
Juvenile Membranous Nephropathy Developed after Human Papillomavirus (HPV) Vaccination
 ,
,
Abstract
:1. Introduction
2. Case Presentation
3. Renal Biopsy and Laser-Microdissection Mass Spectrometry
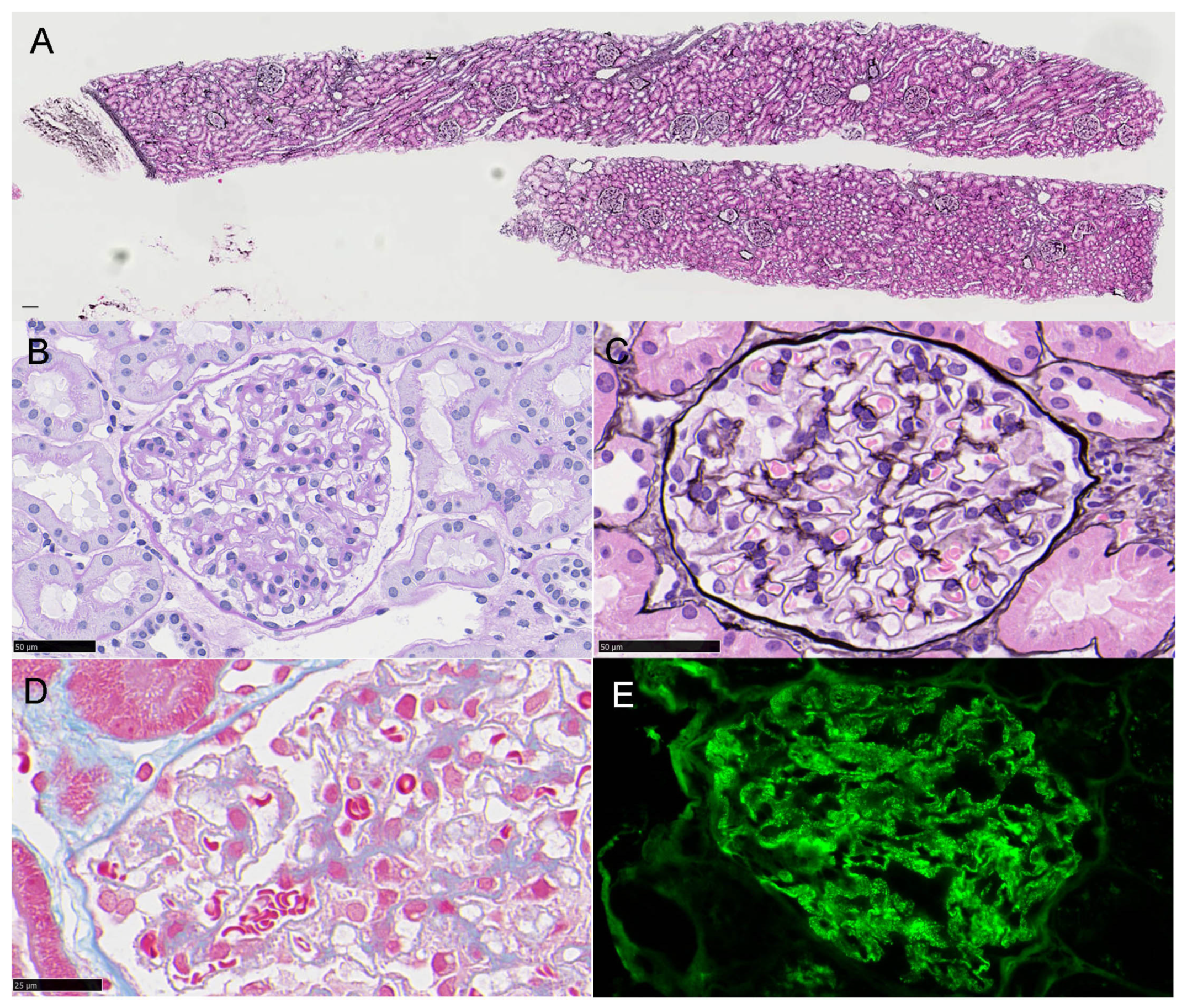
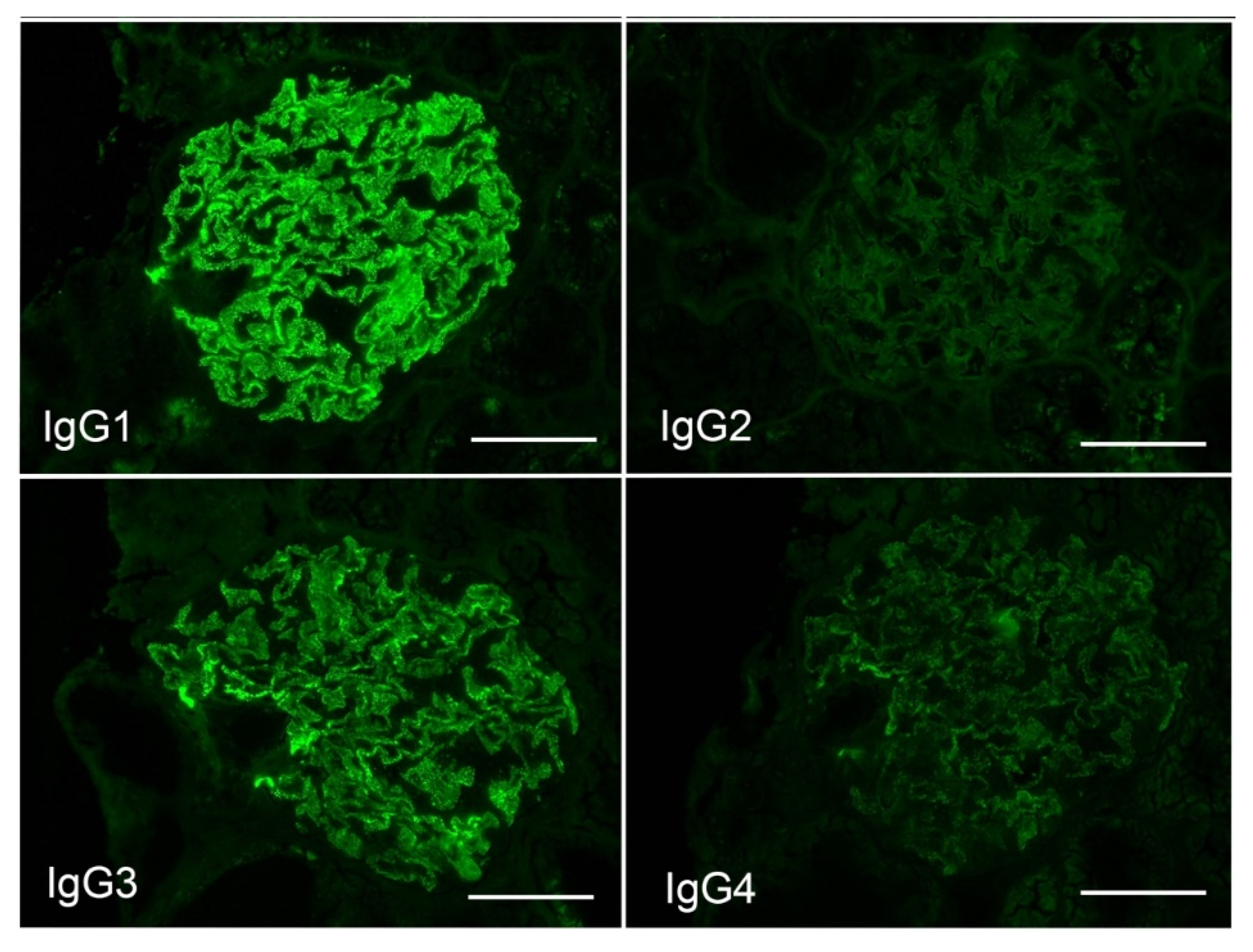
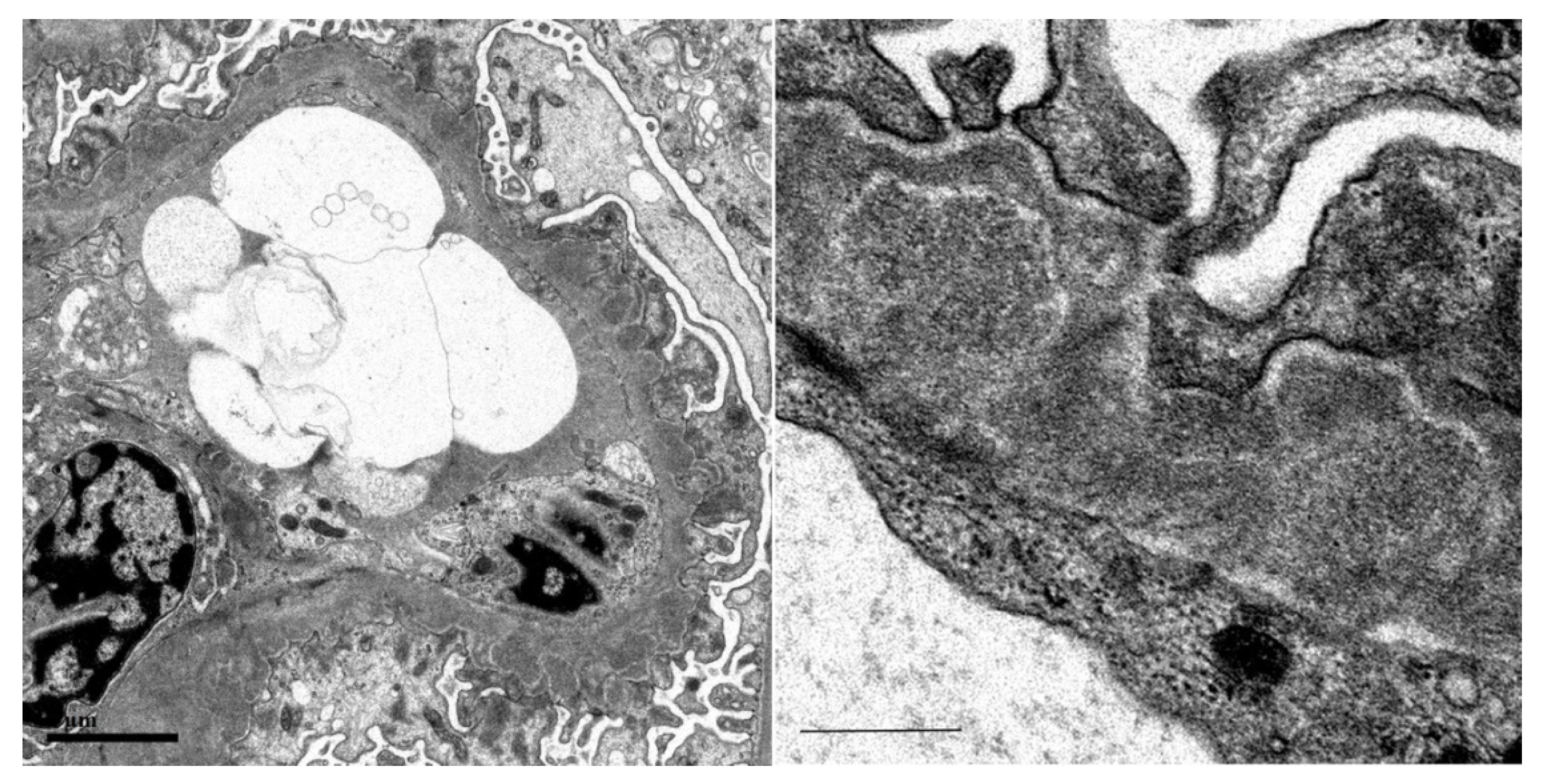
3.1. Renal Biopsy
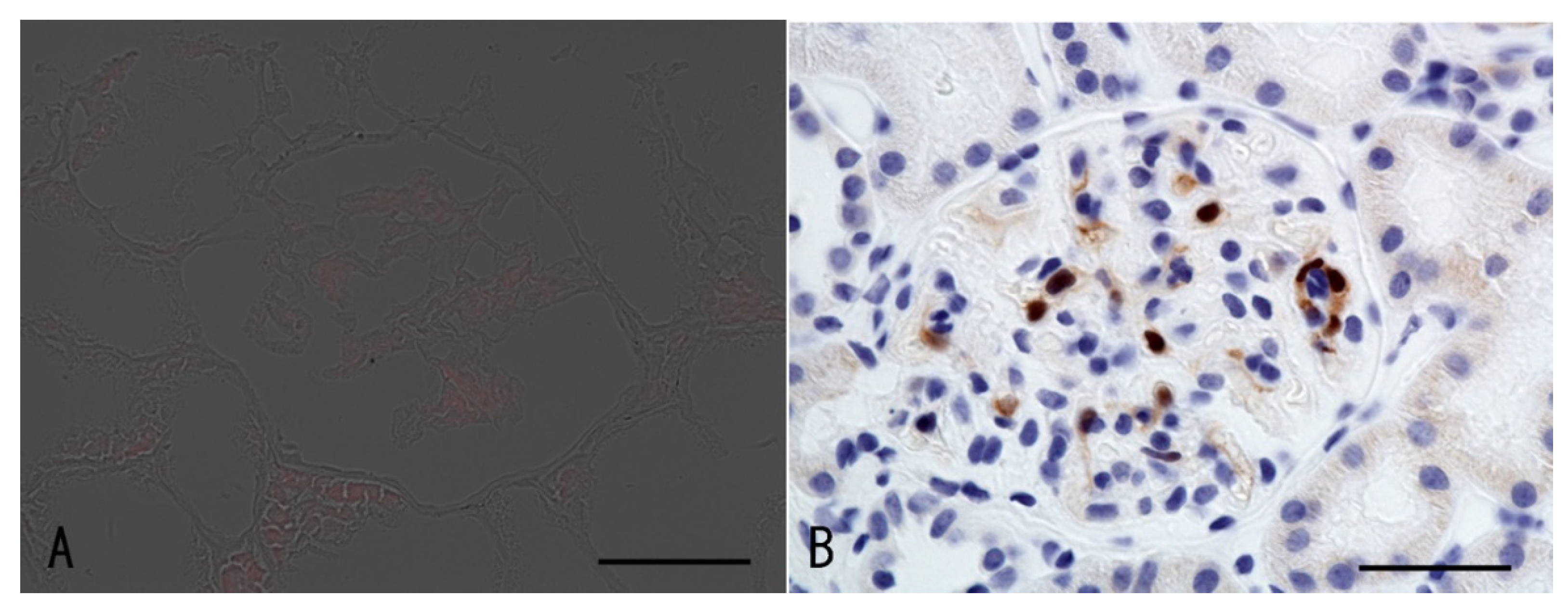
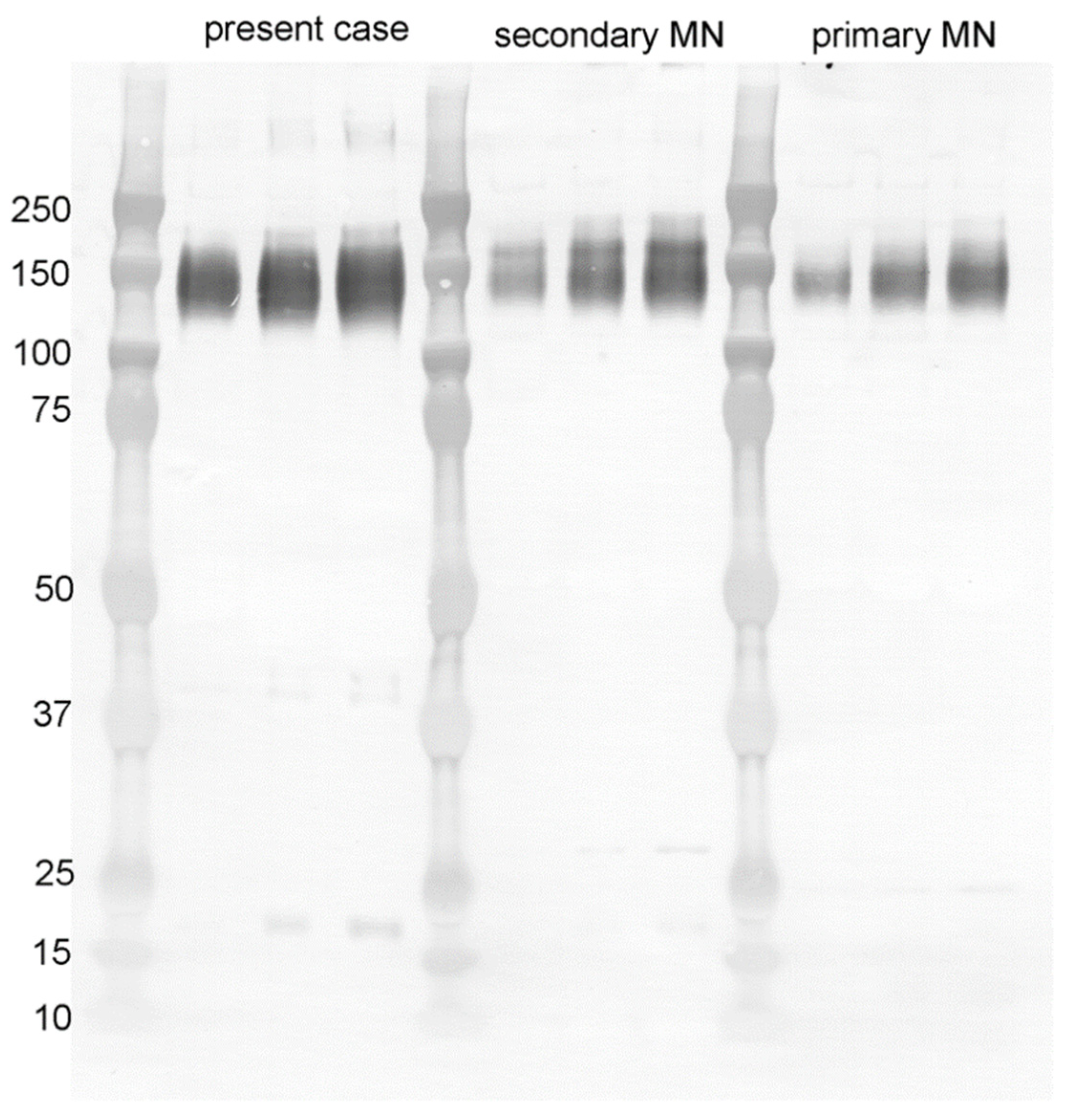
3.2. Surrogate Marker for HPV Infection
3.3. Laser Microdissection Mass Spectrometry
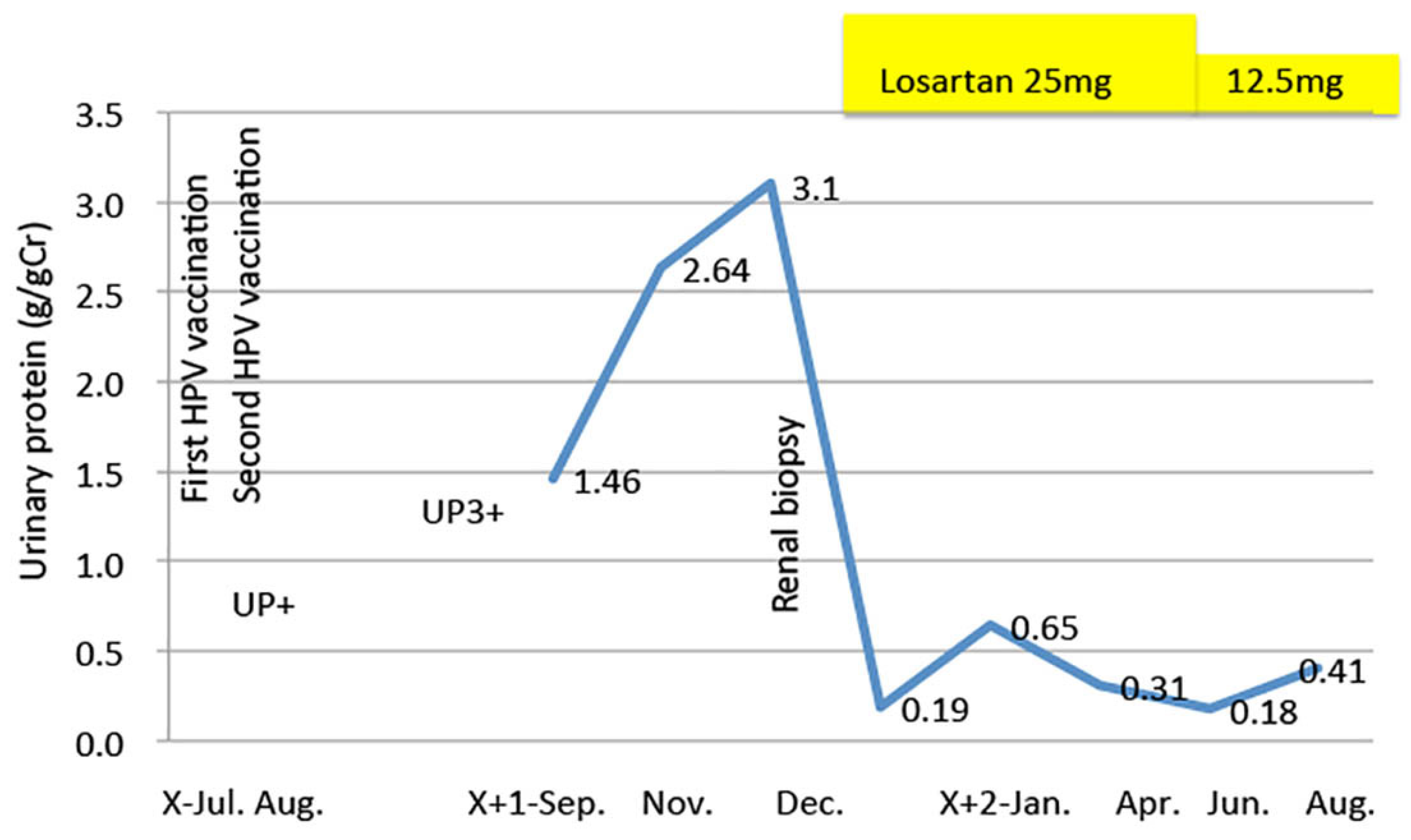
3.4. Clinical Course
4. Discussion
4.1. Characteristics of Adolescent Membranous Nephropathy
4.2. HPV Virus Infection and Kidney Disease
4.3. Kidney Disease associated with Vaccination
5. Conclusions
6. Take-Home Message and Lessons Learned
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lebedev, L.; Sapojnikov, M.; Wechsler, A.; Varadi-Levi, R.; Zamir, D.; Tobar, A.; Levin-Iaina, N.; Fytlovich, S.; Yagil, Y. Minimal Change Disease Following the Pfizer-BioNTech COVID-19 Vaccine. Am. J. Kidney Dis. 2021, 78, 142–145. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.H.; Han, M.H.; Kim, Y.J.; Kim, M.S.; Jung, H.Y.; Choi, J.Y.; Cho, J.H.; Kim, C.D.; Kim, Y.L.; Park, S.H. New-onset Nephrotic Syndrome after Janssen COVID-19 Vaccination: A Case Report and Literature Review. J. Korean Med. Sci. 2021, 36, e218. [Google Scholar] [CrossRef] [PubMed]
- Mancianti, N.; Guarnieri, A.; Tripodi, S.; Salvo, D.P.; Garosi, G. Minimal change disease following vaccination for SARS-CoV-2. J. Nephrol. 2021, 34, 1039–1040. [Google Scholar] [CrossRef] [PubMed]
- Negrea, L.; Rovin, B.H. Gross hematuria following vaccination for severe acute respiratory syndrome coronavirus 2 in 2 patients with IgA nephropathy. Kidney Int. 2021, 99, 1487. [Google Scholar] [CrossRef]
- Okuhara, T.; Ishikawa, H.; Okada, M.; Kato, M.; Kiuchi, T. Contents of Japanese pro- and anti-HPV vaccination websites: A text mining analysis. Patient Educ. Couns. 2018, 101, 406–413. [Google Scholar] [CrossRef]
- Cutts, F.T.; Franceschi, S.; Goldie, S.; Castellsague, X.; de Sanjose, S.; Garnett, G.; Edmunds, W.J.; Claeys, P.; Goldenthal, K.L.; Harper, D.M.; et al. Human papillomavirus and HPV vaccines: A review. Bull. World Health Organ. 2007, 85, 719–726. [Google Scholar] [CrossRef]
- Egawa, N.; Egawa, K.; Griffin, H.; Doorbar, J. Human Papillomaviruses; Epithelial Tropisms, and the Development of Neoplasia. Viruses 2015, 7, 3863–3890. [Google Scholar] [CrossRef]
- Onuki, M.; Matsumoto, K.; Iwata, T.; Yamamoto, K.; Aoki, Y.; Maenohara, S.; Tsuda, N.; Kamiura, S.; Takehara, K.; Horie, K.; et al. Human papillomavirus genotype contribution to cervical cancer and precancer: Implications for screening and vaccination in Japan. Cancer Sci. 2020, 111, 2546–2557. [Google Scholar] [CrossRef]
- Ikeda, S.; Ueda, Y.; Yagi, A.; Matsuzaki, S.; Kobayashi, E.; Kimura, T.; Miyagi, E.; Sekine, M.; Enomoto, T.; Kudoh, K. HPV vaccination in Japan: What is happening in Japan? Expert Rev. Vaccines 2019, 18, 323–325. [Google Scholar] [CrossRef]
- Nakayama, T. An inflammatory response is essential for the development of adaptive immunity-immunogenicity and immunotoxicity. Vaccine 2016, 34, 5815–5818. [Google Scholar] [CrossRef]
- Kashiwagi, Y.; Maeda, M.; Kawashima, H.; Nakayama, T. Inflammatory responses following intramuscular and subcutaneous immunization with aluminum-adjuvanted or non-adjuvanted vaccines. Vaccine 2014, 32, 3393–3401. [Google Scholar] [CrossRef] [PubMed]
- Carozzi, F.; Confortini, M.; Dalla Palma, P.; Del Mistro, A.; Gillio-Tos, A.; De Marco, L.; Giorgi-Rossi, P.; Pontenani, G.; Rosso, S.; Sani, C.; et al. Use of p16-INK4A overexpression to increase the specificity of human papillomavirus testing: A nested substudy of the NTCC randomised controlled trial. Lancet Oncol. 2008, 9, 937–945. [Google Scholar] [CrossRef]
- Rischin, D.; Young, R.J.; Fisher, R.; Fox, S.B.; Le, Q.T.; Peters, L.J.; Solomon, B.; Choi, J.; O’Sullivan, B.; Kenny, L.M.; et al. Prognostic significance of p16INK4A and human papillomavirus in patients with oropharyngeal cancer treated on TROG 02.02 phase III trial. J. clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2010, 28, 4142–4148. [Google Scholar] [CrossRef] [PubMed]
- Ishimitsu, A.; Tojo, A.; Hirao, J.; Yokoyama, S.; Ohira, T.; Murayama, Y.; Ishimitsu, T.; Kang, D.; Honda, K.; Ehara, T.; et al. AL-Kappa Primary Amyloidosis with Apolipoprotein A-IV Deposition. Intern. Med. 2022, 61, 871–876. [Google Scholar] [CrossRef]
- Sethi, S. New ‘Antigens’ in Membranous Nephropathy. J. Am. Soc. Nephrol. JASN 2021, 32, 268–278. [Google Scholar] [CrossRef]
- Caza, T.N.; Al-Rabadi, L.F.; Beck, L.H., Jr. How Times Have Changed! A Cornucopia of Antigens for Membranous Nephropathy. Front. Immunol. 2021, 12, 800242. [Google Scholar] [CrossRef]
- International Study of Kidney Disease in Children. Nephrotic Syndrome in Children—Prediction of Histopathology from Clinical and Laboratory Characteristics at Time of Diagnosis. Kidney Int. 1978, 13, 159–165. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, G.P.; Li, B.M.; Chen, Q.K. Clinicopathological analysis of idiopathic membranous nephropathy in young adults. Genet. Mol. Res. 2015, 14, 4541–4548. [Google Scholar] [CrossRef]
- Li, C.; Li, H.; Wen, Y.B.; Li, J.N.; Lin, W.F.; Cai, J.F.; Duan, L.; Li, Y.; Li, X.M.; Li, X.W. Clinicopathological Features of Idiopathic Membranous Nephropathy in 33 Adolescents. Zhongguo Yi Xue Ke Xue Yuan Xue Bao Acta Acad. Med. Sin. 2017, 39, 544–551. [Google Scholar]
- Dettmar, A.K.; Wiech, T.; Kemper, M.J.; Soave, A.; Rink, M.; Oh, J.; Stahl, R.A.K.; Hoxha, E. Immunohistochemical and serological characterization of membranous nephropathy in children and adolescents. Pediatric Nephrol. 2018, 33, 463–472. [Google Scholar] [CrossRef]
- Cason, J.; Kaye, J.N.; Jewers, R.J.; Kambo, P.K.; Bible, J.M.; Kell, B.; Shergill, B.; Pakarian, F.; Raju, K.S.; Best, J.M. Perinatal Infection and Persistence of Human Papillomavirus Type-16 and Type-18 in Infants. J. Med. Virol 1995, 47, 209–218. [Google Scholar] [CrossRef]
- Syrjanen, S.; Rintala, M.; Sarkola, M.; Willberg, J.; Rautava, J.; Koskimaa, H.; Paaso, A.; Syrjanen, K.; Grenman, S.; Louvanto, K. Oral Human Papillomavirus Infection in Children during the First 6 Years of Life, Finland. Emerg. Infect. Dis. 2021, 27, 759–766. [Google Scholar] [CrossRef] [PubMed]
- Farhadi, A.; Behzad-Behbahani, A.; Geramizadeh, B.; Sekawi, Z.; Rahsaz, M.; Sharifzadeh, S. High-risk human papillomavirus infection in different histological subtypes of renal cell carcinoma. J. Med. Virol. 2014, 86, 1134–1144. [Google Scholar] [CrossRef] [PubMed]
- Chkhotua, A.B.; Gabusi, E.; Altimari, A.; D’Errico, A.; Yakubovich, M.; Vienken, J.; Stefoni, S.; Chieco, P.; Yussim, A.; Grigioni, W.F. Increased expression of p16(INK4a) and p27(Kip1) cyclin-dependent kinase inhibitor genes in aging human kidney and chronic allograft nephropathy. Am. J. Kidney Dis. 2003, 41, 1303–1313. [Google Scholar] [CrossRef]
- Melk, A.; Schmidt, B.M.; Takeuchi, O.; Sawitzki, B.; Rayner, D.C.; Halloran, P.F. Expression of p16INK4a and other cell cycle regulator and senescence associated genes in aging human kidney. Kidney Int. 2004, 65, 510–520. [Google Scholar] [CrossRef] [PubMed]
- Castro-Muñoz, L.J.; Manzo-Merino, J.; Muñoz-Bello, J.O.; Olmedo-Nieva, L.; Cedro-Tanda, A.; Alfaro-Ruiz, L.A.; Hidalgo-Miranda, A.; Madrid-Marina, V.; Lizano, M. The Human Papillomavirus (HPV) E1 protein regulates the expression of cellular genes involved in immune response. Sci. Rep. 2019, 9, 13620. [Google Scholar] [CrossRef] [PubMed]
- Patel, C.; Shah, H.H. Membranous nephropathy and severe acute kidney injury following influenza vaccination. Saudi J. Kidney Dis. Transplant. Off. Publ. Saudi Cent. Organ Transplant. Saudi Arabia 2015, 26, 1289–1293. [Google Scholar]
- Işlek, I.; Cengiz, K.; Cakir, M.; Küçüködük, S. Nephrotic syndrome following hepatitis B vaccination. Pediatric Nephrol. 2000, 14, 89–90. [Google Scholar]
- Kikuchi, Y.; Imakiire, T.; Hyodo, T.; Higashi, K.; Henmi, N.; Suzuki, S.; Miura, S. Minimal change nephrotic syndrome, lymphadenopathy and hyperimmunoglobulinemia after immunization with a pneumococcal vaccine. Clin. Nephrol. 2002, 58, 68–72. [Google Scholar] [CrossRef]
- Anupama, Y.J.; Patel, R.G.N.; Vankalakunti, M. Nephrotic Syndrome Following ChAdOx1 nCoV-19 Vaccine Against SARScoV-2. Kidney Int. Rep. 2021, 6, 2248. [Google Scholar] [CrossRef]
- Kutlucan, A.; Gonen, I.; Yildizhan, E.; Aydin, Y.; Sav, T.; Yildirim, U. Can influenza H1N1 vaccination lead to the membranous glomerulonephritis? Indian J. Pathol. Microbiol. 2012, 55, 239–241. [Google Scholar] [PubMed]
- Kao, C.D.; Chen, J.T.; Lin, K.P.; Shan, D.E.; Wu, Z.A.; Liao, K.K. Guillain-Barré syndrome coexisting with pericarditis or nephrotic syndrome after influenza vaccination. Clin. Neurol. Neurosurg. 2004, 106, 136–138. [Google Scholar] [CrossRef] [PubMed]
- Kielstein, J.T.; Termühlen, L.; Sohn, J.; Kliem, V. Minimal change nephrotic syndrome in a 65-year-old patient following influenza vaccination. Clin. Nephrol. 2000, 54, 246–248. [Google Scholar] [PubMed]
- Gutiérrez, S.; Dotto, B.; Petiti, J.P.; De Paul, A.L.; Dionisio de Cabalier, M.E.; Torres, A.I.; Mukdsi, J.H. Minimal change disease following influenza vaccination and acute renal failure: Just a coincidence? Nefrol. Publ. Off. Soc. Esp. Nefrol. 2012, 32, 414–415. [Google Scholar]
- Mader, R.; Narendran, A.; Lewtas, J.; Bykerk, V.; Goodman, R.C.; Dickson, J.R.; Keystone, E.C. Systemic vasculitis following influenza vaccination--report of 3 cases and literature review. J. Rheumatol. 1993, 20, 1429–1431. [Google Scholar]
- Patel, U.; Bradley, J.R.; Hamilton, D.V. Henoch-Schonlein Purpura after Influenza Vaccination. Br. Med. J. 1988, 296, 1800. [Google Scholar] [CrossRef]
- Yanai-Berar, N.; Ben-Itzhak, O.; Gree, J.; Nakhoul, F. Influenza vaccination induced leukocytoclastic vasculitis and pauci-immune crescentic glomerulonephritis. Clin. Nephrol. 2002, 58, 220–223. [Google Scholar] [CrossRef]
- Clajus, C.; Spiegel, J.; Bröcker, V.; Chatzikyrkou, C.; Kielstein, J.T. Minimal change nephrotic syndrome in an 82 year old patient following a tetanus-diphteria-poliomyelitis-vaccination. BMC Nephrol. 2009, 10, 21. [Google Scholar] [CrossRef]
- Maas, R.J.; Gianotten, S.; van der Meijden, W.A.G. An Additional Case of Minimal Change Disease Following the Pfizer-BioNTech COVID-19 Vaccine. Am. J. Kidney Dis. 2021, 78, 312. [Google Scholar] [CrossRef]
- Gherardi, R.K.; Authier, F.J. Macrophagic myofasciitis: Characterization and pathophysiology. Lupus 2012, 21, 184–189. [Google Scholar] [CrossRef]
- Gherardi, R.K.; Coquet, M.; Cherin, P.; Authier, F.J.; Laforet, P.; Belec, L.; Figarella-Branger, D.; Mussini, J.M.; Pellissier, J.F.; Fardeau, M.; et al. Macrophagic myofasciitis: An emerging entity. Lancet 1998, 352, 347–352. [Google Scholar] [CrossRef]
- Agmon-Levin, N.; Paz, Z.; Israeli, E.; Shoenfeld, Y. Vaccines and autoimmunity. Nat. Rev. Rheumatol. 2009, 5, 648–652. [Google Scholar] [CrossRef] [PubMed]
- Shoenfeld, Y.; Agmon-Levin, N. ‘ASIA’—Autoimmune/inflammatory syndrome induced by adjuvants. J. Autoimmun. 2011, 36, 4–8. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MS/MS View: 899 Proteins in 665 Clusters | Alternate ID | Control | Pt. Glm1 | Pt. Glm2 | Pt. Glm3 | Pt. Glm4 | Pt. Mean | Fold (Pt./Control) |
|---|---|---|---|---|---|---|---|---|
| Increased proteins | ||||||||
| Desmoplakin | SDP | 1 | 198 | 224 | 201 | 331 | 239 | 238.5 |
| Keratin, type I cytoskeletal 24 | KRT24 | 26 | 173 | 169 | 182 | 176 | 175 | 6.7 |
| Keratin, type II cytoskeletal 78 | KRT78 | 26 | 154 | 146 | 143 | 109 | 138 | 5.3 |
| Junction plakoglobin | JUP | nd | 93 | 95 | 97 | 121 | 102 | ∞ |
| luster of Keratin, type II cytoskeletal 73 | KRT73 | 8 | 89 | 80 | 90 | 62 | 80 | 10.0 |
| Hornerin | HRNR | nd | 43 | 53 | 55 | 101 | 63 | ∞ |
| Keratin, type I cytoskeletal 23 | KRT23 | nd | 57 | 59 | 50 | 50 | 54 | ∞ |
| Desmoglein-1 | DSG1 | 0 | 48 | 49 | 43 | 70 | 53 | ∞ |
| Calmodulin-like protein 5 | CALML5 | nd | 42 | 43 | 39 | 45 | 42 | ∞ |
| Fatty acid-binding protein 5 | FABP5 | nd | 42 | 43 | 39 | 45 | 42 | ∞ |
| Galectin-7 | LGALS7 | nd | 20 | 18 | 22 | 34 | 24 | ∞ |
| Cystatin-A | CSTA | nd | 17 | 22 | 18 | 25 | 21 | ∞ |
| Plakophilin-1 | PKP1 | 1 | 15 | 18 | 21 | 36 | 23 | 22.5 |
| Serpin B12 | SERPIN | nd | 15 | 19 | 12 | 27 | 18 | ∞ |
| Protein-glutamine gamma-glutamyltransferase E | TGM3 | nd | 12 | 14 | 9 | 24 | 15 | ∞ |
| Filaggrin-2 | FLG2 | 1 | 10 | 12 | 6 | 18 | 12 | 11.5 |
| Arginase-1 | ARG1 | nd | 7 | 9 | 9 | 15 | 10 | ∞ |
| Complement C3 | C3 | 3 | 48 | 55 | 64 | 108 | 69 | 22.9 |
| Cluster of Keratin, type II cytoskeletal 6A | KRT6A | 236 | 2584 | 2466 | 2588 | 3111 | 2687 | 11.4 |
| Cluster of Keratin, type I cytoskeletal 16 | KRT16 | 158 | 2548 | 2420 | 2509 | 2754 | 2558 | 16.2 |
| Keratin, type II cytoskeletal 1 | KRT1 | 403 | 2078 | 1946 | 2049 | 2205 | 2070 | 5.1 |
| Keratin, type I cytoskeletal 9 | KRT9 | 311 | 1395 | 1269 | 1324 | 1416 | 1351 | 4.3 |
| Deceased proteins | ||||||||
| Cluster of Vimentin | VIM | 622 | 233 | 239 | 220 | 257 | 237 | 0.4 |
| Cluster of Actin, cytoplasmic 2 | ACTG1 | 500 | 249 | 230 | 234 | 227 | 235 | 0.5 |
| Cluster of Alpha-actinin-4 | ACTN4 | 264 | 84 | 92 | 80 | 153 | 102 | 0.4 |
| Myosin-9 | MYH9 | 213 | 78 | 85 | 93 | 185 | 110 | 0.5 |
| Cluster of Tubulin beta chain | TUBB | 103 | 36 | 36 | 34 | 59 | 41 | 0.4 |
| Laminin subunit alpha-5 | LAMA5 | 77 | 25 | 30 | 31 | 54 | 35 | 0.5 |
| Cluster of Histone H2B type 1-M | H2BC14 | 101 | 47 | 40 | 46 | 61 | 49 | 0.5 |
| basement membrane-specific heparan sulfate proteoglycan core pr. | HSPG2 | 26 | 13 | 14 | 11 | 46 | 21 | 0.8 |
| Vinculin | VCL | 51 | 13 | 13 | 15 | 40 | 20 | 0.4 |
| Podocin | NPHS2 | 14 | 7 | 2 | 3 | 7 | 5 | 0.3 |
| Podocalyxin | PODXL | 9 | 5 | 4 | 4 | 8 | 5 | 0.6 |
| Membranous nephropathy antigens | ||||||||
| Secretory phospholipase A2 receptor | PLA2R1 | nd | nd | 0 | nd | 5 | 1 | |
| Thrombospondin-type -1 domain-containing 7A | THSD7A | nd | nd | nd | nd | nd | nd | |
| Exostosin 1 and exostosin 2 | EXT1/2 | nd | nd | nd | nd | nd | nd | |
| Protein kinase C-binding protein NELL1 | NELL1 | nd | nd | nd | nd | 1 | 0.25 | |
| Semaphorin 3b | Sema 3B | nd | nd | nd | nd | nd | nd | |
| Protocadherin 7 | PCDH7 | nd | nd | nd | nd | nd | nd | |
| Human high-temperature requirement A1 | HTRA1 | nd | nd | nd | nd | nd | nd | |
| Contactin 1 | nd | nd | nd | nd | nd | nd |
| Reference | Age Sex | Vaccine | Onset after Injection | Proteinuria | Renal Function | Renal Biopsy | Treatment | Prognosis |
|---|---|---|---|---|---|---|---|---|
| Patel [27] | 60 F | Influenza | 2 weeks | 20.5 g/day | AKI | MN stage 1, AIN | HD, PSL | CR with relapse |
| Kutlucan [31] | 56 M | Influenza | 20 days | 7.3 g/day | Cr 1.2 mg/dL | MN IgG, C3 | PSL1 mg/kg | CR |
| Kao [32] | 72 M | Influenza | <2 weeks | 5.7 g/day | ND | ND | mPSL pulse PEX | GBS UP decreased after 10 M |
| Kielstein [33] | 65 F | Influenza | 4 days | 10.8 g/day | Ccr 65 mL/min | MCNS | Conservative | CR |
| Gutiérrez [34] | 44 M | Influenza | 18 days | 4 g/day | Cr 4.4 mg/dL | MCNS | PSL60 mg | CR |
| Mader [35] | 86 F | Influenza | HSP | CR | ||||
| Patel [36] | 77 M | Influenza | 10 days | ND | Cr2.31 mg/dL | Mesangial proliferative GN, HSP | PSL60 mg | CR |
| Yanai-Berar [37] | 63 M | Influenza | 11 days | 1.5 g/day | Cr 1.8 mg/dL | Pauci-immune crescentic GN | PSL60 mg | CR |
| Islek [28] | 4 M | HBV | 8 days | 2 g/m2/day | ND | ND | PSL | CR |
| Kikuchi [29] | 67 F | Polyvalent pneumococcal polysaccharide | 1 week | 10.4 g/day | Cr 1.33 mg/dL | MCNS with TIN | mPSL pulse | CR |
| Claujus [38] | 82 F | Tetanus–diphtheria–poliomyelitis | 6 weeks | 12 g/day | Cr 0.84 mg/dL | MCNS | PSL75 mg | CR |
| Anupama [30] | 19 F | hAdOx1 nCoV-19 | 8 days | 3.18 g/gCr | Cr1.09 mg/dL | MCNS | PSL1 mg/kg | CR |
| Lebedev [1] | 50 M | BNT162b2 COVID-19 | 10 days | 6.9 g/day | Cr 2.31 mg/dL | MCNS AIN | PSL | CR |
| Maas [39] | 80 M | BNT162b2 COVID-19 | 7 days | 15.3 g/gCr | Cr 1.43 mg/dL | MCNS | PSL80 mg | PR1 |
| Present case | 16 F | HPV | 5 days | 1.46 g/gCr | Cr 0.47 mg/dL | MN | ARB | PR1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arakawa, H.; Yokoyama, S.; Ohira, T.; Kang, D.; Honda, K.; Ueda, Y.; Tojo, A. Juvenile Membranous Nephropathy Developed after Human Papillomavirus (HPV) Vaccination. Vaccines 2022, 10, 1442. https://doi.org/10.3390/vaccines10091442
Arakawa H, Yokoyama S, Ohira T, Kang D, Honda K, Ueda Y, Tojo A. Juvenile Membranous Nephropathy Developed after Human Papillomavirus (HPV) Vaccination. Vaccines. 2022; 10(9):1442. https://doi.org/10.3390/vaccines10091442
Chicago/Turabian StyleArakawa, Haruna, Shohei Yokoyama, Takehiro Ohira, Dedong Kang, Kazuho Honda, Yoshihiko Ueda, and Akihiro Tojo. 2022. "Juvenile Membranous Nephropathy Developed after Human Papillomavirus (HPV) Vaccination" Vaccines 10, no. 9: 1442. https://doi.org/10.3390/vaccines10091442