. 2018, 14, 2297–2302. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control (ECDC). ECDC Expert Opinion on Rotavirus Vaccination in Infancy; ECDC: Stockholm, Sweden, 2017; ISBN 9789294980847.
- VIEW-Hub by IVAC Rotavirus Vaccine-Introduction and Use-Current Vaccine Intro Status. Available online: https://view-hub.org/vaccine/rota (accessed on 12 April 2023).
- European Observatory on Health Systems and Policies. Decentralization in Health Care: Strategies and Outcomes; Saltman, R.B., Bankauskaite, V., Vrangbaek, K., Eds.; McGraw-Hill: Berkshire, UK, 2007. [Google Scholar]
- Gazzetta Ufficiale della Repubblica Italiana. Legge 31 Luglio 2017, n. 119. Conversione in Legge, Con Modificazioni, del Decreto-Legge 7 Giugno 2017, n. 73, Recante Disposizioni Urgenti in Materia di Prevenzione Vaccinale. (17G00132). GU Serie Generale n. 182 del 05-08-2017; Gazzetta Ufficiale della Repubblica Italiana: Roma, Italy, 2017; pp. 1–12. [Google Scholar]
- Ministry of Health. Piano Nazionale Della Prevenzione Vaccinale (PNPV) 2017–2019; Ministry of Health: Roma, Italy, 2017; pp. 1–22.
- Ministry of Health. Vaccinazioni Dell’età Pediatrica e Dell’adolescenza—Coperture Vaccinali. Available online: https://www.salute.gov.it/portale/documentazione/p6_2_8_3_1.jsp?lingua=italiano&id=20 (accessed on 11 December 2022).
- Martinelli, D.; Fortunato, F.; Marchetti, F.; Prato, R. Rotavirus vaccine administration patterns in Italy: Potential impact on vaccine coverage, compliance and adherence. Hum. Vaccines Immunother. 2021, 17, 1546–1551. [Google Scholar] [CrossRef]
- Di Pietro, A.; Visalli, G.; Antonuccio, G.M.; Facciolà, A. Today’s vaccination policies in Italy: The National Plan for Vaccine Prevention 2017–2019 and the Law 119/2017 on the mandatory vaccinations. Ann. Ig. Med. Prev. Comunita 2019, 31, 54–64. [Google Scholar]
- Dettori, S.; Cortesia, I.; Mariani, M.; Opisso, A.; Mesini, A.; Saffioti, C.; Castagnola, E. Impact of rotavirus vaccine in reducing hospitalization rates in pediatric patients: A single center experience in Italy. Hum. Vaccines Immunother. 2021, 17, 5646–5649. [Google Scholar] [CrossRef]
- Vitale, F.; Tramuto, F.; Amodio, E.; Restivo, V.; Costantino, C. Results after one year of rotavirus universal mass vaccination in Sicily. Ital. J. Pediatr. 2015, 41, 4–5. [Google Scholar] [CrossRef]
- Saia, M.; Giliberti, A.; Callegaro, G.; Baldovin, T.; Busana, M.C.; Pietrobon, F.; Bertoncello, C.; Baldo, V. Hospitalisation for rotavirus gastroenteritis in the paediatric population in the Veneto Region, Italy. BMC Public Health 2010, 10, 636. [Google Scholar] [CrossRef]
- Bonanni, P.; Conforti, G.; Franco, E.; Gabutti, G.; Marchetti, F.; Mattei, A.; Prato, R.; Vitali Rosati, G.; Vitale, F. Fourteen years’ clinical experience and the first million babies protected with human live-attenuated vaccine against rotavirus disease in Italy. Hum. Vaccines Immunother. 2021, 17, 4636–4645. [Google Scholar] [CrossRef]
- Ministry of Health. La Scheda di Dimissione Ospedaliera (SDO). Available online: http://www.salute.gov.it/portale/temi/p2_6.jsp?lingua=italiano&id=1232&area=ricoveriOspedalieri&menu=vuoto. (accessed on 7 May 2020).
- Sabbatucci, M.; Odone, A.; Signorelli, C.; Siddu, A.; Silenzi, A.; Maraglino, F.P.; Rezza, G. Childhood Immunisation Coverage during the COVID-19 Epidemic in Italy. Vaccines 2022, 10, 120. [Google Scholar] [CrossRef]
- Bencina, G.; Costantino, C.; Mameli, C.; Sabale, U.; Murtagh, J.; Newman, R.; Ahern, A.; Bhaila, R.; Sanchez, A.O.; Martinon-Torres, F.; et al. Real-world impact of rotavirus vaccination in European healthcare settings: A systematic literature review. Expert Rev. Vaccines 2022, 21, 1121–1136. [Google Scholar] [CrossRef] [PubMed]
- Karafillakis, E.; Hassounah, S.; Atchison, C. Effectiveness and impact of rotavirus vaccines in Europe, 2006–2014. Vaccine 2015, 33, 2097–2107. [Google Scholar] [CrossRef] [PubMed]
- Cohen, R.; Martinón-Torres, F.; Posiuniene, I.; Benninghoff, B.; Oh, K.B.; Poelaert, D. The Value of Rotavirus Vaccination in Europe: A Call for Action. Infect. Dis. Ther. 2023, 12, 9–29. [Google Scholar] [CrossRef] [PubMed]
- Buttery, J.P.; Lambert, S.B.; Grimwood, K.; Nissen, M.D.; Field, E.J.; MacArtney, K.K.; Akikusa, J.D.; Kelly, J.J.; Kirkwood, C.D. Reduction in rotavirus-associated acute gastroenteritis following introduction of rotavirus vaccine into australia’s national childhood vaccine schedule. Pediatr. Infect. Dis. J. 2011, 30, 25–29. [Google Scholar] [CrossRef]
- Tate, J.E.; Cortese, M.M.; Payne, D.C.; Curns, A.T.; Yen, C.; Esposito, D.H.; Cortes, J.E.; Lopman, B.A.; Patel, M.M.; Gentsch, J.R.; et al. Uptake, impact, and effectiveness of rotavirus vaccination in the United States: Review of the first 3 years of postlicensure data. Pediatr. Infect. Dis. J. 2011, 30, 56–60. [Google Scholar] [CrossRef]
- Mattei, A.; Sbarbati, M.; Fiasca, F.; Angelone, A.M.; Mazzei, M.C.; di Orio, F. Temporal trends in hospitalization for rotavirus gastroenteritis: A nationwide study in Italy, 2005–2012. Hum. Vaccines Immunother. 2016, 12, 534–539. [Google Scholar] [CrossRef]
- Du, Y.; Chen, C.; Zhang, X.; Yan, D.; Jiang, D.; Liu, X.; Yang, M.; Ding, C.; Lan, L.; Hecht, R.; et al. Global burden and trends of rotavirus infection-associated deaths from 1990 to 2019: An observational trend study. Virol. J. 2022, 19, 166. [Google Scholar] [CrossRef]
- Payne, D.C.; Staat, M.A.; Edwards, K.M.; Szilagyi, P.G.; Weinberg, G.A.; Hall, C.B.; Chappell, J.; Curns, A.T.; Wikswo, M.; Tate, J.E.; et al. Direct and indirect effects of rotavirus vaccination upon childhood hospitalizations in 3 US counties, 2006–2009. Clin. Infect. Dis. 2011, 53, 245–253. [Google Scholar] [CrossRef]
- Causey, K.; Fullman, N.; Sorensen, R.J.D.; Galles, N.C.; Zheng, P.; Aravkin, A.; Danovaro-Holliday, M.C.; Martinez-Piedra, R.; Sodha, S.V.; Velandia-González, M.P.; et al. Estimating global and regional disruptions to routine childhood vaccine coverage during the COVID-19 pandemic in 2020: A modelling study. Lancet 2021, 398, 522–534. [Google Scholar] [CrossRef]
- Apte, A.; Roy, S.; Bavdekar, A.; Juvekar, S.; Hirve, S. Facilitators and barriers for use of rotavirus vaccine amongst various stakeholders and its implications for Indian context–A systematic review. Hum. Vaccines Immunother. 2018, 14, 2760–2767. [Google Scholar] [CrossRef]
- Marchetti, F.; Vetter, V.; Conforti, G.; Esposito, S.; Bonanni, P. Parents’ insights after pediatric hospitalization due to rotavirus gastroenteritis in Italy. Hum. Vaccines Immunother. 2017, 13, 2155–2159. [Google Scholar] [CrossRef] [PubMed]
- Restivo, V.; Costantino, C.; Giorgianni, G.; Cuccia, M.; Tramuto, F.; Corsello, G.; Casuccio, A.; Vitale, F. Case–control study on intestinal intussusception: Implications for anti-rotavirus vaccination. Expert Rev. Vaccines 2018, 17, 1135–1141. [Google Scholar] [CrossRef] [PubMed]
- Costantino, C.; Conforto, A.; Bonaccorso, N.; Cimino, L.; Sciortino, M.; Palermo, M.; Maiolo, K.; Tina, L.G.; Betta, P.M.; Caracciolo, M.; et al. Safety of Rotavirus Vaccination in Preterm Infants Admitted in Neonatal Intensive Care Units in Sicily, Italy: A Multicenter Observational Study. Vaccines 2023, 11, 718. [Google Scholar] [CrossRef] [PubMed]
- Napolitano, F.; Adou, A.A.; Vastola, A.; Angelillo, I.F. Rotavirus infection and vaccination: Knowledge, beliefs, and behaviors among parents in Italy. Int. J. Environ. Res. Public Health 2019, 16, 1807. [Google Scholar] [CrossRef]
- Siena, L.M.; Isonne, C.; Sciurti, A.; De Blasiis, M.R.; Migliara, G.; Marzuillo, C.; De Vito, C.; Villari, P.; Baccolini, V. The Association of Health Literacy with Intention to Vaccinate and Vaccination Status: A Systematic Review. Vaccines 2022, 10, 1832. [Google Scholar] [CrossRef]
- Rosso, A.; Massimi, A.; Pitini, E.; Nardi, A.; Baccolini, V.; Marzuillo, C.; De Vito, C.; Villari, P. Factors affecting the vaccination choices of pregnant women for their children: A systematic review of the literature. Hum. Vaccines Immunother. 2020, 16, 1969–1980. [Google Scholar] [CrossRef]
- Sindoni, A.; Baccolini, V.; Adamo, G.; Massimi, A.; Migliara, G.; De Vito, C.; Marzuillo, C.; Villari, P. Effect of the mandatory vaccination law on measles and rubella incidence and vaccination coverage in Italy (2013–2019). Hum. Vaccines Immunother. 2022, 18, 1950505. [Google Scholar] [CrossRef]
- Mita, V.; Arigliani, M.; Zaratti, L.; Arigliani, R.; Franco, E. Italian physicians’ opinions on rotavirus vaccine implementation. Pathogens 2017, 6, 56. [Google Scholar] [CrossRef]
- Gualano, M.R.; Thomas, R.; Gili, R.; Scaioli, G.; Voglino, G.; Zotti, C. Cost-effectiveness estimates of vaccination against rotavirus in Piedmont, Italy. J. Infect. Public Health 2018, 11, 867–872. [Google Scholar] [CrossRef]
- Favaretti, C.; Di Pietro, M.L.; Kheiraoui, F.; Capri, S.; Specchia, M.L.; Cadeddu, C.; Lovato, E.; Di Nardo, F.; Ferriero, A.M.; Mancuso, A.; et al. Health Technology Assessment della vaccinazione anti-rotavirus con il vaccino Rotarix. Quad. Ital. J. Public Health 2014, 3, 1–80. [Google Scholar]
- Ricciardi, W.; Tarricone, R. The evolution of the Italian National Health Service. Lancet 2021, 398, 2193–2206. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Frequency | Percentage | |
|---|---|---|
| Sex | ||
| Female | 125,204 | 45.2 |
| Male | 151,777 | 54.8 |
| Age in months | ||
| 0–11 | 72,126 | 26.0 |
| 12–23 | 82,438 | 29.8 |
| 24–35 | 51,834 | 18.7 |
| 36–47 | 32,283 | 11.7 |
| 48–59 | 21,802 | 7.9 |
| 60–71 | 16,498 | 6.0 |
| ICD-9-CM codes | ||
| 00861 | 82,590 | 29.8 |
| 0090 | 33,161 | 12.0 |
| 0091 | 89,080 | 32.2 |
| 0092 | 4810 | 1.7 |
| 0093 | 7449 | 2.7 |
| 5589 | 46,586 | 16.8 |
| 5645 | 351 | 0.1 |
| 78791 | 12,954 | 4.7 |
| Year | Raw Incidence (×100,000 Persons) | Standardized Incidence (×100,000 Persons) |
|---|---|---|
| 2009 | 17.8 | 17.2 |
| 2010 | 20.7 | 20.1 |
| 2011 | 16.7 | 16.2 |
| 2012 | 18.1 | 17.7 |
| 2013 | 13.6 | 13.3 |
| 2014 | 15.4 | 15.2 |
| 2015 | 18.7 | 18.6 |
| 2016 | 10.5 | 10.5 |
| 2017 | 13.2 | 13.2 |
| 2018 | 9.9 | 9.8 |
| 2019 | 10.0 | 9.9 |
| AGE: Acute Gastroenteritis | ||
| Year | Forecasted Rates | Actual Rates | Difference between Rates | % of Avoided Discharges * |
|---|---|---|---|---|
| 2015 | 13.9 | 18.6 | −4.7 | −34.2 |
| 2016 | 13.2 | 10.5 | 2.7 | 20.4 |
| 2017 | 12.5 | 13.2 | −0.7 | −5.2 |
| 2018 | 11.9 | 9.8 | 2.1 | 17.3 |
| 2019 | 11.3 | 9.9 | 1.4 | 12.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Isonne, C.; Petrone, D.; Del Manso, M.; Iera, J.; Caramia, A.; Bandini, L.; Fadda, G.; Grossi, A.; Baccolini, V.; Costantino, C.; et al. The Impact of Rotavirus Vaccination on Discharges for Pediatric Gastroenteritis in Italy: An Eleven Year (2009–2019) Nationwide Analysis. Vaccines 2023, 11, 1037. https://doi.org/10.3390/vaccines11061037
Isonne C, Petrone D, Del Manso M, Iera J, Caramia A, Bandini L, Fadda G, Grossi A, Baccolini V, Costantino C, et al. The Impact of Rotavirus Vaccination on Discharges for Pediatric Gastroenteritis in Italy: An Eleven Year (2009–2019) Nationwide Analysis. Vaccines. 2023; 11(6):1037. https://doi.org/10.3390/vaccines11061037
Chicago/Turabian StyleIsonne, Claudia, Daniele Petrone, Martina Del Manso, Jessica Iera, Alessandra Caramia, Lorenzo Bandini, Giulia Fadda, Adriano Grossi, Valentina Baccolini, Claudio Costantino, and et al. 2023. "The Impact of Rotavirus Vaccination on Discharges for Pediatric Gastroenteritis in Italy: An Eleven Year (2009–2019) Nationwide Analysis" Vaccines 11, no. 6: 1037. https://doi.org/10.3390/vaccines11061037