
HPV-Vaccine Hesitancy in Colombia: A Mixed-Methods Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
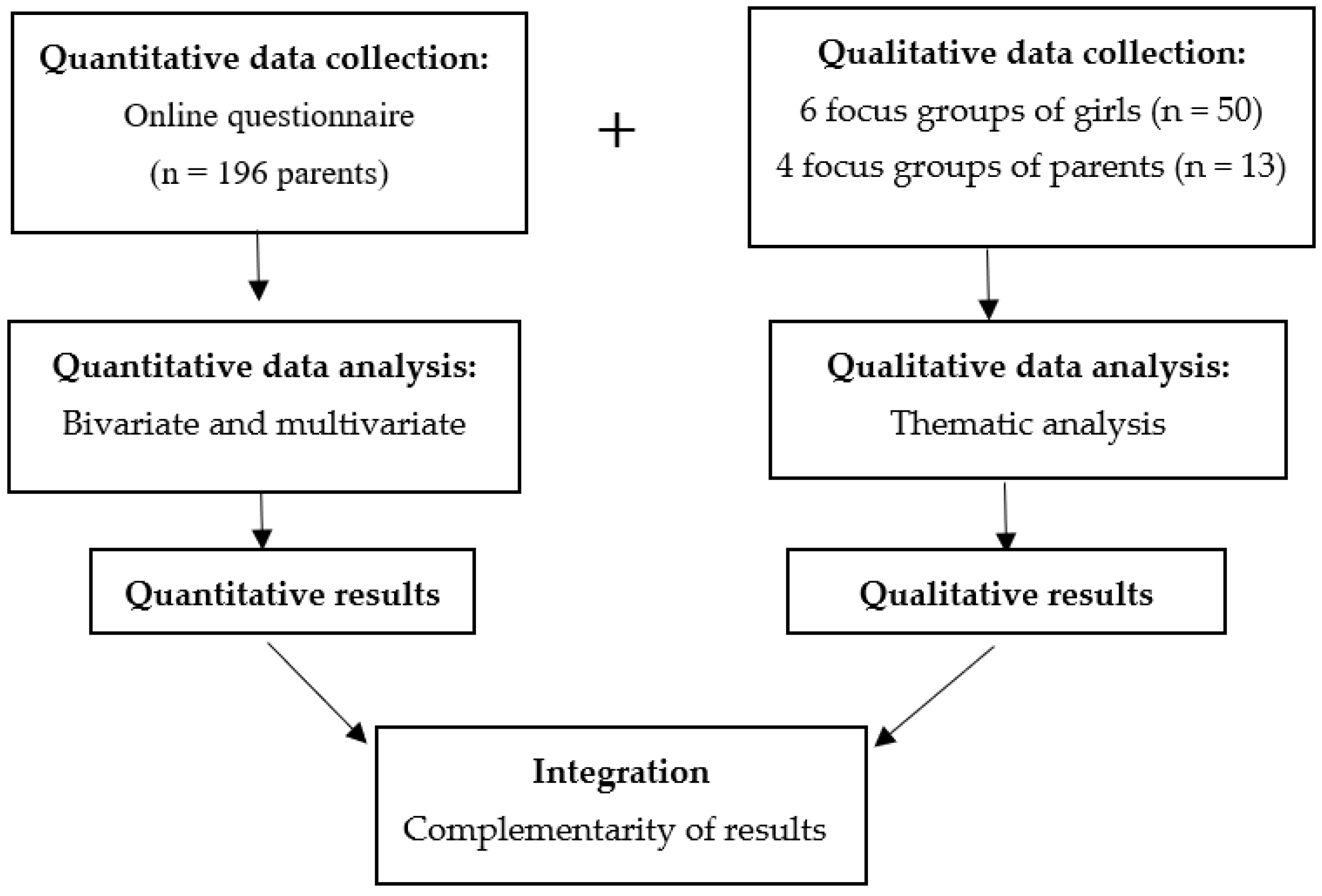
2.1. Study Design
2.2. Setting
2.3. Study Model
2.4. Participants
2.5. Study Measures
2.6. Procedure
2.7. Ethics
2.8. Data Analysis
3. Results
3.1. Description of the Sample
3.2. Analysis Based on the COM-B Model
3.2.1. Capability
Lack of Information
“I think that there has been a need for an education campaign, that is, promulgation of what papilloma is and what the vaccine does, because normally when a vaccine is talked about repeatedly by many media and people get educated, people have more awareness and then they do it conscientiously, but I have not heard that there has been much of a campaign or education on the subject”.(mother of unvaccinated girl, 51 years old, private school)
“I was diagnosed with HPV 10 or 12 years ago (…) they explained to me that even the nuns get it [HPV], even if they haven’t had sex. I am in this meeting because I have many gaps [in my knowledge] and ignorance on the subject”.(mother of unvaccinated girl, 45 years old, private school)
Relationship between HPV and Cervical Cancer
3.2.2. Opportunity
Trust in Traditional Institutions
“I wanted to say that my ignorance is even bigger because my children were born in Ecuador and there nobody talks about HPV (…). I was one of those mothers who said that I would not give my daughter that vaccine, until recently, when I went to get a booster for my other 10-year-old son and I spoke with a doctor who explained to me that it was absolutely safe, so I began to think differently”.(mother of unvaccinated girl, 45 years old, private school)
3.2.3. Motivation
The Vaccine as an Act of Care
“It is a matter of avoiding the disease; one does not know when it could happen, God willing it does not happen, but it is a way of caring for and protecting them”.(mother of girl with one dose, 41 years old, private school)
“I have heard many mothers who did not want to vaccinate their daughters; I do not know why. A long time ago there was a problem with some vaccine, after which many mothers believe in these things, and they are scared to vaccinate their daughters”.(mother of unvaccinated girl, 43 years old, private school)
Respect for the Personal Decision to Be Vaccinated
“I never had the power to decide if I wanted to get vaccinated or not; it was not a subject that I could get into”.(Girl, one dose, 15 years old, public rural school)
Association of HPV with Sexuality
“I consider that in the subject of the infection with the human papilloma virus, it is possible to take a look from the biological point of view as the subject of the disease; let’s say that it is detached from the subject of sexuality and that is perfectly well because one can approach the subject with one’s daughter like that”.(Father of girl with one dose, 53 years old, private school)
3.2.4. The Impact of COVID-19 on HPV Hesitancy
“I don’t know exactly how the virus spreads, but I suppose that, like a normal virus, like when you get vaccinated against the coronavirus, you prevent yourself and others, that you don’t spread it, nor are you infected”.(girl with one dose, 15 years old, public school)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Online Questionnaire
- Do you think your daughter may get cervical cancer at some point in her life? Yes/No
- Do you think your daughter could get HPV? Yes/No
- Have you heard of the HPV vaccine? Yes/No
- Has anyone told you that your daughter needs to be vaccinated against HPV? Yes/No
- Is your daughter going to complete the vaccination schedule? Yes/No
- How concerned are you that your daughter might have a serious side effect from a shot?
- How concerned are you that anyone of the childhood shots might not be safe?
- How concerned are you that a shot might not prevent the disease?
- “If a vaccine against HPV was available for your daughter, how likely is it that she would have it?” 0 (Extremely likely) to 3 (Not at all likely).
- Cost
- Ease
- Knowing that other people have put it on
- Doctor’s recommendation
- Someone else’s recommendation
- Knowing that the vaccine is safe
- Thinking that my daughter is at higher risk for HPV
- Listening to positive opinions about the vaccine.
References
- Bruni, L.; Albero, G.; Serrano, B.; Mena, M.; Collado, J.J.; Gómez, D.; Muñoz, J.; Bosch, X.; de Sanjosé, S. Human Papillomavirus and Related Diseases Report WORLD; Barcelona, Spain, 2021; Available online: https://hpvcentre.net/statistics/reports/XWX.pdf (accessed on 4 June 2022).
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bruni, L.; Albero, G.; Serrano, B.; Mena, M.; Collado, J.J.; Gómez, D.; Muñoz, J.; Bosch, X.; de Sanjosé, S. Human Papillomavirus and Related Diseases Report COLOMBIA; Barcelona, Spain, 2021; Available online: https://hpvcentre.net/statistics/reports/COL.pdf?t=1624248056406 (accessed on 4 June 2022).
- IARC [International Agency for Cancer Research]. Colombia Facts Sheet; UNHCR: Geneva, Switzerland, 2020. [Google Scholar]
- Hernández Vargas, J.A.; Ramírez Barbosa, P.X.; Gil Quijano, A.M.; Valbuena, A.M.; Acuña, L.; González, J.A. Patterns of breast, prostate and cervical cancer incidence and mortality in Colombia: An administrative registry data analysis. BMC Cancer 2020, 20, 1097. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, N.; Bravo, L.E. Epidemiology of cervical cancer in Colombia. Colomb. Med. 2012, 43, 298–304. [Google Scholar] [CrossRef] [Green Version]
- Walboomers, J.M.M.; Jacobs, M.V.; Manos, M.M.; Bosch, F.X.; Kummer, J.A.; Shah, K.V.; Snijders, P.J.F.; Peto, J.; Meijer, C.J.L.M.; Muñoz, N. Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J. Pathol. 1999, 189, 12–19. [Google Scholar] [CrossRef]
- Muñoz, N.; Bosch, F.X.; de Sanjosé, S.; Herrero, R.; Castellsagué, X.; Shah, K.V.; Snijders, P.J.F.; Meijer, C.J.L.M. Epidemiologic classification of human papillomavirus types associated with cervical cancer. N. Engl. J. Med. 2003, 348, 518–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jones, B.A.; Davey, D.D. Quality management in gynecologic cytology using interlaboratory comparison. Arch. Pathol. Lab. Med. 2000, 124, 672–681. [Google Scholar] [CrossRef]
- De Rijke, J.M.; Van der Putten, H.W.H.M.; Lutgens, L.C.H.W.; Voogd, A.C.; Kruitwagen, R.F.P.M.; Van Dijck, J.A.A.M.; Schouten, L.J. Age-specific differences in treatment and survival of patients with cervical cancer in the southeast of The Netherlands, 1986–1996. Eur. J. Cancer 2002, 38, 2041–2047. [Google Scholar] [CrossRef]
- Smith, M.A.; Liu, B.; McIntyre, P.; Menzies, R.; Dey, A.; Canfell, K. Fall in genital warts diagnoses in the general and indigenous Australian population following implementation of a national human papillomavirus vaccination program: Analysis of routinely collected national hospital data. J. Infect. Dis. 2015, 211, 91–99. [Google Scholar] [CrossRef] [Green Version]
- Robertson, G.; Robson, S.J. Excisional Treatment of Cervical Dysplasia in Australia 2004–2013: A Population-Based Study. J. Oncol. 2016, 2016, 3056407. [Google Scholar] [CrossRef] [Green Version]
- Australian Institute of Health and Welfare. Cervical Screening in Australia 2014–2015; Australian Institute of Health and Welfare: Canberra, Australia, 2017.
- Goldie, S.J.; Kohli, M.; Grima, D.; Weinstein, M.C.; Wright, T.C.; Xavier Bosch, F.; Franco, E. Projected clinical benefits and cost-effectiveness of a human papillomavirus 16/18 vaccine. J. Natl. Cancer Inst. 2004, 96, 604–615. [Google Scholar] [CrossRef] [Green Version]
- Watson, M.; Benard, V.; Flagg, E.W. Assessment of trends in cervical cancer screening rates using healthcare claims data: United States, 2003–2014. Prev. Med. Rep. 2018, 9, 124–130. [Google Scholar] [CrossRef] [PubMed]
- U.S. Cancer Statistics Working Group. U.S. Cancer Statistics Data Visualizations Tool. The Centers for Disease Control and Prevention (CDC) and the National Cancer Institute (NCI); 2016. Available online: https://www.cdc.gov/cancer/uscs/dataviz/index.htm (accessed on 24 March 2022).
- Quinn, M.; Babb, P.; Jones, J.; Allen, E. Effect of screening on incidence of and mortality from cancer of cervix in England: Evaluation based on routinely collected statistics. BMJ 1999, 318, 904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arbyn, M.; Xu, L.; Simoens, C.; Martin-Hirsch, P.P.L. Prophylactic vaccination against human papillomaviruses to prevent cervical cancer and its precursors. Cochrane Database Syst. Rev. 2018, 5, 1. [Google Scholar] [CrossRef] [PubMed]
- Arbyn, M.; Ronco, G.; Anttila, A.; Chris, C.J.L.; Poljak, M.; Ogilvie, G.; Koliopoulos, G.; Naucler, P.; Sankaranarayanan, R.; Peto, J. Evidence regarding human papillomavirus testing in secondary prevention of cervical cancer. Vaccine 2012, 30 (Suppl. S5), F88–F99. [Google Scholar] [CrossRef]
- Ronco, G.; Dillner, J.; Elfström, K.M.; Tunesi, S.; Snijders, P.J.F.; Arbyn, M.; Kitchener, H.; Segnan, N.; Gilham, C.; Giorgi-Rossi, P.; et al. Efficacy of HPV-based screening for prevention of invasive cervical cancer: Follow-up of four European randomised controlled trials. Lancet 2014, 383, 524–532. [Google Scholar] [CrossRef]
- Machalek, D.A.; Garland, S.M.; Brotherton, J.M.L.; Bateson, D.; McNamee, K.; Stewart, M.; Rachel Skinner, S.; Liu, B.; Cornall, A.M.; Kaldor, J.M.; et al. Very Low Prevalence of Vaccine Human Papillomavirus Types Among 18- to 35-Year Old Australian Women 9 Years Following Implementation of Vaccination. J. Infect. Dis. 2018, 217, 1590–1600. [Google Scholar] [CrossRef]
- Chesson, H.W.; Mayaud, P.; Aral, S.O. Sexually Transmitted Infections: Impact and Cost-Effectiveness of Prevention. In Disease Control Priorities, Third Edition: Major Infectious Diseases; World Bank: Washington DC, USA, 2017; Volume 6, pp. 203–232. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Strategy to Accelerate the Elimination of Cervical Cancer as a Public Health Problem; WHO: Geneva, Switzerland, 2020.
- OMS [Organización Mundial de la Salud]. Por un Futuro sin Cáncer del Cuello Uterino: Por Primera vez el Mundo se ha Comprometido a Eliminar un Cáncer—OPS/OMS|Organización Panamericana de la Salud. 2020. Available online: https://www.who.int/es/news/item/17-11-2020-a-cervical-cancer-free-future-first-ever-global-commitment-to-eliminate-a-cancer (accessed on 1 December 2021).
- Ministerio de Salud y Protección Social República de Colombia. Colombia Cuenta con las Mejores Coberturas de Vacunación Contra VPH del Mundo 2014. Available online: https://www.minsalud.gov.co/Paginas/Colombia-cuenta-con-las-mejores-coberturas-de-vacunacion.aspx (accessed on 2 December 2021).
- Simas, C.; Munoz, N.; Arregoces, L.; Larson, H.J. HPV vaccine confidence and cases of mass psychogenic illness following immunization in Carmen de Bolivar, Colombia. Hum. Vaccines Immunother. 2019, 15, 163–166. [Google Scholar] [CrossRef]
- Martinez, M.; Estevez, A.; Quijada, H.; Walteros, D.; Tolosa, N.; Paredes, A.; Alvarez, C.; Armenta, A.; Osorio, L.; Castillo, O.; et al. Brote de evento de etiología desconocida en el municipio de El Carmen de Bolívar, Bolívar, 2014. Inf. Quinc. Epidemiol. Nac. 2015, 20, 41–76. [Google Scholar]
- Silva Numa, S. ¿Quién salvará la vacunación contra el VPH en Colombia? El Espectador, 16 December 2021. [Google Scholar]
- Suppli, C.H.; Hansen, N.D.; Rasmussen, M.; Valentiner-Branth, P.; Krause, T.G.; Mølbak, K. Decline in HPV-vaccination uptake in Denmark—The association between HPV-related media coverage and HPV-vaccination. BMC Public Health 2018, 18, 1360. [Google Scholar] [CrossRef]
- Baandrup, L.; Valentiner-Branth, P.; Kjaer, S.K. HPV vaccination crisis and recovery: The Danish case. HPV World Newsl. 2021, 1–5. Available online: https://www.hpvworld.com/articles/hpv-vaccination-crisis-and-recovery-the-danish-case (accessed on 4 June 2022).
- Haruyama, R.; Obara, H.; Fujita, N. What is the current status of Japan’s efforts to meet global goals and targets to eliminate cervical cancer? Glob. Health Med. 2021, 3, 44. [Google Scholar] [CrossRef]
- Paul, K.T. “Saving lives”: Adapting and adopting Human Papilloma Virus (HPV) vaccination in Austria. Soc. Sci. Med. 2016, 153, 193–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Notejane, M.; Zunino, C.; Aguirre, D.; Méndez, P.; García, L.; Pérez, W.; Notejane, M.; Zunino, C.; Aguirre, D.; Méndez, P.; et al. Estado vacunal y motivos de no vacunación contra el virus del papiloma humano en adolescentes admitidas en el Hospital Pediátrico del Centro Hospitalario Pereira Rossell. Rev. Méd. Urug. 2018, 34, 10–28. [Google Scholar] [CrossRef]
- Cordoba-Sanchez, V.; Tovar-Aguirre, O.L.; Franco, S.; Arias Ortiz, N.E.; Louie, K.; Sanchez, G.I.; Garces-Palacio, I.C. Perception about barriers and facilitators of the school-based HPV vaccine program of Manizales, Colombia: A qualitative study in school-enrolled girls and their parents. Prev. Med. Rep. 2019, 16, 100977. [Google Scholar] [CrossRef] [PubMed]
- Patel, P.R.; Berenson, A.B. Sources of HPV vaccine hesitancy in parents. Hum. Vaccines Immunother. 2013, 9, 2649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shapiro, G.K.; Head, K.J.; Rosberger, Z.; Zimet, G.D. Parents hesitancy about HPV vaccination. HPV World 2018, 72, 1–4. [Google Scholar]
- Michie, S.; van Stralen, M.M.; West, R. The behaviour change wheel: A new method for characterising and designing behaviour change interventions. Implement. Sci. 2011, 6, 42. [Google Scholar] [CrossRef] [Green Version]
- Czajkowski, S.M.; Powell, L.H.; Adler, N.; Naar-King, S.; Reynolds, K.D.; Hunter, C.M.; Laraia, B.; Olster, D.H.; Perna, F.M.; Peterson, J.C.; et al. From ideas to efficacy: The ORBIT model for developing behavioral treatments for chronic diseases. Health Psychol. 2015, 34, 971–982. [Google Scholar] [CrossRef]
- Secretaría de Educación de Medellín. 66.8% de las Instituciones Públicas de Medellín ya Aplican la Alternancia ⋆ Secretaría de Educación 2021. Available online: https://www.medellin.edu.co/66-8-de-las-instituciones-publicas-de-medellin-ya-aplican-la-alternancia/ (accessed on 6 January 2022).
- Ministerio de Salud y Protección Social República de Colombia. Vacuna Contra el Cáncer de Cuello Uterino n.d. Available online: https://www.minsalud.gov.co/salud/publica/Vacunacion/Paginas/ABC-de-la-vacuna-contra-el-cancer-cuello-uterino.aspx (accessed on 6 January 2022).
- Vallis, M.; Bacon, S.; Corace, K.; Joyal-Desmarais, K.; Gorin, S.S.; Paduano, S.; Presseau, J.; Rash, J.; Yohannes, A.M.; Lavoie, K. Ending the Pandemic: How Behavioural Science Can Help Optimize Global COVID-19 Vaccine Uptake. Vaccines 2021, 10, 7. [Google Scholar] [CrossRef]
- Winkinson, S. Using focus groups. Exploring the meanings of health and illness. In A Handbook of Reseach Methods for Clinical and Health Psychology; Miles, J., Gilbert, P., Eds.; Oxford University Press: New York, NY, USA, 2005; pp. 79–94. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- McCrudden, M.T.; Marchand, G.; Schutz, P.A. Joint displays for mixed methods research in psychology. Methods Psychol. 2021, 5, 100067. [Google Scholar] [CrossRef]
- Bruni, L.; Saura-Lázaro, A.; Montoliu, A.; Brotons, M.; Alemany, L.; Diallo, M.S.; Afsar, O.Z.; LaMontagne, D.S.; Mosina, L.; Contreras, M.; et al. HPV vaccination introduction worldwide and WHO and UNICEF estimates of national HPV immunization coverage 2010–2019. Prev. Med. 2021, 144, 106399. [Google Scholar] [CrossRef] [PubMed]
- Habersaat, K.B.; Jackson, C. Understanding vaccine acceptance and demand-and ways to increase them. Bundesgesundheitsblatt Gesundh. Gesundh. 2020, 63, 32–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ling, W.Y.; Razali, S.M.; Ren, C.K.; Omar, S.Z. Does the success of a school-based HPV vaccine programme depend on teachers’ knowledge and religion?—A survey in a multicultural society. Asian Pac. J. Cancer Prev. 2012, 13, 4651–4654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nwanodi, O.; Salisbury, H.; Bay, C. Multimodal Counseling Interventions: Effect on Human Papilloma Virus Vaccination Acceptance. Healthcare 2017, 5, 85S. [Google Scholar] [CrossRef]
- Paskett, E.D.; Krok-Schoen, J.L.; Pennell, M.L.; Tatum, C.M.; Reiter, P.L.; Peng, J.; Bernardo, B.M.; Weier, R.C.; Richardson, M.S.; Katz, M.L. Results of a Multilevel Intervention Trial to Increase Human Papillomavirus (HPV) Vaccine Uptake among Adolescent Girls. Cancer Epidemiol. Biomark. Prev. 2016, 25, 593–602. [Google Scholar] [CrossRef] [Green Version]
- WHO; HPV Vaccine Communication. Special Considerations for a Unique Vaccine. Who/Ivb/1312 2013:31–2. Available online: https://www.who.int/publications/i/item/10665250279 (accessed on 2 December 2021).
- McNally, V.V.; Bernstein, H.H. The Effect of the COVID-19 Pandemic on Childhood Immunizations: Ways to Strengthen Routine Vaccination. Pediatr. Ann. 2020, 49, e516–e522. [Google Scholar] [CrossRef]
- Gallagher, K.E.; Howard, N.; Kabakama, S.; Mounier-Jack, S.; Griffiths, U.K.; Feletto, M.; Burchett, H.E.D.; LaMontagne, D.S.; Watson-Jones, D. Lessons learnt from human papillomavirus (HPV) vaccination in 45 low- and middle-income countries. PLoS ONE 2017, 12, e0177773. [Google Scholar] [CrossRef] [Green Version]
- Da Silva, P.M.C.; Silva, I.M.B.; da Conceição Souza Interaminense, I.N.; Linhares, F.M.P.; Serrano, S.Q.; Pontes, C.M. Knowledge and attitudes about human papillomavirus and vaccination. Esc. Anna Nery 2018, 22, 2018. [Google Scholar] [CrossRef] [Green Version]
- Hendaus, M.A.; Hassan, M.; Alsulaiti, M.; Mohamed, T.; Mohamed, R.; Yasrab, D.; Mahjoob, H.; Alhammadi, A.H. Parents attitudes toward the human papilloma virus (HPV) vaccine: A new concept in the State of Qatar. J. Fam. Med. Prim. Care 2021, 10, 2488. [Google Scholar] [CrossRef]
- Dolan, P.; Hallsworth, M.; Halpern, D.; King, D.; Metcalfe, R.; Vlaev, I. Influencing behaviour: The mindspace way. J. Econ. Psychol. 2012, 33, 264–277. [Google Scholar] [CrossRef]
- Vorsters, A.; Bosch, F.X.; Bosch, F.X.; Bonanni, P.; Franco, E.L.; Baay, M.; Simas, C.; Waheed, D.E.N.; Castro, C.; Murillo, R.; et al. Prevention and control of HPV infection and HPV-related cancers in Colombia- a meeting report. BMC Proc. 2020, 14, 8. [Google Scholar] [CrossRef] [PubMed]
- Aquino Rojas, E.; Aquino Rojas, W.A.; Soto Flores, R.; Soto Flores, O. Tácticas de fortalecimiento para la prevención del cáncer cervico uterino a través de la vacunación contra el virus del papiloma humano, agosto de 2017 a marzo de 2018. Gac. Méd. Boliv. 2019, 42, 52–58. [Google Scholar] [CrossRef]
- Congreso de Colombia. Ley 1626, por Medio de la Cual se Garantiza la Vacunación Gratuita y Obligatoria a la Población Colombiana Objeto de la Misma, se Adoptan Medidas Integrales para la Prevención del Cáncer Cérvico Uterino y se Dictan otras Disposiciones. 2013. Available online: http://www.secretariasenado.gov.co/senado/basedoc/ley_1626_2013.html (accessed on 4 June 2022).
- Hintze, J.M.; O’Neill, J.P. Strengthening the case for gender-neutral and the nonavalent HPV vaccine. Eur. Arch. Otorhinolaryngol. 2018, 275, 857–865. [Google Scholar] [CrossRef] [PubMed]
- Friedman, A.L.; Oruko, K.O.; Habel, M.A.; Ford, J.; Kinsey, J.; Odhiambo, F.; Phillips-Howard, P.A.; Wang, S.A.; Collins, T.; Laserson, K.F.; et al. Preparing for human papillomavirus vaccine introduction in Kenya: Implications from focus-group and interview discussions with caregivers and opinion leaders in Western Kenya. BMC Public Health 2014, 14, 855. [Google Scholar] [CrossRef] [Green Version]
- Morales-Campos, D.Y.; Snipes, S.A.; Villarreal, E.K.; Crocker, L.C.; Guerrero, A.; Fernandez, M.E. Cervical cancer, human papillomavirus (HPV), and HPV vaccination: Exploring gendered perspectives, knowledge, attitudes, and cultural taboos among Mexican American adults. Ethn. Health 2021, 26, 206–224. [Google Scholar] [CrossRef]
- World Health Organization. Cervical Cancer. Cerv Cancer Fact Sheets 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/cervical-cancer (accessed on 6 July 2022).
- Burger, E.A.; De Kok, I.M.C.M.; Groene, E.; Killen, J.; Canfell, K.; Kulasingam, S.; Kuntz, K.M.; Matthijsse, S.; Regan, C.; Simms, K.T.; et al. Estimating the Natural History of Cervical Carcinogenesis Using Simulation Models: A CISNET Comparative Analysis. J. Natl. Cancer Inst. 2020, 112, 955–963. [Google Scholar] [CrossRef]
- Hansen, P.R.; Schmidtblaicher, M.; Brewer, N.T. Resilience of HPV vaccine uptake in Denmark: Decline and recovery. Vaccine 2020, 38, 1842–1848. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Top 10 Tips to Improve HPV Vaccine Rates|CDC 2018. Available online: https://www.cdc.gov/hpv/hcp/2-dose/top-10-vaxsuccess.html (accessed on 4 June 2022).
- Gray, L.M.; Wong-Wylie, G.; Rempel, G.R.; Cook, K. Expanding Qualitative Research Interviewing Strategies: Zoom Video Communications. Qual. Rep. 2020, 25, 1292–1301. [Google Scholar] [CrossRef]
- Hensen, B.; Mackworth-Young, C.R.S.; Simwinga, M.; Abdelmagid, N.; Banda, J.; Mavodza, C.; Doyle, A.M.; Bonell, C.; Weiss, H.A. Remote data collection for public health research in a COVID-19 era: Ethical implications, challenges and opportunities. Health Policy Plan. 2021, 36, 360–368. [Google Scholar] [CrossRef]
- Nguyen, K.H.; Santibanez, T.A.; Stokley, S.; Lindley, M.C.; Fisher, A.; Kim, D.; Greby, S.; Srivastav, A.; Singleton, J. Parental vaccine hesitancy and its association with adolescent HPV vaccination. Vaccine 2021, 39, 2416. [Google Scholar] [CrossRef]
- Fetters, M.D.; Freshwater, D. The 1 + 1 = 3 Integration Challenge. J. Mix. Methods Res. 2015, 9, 115–117. [Google Scholar] [CrossRef]


{kind=link}
| Adults | % | N |
|---|---|---|
| Sex | ||
| Female | 89.3% | 175 |
| Male | 10.7% | 21 |
| Socioeconomic status | ||
| Low | 15.8% | 31 |
| Medium | 23.5% | 46 |
| High | 60.7% | 119 |
| Daughter’s school type | ||
| Private | 71.4% | 140 |
| Public | 28.6% | 56 |
| Doses | ||
| 0 | 57.1% | 112 |
| 1 | 42.9% | 84 |
| Religious practice | ||
| Yes | 82.7 | 162 |
| No | 17.3 | 34 |
| Healthcare-system affiliation | ||
| Contributory plan | 96.9% | 190 |
| Subsidized plan | 3.1% | 6 |
| Girls and Adolescents | % | N |
|---|---|---|
| Education level | ||
| Primary | 60% | 30 |
| Secondary | 40% | 20 |
| Type of school | ||
| Private | 48% | 24 |
| Public | 52% | 26 |
| School location | ||
| Urban | 74% | 37 |
| Rural | 26% | 13 |
| Doses | ||
| 0 | 42% | 21 |
| 1 | 58% | 29 |
| Source of Behaviour | Quantitative Data from the Online Questionnaire | Themes from the Focus Groups |
|---|---|---|
| Capability | 11.7% did not perceive that their daughter would be susceptible to contracting HPV. Relationship between likelihood of vaccinating daughter and perceived susceptibility to HPV; Spearman r = 0.309, p < 0.001. 84.7% perceived that their daughter was susceptible to cervical cancer. 96.9% were aware that they should get their daughter vaccinated. 69.4% did not receive any information about HPV vaccination for their daughter. 87.8% trusted the information they received about vaccines. Relationship between likelihood of getting vaccinated and receiving positive information about the vaccine; Spearman r = 0.338, p < 0.001 | Lack of information Relationship between HPV and cervical cancer |
| Opportunity | Relationship between likelihood of getting vaccinated and medical recommendation; Spearman r = 0.221, p < 0.01 Relationship between likelihood of getting vaccinated and seeing others get vaccinated; Spearman r = 0.158, p < 0.05 | Trust in traditional institutions |
| Motivation | 30.1% were concerned about vaccine effectiveness 32.7% were concerned because vaccines may have adverse effects 31.6% were concerned about vaccine safety Relationship between likelihood of getting vaccinated and vaccine safety; Spearman r = 0.277, p < 0.001. | Association of HPV with sexuality The vaccine as an act of care Respect for the personal decision to be vaccinated |
| Step | Variable Entered | B | Wald | Sig | Exp (B) | C.I for Exp (B) | |
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| 1 | SEP medium | −0.575 | 0.616 | 0.432 | 0.562 | 0.134 | 2.366 |
| SEP high | −0.736 | 1.424 | 0.233 | 0.479 | 0.143 | 1.604 | |
| Religion | −0.532 | 0.828 | 0.363 | 0.587 | 0.187 | 1.847 | |
| 2 | Cost | −0.065 | 0.045 | 0.832 | 0.937 | 0.514 | 1.709 |
| Easy access to vaccine | 0.142 | 0.245 | 0.620 | 1.153 | 0.657 | 2.025 | |
| Social norms | −0.053 | 0.017 | 0.896 | 0.949 | 0.431 | 2.088 | |
| Medical recommendation | −0.713 | 5.167 | 0.023 | 0.490 | 0.265 | 0.906 | |
| Others’ recommendations | −0.593 | 2.408 | 0.121 | 0.553 | 0.261 | 1.169 | |
| Safety | 0.873 | 3.200 | 0.074 | 2.394 | 0.920 | 6.233 | |
| Susceptibility | −0.584 | 3.617 | 0.057 | 0.558 | 0.306 | 1.018 | |
| Positive information | −0.460 | 2.365 | 0.124 | 0.631 | 0.351 | 1.135 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cordoba-Sanchez, V.; Lemos, M.; Tamayo-Lopera, D.A.; Sheinfeld Gorin, S. HPV-Vaccine Hesitancy in Colombia: A Mixed-Methods Study. Vaccines 2022, 10, 1187. https://doi.org/10.3390/vaccines10081187
Cordoba-Sanchez V, Lemos M, Tamayo-Lopera DA, Sheinfeld Gorin S. HPV-Vaccine Hesitancy in Colombia: A Mixed-Methods Study. Vaccines. 2022; 10(8):1187. https://doi.org/10.3390/vaccines10081187
Chicago/Turabian StyleCordoba-Sanchez, Veronica, Mariantonia Lemos, Diego Alfredo Tamayo-Lopera, and Sherri Sheinfeld Gorin. 2022. "HPV-Vaccine Hesitancy in Colombia: A Mixed-Methods Study" Vaccines 10, no. 8: 1187. https://doi.org/10.3390/vaccines10081187