
Vaccinating Front-Line Healthcare Workers: Results of a Pre-Pandemic Cross-Sectional Study from North-Eastern Italy on First Responders


Abstract
:1. Introduction
2. Materials and Methods
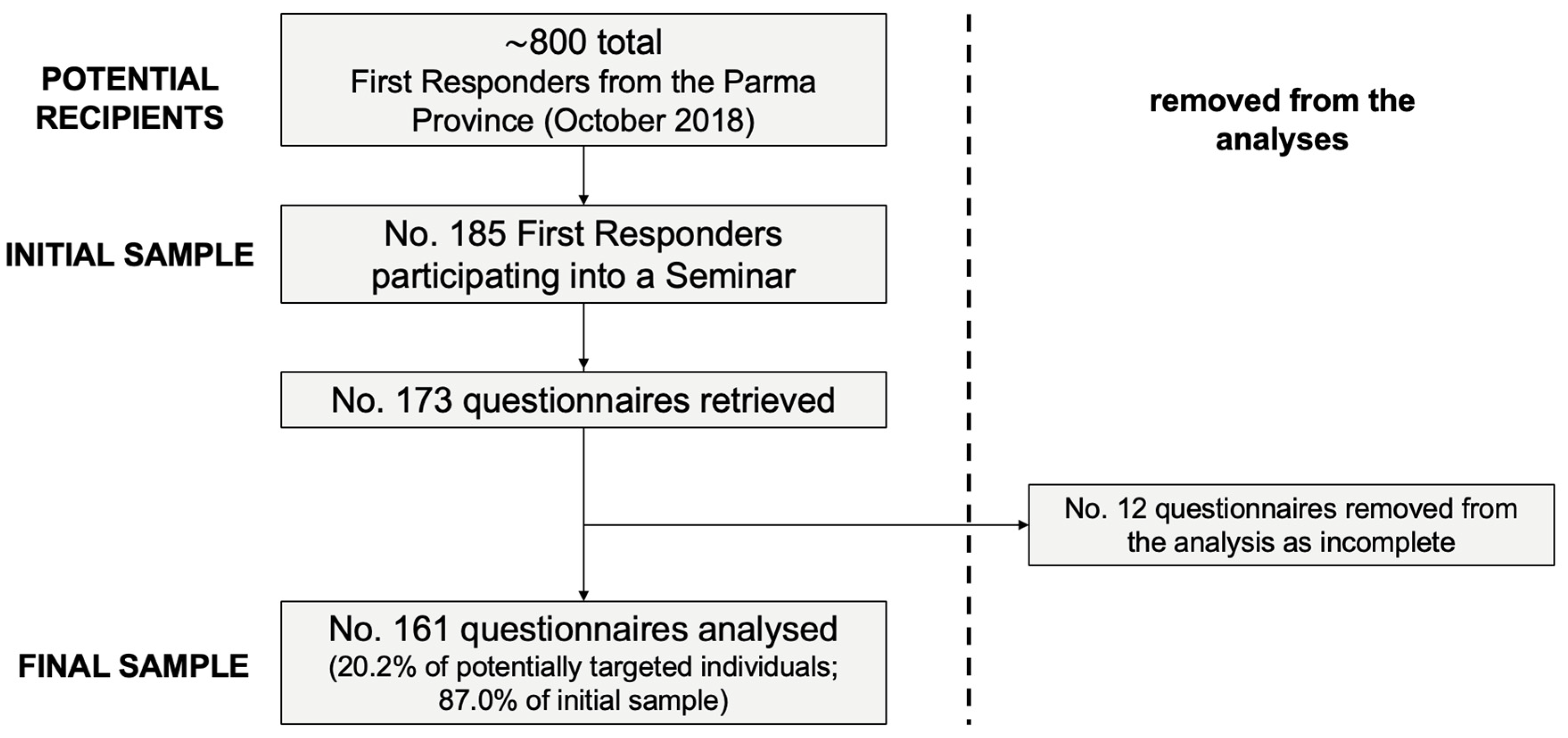
2.1. Study Design
2.2. Study Population
2.3. Ethical Considerations
2.4. Questionnaire
2.4.1. General Knowledge
2.4.2. Knowledge of Official Vaccination Recommendations
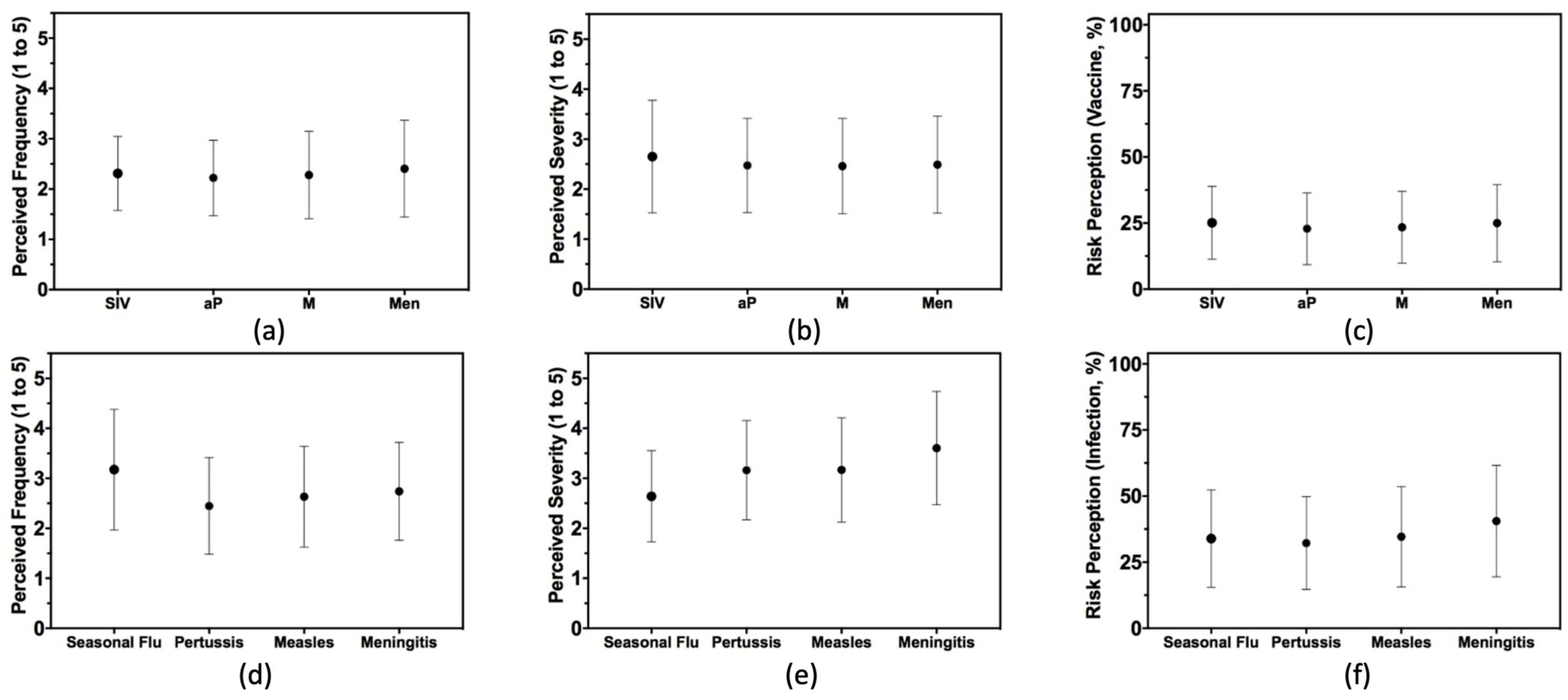
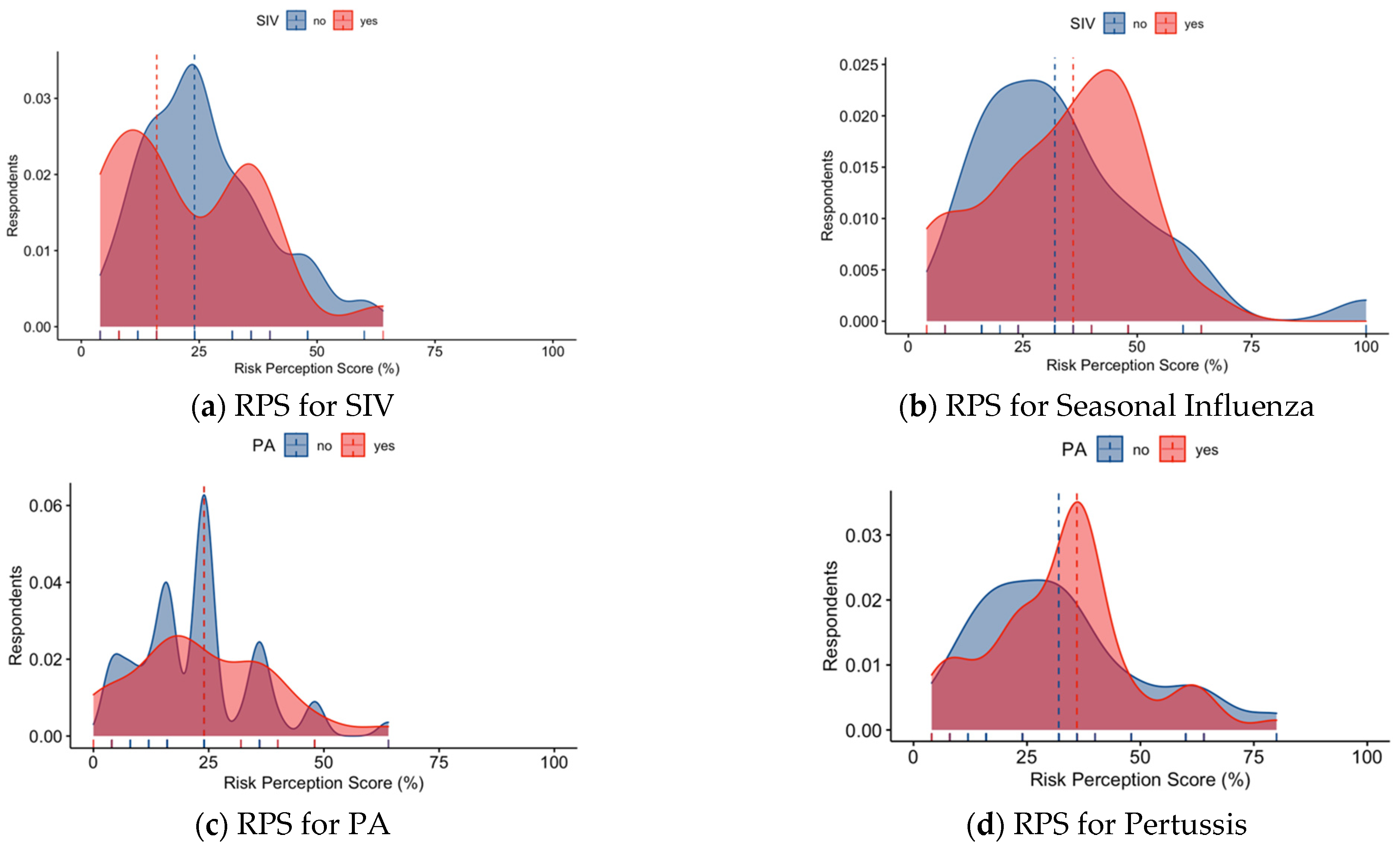
2.4.3. Risk Perception
2.4.4. Attitudes
2.4.5. Practices
2.5. Data Analysis
3. Results
3.1. Characteristics of the Sample
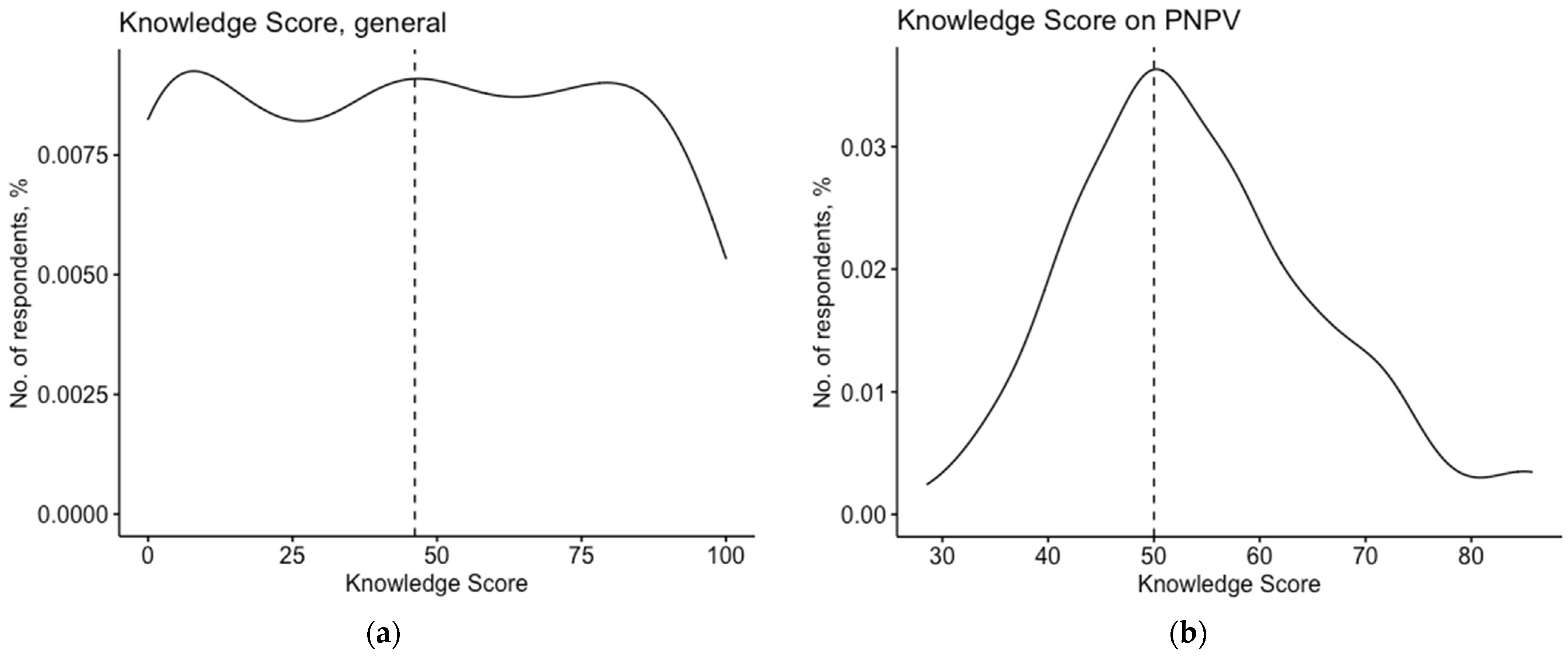
3.2. Knowledge Status
3.3. Attitudes
3.4. Practices
3.5. Univariate Analysis
3.6. Multivariable Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A


References
- Tuckerman, J.L.; Collins, J.E.; Marshall, H.S. Factors Affecting Uptake of Recommended Immunizations among Health Care Workers in South Australia. Hum. Vaccines Immunother. 2015, 11, 704–712. [Google Scholar] [CrossRef] [PubMed]
- Riccò, M.; Vezzosi, L.; Odone, A.; Signorelli, C. Invasive Meningococcal Disease on the Workplaces: A Systematic Review. Acta Biomed. 2017, 88, 337–351. [Google Scholar] [CrossRef] [PubMed]
- De Serres, G.; Skowronski, D.M.; Ward, B.J.; Gardam, M.; Lemieux, C.; Yassi, A.; Patrick, D.M.; Krajden, M.; Loeb, M.; Collignon, P.; et al. Influenza Vaccination of Healthcare Workers: Critical Analysis of the Evidence for Patient Benefit Underpinning Policies of Enforcement. PLoS ONE 2017, 12, e0163586. [Google Scholar] [CrossRef] [PubMed]
- Glaser, M.S.; Chui, S.; Webber, M.P.; Gustave, J.; Lee, R.; McLaughlin, M.T.; Ortiz, V.; Prezant, D.; Kelly, K. Predictors of Acceptance of H1N1 Influenza Vaccination by FDNY Firefighters and EMS Workers. Vaccine 2011, 29, 5675–5680. [Google Scholar] [CrossRef] [PubMed]
- Ganczak, M.; Topczewska, K.; Biesiada, D.; Korzeń, M. Frequency of Occupational Bloodborne Infections and Sharps Injuries among Polish Paramedics from Selected Ambulance Stations. Int. J. Environ. Res. Public Health 2021, 18, 60. [Google Scholar] [CrossRef]
- Porretta, A.; Pistello, M.; Vatteroni, M.L.; Lopalco, P.L.; Pieve, G.; Aquino, F.; Gemignani, G.; Bruni, B.; Quattrone, F.; Privitera, G.P. A Nosocomial Measles Outbreak in Italy, February–April 2017. Eurosurveillance 2017, 22, 30597. [Google Scholar] [CrossRef] [PubMed]
- Van den Hoogen, A.; Duijn, J.M.; Bode, L.G.M.; Vijlbrief, D.C.; de Hooge, L.; Ockhuijsen, H.D.L. Systematic Review Found That There Was Moderate Evidence That Vaccinating Healthcare Workers Prevented Pertussis in Infants. Int. J. Lab. Hematol. 2018, 107, 210–218. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Wicker, S.; Borg, M.; Heininger, U.; Puro, V.; Theodoridou, M.; Poland, G.A. Vaccination Policies for Health-Care Workers in Acute Health-Care Facilities in Europe. Vaccine 2011, 29, 9557–9562. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Wicker, S. Measles in Health-Care Settings. Am. J. Infect. Control 2013, 41, 661–663. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Poland, G.A. Vaccination Policies for Healthcare Workers in Europe. Vaccine 2014, 32, 4876–4880. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Theodoridou, K.; Ledda, C.; Rapisarda, V.; Theodoridou, M. Vaccination of Healthcare Workers: Is Mandatory Vaccination Needed? Expert Rev. Vaccines 2019, 18, 5–13. [Google Scholar] [CrossRef]
- Taddei, C.; Ceccherini, V.; Niccolai, G.; Porchia, B.R.; Boccalini, S.; Levi, M.; Tiscione, E.; Santini, M.G.; Baretti, S.; Bonanni, P.; et al. Attitude toward Immunization and Risk Perception of Measles, Rubella, Mumps, Varicella, and Pertussis in Health Care Workers Working in 6 Hospitals of Florence, Italy 2011. Hum. Vaccines Immunother. 2014, 10, 2612–2622. [Google Scholar] [CrossRef]
- Alicino, C.; Iudici, R.; Barberis, I.; Paganino, C.; Cacciani, R.; Zacconi, M.; Battistini, A.; Bellina, D.; di Bella, A.M.; Talamini, A.; et al. Influenza Vaccination among Healthcare Workers in Italy: The Experience of a Large Tertiary Acute-Care Teaching Hospital. Hum. Vaccines Immunother. 2015, 11, 95–100. [Google Scholar] [CrossRef]
- Bonaccorsi, G.; Santomauro, F.; Porchia, B.; Niccolai, G.; Pellegrino, E.; Bonanni, P.; Lorini, C. Beliefs and Opinions of Health Care Workers and Students Regarding Influenza and Influenza Vaccination in Tuscany, Central Italy. Vaccines 2015, 3, 137–147. [Google Scholar] [CrossRef]
- Bonanni, P.; Ferrero, A.; Guerra, R.; Iannazzo, S.; Odone, A.; Pompa, M.; Rizzuto, E.; Signorelli, C. Vaccine Coverage in Italy and Assessment of the 2012–2014 National Immunization Prevention Plan. Epidemiol. Prev. 2015, 39, 146–158. [Google Scholar] [CrossRef]
- Kim, D.K.; Riley, L.E.; Paul, H. Morbidity and Mortality Weekly Report Advisory Committee on Immunization Practices Recommended Immunization Schedule for Adults Aged 19 Years or Older—United States, 2018. MMWR Morb. Mortal. Wkly. Rep. 2018, 67, 158–160. [Google Scholar] [CrossRef]
- Childre, F.; Nord, D.D. Measles, Mumps, Rubella, and Varicella Immunization Status of First Responders—A Policy Proposal. AAOHN J. 2009, 57, 187–189. [Google Scholar] [CrossRef]
- Gargano, L.M.; Jessica, M.; Jones, L.M.; Murray, D.; Wingood, G.M.; Diclemente, R.J.; Hughes, J.M. Seasonal and 2009 H1N1 influenza vaccine uptake, predictors of vaccination, and self-reported barriers to vaccination among secondary school teachers and staff. Hum. Vaccines 2011, 7, 89–95. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Poland, G.A. Immunization of healthcare personnel in Europe: Time to move forward with a common program. Vaccine 2020, 38, 3187–3190. [Google Scholar] [CrossRef]
- Quach, S.; Pereira, J.A.; Kwong, J.C.; Quan, S.; Crowe, L.; Guay, M.; Bettinger, J.A. Immunizing Health Care Workers against Influenza: A Glimpse into the Challenges with Voluntary Programs and Considerations for Mandatory Policies. Am. J. Infect. Control 2013, 41, 1017–1023. [Google Scholar] [CrossRef]
- Quach, S.; Pereira, J.A.; Heidebrecht, C.L.; Kwong, J.C.; Guay, M.; Crowe, L.; Quan, S.; Bettinger, J.A. Health Care Worker Influenza Immunization Rates: The Missing Pieces of the Puzzle. Am. J. Infect. Control 2013, 41, 685–690. [Google Scholar] [CrossRef] [PubMed]
- Backhaus, I.; Hermsen, D.; Timm, J.; Boege, F.; Lübke, N.; Göbels, K.; von der Lieth, D.; Dragano, N. Underascertainment of COVID-19 Cases among First Responders: A Seroepidemiological Study. Occup. Med. 2022, 72, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Riccò, M.; Cattani, S.; Casagranda, F.; Gualerzi, G.; Signorelli, C. Knowledge, Attitudes, Beliefs and Practices of Occupational Physicians towards Vaccinations of Health Care Workers: A Cross Sectional Pilot Study in North-Eastern Italy. Int. J. Occup. Med. Environ. Health 2017, 30, 775–790. [Google Scholar] [CrossRef] [PubMed]
- La Torre, G.; Scalingi, S.; Garruto, V.; Siclari, M.; Chiarini, M.; Mannocci, A. Knowledge, Attitude and Behaviours towards Recommended Vaccinations among Healthcare Workers. Healthcare 2017, 5, 13. [Google Scholar] [CrossRef] [PubMed]
- Alfonsi, A.; Azzari, C.; Bonanni, P.; Chiamenti, G.; Conversano, M.; Cristaudo, A.; D’Ancona, P.; Durando, P.; Filia, A.; Foddis, R.; et al. Position Paper: La Carta Di Pisa Delle Vaccinazioni Negli Operatori Sanitari (The Pisas’ Paper of Vaccinations in Healthcare). GlmPIOS 2017, 7, 155–157. [Google Scholar]
- Boccia, S.; Colamesta, V.; Grossi, A.; Villari, P.; Ricciardi, W. Improving Vaccination Coverage among Healthcare Workers in Italy. Epidemiol. Biostat. Public Health 2018, 15, 2017–2019. [Google Scholar] [CrossRef]
- Dojmi Di Delupis, F.; Mancini, N.; Ruggeri, M.; Pisanelli, P. Perceptions of Emergency Department Triage Nurses About Prehospital Emergency Rescuers in Italy. J. Patient Saf. 2020, 16, e34–e38. [Google Scholar] [CrossRef]
- Toh, M.P.; Kannan, P.; Chen, Y.; Chng, F.L.; Tang, W.E. Healthcare workers and H1N1 vaccination: Does having a chronic disease make a difference? Vaccine 2012, 30, 1064–1070. [Google Scholar] [CrossRef]
- Piccirillo, B.; Gaeta, T. Survey on Use of and Attitudes Toward Influenza Vaccination Among Emergency Department Staff in a New York Metropolitan Hospital. Infect. Control Hosp. Epidemiol. 2006, 27, 618–622. [Google Scholar] [CrossRef]
- Hulo, S.; Nuvoli, A.; Sobaszek, A.; Salembier-trichard, A. Knowledge and Attitudes towards Influenza Vaccination of Health Care Workers in Emergency Services. Vaccine 2017, 35, 205–207. [Google Scholar] [CrossRef]
- Betsch, C.; Wicker, S. Personal Attitudes and Misconceptions, Not Official Recommendations Guide Occupational Physicians’ Vaccination Decisions. Vaccine 2014, 32, 4478–4484. [Google Scholar] [CrossRef]
- Zingg, A.; Siegrist, M. Measuring People’s Knowledge about Vaccination: Developing a One-Dimensional Scale. Vaccine 2012, 30, 3771–3777. [Google Scholar] [CrossRef]
- Riccò, M.; Cattani, S.; Casagranda, F.; Gualerzi, G.; Signorelli, C. Knowledge, Attitudes, Beliefs and Practices of Occupational Physicians towards Seasonal Influenza Vaccination: A Cross-Sectional Study from North-Eastern Italy. J. Prev. Med. Hyg. 2017, 58, E141–E154. [Google Scholar]
- Riccò, M.; Razio, B.; Panato, C.; Poletti, L.; Signorelli, C. Knowledge, Attitudes and Practices of Agricultural Workers towards Tetanus Vaccine: A Field Report. Ann. Ig 2017, 29, 239–255. [Google Scholar] [CrossRef]
- Riccò, M.; Vezzosi, L.; Gualerzi, G.; Signorelli, C. Knowledge, Attitudes and Practices (KAP) towards Vaccinations in the School Settings: An Explorative Survey. J. Prev. Med. Hyg. 2017, 58, 266–278. [Google Scholar]
- Betsch, C.; Korn, L.; Holtmann, C. Don’t Try to Convert the Antivaccinators, Instead Target the Fence-Sitters. Proc. Natl. Acad. Sci. USA 2015, 112, E6725–E6726. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Botelho-Nevers, E.; Brantsæter, A.B.; Carlsson, R.M.; Heininger, U.; Hübschen, J.M.; Josefsdottir, K.S.; Kassianos, G.; Kyncl, J.; Ledda, C.; et al. Vaccination of Healthcare Personnel in Europe: Update to Current Policies. Vaccine 2019, 37, 7576–7584. [Google Scholar] [CrossRef]
- Mani, N.S.; Budak, J.Z.; Lan, K.F.; Bryson-Cahn, C.; Zelikoff, A.; Barker, G.E.C.; Grant, C.W.; Hart, K.; Barbee, C.J.; Sandoval, M.D.; et al. Prevalence of COVID-19 Infection and Outcomes Among Symptomatic Healthcare Workers in Seattle, Washington. Clin. Infect. Dis. 2020, 71, 2702–2707. [Google Scholar] [CrossRef]
- Garzaro, G.; Clari, M.; Ciocan, C.; Grillo, E.; Mansour, I.; Godono, A.; Borgna, L.G.; Sciannameo, V.; Costa, G.; Raciti, I.M.; et al. COVID-19 Infection and Diffusion among the Healthcare Workforce in a Large University-Hospital in Northwest Italy. Med. Lav. 2020, 111, 13–15. [Google Scholar] [CrossRef]
- Riccò, M.; Vezzosi, L.; Balzarini, F.; Bragazzi, N.L. Inappropriate Risk Perception for SARS-CoV-2 Infection among Italian HCWs in the Eve of COVID-19 Pandemic. Acta Biomed. 2020, 91, e2020040. [Google Scholar] [CrossRef]
- Signorelli, C.; Guerra, R.; Siliquini, R.; Ricciardi, W. Italy’s Response to Vaccine Hesitancy: An Innovative and Cost Effective National Immunization Plan Based on Scientific Evidence. Vaccine 2017, 35, 4057–4059. [Google Scholar] [CrossRef] [PubMed]
- Cioffi, A.; Cecannecchia, C. Compulsory Vaccination against SARS-CoV-2 in Health Care Professionals in Italy: Bioethical-Legal Issues. Med. Sci. Law 2022, 002580242211145. [Google Scholar] [CrossRef] [PubMed]
- Riccò, M.; Ferraro, P.; Peruzzi, S.; Balzarini, F.; Ranzieri, S. Mandate or Not Mandate: Knowledge, Attitudes, and Practices of Italian Occupational Physicians towards SARS-CoV-2 Immunization at the Beginning of Vaccination Campaign. Vaccines 2021, 9, 889. [Google Scholar] [CrossRef] [PubMed]
- ANSA. COVID: Italy’s Vaccination Campaign Struggling to Take Off; ANSA: Rome, Italy, 2021. [Google Scholar]
- Di Giuseppe, G.; Pelullo, C.P.; della Polla, G.; Montemurro, M.V.; Napolitano, F.; Pavia, M.; Angelillo, I.F. Surveying Willingness towards SARS-CoV-2 Vaccination of Healthcare Workers in Italy. Expert Rev. Vaccines 2021, 20, 881–889. [Google Scholar] [CrossRef] [PubMed]
- Gianino, M.M.; Politano, G.; Scarmozzino, A.; Charrier, L.; Testa, M.; Giacomelli, S.; Benso, A.; Zotti, C.M. Estimation of Sickness Absenteeism among Italian Healthcare Workers during Seasonal Influenza Epidemics. PLoS ONE 2017, 12, e0182510. [Google Scholar] [CrossRef] [PubMed]
- Bonaccorsi, G.; Lorini, C.; Santomauro, F.; Guarducci, S.; Pellegrino, E.; Puggelli, F.; Balli, M.; Bonanni, P. Predictive Factors Associated with the Acceptance of Pandemic and Seasonal Influenza Vaccination in Health Care Workers and Students in Tuscany, Central Italy. Hum. Vaccines Immunother. 2013, 9, 2603–2612. [Google Scholar] [CrossRef] [PubMed]
- Calimeri, S.; la Fauci, V.; Squeri, R.; lo Giudice, D. Susceptibility to Measles among Health Workers in a University Hospital in Southern Italy. Clin. Ter. 2020, 171, E486–E489. [Google Scholar] [CrossRef]
- Guillari, A.; Polito, F.; Pucciarelli, G.; Serra, N.; Gargiulo, G.; Esposito, M.R.; Botti, S.; Rea, T.; Simeone, S. Influenza Vaccination and Healthcare Workers: Barriers and Predisposing Factors. A Literature Review. Acta Biomed. 2021, 92, e2021004. [Google Scholar] [CrossRef]
- Di Giuseppe, G.; Pelullo, C.P.; della Polla, G.; Pavia, M. Meningococcal Disease and Related Vaccinations: Knowledge, Attitudes, and Practices among Healthcare Workers Who Provide Care to Patients with Underlying High-Risk Medical Conditions. Vaccines 2020, 8, 543. [Google Scholar] [CrossRef]
- Schmid, P.; Rauber, D.; Betsch, C.; Lidolt, G.; Denker, M.L. Barriers of Influenza Vaccination Intention and Behavior—A Systematic Review of Influenza Vaccine Hesitancy, 2005–2016. PLoS ONE 2017, 12, e0170550. [Google Scholar] [CrossRef]
- Lorenc, T.; Marshall, D.; Wright, K.; Sutcliffe, K.; Sowden, A. Seasonal Influenza Vaccination of Healthcare Workers: Systematic Review of Qualitative Evidence. BMC Health Serv. Res. 2017, 17, 732. [Google Scholar] [CrossRef]
- Dini, G.; Toletone, A.; Sticchi, L.; Orsi, A.; Bragazzi, N.L.; Durando, P. Influenza Vaccination in Healthcare Workers: A Comprehensive Critical Appraisal of the Literature. Hum. Vaccines Immunother. 2018, 14, 772–789. [Google Scholar] [CrossRef]
- Hofmann, F.; Ferracin, C.; Marsh, G.; Dumas, R. Influenza Vaccination of Healthcare Workers: A Literature Review of Attitudes and Beliefs. Infection 2006, 34, 142–147. [Google Scholar] [CrossRef]
- Dzieciolowska, S.; Hamel, D.; Gadio, S.; Dionne, M.; Gagnon, D.; Robitaille, L.; Cook, E.; Caron, I.; Talib, A.; Parkes, L.; et al. Covid-19 Vaccine Acceptance, Hesitancy and Refusal among Canadian Healthcare Workers: A Multicenter Survey. Am. J. Infect. Control 2021, 49, 1152–1157. [Google Scholar] [CrossRef]
- Wicker, S.; Zielen, S.; Rose, M.A. Attitudes of Healthcare Workers toward Pertussis Vaccination. Expert Rev. Vaccines 2008, 7, 1325–1328. [Google Scholar] [CrossRef]
- Janssen, C.; Maillard, A.; Bodelet, C.; Claudel, A.-L.; Gaillat, J.; Delory, T. Hesitancy towards COVID-19 Vaccination among Healthcare Workers: A Multi-Centric Survey in France. Vaccines 2021, 9, 547. [Google Scholar] [CrossRef]
- Di Gennaro, F.; Murri, R.; Segala, F.V.; Cerruti, L.; Abdulle, A.; Saracino, A.; Bavaro, D.F.; Fantoni, M. Attitudes towards Anti-Sars-Cov2 Vaccination among Healthcare Workers: Results from a National Survey in Italy. Viruses 2021, 13, 371. [Google Scholar] [CrossRef]
- Fedeli, U.; Zanetti, C.; Saia, B. Susceptibility of Healthcare Workers to Measles, Mumps Rubella and Varicella. J. Hosp. Infect. 2002, 51, 133–135. [Google Scholar] [CrossRef]
- Loulergue, P.; Moulin, F.; Vidal-Trecan, G.; Absi, Z.; Demontpion, C.; Menager, C.; Gorodetsky, M.; Gendrel, D.; Guillevin, L.; Launay, O. Knowledge, Attitudes and Vaccination Coverage of Healthcare Workers Regarding Occupational Vaccinations. Vaccine 2009, 27, 4240–4243. [Google Scholar] [CrossRef]
- Carrillo-Santisteve, P.; Lopalco, P.L. Measles Still Spreads in Europe: Who Is Responsible for the Failure to Vaccinate? Clin. Microbiol. Infect. 2012, 18, 50–56. [Google Scholar] [CrossRef]
- Riccò, M.; Vezzosi, L.; Gualerzi, G.; Balzarini, F.; Mezzoiuso, G.; Odone, A.; Signorelli, C. Measles Vaccine in the School Settings: A Cross-Sectional Study about Knowledge, Personal Beliefs, Attitudes and Practices of Schoolteachers in Northern Italy. Minerva Pediatrics 2022. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Esposito, S.; Principi, N. Prevention of Pertussis: An Unresolved Problem. Hum. Vaccines Immunother. 2018, 14, 2452–2459. [Google Scholar] [CrossRef] [PubMed]
- Wicker, S.; Rose, M.A. Health Care Workers and Pertussis: An Underestimated Issue. Med. Klin. 2010, 105, 882–886. [Google Scholar] [CrossRef]
- Gabutti, G.; Rota, M.C. Pertussis: A Review of Disease Epidemiology Worldwide and in Italy. Int. J. Environ. Res. Public Health 2012, 9, 4626–4638. [Google Scholar] [CrossRef]
- Vittucci, A.C.; Spuri Vennarucci, V.; Grandin, A.; Russo, C.; Lancella, L.; Tozzi, A.E.; Bartuli, A.; Villani, A. Pertussis in Infants: An Underestimated Disease. BMC Infect Dis 2016, 16, 414. [Google Scholar] [CrossRef]
- Luthy, K.E.; Bainum, J.L.; Beckstrand, R.L.; MacIntosh, J.L.B.; Eden, L.M.; Saunders, B. Promoting Adult Pertussis Vaccination in the Workplace. Workplace Health Saf. 2016, 64, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Laenen, J.; Roelants, M.; Devlieger, R.; Vandermeulen, C. Influenza and Pertussis Vaccination Coverage in Pregnant Women. Vaccine 2015, 33, 2125–2131. [Google Scholar] [CrossRef] [PubMed]
- Wicker, S.; Zielen, S.; Rose, M.A. Obstacles in the Motivation of Health Care Workers for Pertussis Vaccination. Procedia Vaccinol. 2010, 2, 106–108. [Google Scholar] [CrossRef]
- De Waure, C.; Quaranta, G.; Ianuale, C.; Panatto, D.; Amicizia, D.; Apprato, L.; Campanella, P.; Colotto, M.; de Meo, C.; di Nardo, F.; et al. Knowledge, Attitudes and Behaviors of the Italian Population towards Neisseria Meningitidis, Streptococcus Pneumoniae and HPV Diseases and Vaccinations: A Cross-Sectional Multicentre Study. Public Health 2016, 141, 136–142. [Google Scholar] [CrossRef]
- Stephens, D.S.; Greenwood, B.; Brandtzaeg, P. Epidemic Meningitis, Meningococcemia, and Neisseria Meningitidis. Lancet 2007, 369, 2196–2210. [Google Scholar] [CrossRef]
- Caugant, D.A. Genetics and Evolution of Neisseria Meningitidis: Importance for the Epidemiology of Meningococcal Disease. Infect. Genet. Evol. 2008, 8, 558–565. [Google Scholar] [CrossRef]
- Eilers, R.; de Melker, H.E.; Veldwijk, J.; Krabbe, P.F.M. Vaccine Preferences and Acceptance of Older Adults. Vaccine 2017, 35, 2823–2830. [Google Scholar] [CrossRef]
- Eppes, C.; Wu, A.; Cameron, K.A.; Garcia, P.; Grobman, W. Does Obstetrician Knowledge Regarding Influenza Increase HINI Vaccine Acceptance among Their Pregnant Patients? Vaccine 2012, 30, 5782–5784. [Google Scholar] [CrossRef]
- Marshall, H.; Clarke, M.; Sullivan, T. Parental and Community Acceptance of the Benefits and Risks Associated with Meningococcal B Vaccines. Vaccine 2014, 32, 338–344. [Google Scholar] [CrossRef]
- Lefebvre, M.; Grossi, O.; Chalopin, M.; Ferré, C.; Prel, E.; Coutherut, J.; Briend-Godet, V.; Biron, C.; Raffi, F. Acceptance of Pregnant Women’s Vaccination against Pertussis among French Women and Health Professionals: PREVACOQ-1 and -2 Studies. Med. Mal. Infect. 2019, 49, 593–601. [Google Scholar] [CrossRef]
- Garcia, L.Y.; Cerda, A.A. Acceptance of a COVID-19 Vaccine: A Multifcatorial Consideration. Vaccine 2020, 38, 7587. [Google Scholar] [CrossRef]
- Machida, M.; Nakamura, I.; Kojima, T.; Saito, R.; Nakaya, T.; Hanibuchi, T. Acceptance of a COVID-19 Vaccine in Japan during the COVID-19 Pandemic. Vaccines 2021, 9, 210. [Google Scholar] [CrossRef]
- Shekhar, R.; Sheikh, A.B.; Upadhyay, S.; Singh, M.; Kottewar, S.; Mir, H.; Barrett, E.; Pal, S. COVID-19 Vaccine Acceptance among Health Care Workers in the United States. Vaccines 2021, 9, 119. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control (ECDC). Vaccine Hesitancy among Healthcare Workers and Their Patients in Europe; European Centre for Disease Prevention and Control: Stockholm, Sweden, 2015; ISBN 9789291937226. [Google Scholar]
- Brunelli, L.; Antinolfi, F.; Malacarne, F.; Cocconi, R.; Brusaferro, S. A Wide Range of Strategies to Cope with Healthcare Workers’ Vaccine Hesitancy in A North-Eastern Italian Region: Are They Enough? Healthcare 2020, 9, 4. [Google Scholar] [CrossRef]
- Prato, R.; Martinelli, D.; Marchetti, F.; Fortunato, F.; Tafuri, S.; Germinario, C.A. Feasibility of a Cocoon Strategy for the Prevention of Pertussis in Italy: A Survey of Prevention Department Healthcare Providers. Pediatric Infect. Dis. J. 2012, 31, 1304–1307. [Google Scholar] [CrossRef]
- Gabutti, G.; Cristina Rota, M.; Bonato, B.; Pirani, R.; Turlà, G.; Cucchi, A.; Cavallaro, A. Hospitalizations for Pertussis in Italy, 1999–2009: Analysis of the Hospital Discharge Database. Eur. J. Pediatrics 2012, 171, 1651–1655. [Google Scholar] [CrossRef] [PubMed]
- Gonfantini, M.V.; Carloni, E.; Gesualdo, F.; Pandolf, E.; Agricola, E.; Rizzuto, E.; Iannazzo, S.; Ciof Degli Atti, M.L.; Villani, A.; Tozzi, A.E. Epidemiology of Pertussis in Italy: Disease Trends over the Last Century. Eurosurveillance 2014, 19, 20921. [Google Scholar] [CrossRef]
- Palazzo, R.; Carollo, M.; Fedele, G.; Rizzo, C.; Rota, M.C.; Giammanco, A.; Iannazzo, S.; Ausiello, C.M. Evidence of Increased Circulation of Bordetella Pertussis in the Italian Adult Population from Seroprevalence Data (2012–2013). J. Med. Microbiol. 2016, 65, 649–657. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonfiantini, M.V.; Villani, A.; Gesualdo, F.; Pandolfi, E.; Agricola, E.; Bozzola, E.; Arigliani, R.; Tozzi, A.E. Attitude of Italian Physicians toward Pertussis Diagnosis. Hum. Vaccines Immunother. 2013, 9, 1485–1488. [Google Scholar] [CrossRef] [PubMed]
- Ives, J.; Greenfield, S.; Parry, J.M.; Draper, H.; Gratus, C.; Petts, J.I.; Sorell, T.; Wilson, S. Healthcare Workers’ Attitudes to Working during Pandemic Influenza: A Qualitative Study. BMC Public Health 2009, 9, 56. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, F.; Lindley, M.C.; Allred, N.; Weinbaum, C.M.; Grohskopf, L. Effect of Influenza Vaccination of Healthcare Personnel on Morbidity and Mortality among Patients: Systematic Review and Grading of Evidence. Clin. Infect. Dis. 2014, 58, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Riphagen-Dalhuisen, J.; Gefenaite, G.; Hak, E. Predictors of Seasonal Influenza Vaccination among Healthcare Workers in Hospitals: A Descriptive Meta-Analysis. Occup. Environ. Med. 2012, 69, 230–235. [Google Scholar] [CrossRef]
- Aoyagi, Y.; Beck, C.R.; Dingwall, R.; Nguyen-Van-Tam, J.S. Healthcare Workers’ Willingness to Work during an Influenza Pandemic: A Systematic Review and Meta-Analysis. Influenza Other Respir. Viruses 2015, 9, 120–130. [Google Scholar] [CrossRef]
- Thomas, R.E.; Jefferson, T.; Lasserson, T.J. Influenza Vaccination for Healthcare Workers Who Work with the Elderly: Systematic Review. Vaccine 2010, 29, 344–356. [Google Scholar] [CrossRef]
- Mo, P.K.H.; Lau, J.T.F. Influenza Vaccination Uptake and Associated Factors among Elderly Population in Hong Kong: The Application of the Health Belief Model. Health Educ. Res. 2015, 30, 706–718. [Google Scholar] [CrossRef]
- Fall, E.; Izaute, M.; Baggioni, N.C. How Can the Health Belief Model and Self-Determination Theory Predict Both Influenza Vaccination and Vaccination Intention? A Longitudinal Study among University Students. Psychol. Health 2017, 33, 746–764. [Google Scholar] [CrossRef]
- Yates, F.J.; Stone, E.R. The Risk Construct. In Risk-Taking Behaviour; Yates, F.J., Ed.; John Wiley & Sons: Chichester, UK, 1992; pp. 1–25. ISBN 0471922501. [Google Scholar]
- Gaube, S.; Lermer, E.; Fischer, P. The Concept of Risk Perception in Health-Related Behavior Theory and Behavior Change. In Perceived Safety: Risk Engineering; Raue, M., Streicher, B., Lermer, E., Eds.; Springer: Cham, Switzerland, 2019; pp. 101–118. ISBN 9783030114565. [Google Scholar]
- Bonanni, P.; Boccalini, S.; Zanobini, P.; Dakka, N.; Lorini, C.; Santomauro, F.; Bechini, A. The Appropriateness of the Use of Influenza Vaccines: Recommendations from the Latest Seasons in Italy. Hum. Vaccines Immunother. 2018, 14, 699–705. [Google Scholar] [CrossRef]
- Nicholson, K.G.; McNally, T.; Silverman, M.; Simons, P.; Stockton, J.D.; Zambon, M.C. Rates of Hospitalisation for Influenza, Respiratory Syncytial Virus and Human Metapneumovirus among Infants and Young Children. Vaccine 2006, 24, 102–108. [Google Scholar] [CrossRef]
- Levi, M.; Bonanni, P.; Biffino, M.; Conversano, M.; Corongiu, M.; Morato, P.; Maio, T. Influenza Vaccination 2014–2015: Results of a Survey Conducted among General Practitioners in Italy. Hum. Vaccines Immunother. 2018, 14, 1342–1350. [Google Scholar] [CrossRef]
- Mahroum, N.; Watad, A.; Rosselli, R.; Brigo, F.; Chiesa, V.; Siri, A.; Ben-Ami Shor, D.; Martini, M.; Bragazzi, N.L.; Adawi, M. An Infodemiological Investigation of the So-Called “Fluad Effect” during the 2014/2015 Influenza Vaccination Campaign in Italy: Ethical and Historical Implications. Hum. Vaccines Immunother. 2018, 14, 712–718. [Google Scholar] [CrossRef]
- Giannattasio, A.; Mariano, M.; Romano, R.; Chiatto, F.; Liguoro, I.; Borgia, G.; Guarino, A.; lo Vecchio, A. Sustained Low Influenza Vaccination in Health Care Workers after H1N1 Pandemic: A Cross Sectional Study in an Italian Health Care Setting for at-Risk Patients. BMC Infect. Dis. 2015, 15, 329. [Google Scholar] [CrossRef]
- MacDougall, D.M.; Halperin, B.A.; MacKinnon-Cameron, D.; Li, L.; McNeil, S.A.; Langley, J.M.; Halperin, S.A. The Challenge of Vaccinating Adults: Attitudes and Beliefs of the Canadian Public and Healthcare Providers. BMJ Open 2015, 5, e009062. [Google Scholar] [CrossRef]
- Prati, G.; Pietrantoni, L.; Zani, B. Compliance with Recommendations for Pandemic Influenza H1N1 2009: The Role of Trust and Personal Beliefs. Health Educ. Res. 2011, 26, 761–769. [Google Scholar] [CrossRef]
- Bert, F.; Olivero, E.; Rossello, P.; Gualano, M.R.; Castaldi, S.; Damiani, G.; D’Errico, M.M.; di Giovanni, P.; Fantini, M.P.; Fabiani, L.; et al. Knowledge and Beliefs on Vaccines among a Sample of Italian Pregnant Women: Results from the NAVIDAD Study. Eur. J. Public Health 2019, 30, 286–292. [Google Scholar] [CrossRef]
- Riccò, M.; Gualerzi, G.; Ranzieri, S.; Ferraro, P.; Bragazzi, N.L. Knowledge, Attitudes, Practices (KAP) of Italian Occupational Physicians towards Tick Borne Encephalitis. Trop. Med. Infect. Dis. 2020, 5, 117. [Google Scholar] [CrossRef]
- Vezzosi, L.; Riccò, M.; Agozzino, E.; Odone, A.; Signorelli, C. Knowledge, Attitudes, and Practices of General Practitioners from the Province of Parma (Northern Italy) towards Vaccinations in Adults ≥ 65 Year-Old. Acta Biomed. 2019, 90, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Riccò, M.; Vezzosi, L.; Gualerzi, G.; Balzarini, F.; Capozzi, V.A.; Volpi, L. Knowledge, Attitudes, Beliefs and Practices of Obstetrics-Gynecologists on Seasonal Influenza and Pertussis Immunizations in Pregnant Women: Preliminary Results from North-Western Italy. Minerva Ginecol. 2019, 71, 288–297. [Google Scholar] [CrossRef] [PubMed]
- Riccò, M.; Vezzosi, L.; Gualerzi, G.; Bragazzi, N.L.; Balzarini, F. Pertussis Immunization in Healthcare Workers Working in Pediatric Settings: Knowledge, Attitudes and Practices (KAP) of Occupational Physicians. Preliminary Results from a Web-Based Survey (2017). J. Prev. Med. Hyg. 2020, 61, E66–E75. [Google Scholar] [PubMed]
- Flahault, A.; Cadilhac, M.; Thomas, G. Sample Size Calculation Should Be Performed for Design Accuracy in Diagnostic Test Studies. J. Clin. Epidemiol. 2005, 58, 859–862. [Google Scholar] [CrossRef]
- Caranci, N.; di Girolamo, C.; Bartolini, L.; Fortuna, D.; Berti, E.; Sforza, S.; Rossi, P.G.; Moro, M.L. General and COVID-19-Related Mortality by Pre-Existing Chronic Conditions and Care Setting during 2020 in Emilia-Romagna Region, Italy. Int. J. Environ. Res. Public Health 2021, 18, 13224. [Google Scholar] [CrossRef] [PubMed]
- Alicandro, G.; Remuzzi, G.; Centanni, S.; Gerli, A.; La Vecchia, C. Excess Total Mortality during the Covid-19 Pandemic in Italy: Updated Estimates Indicate Persistent Excess in Recent Months. Med. Lav. 2022, 113, e2022021. [Google Scholar] [CrossRef]
- Scortichini, M.; Schneider Dos Santos, R.; De’ Donato, F.; de Sario, M.; Michelozzi, P.; Davoli, M.; Masselot, P.; Sera, F.; Gasparrini, A. Excess Mortality during the COVID-19 Outbreak in Italy: A Two-Stage Interrupted Time-Series Analysis. Int. J. Epidemiol. 2020, 49, 1909–1917. [Google Scholar] [CrossRef]
- Trumello, C.; Bramanti, S.M.; Ballarotto, G.; Candelori, C.; Cerniglia, L.; Cimino, S.; Crudele, M.; Lombardi, L.; Pignataro, S.; Viceconti, M.L.; et al. Psychological Adjustment of Healthcare Workers in Italy during the COVID-19 Pandemic: Differences in Stress, Anxiety, Depression, Burnout, Secondary Trauma, and Compassion Satisfaction between Frontline and Non-Frontline Professionals. Int. J. Environ. Res. Public Health 2020, 17, 8358. [Google Scholar] [CrossRef]
- Marinaccio, A.; Boccuni, F.; Rondinone, B.M.; Brusco, A.; D’Amario, S.; Iavicoli, S. Occupational Factors in the COVID-19 Pandemic in Italy: Compensation Claims Applications Support Establishing an Occupational Surveillance System. Occup. Environ. Med. 2020, 77, 818–821. [Google Scholar] [CrossRef]
- National Institute for Insurance against Accidents at Work (INAIL). National Institute for Insurance against Accidents at Work (INAIL)—Regional Data about COVID-19 Related Injuries (January—30 June 2020); National Institute for Insurance against Accidents at Work: Rome, Italy, 2020. [Google Scholar]
- WHO Regional Office for Europe. An Unprecedented Challenge: Italy’s First Response to COVID-19; WHO Regional Office for Europe: Copenhagen, Denmark, 2020. [Google Scholar]
- Heiervang, E.; Goodman, R. Advantages and Limitations of Web-Based Surveys: Evidence from a Child Mental Health Survey. Soc. Psychiatry Psychiatr. Epidemiol. 2011, 46, 69–76. [Google Scholar] [CrossRef]
- Prochaska, J.O.; Velicer, W.F. The Transtheoretical Model of Health Behavior Change. Am. J. Health Promot. 1997, 12, 38–48. [Google Scholar] [CrossRef]
- MacDonald, N.E.; Eskola, J.; Liang, X.; Chaudhuri, M.; Dube, E.; Gellin, B.; Goldstein, S.; Larson, H.; Manzo, M.L.; Reingold, A.; et al. Vaccine Hesitancy: Definition, Scope and Determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Bloom, B.R.; Marcuse, E.; Mnookin, S. Addressing Vaccine Hesitancy. Science 2014, 344, 339. [Google Scholar] [CrossRef] [Green Version]
- Aldossri, M.; Okoronkwo, C.; Dodd, V.; Manson, H.; Singhal, S. Determinants of Dentists’ Readiness to Assess HPV Risk and Recommend Immunization: A Transtheoretical Model of Change-Based Cross-Sectional Study of Ontario Dentists. PLoS ONE 2021, 16, e0247043. [Google Scholar] [CrossRef]
- Riccò, M.; Peruzzi, S. Tetanus Vaccination Status and Vaccine Hesitancy in Amateur Basketball Players (Italy, 2020). Vaccines 2022, 10, 131. [Google Scholar] [CrossRef]
- Riccò, M.; Ferraro, P.; Camisa, V.; di Palma, P.; Minutolo, G.; Ranzieri, S.; Zaffina, S.; Baldassarre, A.; Restivo, V. Managing of Migraine in the Workplaces: Knowledge, Attitudes and Practices of Italian Occupational Physicians. Medicina 2022, 58, 686. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No./161, % | Average ± S.D. | |
|---|---|---|
| Sex | ||
| Male | 103, 64.0% | |
| Female | 58, 36.0% | |
| Age (years) | 45.1 ± 14.1 | |
| ≥50 y.o. | 69, 42.9% | |
| Seniority (years) | 10.8 ± 8.6 | |
| ≥10 years | 77, 47.8% | |
| Migration background | 8, 5.0% | |
| Educational achievements | ||
| 0–8 years (primary school) | 13, 8.1% | |
| 9–13 years (secondary school/high school) | 105, 65.2% | |
| 14 or more (university or higher) | 43, 26.7% | |
| Occupational background from healthcare settings | 19, 11.8% | |
| Knowledge Status | ||
| General Knowledge Score (%) | 46.5% ± 32.4 | |
| Knowledge of the official recommendation from the National Immunization Prevention Plan 2017–2019 (%) | 54.1% ± 11.8 | |
| Somehow favorable towards ... | ||
| Seasonal Influenza Vaccine | 89, 55.3% | |
| Pertussis Vaccine | 132, 82.0% | |
| Measles Vaccine | 141, 87.5% | |
| Meningococcal Vaccines | 144, 89.4% | |
| SIV, perceived facilitators in subjects somehow favorable | No./89, % | |
| Protecting subjects who cannot be vaccinated | 66, 74.2% | |
| Avoid spreading of seasonal influenza | 67, 75.3% | |
| Avoid complications (respondent) | 60, 67.4% | |
| Avoid natural infection (respondent) | 41, 46.1% | |
| It was recommended by GP | 5, 5.6% | |
| It was recommended by an OPh | 5, 5.6% | |
| I bear some specific recommendations | 13, 14.6% | |
| SIV, perceived barriers in subjects somehow not favorable | No./72, % | |
| Reputed as unnecessary (I’m otherwise immunized) | 11, 15.3% | |
| Fear of injections | 1, 1.4% | |
| Preference to other preventive measures | 27, 37.5% | |
| Not enough trust in SIV | 32, 44.4% | |
| SIV is useless | 2, 2.8% | |
| Lifestyles are more efficient | 2, 2.8% | |
| Fear of side effects | 10, 13.9% | |
| Previously Vaccinated against ... (self-reported) | ||
| Influenza, 2018 | 45, 28.0% | |
| Influenza, 2017 | 42, 26.1% | |
| Pertussis | 56, 34.8% | |
| Measles | 68, 42.2% | |
| Meningococcus | 42, 26.1% |
| Statement | Correct Answer | No./161, % |
|---|---|---|
| The additives used in the vaccines are not dangerous to humans | TRUE | 61, 37.9% |
| Multiple Sclerosis may be induced by the HBV vaccine | FALSE | 69, 42.9% |
| Subacute sclerosing panencephalitis may be induced by the measles vaccine | FALSE | 67, 41.6% |
| Autism is more frequent in subjects who have received the measles vaccine | FALSE | 77, 47.8% |
| Diabetes mellitus may be triggered by vaccination shoots | FALSE | 75, 46.6% |
| Vaccinations increase the occurrence of autoimmune diseases | FALSE | 52, 32.3% |
| Vaccinations increase the risk of allergic disorders | FALSE | 58, 36.0% |
| Vaccines are superfluous, as infectious diseases can always be treated with antibiotics | FALSE | 96, 59.6% |
| Without massive vaccination programs, smallpox would still exist | TRUE | 109, 67.7% |
| The efficacy of vaccines has been extensively proven | TRUE | 103, 64.0% |
| Children would be more resistant to infections if they were not always treated against all diseases | FALSE | 80, 49.7% |
| Many vaccinations are administered too early. As a result, the immune system has no possibility to fully develop by itself | FALSE | 66, 41.0% |
| The immune system of children may be overwhelmed by a high number of vaccines | FALSE | 61, 37.9% |
| Recommendations of Italian PNPV 2017–2019 | ||
| Diphtheria | NO | 96, 59.6% |
| Tetanus | NO | 25, 15.5% |
| Pertussis | YES | 64, 39.8% |
| Poliomyelitis | NO | 109, 67.7% |
| HAV | NO | 56, 34.8% |
| HBV | YES | 148, 91.9% |
| Influenza | YES | 142, 88.2% |
| Pneumococcus | NO | 76, 47.2% |
| H influenzae | NO | 116, 72.0% |
| Measles | YES | 98, 60.9% |
| Rubella | YES | 83, 51.6% |
| Parotitis | YES | 69, 42.9% |
| Varicella | YES | 83, 51.6% |
| Meningitis | NO | 55, 34.2% |
| HPV | NO | 111, 68.9% |
| Tuberculosis (BCG) | NO | 77, 47.8% |
| Risk Perception on… | ||
|---|---|---|
| Natural Infection | Vaccine | |
| Seasonal Influenza | −0.081 (p = 0.310) | −0.239 (p = 0.002) |
| Pertussis | 0.035 (p = 0.656) | −0.294 (p < 0.001) |
| Measles | 0.151 (p = 0.057) | −0.278 (p < 0.001) |
| N meningitidis infections | 0.161 (p = 0.042) | −0.260 (p = 0.001) |
| Variables | SIV 2018 | Pa | MeV | MEN | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SIV pos. (No./45, %) | SIV neg. (No./116, %) | p Value | Pa pos. (No./56, %) | Pa neg. (No./105, %) | p Value | MeV pos. (No./68, %) | MeV neg. (No./92, %) | p Value | MEN pos. (No./45) | Men neg. (No./116) | p Value | |
| Age ≥ 50 years | 20, 44.4% | 49, 42.2% | 0.939 | 12, 21.4% | 57, 54.3% | <0.001 | 13, 19.1% | 56, 60.9% | <0.001 | 11, 26.2% | 58, 48.7% | 0.018 |
| Male Sex | 35, 77.8% | 68, 58.6% | 0.037 | 36, 64.3% | 67, 63.8% | 1.000 | 45, 66.2% | 57, 62.0% | 0.702 | 30, 71.4% | 73, 61.3% | 0.325 |
| Migration background | 1, 2.2% | 7, 6.0% | 0.552 | 7, 12.5% | 1, 1.0% | 0.005 | 7, 10.3% | 1, 1.1% | 0.023 | 2, 4.8% | 6, 5.0% | 1.000 |
| Education ≥ University | 10, 22.2% | 33, 28.4% | 0.547 | 21, 37.5% | 22, 21.0% | 0.038 | 25, 36.8% | 18, 19.6% | 0.025 | 7, 16.7% | 36, 30.3% | 0.132 |
| Seniority ≥ 10 years | 31, 68.9% | 46, 39.7% | 0.002 | 16, 28.6% | 61, 58.1% | 0.001 | 21, 30.9% | 56, 60.9% | <0.001 | 20, 47.6% | 57, 47.9% | 1.000 |
| Healthcare background | 10, 22.2% | 9, 7.8% | 0.023 | 12, 21.4% | 7, 6.7% | 0.012 | 7, 10.3% | 12, 13.0% | 0.090 | 5, 11.9% | 14, 11.8% | 1.000 |
| Knowledge of Official recommendations for HCW | 25, 55.6% | 49, 42.2% | 0.179 | 29, 51.8% | 45, 42.9% | 0.359 | 33, 48.5% | 40, 43.5% | 0.636 | 21, 46.7% | 53, 44.5% | 0.667 |
| General Knowledge Score > median | 20, 44.4% | 56, 48.3% | 0.794 | 27, 48.2% | 49, 46.7% | 0.983 | 35, 51.5% | 41, 44.6% | 0.481 | 23, 54.8% | 53, 44.5% | 0.336 |
| Risk Perception Score for Vaccine > median | 18, 40.0% | 41, 35.3% | 0.713 | 20, 35.7% | 24, 22.9% | 0.119 | 21, 30.9% | 27, 29.3% | 0.972 | 14, 33.3% | 43, 36.1% | 0.890 |
| Risk Perception Score for Natural infection > median | 27, 60.0% | 42, 36.2% | 0.010 | 31, 55.4% | 38, 36.2% | 0.030 | 37, 54.4% | 35, 38.0% | 0.038 | 15, 35.7% | 58, 48.7% | 0.201 |
| Somehow Favorable attitude | 36, 80.0% | 53, 45.7% | <0.001 | 48, 85.7% | 84, 80.0% | 0.494 | 60, 88.2% | 80, 87.0% | 1.000 | 39, 92.9% | 105, 88.2% | 0.585 |
| Variable | SIV 2018 | Pa | MeV | MEN | ||||
|---|---|---|---|---|---|---|---|---|
| aOR | 95%CI | aOR | 95%CI | aOR | 95%CI | aOR | 95%CI | |
| Age ≥ 50 years | 1.116 | (0.471; 2.645) | 0.169 | (0.068; 0.420) | 0.114 | (0.047; 0.278) | 0.316 | (0.142; 0.704) |
| Male Sex | 1.753 | (0.689; 4.459) | 0.968 | (0.427; 2.261) | 1.316 | (0.579; 2.993) | 1.482 | (0.663; 3.312) |
| Migration background | 0.820 | (0.085; 7.881) | 15.330 | (1.418; 165.737) | 6.958 | (0.638; 75.839) | 0.903 | (0.163; 5.003) |
| Education ≥ University | 0.537 | (0.198; 1.454) | 3.274 | (1.291; 8.304) | 2.693 | (1.090; 6.651) | 0.376 | (0.147; 0.964) |
| Seniority ≥ 10 years | 3.262 | (1.346; 7.905) | 0.198 | (0.080; 0.489) | 0.197 | (0.085; 0.445) | - | - |
| Healthcare background | 3.184 | (0.908; 11.167) | 10.898 | (2.638; 45.017) | - | - | - | - |
| Risk Perception Score for Natural infection > median | 3.374 | (1.367; 8.332) | 1.266 | (0.547; 2.932) | 1.285 | (0.502; 3.285) | - | - |
| Somehow Favorable attitude | 8.404 | (3.070; 23.009) | - | - | - | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Riccò, M.; Vezzosi, L.; Marchesi, F. Vaccinating Front-Line Healthcare Workers: Results of a Pre-Pandemic Cross-Sectional Study from North-Eastern Italy on First Responders. Vaccines 2022, 10, 1492. https://doi.org/10.3390/vaccines10091492
Riccò M, Vezzosi L, Marchesi F. Vaccinating Front-Line Healthcare Workers: Results of a Pre-Pandemic Cross-Sectional Study from North-Eastern Italy on First Responders. Vaccines. 2022; 10(9):1492. https://doi.org/10.3390/vaccines10091492
Chicago/Turabian StyleRiccò, Matteo, Luigi Vezzosi, and Federico Marchesi. 2022. "Vaccinating Front-Line Healthcare Workers: Results of a Pre-Pandemic Cross-Sectional Study from North-Eastern Italy on First Responders" Vaccines 10, no. 9: 1492. https://doi.org/10.3390/vaccines10091492