
Graves’ Disease Following SARS-CoV-2 Vaccination: A Systematic Review

 , and
, and
Abstract
:1. Introduction
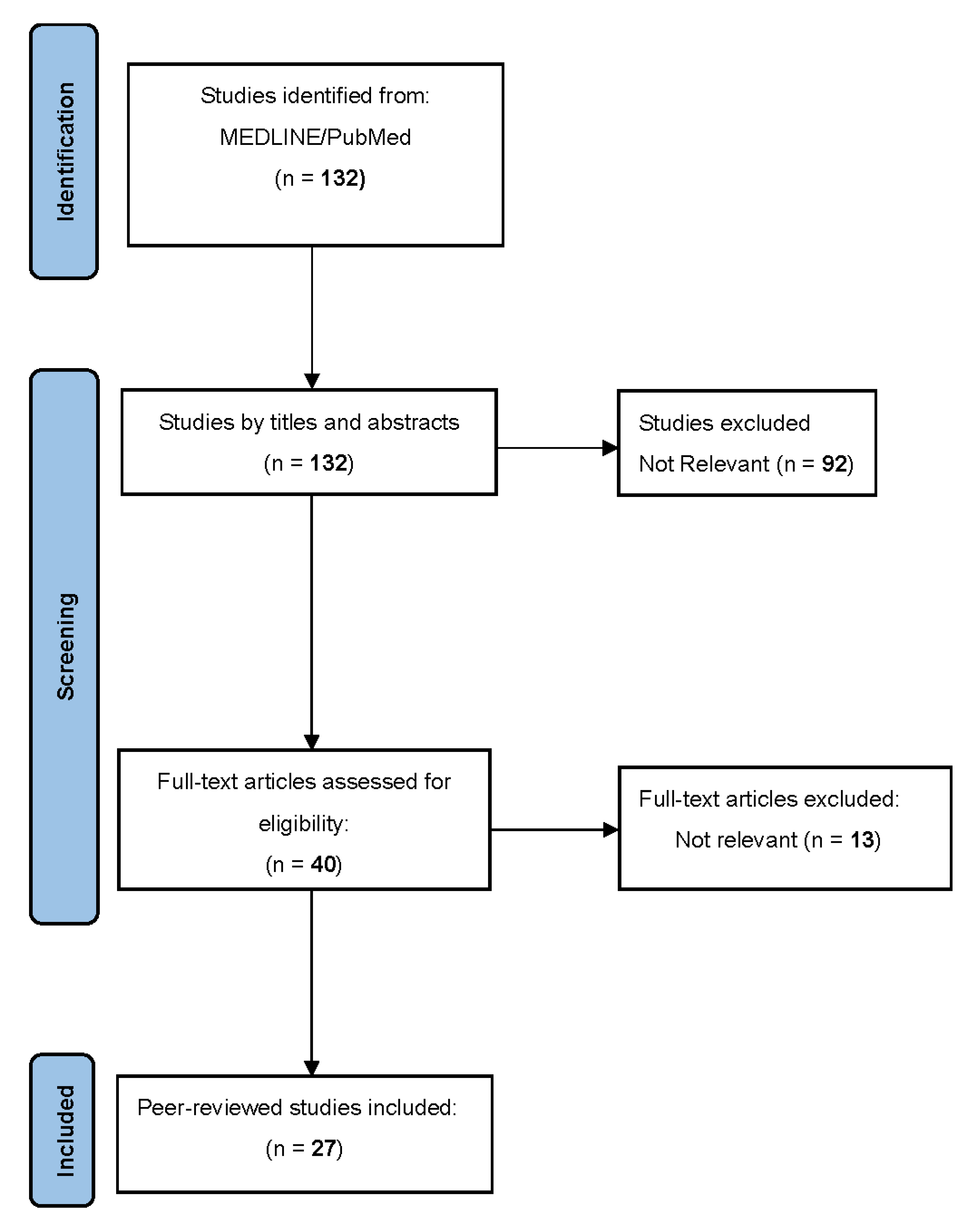
2. Materials and Methods
3. Results
3.1. General Characteristics
3.2. Clinical Features
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 31 July 2022).
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.; He, J.; Liu, L.; Shan, H.; Lei, C.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Mathieu, E.; Ritchie, H.; Ortiz-Ospina, E.; Rosr, M.; Hasell, J.; Appel, C.; Giattin, C.; Rodes-Guirao, L. A global database of COVID-19 vaccinations. Nat. Hum. Behav. 2021, 5, 947–953. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Ciembert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Perez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Castells, M.C.; Phillips, E.J. Maintaining Safety with SARS-CoV-2. N. Engl. J. Med. 2021, 384, 643–649. [Google Scholar] [CrossRef]
- Mevorach, D.; Anis, E.; Cedar, N.; Bromber, M.; Haas, E.J.; Nadir, E.; Olsha-Castell, S.; Arad, D.; Hasin, T.; Levi, N.; et al. Myocarditis after BNT162b2 mRNA Vaccine against COVID-19 in Israel. N. Engl. J. Med. 2021, 385, 2140–2149. [Google Scholar] [CrossRef]
- Arepally, G.M.; Ortel, T.L. Vaccine-induced immune thrombotic thrombocytopenia: What we know and do not know. Blood 2021, 138, 293–298. [Google Scholar] [CrossRef]
- Chen, Y.; Xu, Z.; Wang, P.; Li, X.; Shuai, Z.; Ye, D.; Pan, H. New-onset autoimmune phenomena post-COVID-19 vaccination. Immunology 2022, 165, 386–401. [Google Scholar] [CrossRef]
- Iremli, B.G.; Sendur, S.N.; Unluturk, U. Three Cases of Subacute Thyroiditis Following SARS-CoV-2 Vaccine: Postvaccination ASIA Syndrome. J. Clin. Endocrinol. Metab. 2021, 106, 2600–2605. [Google Scholar] [CrossRef]
- Vera-Lastra, O.; Ordinola Navarro, A.; Pilar Cruz Domigiez, M.; Medina, G.; Sanchez Valadez, T.I.; Jara, L.J. Two cases of Graves’ disease following SARS-CoV-2 vaccination: An aoutoimmune/inflammatory syndrome induced by adjuvants. Thyroid 2021, 136, 168–186. [Google Scholar] [CrossRef]
- Zettining, G.; Krebs, M. Two further cases of Graves’ disease following SARS-CoV-2 vaccination. J. Endocrinol. Investig. 2022, 45, 227–228. [Google Scholar] [CrossRef]
- Patrizio, A.; Ferrari, S.M.; Antonelli, A.; Fallahi, P. A case of Graves’ disease and type 1 diabetes mellitus following SARS-CoV-2 vaccination. J. Autoimmun. 2021, 125, 102738. [Google Scholar] [CrossRef]
- Pla Peris, B.; Merchante Alfaro, A.A.; Maravall Royo, F.J.; Abellan Galiana, P.; Perez Naranjo, S.; Gonzalez Boillos, M. Thyrotoxicosis following SARS-CoV-2 vaccination: A case series and discussion. J. Endocrinol. Investig. 2021, 5, 1071–1077. [Google Scholar] [CrossRef] [PubMed]
- Di Filippo, L.; Castellino, L.; Giustina, A. Occurrence and response to treatment of Graves’ disease after COVID vaccination in two male patients. Endocrine 2022, 75, 19–21. [Google Scholar] [CrossRef] [PubMed]
- Goblirsch, T.J.; Paulson, A.E.; Tashko, G.; Mekonnen, A.J. Graves’ disease following administration of second dose of SARS-CoV-2 vaccine. BMJ Case Rep. 2021, 14, e246432. [Google Scholar] [CrossRef] [PubMed]
- Hamouche, W.; El Soufi, Y.; Alzaraq, S.; Okafor, B.V.; Zhang, F.; Paras, C. A case report of new onset graves’ disease induced by SARS-CoV-2 infection or vaccine? J. Clin. Transl. Endocrinol. Case Rep. 2022, 23, 100104. [Google Scholar] [CrossRef]
- Lee, K.A.; Kim, Y.J.; Jin, H.Y. Thyrotoxicosis after COVID-19 vaccinations: Seven case reports and a literature review. Endocrine 2021, 74, 470–472. [Google Scholar] [CrossRef]
- Pujol, A.; Gomez, L.A.; Gallegos, C.; Nicolau, J.; Sanchis, P.; Gonzalez-Freire, M.; Lopez-Gonzalez, A.A.; Dotres, K.; Masmiquel, L. Thyroid as a target of adjuvant autoimmunity/inflammatory syndrome due to mRNA-based SARS-CoV-2 vaccination: From Graves’ disease to silent thyroiditis. J. Endocrinol. Investig. 2022, 4, 875–882. [Google Scholar] [CrossRef]
- Raven, L.M.; McCormack, A.I.; Greenfield, J.R. Letter to the Editor From Raven et al: “Three Cases of Subacute Thyroiditis Following SARS-CoV-2 Vaccine”. J. Clin. Endocrinol. Metab. 2022, 107, 1767–1768. [Google Scholar] [CrossRef]
- Sriphrapradang, C.; Shantavasinkul, P.C. Graves’ disease following SARS-CoV-2 vaccination. Endocrine 2021, 74, 473–474. [Google Scholar] [CrossRef]
- Wai Lui, D.T.; Lee, K.K.; Lee, C.H.; Lee, A.C.H.; Hung, I.F.N.; Beng Tan, K.C. Development of Graves’ Disease After SARS-CoV-2 mRNA Vaccination: A Case Report and Literature Review. Front. Public Health 2021, 9, 778964. [Google Scholar] [CrossRef] [PubMed]
- Weintraub, M.A.; Ameer, B.; Gregory, N.S. Graves Disease following SARS-CoV-2 Vaccine: Case Series. J. Investig. Med. High Impact Case Rep. 2021, 9, 23247096211063356. [Google Scholar] [CrossRef] [PubMed]
- Sriphrapradang, C. Aggravation of hyperthyroidism after heterologous prime-boost immunization with inactivated and adenovirus-vectored SARS-CoV-2 vaccine in a patient with Graves’ disease. Endocrine 2021, 74, 226–227. [Google Scholar] [CrossRef] [PubMed]
- Pierman, G.; Delgrange, E.; Jonas, C. Recurrence of Graves’ Disease (a Th1-type Cytokine Disease) Following SARS-CoV-2 mRNA Vaccine Administration: A Simple Coincidence? Eur. J. Case Rep. Intern. Med. 2021, 8, 002807. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, K.; Mashiba, T.; Takano, K.; Suzuki, T.; Kami, M.; Takita, M.; Kusumi, E.; Mizuno, Y.; Hamaki, T. A Case of Exacerbation of Subclinical Hyperthyroidism after First Administration of BNT162b2 mRNA COVID-19 Vaccine. Vaccines 2021, 9, 1108. [Google Scholar] [CrossRef]
- Chaudhary, S.; Dogra, V.; Walia, R. Four cases of Graves’ disease following viral vector severe acute respiratory syndrome corona virus-2 (SARS-CoV-2) vaccine. Endocr. J. 2022, 2022, EJ22-0208. [Google Scholar] [CrossRef]
- Sakai, M.; Takao, K.; Kato, T.; Ito, K.; Kubota, S.; Hirose, T.; Liu, Y.; Mizuno, M.; Hirota, T.; Suwa, T.; et al. Graves’ disease after administration of severe respiratoru coronavirus (SARS-CoV-2) vaccine in a type 1 diabetes patient. Intern. Med. 2022, 61, 1561–1565. [Google Scholar] [CrossRef]
- Manta, R.; Martin, C.; Muls, V.; Poppe, K.G. New-onset Graves’ disease following SARS-CoV-2 vaccination: A case report. Eur. Thyroid J. 2022, 11, e220049. [Google Scholar] [CrossRef]
- Bres, F.; Joyeux, M.; Delemer, B.; Vitellius, G.; Barraud, S. Three cases of thyroiditis after COVID-19 RNA-vaccine. Ann. Endocrinol. 2022, 83, 262–264. [Google Scholar] [CrossRef]
- Chua, M.W.J. Graves’ disease after COVID-19 vaccination. Ann. Acad. Med. Singap. 2022, 51, 127–128. [Google Scholar] [CrossRef]
- Taieb, A.; Sawsen, N.; Asma, B.A.; Ghada, S.; Hamza, E.; Yosra, H.; Amel, M.; Molka, C.; Maha, K.; Koussay, A. A rare case of grave’s disease after SARS-CoV-2 vaccine: Is it an adjuvant effect? Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 2627–2630. [Google Scholar] [PubMed]
- Cuenca, D.; Aguilar-Soto, M.; Mercado, M. A case of Graves’ disease following vaccination with the Oxford-AstraZeneca SARS-CoV-2 Vaccine: Case report and review of the literature. Eur. J. Case Rep. Intern. Med. 2022, 9, 003275. [Google Scholar] [CrossRef] [PubMed]
- Shih, S.; Wang, C. SARS-CoV-2 vaccination related hyperthyroidism of Graves’ disease. J. Formos. Med. Assoc. 2022, 121, 1881–1882. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.; Howland, T. Graves’ disease following COVID-19 vaccination. Cureus 2022, 14, e24418. [Google Scholar] [CrossRef] [PubMed]
- Ruggeri, R.M.; Giovanella, L.; Campennì, A. SARS-CoV-2 vaccine may trigger thyroid autoimmunity: Real-life experience and review of the literature. J. Endocrinol. Investig. 2022, 1–7. [Google Scholar] [CrossRef]
- Bostan, H.; Ucan, B.; Kizilgul, M.; Calapkulu, M.; Hepsen, S.; Gul, U.; Unsal, I.; Cakal, E. Relapsed and newly diagnosed Graves’ disease due to immunization against COVID-19: A case series and review of the literature. J. Autoimmun. 2022, 128, 102809. [Google Scholar] [CrossRef]
- Chee, Y.J.; Liew, H.; Han Hoi, W.; Lee, Y.; Lim, B.; Chin, H.X.; Rui Lai, R.T.; Koh, Y.; Tham, M.; Seow, C.J.; et al. SARS-CoV-2 mRNA vaccination and Graves’ diseae: A report of 12 cases and review f the literature. J. Clin. Endocrinol. Metab. 2022, 107, 2324–2330. [Google Scholar] [CrossRef]
- Antonelli, A.; Fallahi, P.; Elia, G.; Ragusa, F.; Paparo, S.R.; Ruffili, I.; Patrizio, A.; Gonnella, D.; Giusti, C.; Virili, C.; et al. Graves’ disease: Clinical manifestations, immune pathogenesis (cytokines and chemokines) and therapy. Best Pract. Res. Clin. Endocrinol. Metabol. 2020, 34, 101388. [Google Scholar] [CrossRef]
- Antonelli, A.; Ferrari, S.M.; Ragusa, F.; Elia, G.; Paparo, S.R.; Ruffili, I.; Patrizio, A.; Giusti, C.; Gonnella, D.; Cristaudo, A.; et al. Graves’ disease: Epidemiology, genetic and environmental risk factors and viruses. Best Pract. Res. Clin. Endocrinol. Metabol. 2020, 34, 101387. [Google Scholar] [CrossRef]
- Ross, D.S.; Burch, H.B.; Copper, D.S.; Greenlee, M.C.; Laurberg, P.; Maia, A.L.; Rivkees, S.A.; Samuels, M.; Sosa, J.A.; Stan, M.N.; et al. 2016 American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and Other Causes of Thyrotoxicosis. Thyroid 2016, 26, 1343–1421. [Google Scholar] [CrossRef]
- Paje, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An uptdate guidelin for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar]
- Pelelgrino, P.; Radice, S.; Clementi, E. Immunogenicity and safety of the human papillomavirus vaccine in patients with autoimmune diseases: A systematic review. Vaccine 2015, 33, 3444–3449. [Google Scholar] [CrossRef] [PubMed]
- Watad, A.; David, P.; Brown, S.; Shoenfeld, Y. Autoimmune/inflammatory Syndrome Induced by Adjuvants and Thyroid Autoimmunity. Front. Endocrinol. 2017, 7, 150. [Google Scholar] [CrossRef]
- Bragazzi, N.L.; Hejly, A.; Watad, A.; Adawi, M.; Amital, H.; Shoenfeld, Y. ASIA syndrome and endocrine autoimmune disorders. Best Pract. Res. Clin. Endocrinol. Metabol. 2020, 34, 101412. [Google Scholar] [CrossRef] [PubMed]
- Ramasamy, M.N.; Minassian, A.M.; Ewer, K.J.; Flaxman, A.L.; Folegatti, P.M.; Owens, D.R.; Voysey, M.; Aley, P.K.; Angus, B.; Babbage, G.; et al. Safety and immunogenicity of ChAdOx1 nCoV-19 vaccine administered in a prime-boost regimen in young and old adults (COV002): A single-blind, randomised, controlled, phase 2/3 trial. Lancet 2021, 396, 1979–1993. [Google Scholar] [CrossRef]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cardenas, V.; Shukarev, G.; Grinsztejn, B.; Goepefert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against Covid-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef]
- Wu, Z.; Hu, Y.; Xu, M.; Chen, Z.; Yang, W.; Jiang, Z.; Li, M.; Jin, H.; Cui, G.; Chen, P.; et al. Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine (CoronaVac) in healthy adults aged 60 years and older: A randomised, double-blind, placebo-controlled, phase 1/2 clinical trial. Lancet Infect. Dis. 2021, 21, 803–812. [Google Scholar] [CrossRef]
- Cagigi, A.; Lorè, K. Immune response induced by mRNA Vaccination in Mice, Monkeys and Humans. Vaccines 2021, 9, 61. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control (ECDC). COVID-19 Vaccine Tracker. Available online: https://vaccinetracker.ecdc.europa.eu/public/extensions/COVID19/vaccinetracker.html#uptake-tab) (accessed on 26 August 2022).
- Shoenfeld, Y.; Agmon-Levin, N. ‘ASIA’—Autoimmune/inflammatory syndrome induced by adjuvants. J. Autoimmun. 2011, 36, 4–8. [Google Scholar] [CrossRef]
- Borgsteede, S.D.; Geersing, T.H.; Tempels-Pavlica, Z. Other excipients than PEG might cause serious hypersensitivity reactions in COVID-19 vaccines. Allergy 2021, 76, 1941–1942. [Google Scholar] [CrossRef]
- Xu, S.; Yang, K.; Li, R.; Zhang, L. mRNA Vaccine Era-Mechanisms, Drug Platform and Clinical Prospection. Int. J. Mol. Sci. 2020, 21, 6582. [Google Scholar] [CrossRef]
- Klimek, L.; Novak, N.; Cabanillas, B.; Jutel, M.; Bousquet, J.; Akdis, C.A. Allergenic components of the mRNA-1273 vaccine for COVID-19: Possible involvement of polyethylene glycol and IgG-mediated complement activation. Allergy 2021, 76, 3307–3313. [Google Scholar] [CrossRef] [PubMed]
- Garvey, L.H.; Nassr, S. Anaphylaxis to the first COVID-19 vaccine: Is polyethylene glycol (PEG) the culprit. Br. J. Anaesth. 2021, 126, 106–108. [Google Scholar] [CrossRef] [PubMed]
- Ndeupen, S.; Qin, Z.; Jacobsen, S.; Bouteau, A.; Estanbouli, H.; Igyarto, B. The mRNA-LNP platform’s lipid nanoparticle component used in preclinical vaccine studies is highly inflammatory. iScience 2021, 24, 103479. [Google Scholar] [CrossRef] [PubMed]
- Sprent, J.; King, C. COVID-19 vaccine side effects: The positives about feeling bad. Sci. Immunol. 2021, 6, eabj9256. [Google Scholar] [CrossRef]
- Antonelli, A.; Ferrari, S.M.; Corrado, A.; Di Domenicantonio, A.; Fallahi, P. Autoimmune thyroid disorders. Autoimmun. Rev. 2015, 14, 174–180. [Google Scholar] [CrossRef]
- Antonelli, A.; Fallahi, P.; Rotondi, M.; Ferrari, S.M.; Romagnani, P.; Grosso, M.; Ferrannini, E.; Serio, M. Increased serum CXCL10 in Graves’ disease or autoimmune thyroiditis is not associated with hyper- or hypothyroidism per se, but is specifically sustained by the autoimmune, inflammatory process. Eur. J. Endocrinol. 2006, 154, 651–658. [Google Scholar] [CrossRef]
- Antonelli, A.; Rotondi, M.; Fallahi, P.; Grosso, M.; Boni, G.; Ferrari, S.M.; Romagnani, P.; Serio, M.; Mariani, G.; Ferrannini, E. Iodine-131 given for therapeutic purposes modulates differently interferon-gamma-inducible alpha-chemokine CXCL10 serum levels in patients with active Graves’ disease or toxic nodular goiter. J. Clin. Endocrinol. Metab. 2007, 92, 1485–1490. [Google Scholar] [CrossRef]
- Fallahi, P.; Ferrari, S.M.; Ragusa, F.; Ruffili, I.; Elia, G.; Paparo, S.R.; Antonelli, A. Th1 Chemokines in Autoimmune Endocrine Disorders. J. Clin. Endocrinol. Metab. 2020, 105, 1046–1060. [Google Scholar] [CrossRef]
- Ferrari, S.M.; Ruffilli, I.; Elia, G.; Ragusa, F.; Paparo, S.R.; Patrizio, A.; Mazzi, V.; Antonelli, A.; Fallahi, P. Chemokines in hyperthyroidism. J. Clin. Transl. Endocrinol. 2019, 16, 100196. [Google Scholar] [CrossRef]
- Poma, M.; Basolo, A.; Bonuccelli, D.; Proietti, A.; Macerola, E.; Ugolini, C.; Torregrossa, L.; Alì, G.; Giannini, R.; Vignali, P.; et al. Activation of Type I and Type II Interferon Signaling in SARS-CoV-2-Positive Thyroid Tissue of Patients Dying from COVID-19. Thyroid 2021, 31, 1766–1775. [Google Scholar] [CrossRef] [PubMed]
- Vojdani, A.; Vojdani, E.; Kharrazian, D. Reaction of Human Monoclonal Antibodies to SARS-CoV-2 Proteins with Tissue Antigens: Implications for Autoimmune Diseases. Front. Immunol. 2021, 11, 3679. [Google Scholar] [CrossRef] [PubMed]
- Kanduc, D.; Shoenfeld, Y. Molecular mimicry between SARS-CoV-2 spike glycoprotein and mammalian proteomes: Implications for the vaccine. Immunol. Res. 2020, 68, 310–313. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Gender | Age | Country | Vaccine | History of COVID | Dose | Personal/Family History of AITD | Medical History | Symptoms | Days until Symptoms | TSH (mIU/L) | fT3 (ng/L) | fT4 (ng/dL) | TgAb (IU/mL) | TPOAb (IU/mL) | TRAb (IU/L) | Thyroid US | Thyroid Scan | Reference |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | 52 | Italy | BNT162b2 | No | 2nd | None | Type 2 Diabetes, Vitiligo | Weight loss, asthenia, insomnia | 20 | <0.004 (N: 0.4–4) | 15 (N: 2.7–5.7) | 5.56 (N: 0.7–1.7) | 30 (N: 0–30) | 21 (N: 0–10) | 6.48 (N: 0–1.49) | Enlargement and hypervascularity | N/A | Patrizio [13] |
| F | 40 | Mexico | BNT162b2 | Yes | 1st | None | None | Nausea, vomiting, fatigue, insomnia, and palpitations | 2 | <0.001 (N: 0.27–4.4) | 10.5 (N: 2.04–4.4) | 3.57 (N: 0.93–1.71) | 210 (N: 0–44) | 3450 (N: 0–5.6) | 16.56 (N: 0–1.75) | Enlargement and hypervascularity | N/A | V.Lastra [11] |
| F | 28 | Mexico | BNT162b2 | No | 1st | None | None | Anxiety, insomnia, palpitations, distal tremors | 3 | <0.001 (N: 0.27–4.4) | 9.2 (N: 2.04–4.4) | 1.84 (N: 0.93–1.71) | 33 (N: 0–44) | 833 (N: 0–5.6) | 5.85 (N: 0–1.75) | N/A | Diffuse toxic goiter | V.Lastra [11] |
| M | 46 | Austria | BNT162b2 | No | 1st | None | None | None | 15 | N/A | 5.18 (N: 2.15–4.12) | 1.63 (N: 0.7–1.7) | N/A | N/A | 2.9 (N: 0–1.5) | Hypoechogenic parenchyma, large anechogenic areas with increased vascularization | Patchy, inhomogenous, normal uptake | Zettining [12] |
| F | 71 | Spain | BNT162b2 | No | 2nd | None | N/A | Weight loss, asthenia, afib | 60 | <0.005 (N: 0.38–5.33) | N/A | 2.3 (N: 0.54–1.24) | <0.9 (N: 0–4) | 30 (N: 0–9) | 3.6 (N: 0–1.75) | Enlargement and hypervascularity | Diffuse toxic goiter | Pla Peris [14] |
| F | 42 | Spain | BNT162b2 | No | 1st | None | N/A | Weight loss, palpitations | 14 | <0.005 (N: 0.38–5.33) | N/A | 2.9 (N: 0.54–1.24) | N/A | 2.5 (N: 0–9) | 4.39 (N: 0–1.75) | Enlargement and hypervascularity | Diffuse toxic goiter | Pla Peris [14] |
| F | 54 | Spain | mRNA-1273 | No | 2nd | None | N/A | Weight loss, asthenia, palpitations | 14 | <0.005 (N: 0.38–5.33) | N/A | 4.7 (N: 0.54–1.24) | 55 (N: 0–4) | 30 (N: 0–9) | 5.1 (N: 0–1.75) | Enlargement and hypervascularity | N/A | Pla Peris [14] |
| F | 46 | Spain | BNT162b2 | No | 1st | None | N/A | Weight loss, palpitations, irritability | 50 | <0.005 (N: 0.38–5.33) | N/A | 3.2 (N: 0.54–1.24) | 90 (N: 0–4) | 60 (N: 0–9) | 3.2 (N: 0–1.75) | Enlargement and hypervascularity | N/A | Pla Peris [14] |
| M | 32 | Italy | ChAdOx1 | No | 2nd | None | None | Anxiety, tachycardia, palpitations | 10 | 0.005 (N: N/A) | 7.9 (N: 2–4.4) | 2.96 (N: 0.6–1.12) | N/A | N/A | 7.98 (N: 0–2.9) | Enlargement and hypervascularity | N/A | Di Filippo [15] |
| M | 35 | Italy | ChAdOx1 | No | 1st | None | None | Nausea, headache, tachycardia, palpitations, asthenia | 5 | <0.004 (N: N/A) | N/A | 4,96 (N: 0.6–1.12) | N/A | N/A | 3.2 (N: 0–2.9) | Enlargement and hypervascularity | N/A | Di Filippo [15] |
| F | 71 | USA | BNT162b2 | No | 2nd | GMN/None | Stage IV breast cancer in remission | Tachycardia, palpitations, fever, dizziness, distal tremors | 14 | <0.02 (N: 0.3–2) | N/A | 7.2 (N: 0.9–1.7) | N/A | 8.9 (N: 0–9) | N/A(TSI +ve) | Multinodular Goiter | N/A | Goblirsch [16] |
| M | 32 | USA | BNT162b2 | Yes | 1st | None | None | Palpitations, insomnia, tremors, irritability, sweating, dyspnea | 10 | <0.005 (N: 0.282–4) | N/A | 5.41 (N: 0.84–1.62) | 53 (N: 0–40) | 119 (N: 0–35) | N/A (TSI +ve) | Heterogeneous thyroid with micronodules | Diffuse uptake | Hamouche [17] |
| M | 70 | Thailand | ChAdOx1 | No | 2nd | None | N/A | Myalgia, palpitations, exertional dyspnea | 2 | <0.0036 (N: 0.35–4.94) | >20 (N: 1.88–3.18) | 3.19 (N: 0.7–1.48) | N/A | N/A | 3.23 (N: 0–1.75) | N/A | N/A | Sriphrapradang [21] |
| F | 38 | Spain | BNT162b2 | No | 1st | None | Schizophrenia | Behavioral disturbance, insomnia, sweating | 12 | <0.008 (N: 0.35–4.95) | 7.46 (N: 0.7–1.48) | 2.01 (N: 0.7–1.48) | 36.57 (N: 0–5.6) | 3303.71 (N: 0–5.6) | 12.54 (N: 0–0.7) | Reduced echogenicity, echogenic septa, hypervascularity | Diffuse toxic goiter | Pujol [19] |
| F | 38 | USA | BNT162b2 | No | 1st | None | None | Fever, tachycardia, GI symptoms (thyroid storm) | 5 | <0.008 (N: 0.45–4.5) | N/A | 8.39 (N: 0.82–1.77) | N/A | 1730 (N: 0–9) | 32 (N: 0–1.75) | Enlargement and hypervascularity | N/A | Weintraub [23] |
| F | 63 | USA | mRNA-1273 | No | 1st | None | N/A (sister with LES) | Pruritic rash upper chest and neck | 7 | 0.011 (N: 0.55–4.78) | N/A | 2.4 (N: 0.9–1.8) | N/A | 1149 (N: 0–9) | 22 (N: 0–1.75) | Heterogeneous thyroid and hypervascularity | Diffuse uptake | Weintraub [23] |
| M | 30 | USA | BNT162b2 | No | 2nd | None | None (mother post- partum GD) | Weight loss, irritability, palpitations, tremors, restless sleep | 28 | <0.005 (N: 0.45–4.5) | N/A | 1.77 (N: 0.82–1.77) | N/A | 15 (N: 0–34) | N/A (TSI +ve) | N/A | N/A | Weintraub [23] |
| F | 40 | China | BNT162b2 | No | 2nd | Hypothyroidism/None | None | Palpitations and tachycardia | 35 | <0.02 (N: 0.47–4.68) | 19.8 (N: 2.77–5.29) | 5.17 (N: 0.7–2.19) | 7.2 (N: 0–4) | 239.2 (N: 0–5) | N/A (TSI +ve) | Heterogeneous thyroid and hypervascularity | Diffuse uptake | Wai Lu [22] |
| F | 35 | Australia | ChAdOx1 | No | 1st | None/Hyperthyroidism | None | Palpitations, hyperphagia, heat intolerance and tremors | 5 | <0.02 (N: 0.5–4) | >19.5 (N: 2.2–3.9) | 4.97 (N: 0.77–1.55) | 33 (N: 0–4.5) | >1300 (N: 0–4.5) | 24 (N: 0–0.55) | Heterogeneous thyroid and hypervascularity/A | Raven [20] | |
| F | 46 | South Korea | ChAdOx1 | N/A | 1st | None | N/A | Chest pain, dyspnea | 1 | 0.01 (N: 0.55–4.78) | N/A | 2.63 (N: 0.89–1.76) | 137.5 (N: 0–115) | 77.72 (N: 0–34) | 6.42 (N: 0–1.75) | Diffuse Hypervascularity | Diffuse uptake | Lee [18] |
| F | 73 | South Korea | ChAdOx1 | N/A | 2nd | None | N/A | Weight loss, dyspnea | 14 | <0.008 (N: 0.55–4.78) | N/A | 5.7 (N: 0.89–1.76) | N/A | 41.03 (N: 0–34) | 6.30 (N: 0–1.75) | Diffuse Hypervascularity | Diffuse uptake | Lee [18] |
| M | 20 | India | ChAdOx1 | N/A | 1st | None | None | Weight Loss, tremors | 7 | 0.002 (N: 0.34–5.60) | N/A | N/A | N/A | N/A | 2.6 (<1.22) | N/A | N/A | Chaudhary [27] |
| F | 46 | India | ChAdOx1 | N/A | 1st | None/AITD | None | Weight loss | 10 | <0.01 (N: 0.34–5.60) | N/A | N/A | N/A | N/A | >40 (<1.22) | N/A | N/A | Chaudhary [27] |
| F | 19 | India | ChAdOx1 | N/A | 1st | None/AITD | None | Weight loss, palpitations, hair loss | 28 | <0.01 (N: 0.34–5.60) | N/A | N/A | N/A | N/A | 7.32 (<1.22) | N/A | N/A | Chaudhary [27] |
| F | 37 | India | ChAdOx1 | N/A | 1st | None/AITD | None | Weight loss, palpitations, increased defecation | 14 | <0.01 (N: 0.34–5.60) | N/A | N/A | N/A | N/A | 4.37 (<1.22) | N/A | N/A | Chaudhary [27] |
| F | 31 | Japan | BNT162b2 | N/A | 2nd | None | Type 1 Diabetes | Dyspnea, sweating, diarrhea | 7 | <0.005 (N: 0.61–4.23) | 32.5 (N: 2.3–4) | >7.77 (N: 0.9–1.7) | 82 (<28) | 481 (<16) | 11.9 (<2.0) | Diffuse Hypervascularity | N/A | Sakai [28] |
| M | 22 | Belgium | BNT162b2 | Yes | 1st | None | Ulcerative Colitis and Nephrotic Syndrome | Tremors | 14 | <0.01 (N: 0.27–4.20) | 17.7 (N: 3.10–6.8) | 3.17 (N: 0.9–1.7) | N/A | N/A | 3.76 (<0.55) | Heterogeneous thyroid and hypervascularity | Diffuse uptake | Manta [29] |
| F | 44 | France | BNT162b2 | N/A | 1st | AITD/None | N/A | None | 5 | <0.01 (N: N/A) | N/A | N/A | N/A | N/A | N/A(+ve) | Diffuse Hypervascularity | N/A | Bres [30] |
| F | 45 | Singapore | BNT162b2 | N/A | 1st | None | None | Chest pain, palpitations | 4 | <0.005 (N: 0.7–4.28) | N/A | 3.5 (N: 0.98–1.57) | N/A | 0.3 (N: N/A) | 5.75 (N: <1.76) | Heterogeneous thyroid and hypervascularity | N/A | Chua [31] |
| F | 43 | Tunisia | BNT162b2 | No | 1st | None | None | Palpitations, sleep disorders, heat intolerance, asthenia | 3 | <0.002 (N: 0.38–5.33) | N/A | 5.12 (N: 0.93–1.7) | N/A | N/A | 3.1 (N: <1) | N/A | Diffuse uptake | Taieb [32] |
| M | 57 | Mexico | ChAdOx1 | No | 1st | None | None | Tremor, palpitations, weight loss, asthenia | 7 | <0.005 (N: 0.3–3) | N/A | 4 (N: 0.6–1.2) | N/A(+ve) | N/A(+ve) | N/A | Enlargement and hypervascularity | Diffuse uptake | Cuenca [33] |
| F | 39 | Taiwan | mRNA-1273 | N/A | 1st | AITD/none | None | Palpitations, tremors | 14 | <0.0038 (N: 0.35–4.94) | N/A | 1.54 (N: 0.7–1.48) | <3.0 (N: <14.4) | 64.58 (N: <5.61) | 42.4 (N: <10) | N/A | N/A | Shih [34] |
| F | 59 | Taiwan | ChAdOx1 | N/A | 1st | None/AITD | None | Dyspnea, palpitations, dizziness | 14 | <0.0038 (N: 0.35–4.94) | N/A | 2.28 (N: 0.7–1.48) | 1494.78 (N: <14.4) | <0.3 (N: <5.61) | 68.7 (N: <10) | N/A | N/A | Shih [34] |
| F | 44 | Taiwan | ChAdOx1 | N/A | 1st | None | None | Tremors, weight loss, heat intolerance | 4 | <0.0038 (N: 0.35–4.94) | N/A | 2.74 (N: 0.7–1.48) | 2904.39 (N: <14.4) | 206.64 (N: <5.61) | 80.9 (N: <10) | N/A | N/A | Shih [34] |
| M | 42 | USA | mRNA-1273 | N/A | 3rd | None | None | Dyspnea, sleep disturbance, weight loss, asthenia, nausea, headache | 2 | <0.015 (N: 0.45–4.5) | N/A | 5.96 (N: 0.78–2.19) | N/A | 70.25 (N: <5.6) | 16.1 (N: <1.75) | Heterogeneous thyroid and hypervascularity | Diffuse uptake | Singh [35] |
| F | 68 | USA | Ad26. COV2.S | N/A | 1st | None | None | Atrial fibrillation | 30 | <0.01 (N: 0.45–4.5) | 13.8 (N: 2.5–3.9) | 3.6 (N: 0.78–0.6–1.3) | N/A | 5.84 (N: <5.6) | 14.3 (N: <1.75) | N/A | Diffuse uptake | Singh [35] |
| M | 50 | Italy | BNT162b2 | N/A | 1st | None/AITD | None | Asthenia, palpitations, tremors, sleep disturbance | 14 | 0.001 (N: 0.25–0.4) | 10.47 (N: 2–4) | 2 (N: 0.7–1.48) | 385.49 (N: <40) | 529.5 (N: <10) | 5 (N: <1) | Enlargement and hypervascularity | Diffuse uptake | Ruggeri [36] |
| M | 50 | Italy | BNT162b2 | N/A | 1st | None/AITD | None | Asthenia, palpitations, tremors, sleep disturbance | 14 | 0.001 (N: 0.25–0.4) | 10.47 (N: 2–4) | 2 (N: 0.7–1.48) | 385.49 (N: <40) | 529.5 (N: <10) | 5 (N: <1) | Enlargement and hypervascularity | Diffuse uptake | Ruggeri [36] |
| F | 47 | Turkey | BNT162b2 | No | 1st | None | None | Sweating, palpitations | 5 | <0.01 (N: 0.27–4.2) | 11 (N: 2.4.4) | 3.32 (N: 0.93–1.7) | 320 (N: <115) | 11.2 (N: <34) | 22.7 (N: <1.5) | Heterogeneous thyroid and hypervascularity | N/A | Bostan [37] |
| M | 46 | Turkey | BNT162b2 | No | 2nd | None | None | Sweating, palpitations, weight loss | 21 | <0.01 (N: 0.27–4.2) | 25.3(N: 2.4.4) | >7.77 (N: 0.93–1.7) | 334 (N: <115) | 146 (N: <34) | 9.10 (N: <1.5) | Enlargement and hypervascularity | N/A | Bostan [37] |
| F | 51 | Turkey | BNT162b2 | N/A | 2nd | None | Type 2 Diabetes, Hypertension | Sweating, palpitations, fever | 4 | <0.01 (N: 0.27–4.2) | 12.6 (N: 2.4.4) | 3.72 (N: 0.93–1.7) | 18.2 (N: <115) | 12.4 (N: <34) | 5.04 (N: <1.5) | Enlargement and hypervascularity | Diffuse toxic goiter | Bostan [37] |
| F | 53 | Turkey | BNT162b2 | Yes | 2nd | AITD/none | None | Sweating, palpitations, weight loss | 7 | <0.01 (N: 0.27–4.2) | 8.83 (N: 2.4.4) | 4.01 (N: 0.93–1.7) | 1197 (N: <115) | 55 (N: <34) | 17.8 (N: <1.5) | Heterogeneous thyroid and hypervascularity | Diffuse uptake | Bostan [37] |
| F | 33 | China | N/A (mRNA) | No | 1st | None/AITD | N/A | N/A | 7 | 0.01 (N:N/A) | N/A | 3.4 (N: 0.62–1.24) | N/A | N/A | 7.3 (N: <1) | N/A | N/A | Chee [38] |
| F | 37 | China | N/A (mRNA) | No | 1st | None | N/A | N/A | 7 | <0.01 (N:N/A) | N/A | 4.6 (N: 0.62–1.24) | N/A | N/A | 3.8 (N: <1) | N/A | N/A | Chee [38] |
| F | 37 | China | N/A (mRNA) | No | 2nd | None | N/A | N/A | 21 | <0.01 (N:N/A) | N/A | 5.5 (N: 0.62–1.24) | N/A | N/A | 11.2 (N: <1) | N/A | N/A | Chee [38] |
| F | 34 | China | N/A (mRNA) | No | 1st | None/AITD | N/A | N/A | 26 | 0.01 (N:N/A) | 23.8 (N: 3.5–6) | 5.28 (N: 0.62–1.24) | N/A | N/A | 32 (N: <1) | N/A | N/A | Chee [38] |
| F | 33 | China | N/A (mRNA) | No | 2nd | None | N/A | N/A | 9 | <0.01 (N:N/A) | N/A | 2.25 (N: 0.62–1.24) | N/A | N/A | 4.6 (N: <1) | N/A | N/A | Chee [38] |
| F | 43 | China | N/A (mRNA) | No | 2nd | None | N/A | N/A | 13 | <0.01 (N:N/A) | >40 (N: 3.5–6) | 5.4 (N: 0.62–1.24) | N/A | N/A | 6.2 (N: <1) | N/A | N/A | Chee [38] |
| Gender | Age | Country | Vaccine | History of COVID | Dose | Personal/Family History of AITD | Medical History | Symptoms | Days until Symptoms | TSH (mIU/L) | fT3 (ng/L) | fT4 (ng/dL) | TgAb (IU/mL) | TPOAb (IU/mL) | TRAb (IU/L) | Thyroid US | Thyroid Scan | Reference |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| F | 71 | Austria | BNT162b2 | No | 2nd | GD/none | N/A | Palpitations and sweating | 30 | N/A | 11.1 (N: 2.15–4.12) | 3.56 (N: 0.7–1.7) | N/A | N/A | 4.2 (N: 0–1.5) | Heterogeneous thyroid and hypervascularization | Mild increased uptake | Zettining [12] |
| F | 64 | Japan | BNT162b2 | No | 1st | Subclinical Hyperthyroidism/none | colorectal cancer, DM, obesity | Palpitations, dyspnea, fever, legs edema | 6 | <0.008 (N: N/A) | 23.2 (N: N/A) | 3.32 (N: N/A) | N/A | N/A | 33.8 (N: N/A) | Enlargement and hypervascularity | N/A | Yamamoto [26] |
| F | 34 | Belgium | BNT162b2 | No | 1st | GD/none | None | Tremors, sweating, weight loss, swelling of eyelids | 10 | <0.01 (N: 0.4–2.75) | 14.3 (N: 1.95–4.23) | 2.54 (N: 0.75–1.6) | N/A | N/A | >40 (N: 0–0.55) | N/A | N/A | Pierman [25] |
| F | 30 | Thailand | CoronaVac+ChAdOx1 | No | 3rd (ChAdOx1) | GD on MTZ/none | None | Palpitations, weight loss, increased appetite | 4 | 0.006 (N: 0.35–4.94) | 3.21 (N: 1.88–3.18) | 1.29 (N: 0.7–1.48 | N/A | N/A | 13.4 (N: 0–1,75) | N/A | N/A | Sriphrapradang [24] |
| M | 34 | South Korea | Ad26. COV2.S | N/A | 1st | GD/none | N/A | Weight loss, palpitations | 14 | <0.008 (N: 0.55–4.78) | N/A | 2.06 (N: 0.89–1.76) | N/A | N/A | 4.24 (N: 0–1.75) | Diffuse Hypervascularity | N/A | Lee [18] |
| M | 41 | Singapore | mRNA-1273 | N/A | 1st | GD/none | N/A | Tremors, palpitations | 5 | <0.001 (N: 0.7–4.28) | N/A | 3.74 (N: 0.98–1.57) | N/A | N/A | 3.85 (N: <1.76) | N/A | N/A | Chua [31] |
| F | 44 | Turkey | CoronaVac | No | 1st | GD/none | None | Sweating, palpitations, asthenia | 7 | <0.01 (N: 0.27–4.2) | 9.65 (N: 2.4.4) | 2.67 (N: 0.93–1.7) | 119 (N: <115) | 284 (N: <34) | 12.18 (N: <1.5) | Heterogeneous thyroid and hypervascularity | N/A | Bostan [37] |
| M | 49 | Turkey | BNT162b2 | No | 2nd | GD/none | None | Sweating, palpitations, tremors | 30 | <0.01 (N: 0.27–4.2) | 13.50 (N: 2.4.4) | 3.86 (N: 0.93–1.7) | 236 (N: <115) | 435 (N: <34) | 3.01 (N: <1.5) | Diffuse Hypervascularity | N/A | Bostan [37] |
| F | 31 | Turkey | BNT162b2 | No | 1st | GD/none | Breast cancer | Sweating, asthenia | 21 | <0.01 (N: 0.27–4.2) | 21.7 (N: 2.4.4) | >7.77 (N: 0.93–1.7) | 11 (N: <115) | 325 (N: <34) | 19.3 (N: <1.5) | Diffuse Hypervascularity | N/A | Bostan [37] |
| M | 59 | China | N/A (mRNA) | No | 1st | GD/AITD | N/A | N/A | 21 | <0.01 (N:N/A) | N/A | 3.8 (N:0.62–1.24) | N/A | N/A | 12.8 (N: <1) | N/A | N/A | Chee [38] |
| F | 74 | China | N/A (mRNA) | No | 2nd | GD/AITD | N/A | N/A | 11 | 0.02 (N:N/A) | N/A | 1.08 (N:0.62–1.24) | N/A | N/A | 6.2 (N: <1) | N/A | N/A | Chee [38] |
| F | 25 | China | N/A (mRNA) | No | 2nd | GD/AITD | N/A | N/A | 11 | 0.01 (N:N/A) | 6.3 (N: 3.5–6) | 1.16 (N:0.62–1.24) | N/A | N/A | 2.9 (N: <1) | N/A | N/A | Chee [38] |
| F | 41 | China | N/A (mRNA) | No | 2nd | GD/none | N/A | N/A | 28 | <0.01 (N:N/A) | N/A | 3.88 (N:0.62–1.24) | N/A | N/A | 3.9 (N: <1) | N/A | N/A | Chee [38] |
| F | 24 | China | N/A (mRNA) | No | 2nd | GD/none | N/A | N/A | 63 | 0.01 (N:N/A) | N/A | 1.55 (N:0.62–1.24) | N/A | N/A | 2.4 (N: <1) | N/A | N/A | Chee [38] |
| F | 22 | China | N/A (mRNA) | No | 1st | GD/none | N/A | N/A | 5 | 0.01 (N:N/A) | >40 (N: 3.5–6) | 5.43 (N:0.62–1.24) | N/A | N/A | 5.8 (N: <1) | N/A | N/A | Chee [38] |
| New Onset GD | GD Recurrence | |
|---|---|---|
| Number of Cases | 48 | 15 |
| Sex | F (70.8%)—M (29.2%) | F (73.3%)—M (26.7%) |
| Age (years), median [IQR] | 43 [IQR 35–50.5] | 41 [IQR 30–59] |
| Type of SARS-Cov-2 vaccine | BNT162b2 50% ChAdOx1 27% mRNA-1273 8.3% Ad26.COV2.S 2.2% Not specified (mRNA) 12.5% | BNT162b2 33.3% ChAdOx1 + CoronaVac 6.6% Ad26.COV2.S 6.6% CoronaVac 6.6% mRNA-1273 6.6% Not specified (mRNA) 40% |
| Days to symptoms onset, median [IQR] | 10 [IQR 5–14] | 11 [IQR 6–28] |
| Major symptoms | palpitations (61.9%) weight loss (35.7%) distal tremor (28.6%) behavioral/sleep disorders (26.1%) asthenia (21.4%) GI symptoms (14.3%) | palpitations (77.8%) sweating (55.5%) weight loss (33.3%) |
| TSH (IU/mL), median [IQR] | 0.008 [0.004–0.01] | 0.01 [0.008–0.01] |
| fT3 (ng/L), median [IQR] | 13.2 [9.83–19.9] | 13.5 [7.97–22.45] |
| fT4 (ng/dL), median [IQR] | 3.58 [254–5.34] | 3.32 [1.55–3.86] |
| TRAb (IU/L), median [IQR] | 6.45 [4.39–16-56] | 5.8 [3.85–13.4] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patrizio, A.; Ferrari, S.M.; Elia, G.; Ragusa, F.; Paparo, S.R.; Mazzi, V.; Antonelli, A.; Fallahi, P. Graves’ Disease Following SARS-CoV-2 Vaccination: A Systematic Review. Vaccines 2022, 10, 1445. https://doi.org/10.3390/vaccines10091445
Patrizio A, Ferrari SM, Elia G, Ragusa F, Paparo SR, Mazzi V, Antonelli A, Fallahi P. Graves’ Disease Following SARS-CoV-2 Vaccination: A Systematic Review. Vaccines. 2022; 10(9):1445. https://doi.org/10.3390/vaccines10091445
Chicago/Turabian StylePatrizio, Armando, Silvia Martina Ferrari, Giusy Elia, Francesca Ragusa, Sabrina Rosaria Paparo, Valeria Mazzi, Alessandro Antonelli, and Poupak Fallahi. 2022. "Graves’ Disease Following SARS-CoV-2 Vaccination: A Systematic Review" Vaccines 10, no. 9: 1445. https://doi.org/10.3390/vaccines10091445