
A Rare Adverse Effect of the COVID-19 Vaccine on Autoimmune Encephalitis

 , , and
, , and
Abstract
:1. Introduction
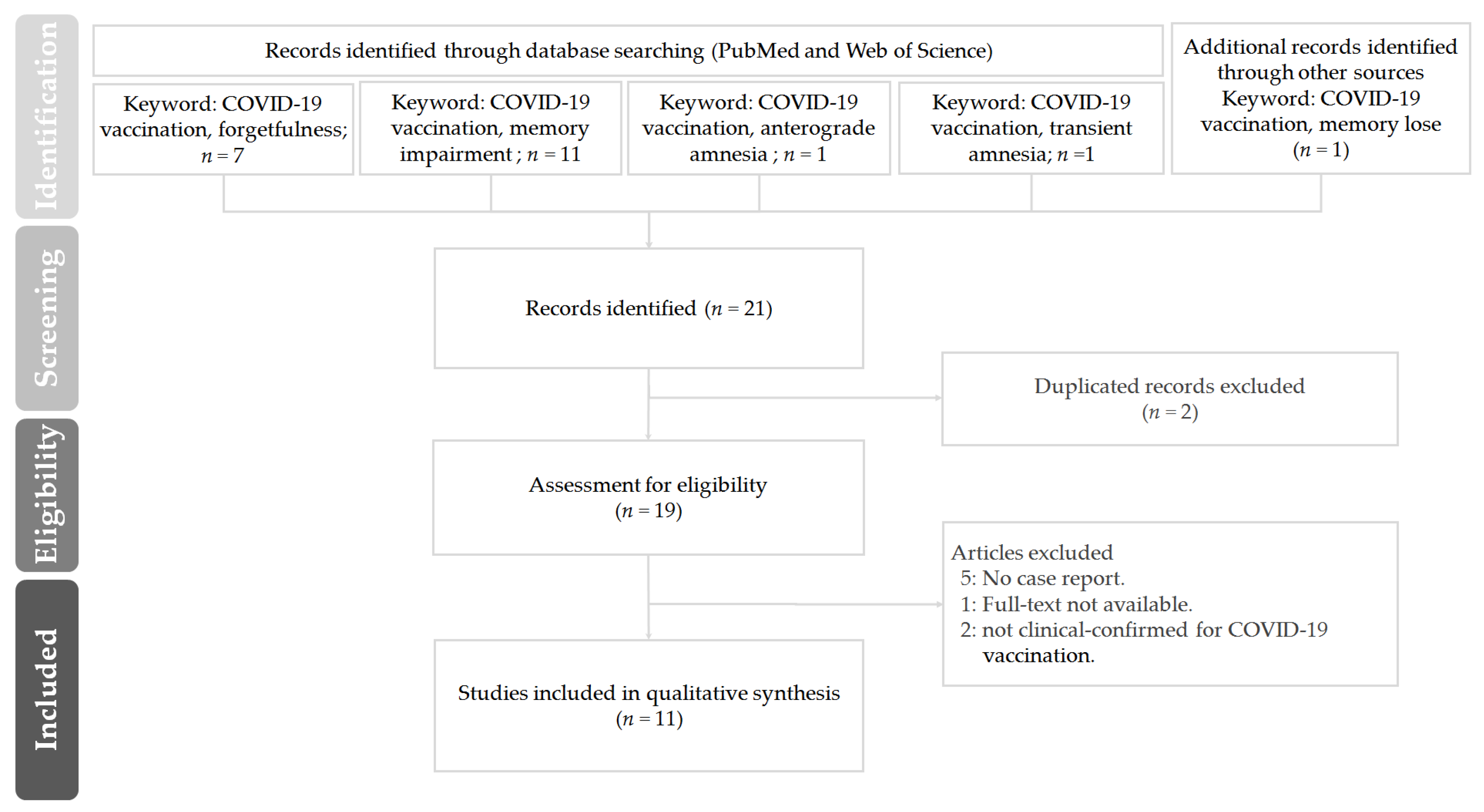
2. Experimental Method
3. Result and Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease (COVID-19) Outbreak. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 24 June 2022).
- Janik, E.; Niemcewicz, M.; Podogrocki, M.; Saluk-Bijak, J.; Bijak, M. Existing Drugs Considered as Promising in COVID-19 Therapy. Int. J. Mol. Sci. 2021, 22, 5434. [Google Scholar] [CrossRef]
- Ho, T.-C.; Wang, Y.-H.; Chen, Y.-L.; Tsai, W.-C.; Lee, C.-H.; Chuang, K.-P.; Chen, Y.-M.; Yuan, C.-H.; Ho, S.-Y.; Yang, M.-H.; et al. Chloroquine and Hydroxychloroquine: Efficacy in the Treatment of the COVID-19. Pathogens 2021, 10, 217. [Google Scholar] [CrossRef]
- Mathieu, E.; Ritchie, H.; Ortiz-Ospina, E.; Roser, M.; Hasell, J.; Appel, C.; Giattion, C.; Rodés-Guirao, L. A global database of COVID-19 vaccinations. Nat. Hum. Behav. 2021, 5, 947–953. [Google Scholar] [CrossRef]
- Coronavirus (COVID-19) Vaccinations. Available online: https://ourworldindata.org/COVID-vaccinations (accessed on 24 June 2022).
- Fernandes, J.; Jaggernauth, S.; Ramnarine, V.; Mohammed, S.R.; Khan, C.; Panday, A. Neurological Conditions following COVID-19 Vaccinations: Chance or Association? Cureus 2022, 14, 21919. [Google Scholar] [CrossRef]
- Rabail, R.; Ahmed, W.; Ilyas, M.; Rajoka, M.S.R.; Hassoun, A.; Khalid, A.R.; Khan, M.R.; Aadil, R.M. The Side Effects and Adverse Clinical Cases Reported after COVID-19 Immunization. Vaccines 2022, 10, 488. [Google Scholar] [CrossRef]
- Butler, M.; Coebergh, J.; Safavi, F.; Carson, A.; Hallett, M.; Michael, B.; Pollak, T.A.; Solomon, T.; Stone, J.; Nicholson, T.R. Functional Neurological Disorder after SARS-CoV-2 Vaccines: Two Case Reports and Discussion of Potential Public Health Implications. J. Neuropsychiatry Clin. Neurosci. 2021, 33, 345–348. [Google Scholar] [CrossRef]
- Kwon, H.; Kim, T. Autoimmune encephalitis following ChAdOx1-S SARS-CoV-2 vaccination. Neurol. Sci. 2022, 43, 1487–1489. [Google Scholar] [CrossRef]
- Zuhorn, F.; Graf, T.; Klingebiel, R.; Schäbitz, W.R.; Rogalewski, A. Postvaccinal Encephalitis after ChAdOx1 nCov-19. Ann. Neurol. 2021, 90, 506–511. [Google Scholar] [CrossRef]
- Taiwan CDC 2021/8/11 Adverse Events Notification after COVID-19 Vaccination. Available online: https://www.cdc.gov.tw/Uploads/da83f743-c251-426e-ab08-a5f4ebb34f23.pdf. (accessed on 11 August 2021).
- Zlotnik, Y.; Gadoth, A.; Abu-Salameh, I.; Horev, A.; Novoa, R.; Ifergane, G. Case Report: Anti-LGI1 Encephalitis following COVID-19 Vaccination. Front. Immunol. 2022, 12, 813487. [Google Scholar] [CrossRef]
- Al-Mashdali, A.F.; Ata, Y.M.; Sadik, N. Post-COVID-19 vaccine acute hyperactive encephalopathy with dramatic response to methylprednisolone: A case report. Ann. Med. Surg. 2021, 69, 102803. [Google Scholar] [CrossRef]
- Vidyanti, A.N.; Maulida Awaliyah, M.T.N.; Fauzi, A.R.; Harahap, I.S.K.; Mulya, D.P. Dementia in a patient with autoimmune disease and hypercoagulable state worsened by COVID-19 vaccination: A case report. Ann. Med. Surg. 2022, 78, 103886. [Google Scholar] [CrossRef]
- Gao, J.J.; Tseng, H.P.; Lin, C.L.; Hsu, R.F.; Lee, M.H.; Liu, C.H. Acute encephalitis after COVID-19 vaccination: A case report and literature review. Hum. Vac. Immunother. 2022, 2082206. [Google Scholar] [CrossRef]
- Li, S.Y.; Chen, H.H.; Liu, P.Y.; Shi, Z.Y.; Lin, Y.H.; Tsai, C.A.; Lin, S.P. Case report of acute encephalitis following the AstraZeneca COVID-19 vaccine. Int. J. Rheum. Dis. 2022; epub ahead of print. [Google Scholar] [CrossRef]
- Cao, L.; Ren, L. Acute disseminated encephalomyelitis after severe acute respiratory syndrome coronavirus 2 vaccination: A case report. Acta Neurol. Belg. 2022, 122, 793–795. [Google Scholar] [CrossRef]
- Chaurasia, B.; Chavda, V.; Lu, B.; Garg, K.; Montemurro, N. Cognitive deficits and memory impairments after COVID-19 (Covishield) vaccination. Brain Behav. Immun. Health 2022, 22, 100463. [Google Scholar] [CrossRef]
- Khan, E.; Shrestha, A.K.; Colantonio, M.A.; Liberio, R.N.; Sriwastava, S. Acute transverse myelitis following SARS-CoV-2 vaccination: A case report and review of literature. J. Neurol. 2022, 269, 1121–1132. [Google Scholar] [CrossRef]
- Giannotta, G.; Giannotta, N. Vaccines and neuroinflammation. Int. J. Public Health Saf. 2018, 3, 1000163. [Google Scholar]
- Hervé, C.; Laupèze, B.; Del Giudice, G.; Didierlaurent, A.M.; Tavares Da Silva, F. The how’s and what’s of vaccine reactogenicity. NPJ Vaccines 2019, 4, 39. [Google Scholar] [CrossRef] [Green Version]
- Liu, B.D.; Ugolini, C.; Jha, P. Two Cases of Post-Moderna COVID-19 Vaccine Encephalopathy Associated with Nonconvulsive Status Epilepticus. Cureus 2021, 13, e16172. [Google Scholar] [CrossRef]
- Karnik, M.; Beeraka, N.M.; Uthaiah, C.A.; Nataraj, S.M.; Bettadapura, A.; Aliev, G.; Madhunapantula, S.V. A Review on SARS-CoV-2-Induced Neuroinflammation, Neurodevelopmental Complications, and Recent Updates on the Vaccine Development. Mol. Neurobiol. 2021, 58, 4535–4563. [Google Scholar] [CrossRef]
- Umapathi, T.; Quek, W.; Yen, J.M.; Khin, H.; Mah, Y.Y.; Chan, C.; Ling, L.M.; Yu, W.Y. Encephalopathy in COVID-19 patients; viral, parainfectious, or both? Neurol. Sci. 2020, 21, 100275. [Google Scholar] [CrossRef]
- Baldelli, L.; Amore, G.; Montini, A.; Panzera, I.; Rossi, S.; Cortelli, P.; Guarino, M.; Rinaldi, R.; D’Angelo, R. Hyperacute reversible encephalopathy related to cytokine storm following COVID-19 vaccine. J. Neuroimmunol. 2021, 358, 577661. [Google Scholar] [CrossRef]
- Garg, R.K.; Paliwal, V.K. Spectrum of neurological complications following COVID-19 vaccination. Neurol. Sci. 2022, 43, 3–40. [Google Scholar] [CrossRef] [PubMed]
- Vogrig, A.; Janes, F.; Gigli, G.L.; Curcio, F.; Negro, I.D.; D’Agostini, S.; Fabris, M.; Valente, M. Acute disseminated encephalomyelitis after SARS-CoV-2 vaccination. Clin. Neurol. Neurosurg. 2021, 208, 106839. [Google Scholar] [CrossRef] [PubMed]
- Armangue, T.; Olivé-Cirera, G.; Martínez-Hernandez, E.; Sepulveda, M.; Ruiz-Garcia, R.; Muñoz-Batista, M.; Ariño, H.; González-Álvarez, V.; Felipe-Rucián, A.; Jesús Martínez-González, M.; et al. Associations of paediatric demyelinating and encephalitic syndromes with myelin oligodendrocyte gly-coprotein antibodies: A multicentre observational study. Lancet Neurol. 2020, 19, 234–246. [Google Scholar] [CrossRef]
- Uthman, I.W.; Gharavi, A.E. Viral infections and antiphospholipid antibodies. Semin. Arthritis Rheum. 2002, 31, 256–263. [Google Scholar] [CrossRef]
- Zhang, Y.; Xiao, M.; Zhang, S.; Xia, P.; Cao, W.; Jiang, W.; Chen, H.; Ding, X.; Zhao, H.; Zhang, H.; et al. Coagulopathy and antiphospholipid antibodies in patients with COVID-19. N. Engl. J. Med. 2020, 382, e38. [Google Scholar] [CrossRef]
- Parodi, A.; Gasparini, G.; Cozzani, E. Could antiphospholipid antibodies contribute to coagulopathy in COVID-19? J. Am. Acad. Dermatol. 2020, 83, e249. [Google Scholar] [CrossRef]
- Maria, A.; Diaz-Cau, I.; Benejean, J.M.; Nutz, A.; Schiffmann, A.; Biron-Andreani, C.; Guilpain, P. Flare of antiphospholipid syndrome in the course of COVID-19. TH Open 2020, 4, e207–e210. [Google Scholar] [CrossRef]
- Talotta, R.; Robertson, E.S. Antiphospholipid antibodies and risk of post-COVID-19 vaccination thrombophilia: The straw that breaks the camel’s back? Cytokine Growth Factor Rev. 2021, 60, 52–60. [Google Scholar] [CrossRef]
- Cruz-Tapias, P.; Blank, M.; Anaya, J.-M.; Shoenfeld, Y. Infections and vaccines in the etiology of antiphospholipid syndrome. Curr. Opin. Rheumatol. 2012, 24, 389–393. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Country | Case | Vaccine | Neurological Disorder of Memory | Clinical Diagnostics | Post-Vaccinal Encephalitis | Ref. |
|---|---|---|---|---|---|---|
| United Kingdom | 38-year-old female | First dose of the Pfizer-BioNTech SARS-CoV-2 vaccine | Ongoing difficulties with short-term memory. | The blood pressure, glucose level, and heart rate were found to be normal, as were electrocardiogram and brain CT data. | Functional neurological disorder. | [8] |
| 36-year-old female | First dose of Moderna SARS-CoV-2 vaccine | Functional weakness, tremor likely due to anxiety, and fatigue symptoms similar to those associated with chronic fatigue syndrome. | MRI of the brain and spine were normal, as were electromyography and nerve conduction velocity studies. | Chronic fatigue syndrome. | [8] | |
| Korea | 57-year-old female | Two doses of the AstraZeneca ChAdOx1-S vaccine | Cognitive decline including attention and memory deficits along with gradually worsening dysphasia. | A cerebrospinal fluid (CSF) study was normal. However, magnetic resonance imaging (MRI) of the brain demonstrated restricted diffusion along the left insular and mesial temporal cortices with corresponding hyperintensity on fluid-attenuated inversion recovery (FLAIR) without contrast enhancement. | The follow-up CSF study revealed pleocytosis (22/μL, lymphocytes 91%), glucose of 114 mg/dl, elevated protein as 88.3 mg/dl, a positive oligoclonal IgG band. Autoimmune encephalitis. | [9] |
| Germany | 21-year-old female | First dose of the AstraZeneca ChAdOx1-S vaccine | Subacute onset of working memory impairment, impaired mental status, or psychiatric symptoms. | Emergency brain magnetic resonance imaging (MRI) was performed with normal status of the parenchyma. The extensive diagnostic workup remained negative, including chest X-ray, sonography of the abdomen, and serological examinations of serum and cerebrospinal fluid (CSF). | A lumbar puncture on the day of admission revealed lymphocytic pleocytosis of 46 leukocytes/μL. Autoimmune encephalitis. | [10] |
| 63-year-old female | First dose of the AstraZeneca ChAdOx1-S vaccine | Subacute onset of working memory impairment, impaired mental status, or psychiatric symptoms. | MRI showed normal status of the parenchyma. | An encephalitis was diagnosed due to the result of lumbar puncture showing a lymphocytic pleocytosis of 115 leukocytes/μL. Autoimmune encephalitis. | [10] | |
| 63-year-old male | AstraZeneca ChAdOx1-S vaccine | Presented with isolated aphasia. | MRI of the brain was normal; in particular, no evidence of ischemia or herpes encephalitis. | A lumbar puncture was performed showing a pleocytosis of 7 leukocytes/μL. Autoimmune encephalitis. | [10] | |
| Taiwan | Age from 42 to 74, 4 females and 6 males | Moderna COVID-19 (mRNA-1273) vaccine | Suspected stroke, transient amnesia, facial nerve palsy, weak hands and feet. | N/A | N/A | [11] |
| Israel | 48-year-old male | Second dose of Pfizer-BioNTech SARS-CoV-2 vaccine | Memory deficits and anterograde amnesia. Severe impairments in short-term memory, temporal orientation, abstraction and language skills. | Electroencephalogram and neurological exam were normal apart from a Montreal Cognitive Assessment (MoCA) score. Cranial magnetic resonance imaging (MRI) showed hyper intense signal on both medial temporal lobes (more on the left) including the parahippocampal gyrus on T2-weighted fluid-attenuated inversion recovery and diffusion-weighted imaging. | CSF cultures were negative and demonstrated normal protein and glucose without pleocytosis. | [12] |
| Qatar | 32-year-old male | Moderna COVID-19 (mRNA-1273) vaccine | Disoriented and amnesic, and onset of forgetfulness and mood disturbance within 24 h of receiving the COVID-19 vaccine dose without remembering what happened after that. | MRI of the brain did not reveal any acute or chronic abnormality. | Lumbar puncture with cerebrospinal fluid (CSF) study was performed, and it showed elevated protein levels (0.76 gm/L, reference range = 0.15–0.45) with average cell counts (white blood cells of 3 u/L) and glucose levels. Acute encephalopathy. | [13] |
| Indonesia | 44-year-old male | Sinovac vaccine | After vaccination, the patient had difficulty communicating verbally. The complaints of difficulty concentrating, and forgetting were getting worse, accompanied by incoherent speech. The patient also had cognitive deficits. The patient’s neurobehavioral status showed short-term memory impairment and impaired concentration. | Brain MRI showed chronic cortical infarct in left temporal lobe and multiple subacute lacunar infarcts in the left corona radiata, left basal ganglia and left frontal lobe. The ENMG results later showed motor and sensory polyradiculoneuropathy on the upper and lower extremities, leading to the diagnosis of chronic inflammatory demyelinating polyradiculoneuropathy (CIDP). | Secondary antiphospholipid syndrome and autoimmune dementia. | [14] |
| Taiwan | 82-year-old female | First dose of the mRNA-1273 SARS-CoV-2 vaccine (Moderna) | Memory impairment, loss of attention and concentration, murmuring, and unsteadiness. | Brain MRI revealed hyperintense signal on fluid-attenuated inversion recovery (FLAIR) sequence imaging and abnormal gyral enhancement on T1-weighted imaging in the right middle and posterior temporal lobe with no evidence of myelitis. | CSF analysis showed no pleocytosis but elevated CSF protein. CSF rapid plasma reagin (RPR), treponema pallidum hemagglutination (TPPA) immunoelectrophoresis, and cytology were negative. | [15] |
| Taiwan | 55-year-old male | First dose of the AstraZeneca ChAdOx1-S vaccine | Impaired verbal expression, progressive disorientation to people and place and slow response. | Magnetic resonance angiography of brain was showed pachymeningeal enhancement without definite abnormal signal intensity over brain parenchyma. | CSF testing showed the white cell count was 16/μL, with a neutrophil/lymphocyte/monocyte count 3/4/7, red cell count was 1/μL, the protein level was 97.3 mg/dL and positive antinuclear antibody. Serum white cell count, platelet count and C-reactive protein were within normal range. | [16] |
| China | 24-year-old female | SARS-CoV-2 vaccine (Vero cells) | Neurological examination showed somnolence, memory decline and poor memory persisted. | Initial brain MRI showed abnormal signals in the bilateral temporal cortex. | The WBC count of CSF was 51 × 106/L. CSF was negative for antibodies to major pathogens and cultures of bacteria and fungi; high-throughput genome sequencing also revealed no pathogens. | [17] |
| India | 65-year-old male | First dose of the AstraZeneca ChAdOx1-S vaccine | Cognitive deficits, memory impairments and sudden memory loss. Unable to describe both short and long-term memory previously acquired. | Non-contrast CT was essentially normal with no evidence of hemorrhage or focal lesion. | All routine blood tests were normal. | [18] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, Y.-F.; Ho, T.-C.; Chang, C.-C.; Shen, D.H.-Y.; Chan, H.-P.; Chuang, K.-P.; Tyan, Y.-C.; Yang, M.-H. A Rare Adverse Effect of the COVID-19 Vaccine on Autoimmune Encephalitis. Vaccines 2022, 10, 1114. https://doi.org/10.3390/vaccines10071114
Huang Y-F, Ho T-C, Chang C-C, Shen DH-Y, Chan H-P, Chuang K-P, Tyan Y-C, Yang M-H. A Rare Adverse Effect of the COVID-19 Vaccine on Autoimmune Encephalitis. Vaccines. 2022; 10(7):1114. https://doi.org/10.3390/vaccines10071114
Chicago/Turabian StyleHuang, Ying-Fong, Tzu-Chuan Ho, Chin-Chuan Chang, Daniel Hueng-Yuan Shen, Hung-Pin Chan, Kuo-Pin Chuang, Yu-Chang Tyan, and Ming-Hui Yang. 2022. "A Rare Adverse Effect of the COVID-19 Vaccine on Autoimmune Encephalitis" Vaccines 10, no. 7: 1114. https://doi.org/10.3390/vaccines10071114