
The Effectiveness of Therapeutic Vaccines for the Treatment of Cervical Intraepithelial Neoplasia 3: A Systematic Review and Meta-Analysis
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection, Inclusion and Exclusion Criteria and Data Extration
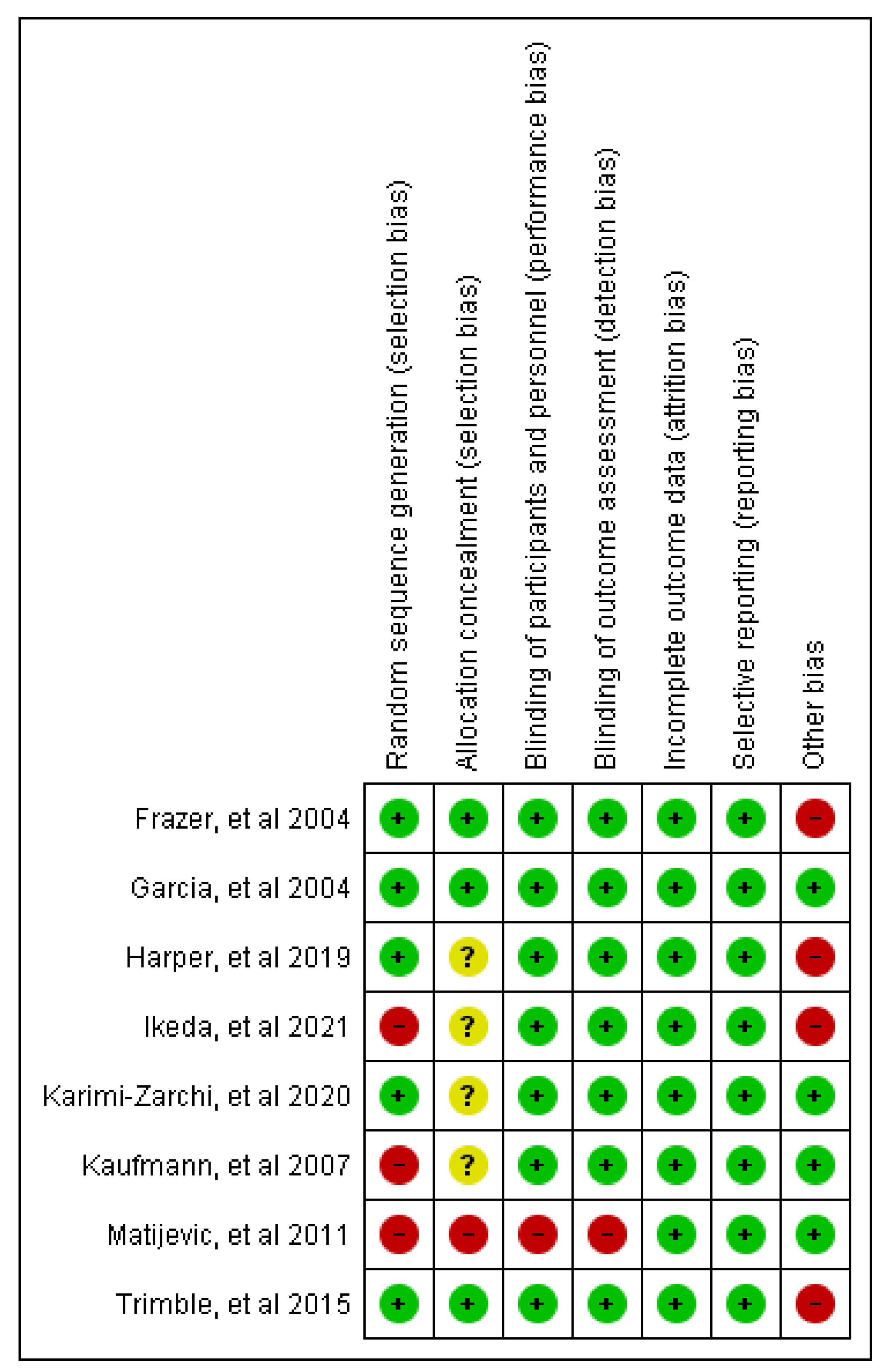
2.3. Risk of Bias Assessment
2.4. Statistical Analyses
3. Results
3.1. Study Identification and Selection
3.2. Included Studies and Characteristics
3.3. Risk of Bias Assessment
3.4. Outcomes
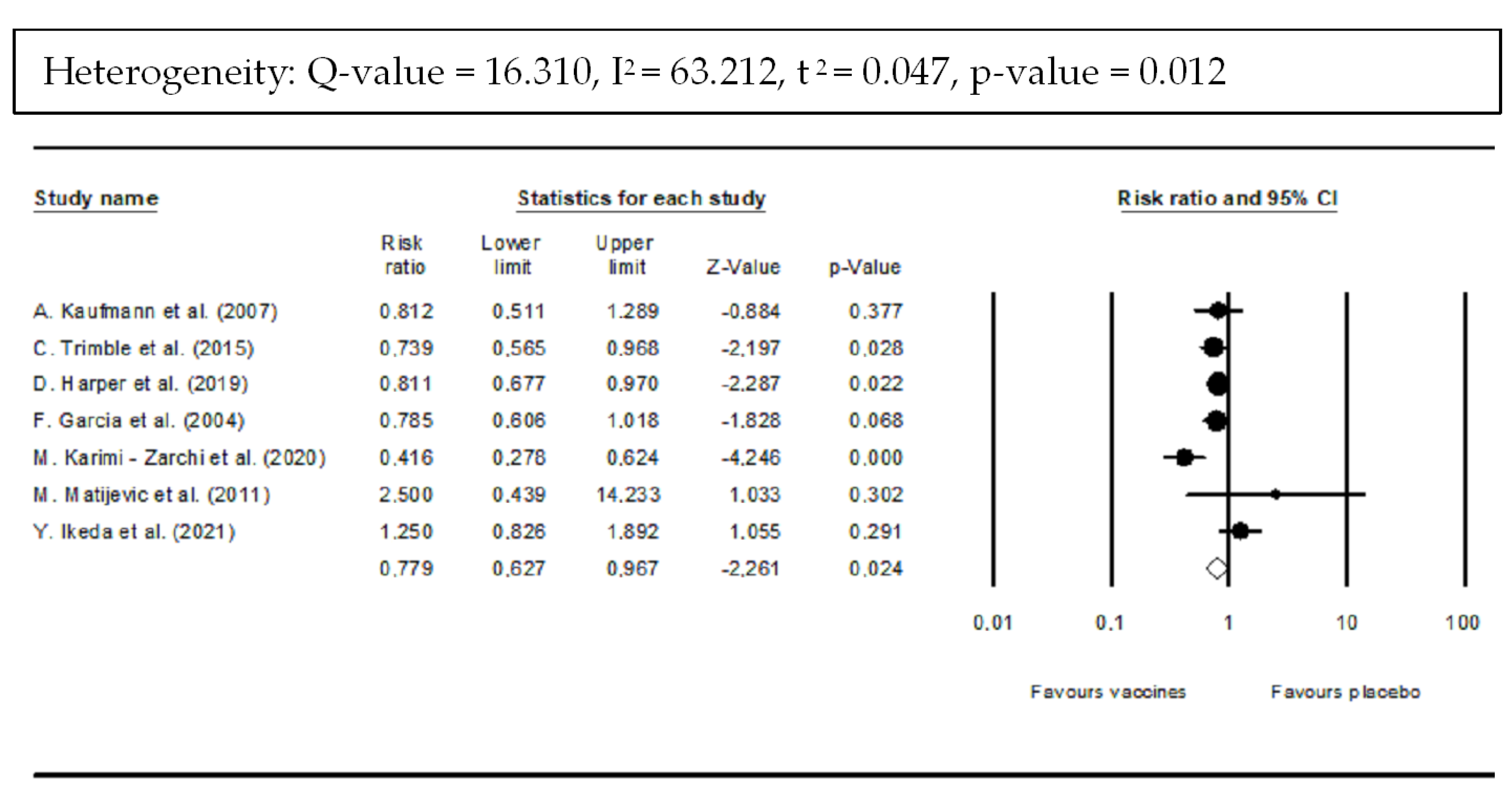
3.4.1. Clinical Efficacy Was Evaluated According to the Histopathological Regression to CIN ≤ 1, and Vaccine Efficacy for Complete Resolution
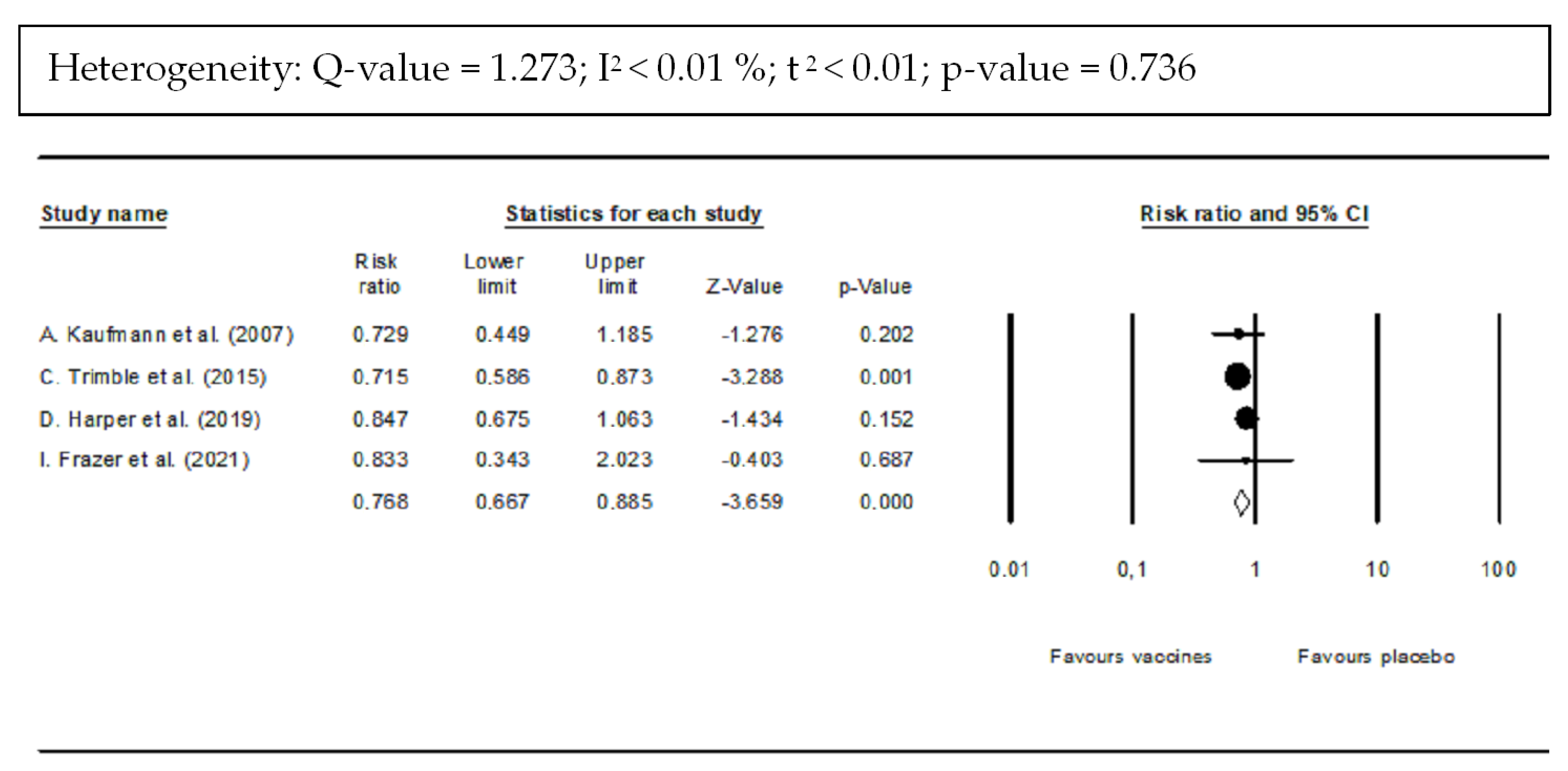
3.4.2. DNA Clearance
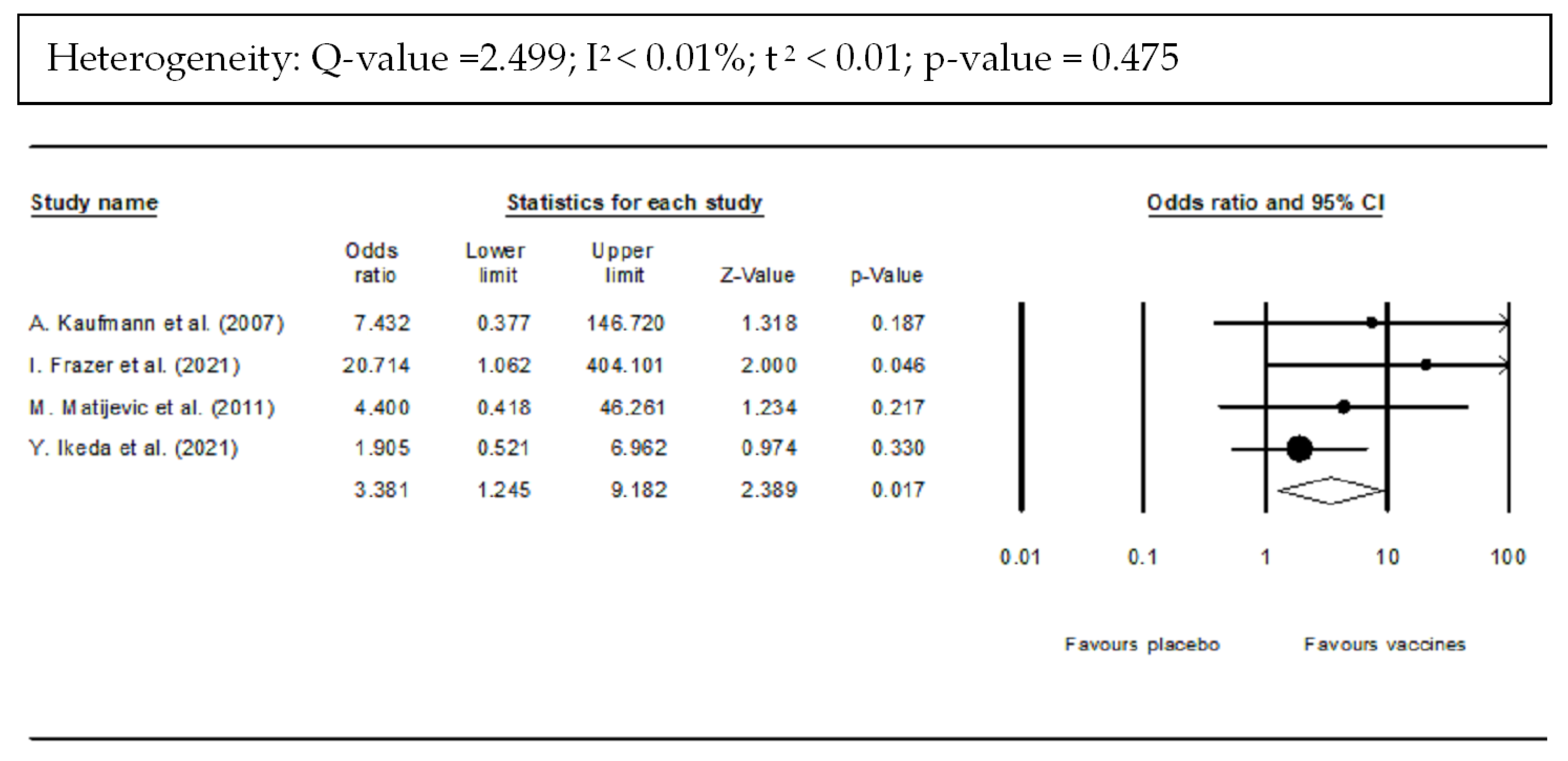
3.4.3. Immunogenicity
3.4.4. Safety
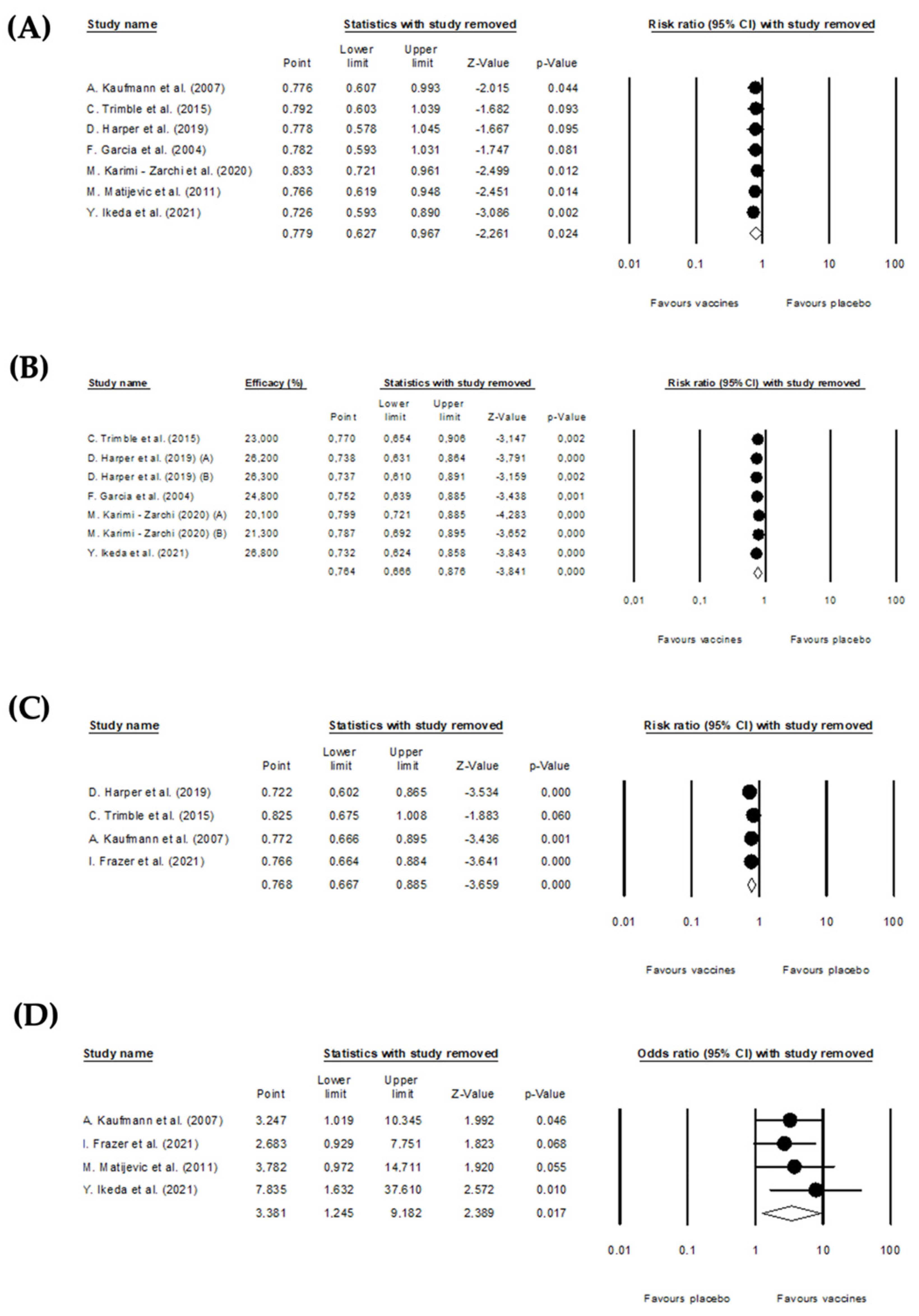
3.5. Sensitivity Analysis
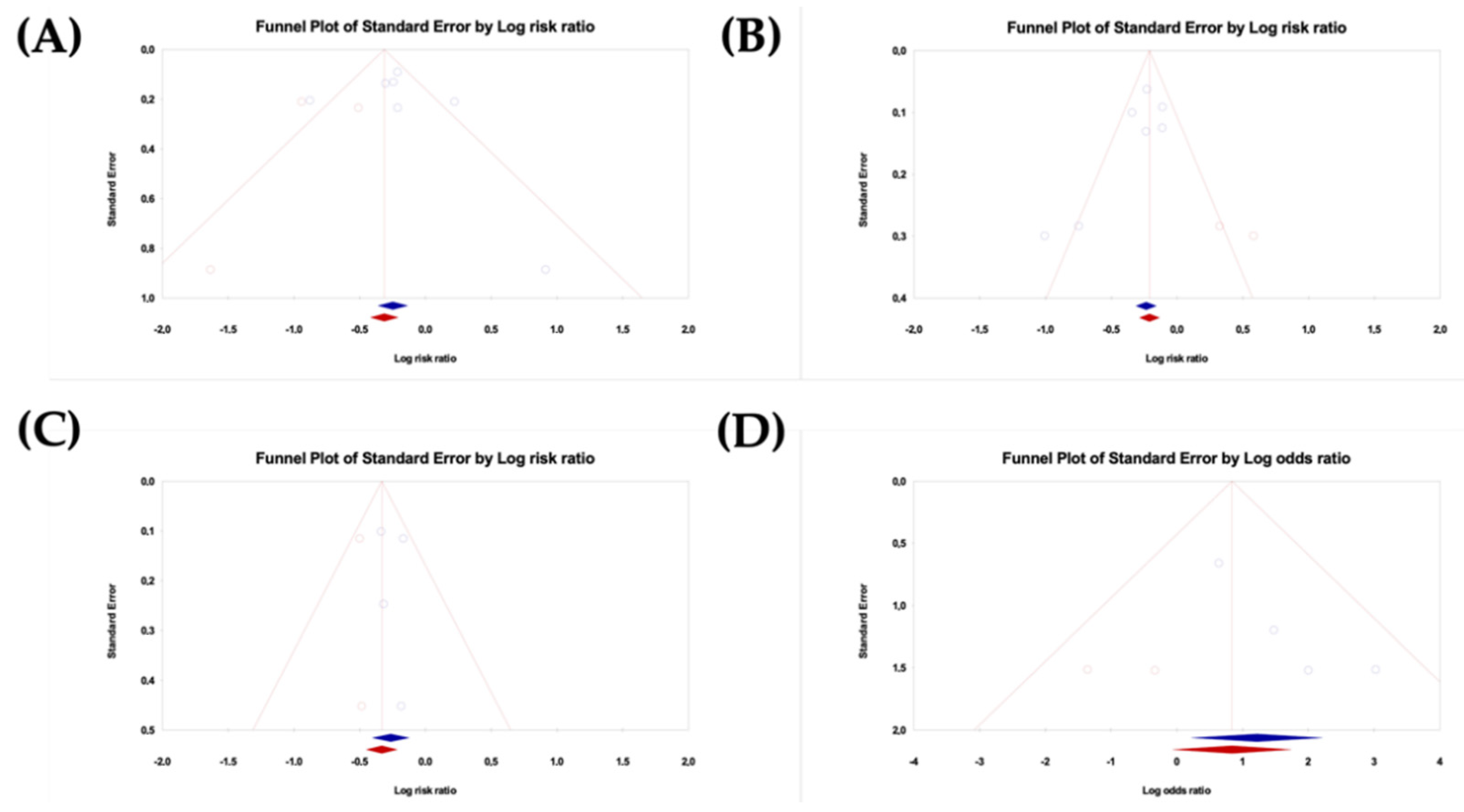
3.6. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McLaughlin-Drubin, M.E.; Munger, K. Viruses Associated with Human Cancer Margaret. Biochim. Biophys. Acta 2008, 1782, 127–150. [Google Scholar] [CrossRef] [PubMed]
- zur Hausen, H. Viruses in Human Cancers. Science 1991, 254, 1167–1173. [Google Scholar] [CrossRef] [PubMed]
- Almeida, A.M.; Queiroz, J.A.; Sousa, F.; Sousa, Â. Cervical Cancer and HPV Infection: Ongoing Therapeutic Research to Counteract the Action of E6 and E7 Oncoproteins. Drug Discov. Today 2019, 24, 2044–2057. [Google Scholar] [CrossRef] [PubMed]
- WHO. Cervix Uteri Source: Globocan 2020. Int. Agency Res. Cancer 2020, 419, 1–2. [Google Scholar]
- Chang, H.K.; Seo, S.S.; Myong, J.P.; Yu, Y.L.; Byun, S.W. Incidence and Costs of Cervical Intraepithelial Neoplasia in the Korean Population. J. Gynecol. Oncol. 2019, 30, e37. [Google Scholar] [CrossRef]
- Henk, H.J.; Insinga, R.P.; Singhal, P.K.; Darkow, T. Incidence and Costs of Cervical Intraepithelial Neoplasia in a US Commercially Insured Population. J. Low. Genit. Tract Dis. 2010, 14, 29–36. [Google Scholar] [CrossRef]
- Choi, Y.J.; Park, J.S. Clinical Significance of Human Papillomavirus Genotyping. J. Gynecol. Oncol. 2016, 27, e21. [Google Scholar] [CrossRef]
- Szymonowicz, K.A.; Chen, J. Biological and Clinical Aspects of HPV-Related Cancers. Cancer Biol. Med. 2020, 17, 864–878. [Google Scholar] [CrossRef]
- Moody, C.A. Regulation of the Innate Immune Response during the Human Papillomavirus Life Cycle. Viruses 2022, 14, 1797. [Google Scholar] [CrossRef]
- Sales, K.J. Human Papillomavirus and Cervical Cancer. Cancer Inflamm. Mech. Chem. Biol. Clin. Asp. 2014, 16, 165–180. [Google Scholar]
- Franconi, R.; Massa, S.; Paolini, F.; Vici, P.; Venuti, A. Plant-Derived Natural Compounds in Genetic Vaccination and Therapy for HPV-Associated Cancers. Cancers 2020, 12, 3101. [Google Scholar] [CrossRef]
- Mittal, S.; Banks, L. Molecular Mechanisms Underlying Human Papillomavirus E6 and E7 Oncoprotein-Induced Cell Transformation. Mutat. Res. Rev. Mutat. Res. 2017, 772, 23–35. [Google Scholar] [CrossRef]
- Martínez-Ramírez, I.; Carrillo-García, A.; Contreras-Paredes, A.; Ortiz-Sánchez, E.; Cruz-Gregorio, A.; Lizano, M. Regulation of Cellular Metabolism by High-Risk Human Papillomaviruses. Int. J. Mol. Sci. 2018, 19, 1839. [Google Scholar] [CrossRef] [PubMed]
- Hoppe-Seyler, K.; Bossler, F.; Braun, J.A.; Herrmann, A.L.; Hoppe-Seyler, F. The HPV E6/E7 Oncogenes: Key Factors for Viral Carcinogenesis and Therapeutic Targets. Trends Microbiol. 2018, 26, 158–168. [Google Scholar] [CrossRef] [PubMed]
- White, E.A.; Kramer, R.E.; Tan, M.J.A.; Hayes, S.D.; Harper, J.W.; Howley, P.M. Comprehensive Analysis of Host Cellular Interactions with Human Papillomavirus E6 Proteins Identifies New E6 Binding Partners and Reflects Viral Diversity. J. Virol. 2012, 86, 13174–13186. [Google Scholar] [CrossRef] [PubMed]
- White, E.A.; Sowa, M.E.; Tan, M.J.A.; Jeudy, S.; Hayes, S.D.; Santha, S.; Munger, K.; Harper, J.W.; Howley, P.M. Systematic Identification of Interactions between Host Cell Proteins and E7 Oncoproteins from Diverse Human Papillomaviruses. Proc. Natl. Acad. Sci. USA 2012, 109, E260–E267. [Google Scholar] [CrossRef]
- Gomes, D.; Silvestre, S.; Duarte, A.P.; Venuti, A.; Soares, C.P.; Passarinha, L.; Sousa, Â. In Silico Approaches: A Way to Unveil Novel Therapeutic Drugs for Cervical Cancer Management. Pharmaceuticals 2021, 14, 741. [Google Scholar] [CrossRef]
- Muñoz-Bello, J.O.; Carrillo-García, A.; Lizano, M. Epidemiology and Molecular Biology of HPV Variants in Cervical Cancer: The State of the Art in Mexico. Int. J. Mol. Sci. 2022, 23, 8566. [Google Scholar] [CrossRef]
- Kalof, A.N.; Cooper, K. Our Approach to Squamous Intraepithelial Lesions of the Uterine Cervix. J. Clin. Pathol. 2007, 60, 449–455. [Google Scholar] [CrossRef]
- de Martel, C.; Plummer, M.; Vignat, J.; Franceschi, S. Worldwide Burden of Cancer Attributable to HPV by Site, Country and HPV Type. Int. J. Cancer 2017, 141, 664–670. [Google Scholar] [CrossRef]
- Cheng, M.A.; Farmer, E.; Huang, C.; Lin, J.; Hung, C.F.; Wu, T.C. Therapeutic DNA Vaccines for Human Papillomavirus and Associated Diseases. Hum. Gene Ther. 2018, 29, 971–996. [Google Scholar] [CrossRef] [PubMed]
- Guo, C.; Manjili, M.H.; Subjeck, J.R.; Sarkar, D.; Fisher, P.B.; Wang, X.Y. Therapeutic Cancer Vaccines. Past, Present, and Future; Academic Press Inc.: Cambridge, MA, USA, 2013; Volume 119, ISBN 9780124071902. [Google Scholar]
- Boilesen, D.R.; Nielsen, K.N.; Holst, P.J. Novel Antigenic Targets of Hpv Therapeutic Vaccines. Vaccines 2021, 9, 1262. [Google Scholar] [CrossRef] [PubMed]
- Vici, P.; Pizzuti, L.; Mariani, L.; Zampa, G.; Santini, D.; di Lauro, L.; Gamucci, T.; Natoli, C.; Marchetti, P.; Barba, M.; et al. Targeting Immune Response with Therapeutic Vaccines in Premalignant Lesions and Cervical Cancer: Hope or Reality from Clinical Studies. Expert Rev. Vaccines 2016, 15, 1327–1336. [Google Scholar] [CrossRef] [PubMed]
- Garbuglia, A.R.; Lapa, D.; Sias, C.; Capobianchi, M.R.; Del Porto, P. The Use of Both Therapeutic and Prophylactic Vaccines in the Therapy of Papillomavirus Disease. Front. Immunol. 2020, 11, 188. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 Explanation and Elaboration: Updated Guidance and Exemplars for Reporting Systematic Reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Introduction to Meta-Analysis; John Wiley & Sons, Ltd.: Cornwall, UK, 2009; ISBN 9783319149080. [Google Scholar]
- Higgins, J.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring Inconsistency in Meta-Analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Light, R.J.; Pillemer, D.B. Summing Up: The Science of Reviewing Research; Harvard University Press: Cambridge, MA, USA, 1984. [Google Scholar]
- Cooper, H.M.; Valentine, J.C.; Hedges, L.V. Handbook of Research Synthesis and Meta-Analysis, 2nd ed.; Russel Sage Foundation: New York, NY, USA, 2009; ISBN 9780871541635. [Google Scholar]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in Meta-Analysis Detected by a Simple, Graphical Test. Br. Med. J. 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R. A Nonparametric “Trim and Fill” Method of Accounting for Publication Bias in Meta-Analysis. J. Am. Stat. Assoc. 2000, 95, 89–98. [Google Scholar]
- Duval, S.; Tweedie, R. Trim and Fill: A Simple Funnel-Plot-Based Method. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Trimble, C.L.; Morrow, M.P.; Kraynyak, K.A.; Shen, X.; Dallas, M.; Yan, J.; Edwards, L. Safety, Efficacy, and Immunogenicity of VGX-3100, a Therapeutic Synthetic DNA Vaccine Targeting Human Papillomavirus 16 and 18 E6 and E7 Proteins for Cervical Intraepithelial Neoplasia 2/3: A Randomised, Double-Blind, Placebo-Controlled Phase 2b Trial. Lancet 2016, 386, 2078–2088. [Google Scholar] [CrossRef]
- Karimi-Zarchi, M.; Allahqoli, L.; Nehmati, A.; Kashi, A.M.; Taghipour-Zahir, S.; Alkatout, I. Can the Prophylactic Quadrivalent HPV Vaccine Be Used as a Therapeutic Agent in Women with CIN? A Randomized Trial. BMC Public Health 2020, 20, 274. [Google Scholar] [CrossRef] [PubMed]
- Harper, D.M.; Nieminen, P.; Donders, G.; Einstein, M.H.; Garcia, F.; Huh, W.K.; Stoler, M.H.; Glavini, K.; Attley, G.; Limacher, J.M.; et al. The Efficacy and Safety of Tipapkinogen Sovacivec Therapeutic HPV Vaccine in Cervical Intraepithelial Neoplasia Grades 2 and 3: Randomized Controlled Phase II Trial with 2.5 years of Follow-Up. Gynecol. Oncol. 2019, 153, 521–529. [Google Scholar] [CrossRef] [Green Version]
- Kaufmann, A.M.; Nieland, J.D.; Jochmus, I.; Baur, S.; Friese, K.; Gabelsberger, J.; Gieseking, F.; Gissmann, L.; Glasschröder, B.; Grubert, T.; et al. Vaccination Trial with HPV16 L1E7 Chimeric Virus-like Particles in Women Suffering from High Grade Cervical Intraepithelial Neoplasia (CIN 2/3). Int. J. Cancer 2007, 121, 2794–2800. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, Y.; Adachi, K.; Tomio, K.; Eguchi-Kojima, S.; Tsuruga, T.; Uchino-Mori, M.; Taguchi, A.; Komatsu, A.; Nagamatsu, T.; Oda, K.; et al. A Placebo-Controlled, Double-Blind Randomized (Phase IIB) Trial of Oral Administration with HPV16 E7-Expressing Lactobacillus, GLBL101c, for the Treatment of Cervical Intraepithelial Neoplasia Grade 2 (CIN2). Vaccines 2021, 9, 329. [Google Scholar] [CrossRef]
- Frazer, I.H.; Quinn, M.; Nicklin, J.L.; Tan, J.; Perrin, L.C.; Ng, P.; O’Connor, V.M.; White, O.; Wendt, N.; Martin, J.; et al. Phase 1 Study of HPV16-Specific Immunotherapy with E6E7 Fusion Protein and ISCOMATRIXTM Adjuvant in Women with Cervical Intraepithelial Neoplasia. Vaccine 2004, 23, 172–181. [Google Scholar] [CrossRef] [PubMed]
- Garcia, F.; Petry, K.U.; Muderspach, L.; Gold, M.A.; Braly, P.; Crum, C.P.; Magill, M.; Silverman, M.; Urban, R.G.; Hedley, M.L.; et al. ZYC101a for Treatment of High-Grade Cervical Intraepithelial Neoplasia: A Randomized Controlled Trial. Obstet. Gynecol. 2004, 103, 317–326. [Google Scholar] [CrossRef]
- Matijevic, M.; Hedley, M.L.; Urban, R.G.; Chicz, R.M.; Lajoie, C.; Luby, T.M. Immunization with a Poly (Lactide Co-Glycolide) Encapsulated Plasmid DNA Expressing Antigenic Regions of HPV 16 and 18 Results in an Increase in the Precursor Frequency of T Cells That Respond to Epitopes from HPV 16, 18, 6 and 11. Cell. Immunol. 2011, 270, 62–69. [Google Scholar] [CrossRef]
- Mohsen, M.O.; Zha, L.; Cabral-Miranda, G.; Bachmann, M.F. Major Findings and Recent Advances in Virus–like Particle (VLP)-Based Vaccines. Semin. Immunol. 2017, 34, 123–132. [Google Scholar] [CrossRef]
- Josefsberg, J.O.; Buckland, B. Vaccine Process Technology. Biotechnol. Bioeng. 2012, 109, 1443–1460. [Google Scholar] [CrossRef]
- Haupt, R.M.; Wheeler, C.M.; Brown, D.R.; Garland, S.M.; Ferris, D.G.; Paavonen, J.A.; Lehtinen, M.O.; Steben, M.; Joura, E.A.; Giacoletti, K.E.D.; et al. Impact of an HPV6/11/16/18 L1 Virus-like Particle Vaccine on Progression to Cervical Intraepithelial Neoplasia in Seropositive Women with HPV16/18 Infection. Int. J. Cancer 2011, 129, 2632–2642. [Google Scholar] [CrossRef] [PubMed]
- Poo, H.; Pyo, H.M.; Lee, T.Y.; Yoon, S.W.; Lee, J.S.; Kim, C.J.; Sung, M.H.; Lee, S.H. Oral Administration of Human Papillomavirus Type 16 E7 Displayed on Lactobacillus Casei Induces E7-Specific Antitumor Effects in C57/BL6 Mice. Int. J. Cancer 2006, 119, 1702–1709. [Google Scholar] [CrossRef] [PubMed]
- Hasson, S.S.A.A.; Al-Busaidi, J.K.Z.; Sallam, T.A. The Past, Current and Future Trends in DNA Vaccine Immunisations. Asian Pac. J. Trop. Biomed. 2015, 5, 344–353. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Petrovsky, N. Molecular Mechanisms for Enhanced DNA Vaccine Immunogenicity. Expert Rev. Vaccines 2016, 15, 313–329. [Google Scholar] [CrossRef]
- Tacken, P.J.; De Vries, I.J.M.; Torensma, R.; Figdor, C.G. Dendritic-Cell Immunotherapy: From Ex Vivo Loading to in Vivo Targeting. Nat. Rev. Immunol. 2007, 7, 790–802. [Google Scholar] [CrossRef]
- Eusébio, D.; Neves, A.R.; Costa, D.; Biswas, S.; Alves, G.; Cui, Z.; Sousa, Â. Methods to Improve the Immunogenicity of Plasmid DNA Vaccines. Drug Discov. Today 2021, 26, 2575–2592. [Google Scholar] [CrossRef]
- Kafshdooz, T.; Kafshdooz, L.; Akbarzadeh, A.; Hanifehpour, Y.; Joo, S.W. Applications of Nanoparticle Systems in Gene Delivery and Gene Therapy. Artif. Cells Nanomed. Biotechnol. 2016, 44, 581–587. [Google Scholar] [CrossRef]
- Paston, S.J.; Brentville, V.A.; Symonds, P.; Durrant, L.G. Cancer Vaccines, Adjuvants, and Delivery Systems. Front. Immunol. 2021, 12, 627932. [Google Scholar] [CrossRef]
- Irache, J.M.; Salman, H.H.; Gamazo, C.; Espuelas, S. Mannose-Targeted Systems for the Delivery of Therapeutics. Expert Opin. Drug Deliv. 2008, 5, 703–724. [Google Scholar] [CrossRef]
- Akhatova, A.; Chan, C.K.; Azizan, A.; Aimagambetova, G. The Efficacy of Therapeutic DNA Vaccines Expressing the Human Papillomavirus E6 and E7 Oncoproteins for Treatment of Cervical Cancer: Systematic Review. Vaccines 2022, 10, 53. [Google Scholar] [CrossRef]
- Henere, C.; Torné, A.; Llupià, A.; Aldea, M.; Martí, C.; Glickman, A.; Saco, A.; Marimon, L.; Manzotti, C.; Rakislova, N.; et al. HPV Vaccination in Women with Cervical Intraepithelial Neoplasia Undergoing Excisional Treatment: Insights into Unsolved Questions. Vaccines 2022, 10, 887. [Google Scholar] [CrossRef] [PubMed]
- Kechagias, K.S.; Kalliala, I.; Bowden, S.J.; Athanasiou, A.; Paraskevaidi, M.; Paraskevaidis, E.; Dillner, J.; Nieminen, P.; Strander, B.; Sasieni, P.; et al. Role of Human Papillomavirus (HPV) Vaccination on HPV Infection and Recurrence of HPV Related Disease after Local Surgical Treatment: Systematic Review and Meta-Analysis. BMJ 2022, 378, e070135. [Google Scholar] [CrossRef] [PubMed]
- Tang, J.; Li, M.; Zhao, C.; Shen, D.; Liu, L.; Zhang, X.; Wei, L. Therapeutic DNA Vaccines against HPV-Related Malignancies: Promising Leads from Clinical Trials. Viruses 2022, 14, 239. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Vaccine | Number of Participants | CIN | Ref | |||
|---|---|---|---|---|---|---|---|---|
| Name | Type | Administration Method | Control | Experimental | ||||
| Cornelia L. Trimble et al. | 2016 | VGX-3100 | pDNA encoding optimized synthetic consensus E6 and E7 genes of HPV 16 and HPV 18 | Intramuscular injection followed by Electroporation | 40 | 114 | 2/3 | [35] |
| Mojgan Karimi-Zarchi et al. | 2020 | Gardasil | Quadrivalent vaccine based on L1 VLPs from HPV 6, 11, 16, and 18 | Intramuscular injection | 69 | 83 | 1+ | [36] |
| Diane M. Harper et al. | 2019 | Tipapkinogen Sovacivec vaccine | Viral vector expressing human cytokine IL-2 and modified HPV 16 E6 and E7 | Subcutaneous injection | 63 | 129 | 2/3 | [37] |
| Andreas M. Kaufmann et al. | 2007 | Chimeric virus-like particle (CVLP) vaccine | CVLP of carboxy-terminally truncated HPV16L1 protein fused to the amino-terminal part of the HPV16 E7 protein | Subcutaneous injection | 12 | 23 | 2/3 | [38] |
| Ikeda, Y. et al. | 2021 | GLBL101c | Heat-attenuated recombinant L. casei expressing mutated HPV16 E7 | Oral administration | 19 | 19 | 2/3 | [39] |
| Ian H. Frazer et al. | 2004 | - | HPV16 E6E7 fusion recombinant protein and ISCOMATRIX adjuvant | Intramuscular injection | 7 | 24 | 1+ | [40] |
| Francisco Garcia et al. | 2004 | ZYC101a | pDNA expressing antigenic regions of E6 and E7 of HPV 16 and 18 | Poly-lactide co-glycolide (PLG) microparticles with intramuscular injection | 50 | 111 | 2/3 | [41] |
| Mark Matijevic et al. | 2011 | ZYC101a | pDNA expressing antigenic regions of E6 and E7 of HPV 16 and 18 | Poly-lactide co-glycolide (PLG) microparticles with intramuscular injection | 5 | 21 | 2/3 | [42] |
| Outcomes | Number of Studies | Number of Patients | Pooled Effect Observed (95% CI) | p-Value | I2 (%) | Model Used | Studies Trimmed | Pooled Effect Adjusted (95% CI) |
|---|---|---|---|---|---|---|---|---|
| Histological improvement to normal or CIN 1 | 7 | 729 | RR: 0.779 (0.697 to 0.967) | 0.024 | 63.612 | Random | 3 | RR: 0.692 (0.553 to 0.866) |
| Vaccine Efficacy for complete resolution | 7 | 675 | VE: 23.6% (12.4% to 33.4%) | <0.001 | 56.516 | Random | 2 | VE: 18.7% (4.2% to 30.8%) |
| DNA clearance | 4 | 386 | RR: 0.768 (0.667 to 0.885) | <0.001 | 0 | Fixed | 2 | RR: 0.717 (0.637 to 0.801) |
| HPV-T cell response after vaccination | 4 | 357 | OR: 3.381 (1.245 to 9.182) | 0.017 | 0 | Fixed | 2 | OR: 2.371 (0.857 to 6.558) |
| Outcomes | Regression Intercept | 95% CI | t-Value | df | p-Value |
|---|---|---|---|---|---|
| Histological improvement to normal or CIN 1 | 0.53 | −3.38 to 4.45 | 0.35 | 5 | 0.74 |
| Vaccine Efficacy for complete resolution | −2.21 | −4.95 to 0.54 | 2.06 | 5 | 0.09 |
| DNA clearance | 0.15 | −3.61 to 3.90 | 0.17 | 2 | 0.88 |
| HPV-T cell response after vaccination | 2.07 | −0.23 to 4.37 | 3.88 | 2 | 0.06 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ventura, C.; Luís, Â.; Soares, C.P.; Venuti, A.; Paolini, F.; Pereira, L.; Sousa, Â. The Effectiveness of Therapeutic Vaccines for the Treatment of Cervical Intraepithelial Neoplasia 3: A Systematic Review and Meta-Analysis. Vaccines 2022, 10, 1560. https://doi.org/10.3390/vaccines10091560
Ventura C, Luís Â, Soares CP, Venuti A, Paolini F, Pereira L, Sousa Â. The Effectiveness of Therapeutic Vaccines for the Treatment of Cervical Intraepithelial Neoplasia 3: A Systematic Review and Meta-Analysis. Vaccines. 2022; 10(9):1560. https://doi.org/10.3390/vaccines10091560
Chicago/Turabian StyleVentura, Cathy, Ângelo Luís, Christiane P. Soares, Aldo Venuti, Francesca Paolini, Luísa Pereira, and Ângela Sousa. 2022. "The Effectiveness of Therapeutic Vaccines for the Treatment of Cervical Intraepithelial Neoplasia 3: A Systematic Review and Meta-Analysis" Vaccines 10, no. 9: 1560. https://doi.org/10.3390/vaccines10091560