
Trends in COVID-19 Vaccination Intent, Determinants and Reasons for Vaccine Hesitancy: Results from Repeated Cross-Sectional Surveys in the Adult General Population of Greece during November 2020–June 2021

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Phone Surveys and Questionnaire
2.2. Statistical Methods
2.3. Ethical Issues
3. Results
3.1. Characteristics of the Participants
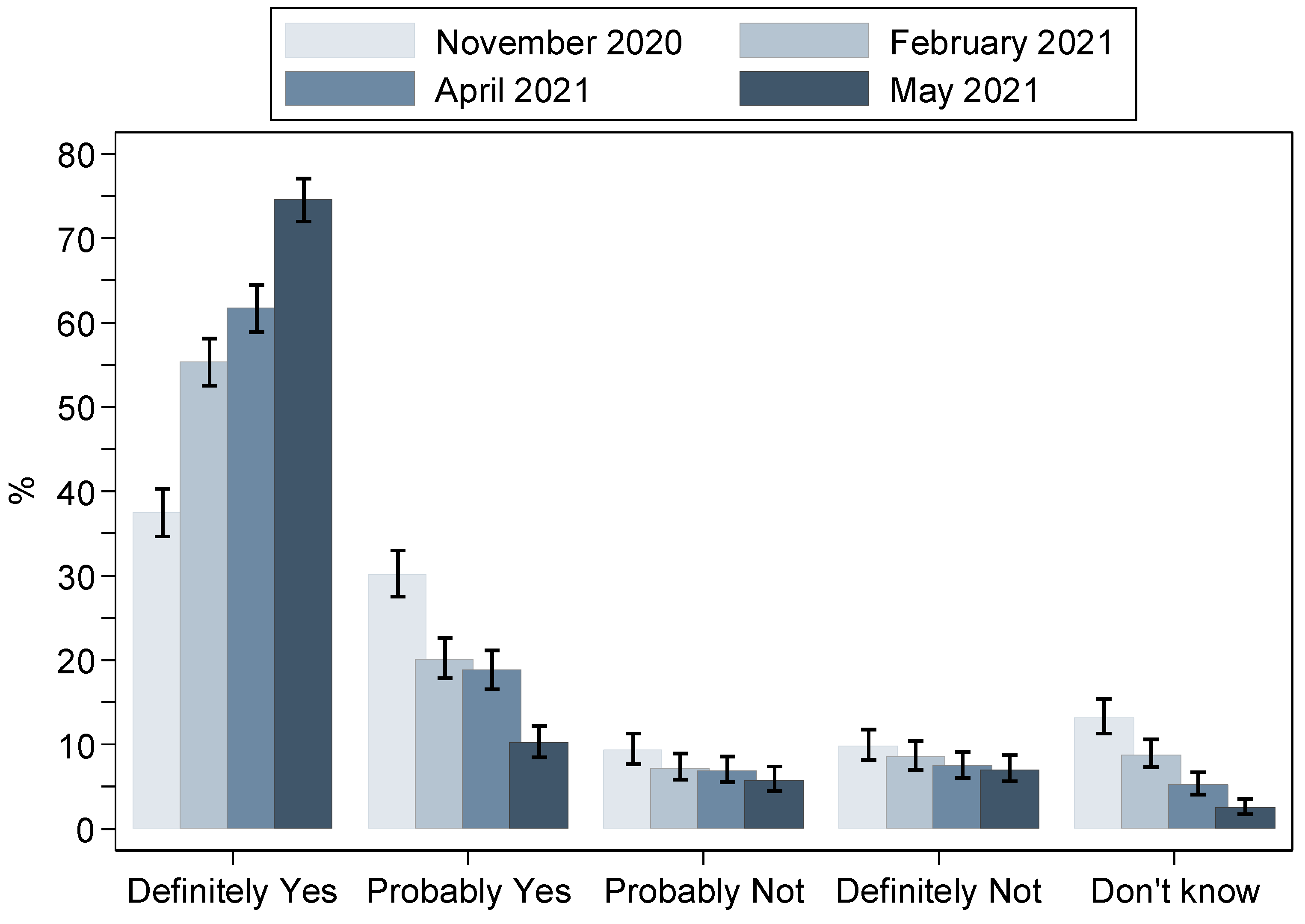
3.2. Trends in Vaccination Intention
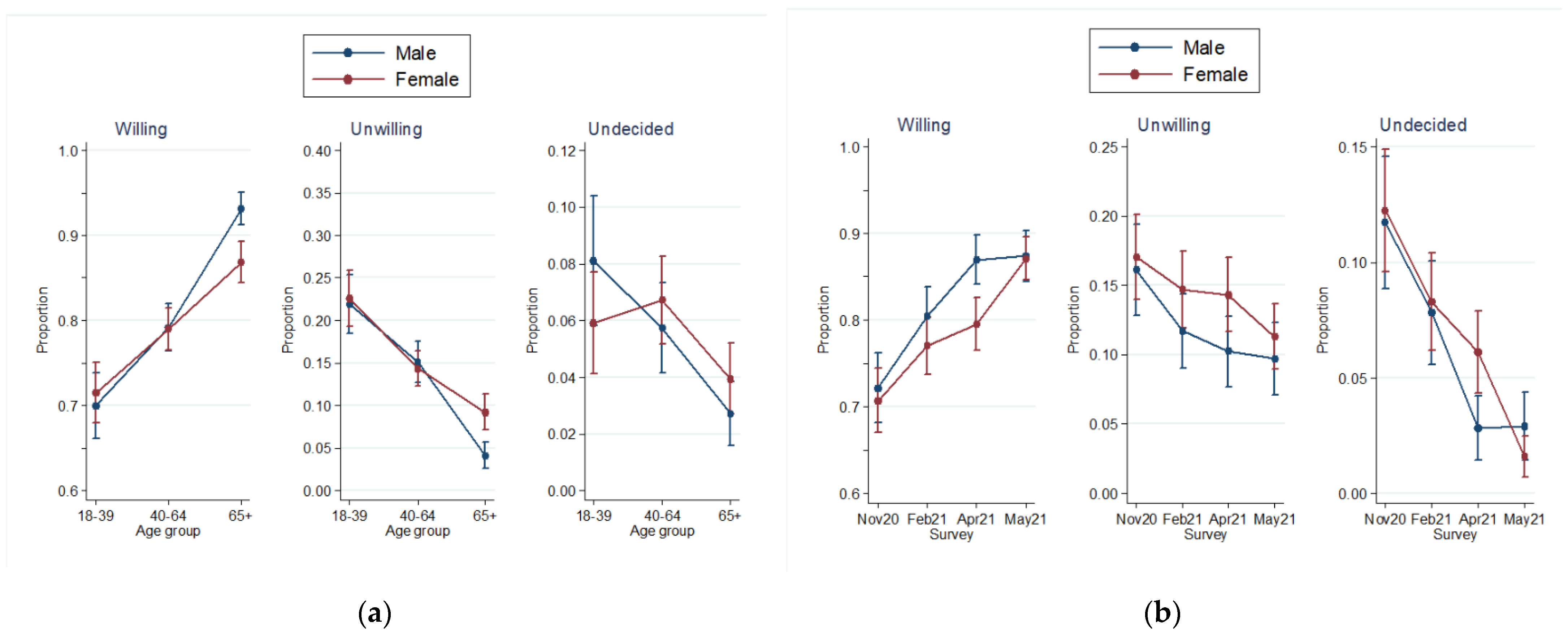
3.3. Trends in Vaccination Intention According to Respondents’ Characteristics
3.4. Predictors of Unwillingness to Be Vaccinated or Uncertainty with Regard to Vaccination
3.5. Reasons for Not Intending to Be Vaccinated
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Weekly Epidemiological Update on COVID-19—8 June 2021. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---8-june-2021 (accessed on 13 June 2021).
- WHO. Pandemic fatigue—reinvigorating the public to prevent COVID-19. In Policy Framework for Supporting Pandemic Prevention and Management; WHO Regional Office for Europe: Copenhagen, Denmark, 2020. [Google Scholar]
- World Health Organization. Status of COVID-19 Vaccines within WHO EUL/PQ evaluation process. Guidance Document 02 March 2022. Available online: https://extranet.who.int/pqweb/sites/default/files/documents/Status_COVID_VAX_02March2022.pdf (accessed on 3 March 2022).
- Hodgson, D.; Flasche, S.; Jit, M.; Kucharski, A.J.; CMMID COVID-19 Working Group; Centre for Mathematical Modelling of Infectious Disease (CMMID) COVID-19 Working Group. The potential for vaccination-induced herd immunity against the SARS-CoV-2 B.1.1.7 variant. Eurosurveillance 2021, 26, 2100428. [Google Scholar] [CrossRef] [PubMed]
- Bollyky, T.J. U.S. COVID-19 Vaccination Challenges Go Beyond Supply. Ann. Intern. Med. 2021, 174, 558–559. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef] [PubMed]
- Hrynick, T.; Ripoll, S.; Schmidt-Sane, M. Rapid Review: Vaccine Hesitancy and Building Confidence in COVID-19 Vaccination; Social Science in Humanitarian Action (SSHAP): Brighton, UK, 2020. [Google Scholar]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Bohm, R. Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef] [Green Version]
- Rosen, B.; Waitzberg, R.; Israeli, A.; Hartal, M.; Davidovitch, N. Addressing vaccine hesitancy and access barriers to achieve persistent progress in Israel’s COVID-19 vaccination program. Isr. J. Health Policy Res. 2021, 10, 43. [Google Scholar] [CrossRef]
- Fagerland, M.W.; Hosmer, D.W.; Bofin, A.M. Multinomial goodness-of-fit tests for logistic regression models. Stat. Med. 2008, 27, 4238–4253. [Google Scholar] [CrossRef]
- Lin, C.; Tu, P.; Beitsch, L.M. Confidence and Receptivity for COVID-19 Vaccines: A Rapid Systematic Review. Vaccines 2020, 9, 16. [Google Scholar] [CrossRef]
- Edwards, B.; Biddle, N.; Gray, M.; Sollis, K. COVID-19 vaccine hesitancy and resistance: Correlates in a nationally representative longitudinal survey of the Australian population. PLoS ONE 2021, 16, e0248892. [Google Scholar] [CrossRef]
- Paul, E.; Steptoe, A.; Fancourt, D. Attitudes towards vaccines and intention to vaccinate against COVID-19: Implications for pub-lic health communications. Lancet Reg. Health Eur. 2021, 1, 100012. [Google Scholar] [CrossRef]
- Viswanath, K.; Bekalu, M.; Dhawan, D.; Pinnamaneni, R.; Lang, J.; McLoud, R. Individual and social determinants of COVID-19 vac-cine uptake. BMC Public Health 2021, 21, 818. [Google Scholar] [CrossRef]
- Coe, A.B.; Elliott, M.H.; Gatewood, S.B.S.; Goode, J.R.; Moczygemba, L.R. Perceptions and predictors of intention to receive the COVID-19 vaccine. Res. Soc. Adm. Pharm. 2021, 18, 2593–2599. [Google Scholar] [CrossRef] [PubMed]
- Hammer, C.C.; Cristea, V.; Dub, T.; Sivela, J. High but slightly declining COVID-19 vaccine acceptance and reasons for vaccine acceptance, Finland April to December 2020. Epidemiol. Infect. 2021, 149, e123. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Global Attitudes Towards a COVID-19 Vaccine. Imperial College London. May 2021. Available online: https://www.imperial.ac.uk/media/imperial-college/institute-of-global-health-innovation/GlobalVaccineInsights (accessed on 3 March 2022).
- Kourlaba, G.; Kourkouni, E.; Maistreli, S.; Tsopela, C.G.; Molocha, N.M.; Triantafyllou, C.; Koniordou, M.; Kopsidas, I.; Chorianopoulou, E.; Maroudi-Manta, S.; et al. Willingness of Greek general population to get a COVID-19 vaccine. Glob. Health Res. Policy 2021, 6, 3. [Google Scholar] [CrossRef] [PubMed]
- Maltezou, H.C.; Pavli, A.; Dedoukou, X.; Georgakopoulou, T.; Raftopoulos, V.; Drositis, I.; Bolikas, E.; Ledda, C.; Adamis, G.; Spyrou, A.; et al. Determinants of intention to get vaccinated against COVID-19 among healthcare personnel in hospitals in Greece. Infect. Dis. Health 2021, 26, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Papagiannis, D.; Rachiotis, G.; Malli, F.; Papathanasiou, I.V.; Kotsiou, O.; Fradelos, E.C.; Giannakopoulos, K.; Gourgoulianis, K.I. Ac-ceptability of COVID-19 Vaccination among Greek Health Professionals. Vaccines 2021, 9, 200. [Google Scholar] [CrossRef]
- Sheeran, P. Intention—Behavior relations: A conceptual and empirical review. Eur. Rev. Soc. Psychol. 2002, 12, 1–36. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Vaccine Tracker Stockholm: ECDC. 2021. Available online: https://vaccinetracker.ecdc.europa.eu/public/extensions/COVID-19/vaccine-tracker.html#uptake-tab (accessed on 2 March 2022).
- Reno, C.; Maietti, E.; Fantini, M.P.; Savoia, E.; Manzoli, L.; Montalti, M.; Gori, D. Enhancing COVID-19 Vaccines Acceptance: Results from a Survey on Vaccine Hesitancy in Northern Italy. Vaccines 2021, 9, 378. [Google Scholar] [CrossRef]
- Wang, K.; Wong, E.L.-Y.; Ho, K.-F.; Cheung, A.W.-L.; Yau, P.S.-Y.; Dong, D.; Wong, S.Y.-S.; Yeoh, E.-K. Change of Willingness to Accept COVID-19 Vaccine and Reasons of Vaccine Hesitancy of Working People at Different Waves of Local Epidemic in Hong Kong, China: Repeated Cross-Sectional Surveys. Vaccines 2021, 9, 62. [Google Scholar] [CrossRef]
- European Medicines Agency. Astrazeneca’s COVID-19 Vaccine: Ema Finds Possible Link to Very Rare Cases of Unusual Blood Clots with Low Blood Plate-Lets. 7 April 2021. Available online: https://www.ema.europa.eu/en/news/astrazenecas-covid-19-vaccine-ema-finds-possible-link-very-rare-cases-unusual-blood-clots-low-blood (accessed on 2 June 2021).
- Bonioli, M.; McIsaac, M.; Xu, L.; Wuliji, T.; Diallo, K.; Campbell, J. Gender Equity in the Health Workforce: Analysis of 104 Countries; Working Paper 1; WHO/HIS/HWF/Gender/WP1/2019.1; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Nguyen, K.H.; Srivastav, A.; Razzaghi, H.; Williams, W.; Lindley, M.C.; Jorgensen, C.; Abad, A.; Singleton, J.A. COVID-19 Vaccination Intent, Perceptions, and Reasons for Not Vaccinating Among Groups Prioritized for Early Vaccination—United States, September and December 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 217–222. [Google Scholar] [CrossRef]
- Troiano, G.; Nardi, A. Vaccine hesitancy in the era of COVID-19. Public Health 2021, 194, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Education Is Now a Bigger Factor than Race in Desire for COVID-19 Vaccine. 2 March 2021. Available online: https://healthpolicy.usc.edu/evidence-base/education-is-now-a-bigger-factor-than-race-in-desire-for-covid-19-vaccine/ (accessed on 2 June 2021).
- Baccolini, V.; Renzi, E.; Isonne, C.; Migliara, G.; Massimi, A.; De Vito, C.; Marzuillo, C.; Villari, P. COVID-19 Vaccine Hesitancy among Italian University Students: A Cross-Sectional Survey during the First Months of the Vaccination Campaign. Vaccines 2021, 9, 1292. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Participants’ Characteristics | 17 November– 3 December 2020 (N = 1097) | 1–18 February 2021 (N = 1196) | 1–12 April 2021 (N = 1189) | 17 May–5 June 2021 (N = 1200) |
|---|---|---|---|---|
| Age, n (%) | ||||
| 18–39 | 329 (30.0) | 305 (25.5) | 305 (25.7) | 322 (26.8) |
| 40–64 | 418 (38.1) | 549 (45.9) | 545 (45.8) | 540 (45.0) |
| 65+ | 350 (31.9) | 342 (28.6) | 339 (28.5) | 338 (28.2) |
| Gender, n (%) | ||||
| Male | 504 (45.9) | 562 (47.0) | 524 (44.1) | 495 (41.3) |
| Female | 593 (54.1) | 634 (53.0) | 665 (55.9) | 705 (58.8) |
| Educational level, n (%) | ||||
| Up to junior high school | 221 (20.2) | 239 (20.1) | 233 (19.7) | 188 (15.8) |
| Up to general high school | 370 (33.7) | 339 (28.4) | 326 (27.5) | 369 (30.9) |
| University | 438 (39.9) | 463 (38.8) | 498 (42.0) | 487 (40.8) |
| Postgraduate education | 68 (6.2) | 151 (12.7) | 128 (10.8) | 149 (12.5) |
| Household size, median (25th, 75th) | 2 (2, 3) | 3 (2, 4) | 3 (2, 4) | 3 (2, 4) |
| Living with a person ≥65 years old, n (%) | 395 (36.0) | 366 (30.6) | 376 (31.6) | 390 (32.5) |
| Living with a child ≤12 years old, n (%) | 158 (14.4) | 227 (19.0) | 235 (19.8) | 194 (16.2) |
| Participants’ Characteristics | 17 November–3 December 2020 | 1–18 February 2021 | 1–12 April 2021 | 17 May–5 June 2021 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (N = 1097) | (N = 1196) | (N = 1189) | (N = 1200) | |||||||||
| Willing | Unwilling | Undecided | Willing | Unwilling | Undecided | Willing | Unwilling | Undecided | Willing | Unwilling | Undecided | |
| Age group | ||||||||||||
| 18–39 | 58.7 [53.2, 63.9] | 26.7 [22.2, 31.8] | 14.6 [11.2, 18.8] | 66.9 [61.4, 72.0] | 23.6 [19.2, 28.7] | 9.5 [6.7, 13.4] | 75.7 [70.6, 80.2] | 18.0 [14.1, 22.8] | 6.2 [4.0, 9.6] | 79.5 [74.7, 83.6] | 18.6 [14.7, 23.3] | 1.9 [0.8, 4.1] |
| 40–64 | 68.9 [64.3, 73.2] | 17.9 [14.5, 21.9] | 13.2 [10.2, 16.8] | 76.3 [72.6, 79.7] | 14.4 [11.7, 17.6] | 9.3 [7.1, 12.0] | 79.6 [76.0, 82.8] | 15.0 [12.3, 18.3] | 5.3 [3.7, 7.6] | 85.4 [82.1, 88.1] | 11.1 [8.7, 14.1] | 3.5 [2.3, 5.5] |
| 65+ | 79.1 [74.6, 83.1] | 10.3 [7.5, 13.9] | 10.6 [7.8, 14.3] | 87.1 [83.1, 90.3] | 5.8 [3.8, 8.9] | 7.0 [4.7, 10.3] | 88.2 [84.3, 91.2] | 8.0 [5.5, 11.4] | 3.8 [2.2, 6.5] | 92.9 [89.6, 95.2] | 5.9 [3.8, 9.0] | 1.2 [0.4, 3.1] |
| Gender | ||||||||||||
| Male | 69.8 [65.7, 73.7] | 18.1 [14.9, 21.7] | 12.1 [9.5, 15.3] | 78.5 [74.9, 81.7] | 13.3 [10.8, 16.4] | 8.2 [6.2, 10.8] | 84.4 [81.0, 87.2] | 12.4 [9.8, 15.5] | 3.2 [2.0, 5.2] | 85.7 [82.3, 88.5] | 11.1 [8.6, 14.2] | 3.2 [2.0, 5.2] |
| Female | 68.5 [64.6, 72.1] | 18.2 [15.3, 21.5] | 13.3 [10.8, 16.3] | 75.7 [72.2, 78.9] | 15.1 [12.6, 18.2] | 9.1 [7.1, 11.7] | 78.5 [75.2, 81.5] | 14.9 [12.4, 17.8] | 6.6 [5.0, 8.8] | 86.1 [83.3, 88.5] | 12.1 [9.8, 14.7] | 1.8 [1.1, 3.2] |
| Educational level | ||||||||||||
| Up to junior high school | 66.5 [60.0, 72.4] | 15.4 [11.2, 20.8] | 18.1 [13.5, 23.8] | 71.1 [65.0, 76.5] | 15.5 [11.4, 20.7] | 13.4 [9.6, 18.3] | 78.1 [72.3, 83.0] | 13.7 [9.9, 18.8] | 8.2 [5.3, 12.4] | 84.0 [78.1, 88.6] | 12.8 [8.7, 18.4] | 3.2 [1.4, 6.9] |
| Up to high school | 70.8 [66.0, 75.2] | 15.9 [12.6, 20.0] | 13.2 [10.1, 17.1] | 72.6 [67.6, 77.1] | 17.1 [13.5, 21.5] | 10.3 [7.5, 14.1] | 77.9 [73.1, 82.1] | 16.3 [12.6, 20.7] | 5.8 [3.7, 9.0] | 83.5 [79.3, 86.9] | 13.8 [10.7, 17.7] | 2.7 [1.5, 5.0] |
| University | 68.5 [64.0, 72.7] | 20.8 [17.2, 24.8] | 10.7 [8.2, 14.0] | 81.0 [77.2, 84.3] | 13.4 [10.6, 16.8] | 5.6 [3.8, 8.1] | 81.9 [78.3, 85.1] | 13.9 [11.1, 17.2] | 4.2 [2.8, 6.4] | 87.3 [84.0, 90.0] | 11.1 [8.6, 14.2] | 1.6 [0.8, 3.3] |
| Postgraduate education | 72.1 [60.2, 81.5] | 22.1 [13.7, 33.6] | 5.9 [2.2, 14.8] | 84.1 [77.3, 89.1] | 9.3 [5.6, 15.1] | 6.6 [3.6, 11.9] | 91.4 [85.1, 95.2] | 7.8 [4.2, 14.0] | 0.8 [0.1, 5.4] | 91.3 [85.5, 94.9] | 6.7 [3.6, 12.1] | 2.0 [0.6, 6.1] |
| Variables | Unwilling | Undecided | ||
|---|---|---|---|---|
| RRR † [95% CI] | p | RRR † [95% CI] | p | |
| Gender Female/Male | 2.2 [1.3, 3.9] | 0.006 | 0.8 [0.3, 1.9] | 0.571 |
| Period | ||||
| April 2021/May 2021 | 1.1 [0.7, 1.6] | 0.778 | 1.0 [0.5, 2.0] | 0.947 |
| February 2021/May 2021 | 1.3 [0.9, 1.9] | 0.170 | 2.9 [1.6, 5.4] | <0.001 |
| November 2020/May 2021 | 2.0 [1.4, 2.9] | <0.001 | 4.9 [2.7, 8.8] | <0.001 |
| Gender × Period | ||||
| Female × April 2021 | 1.3 [0.8, 2.2] | 0.293 | 4.3 [1.6, 11.4] | 0.003 |
| Female × February 2021 | 1.1 [0.7, 1.8] | 0.649 | 2.0 [0.8, 4.8] | 0.120 |
| Female × November 2020 | 0.9 [0.6, 1.5] | 0.757 | 1.9 [0.8, 4.6] | 0.131 |
| Age group | ||||
| 18–39/65+ | 7.1 [4.6, 11.1] | <0.001 | 4.0 [2.4, 6.6] | <0.001 |
| 40–64/65+ | 4.3 [2.8, 6.7] | <0.001 | 2.5 [1.5, 4.1] | <0.001 |
| Age group × Gender | ||||
| 18–39 × Female | 0.4 [0.2, 0.7] | 0.001 | 0.5 [0.2, 0.9] | 0.018 |
| 40–64 × Female | 0.4 [0.2, 0.7] | <0.001 | 0.8 [0.4, 1.4] | 0.359 |
| Education | ||||
| Up to junior high/postgraduate | 2.7 [1.9, 3.9] | <0.001 | 4.3 [2.5, 7.4] | <0.001 |
| Up to high school/postgraduate | 2.1 [1.5, 3.0] | <0.001 | 2.6 [1.5, 4.3] | <0.001 |
| University/postgraduate | 1.8 [1.3, 2.5] | <0.001 | 1.6 [0.9, 2.7] | 0.079 |
| Child at home Yes/No | 1.3 [1.1, 1.6] | 0.015 | 0.9 [0.7, 1.3] | 0.730 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sypsa, V.; Roussos, S.; Engeli, V.; Paraskevis, D.; Tsiodras, S.; Hatzakis, A. Trends in COVID-19 Vaccination Intent, Determinants and Reasons for Vaccine Hesitancy: Results from Repeated Cross-Sectional Surveys in the Adult General Population of Greece during November 2020–June 2021. Vaccines 2022, 10, 470. https://doi.org/10.3390/vaccines10030470
Sypsa V, Roussos S, Engeli V, Paraskevis D, Tsiodras S, Hatzakis A. Trends in COVID-19 Vaccination Intent, Determinants and Reasons for Vaccine Hesitancy: Results from Repeated Cross-Sectional Surveys in the Adult General Population of Greece during November 2020–June 2021. Vaccines. 2022; 10(3):470. https://doi.org/10.3390/vaccines10030470
Chicago/Turabian StyleSypsa, Vana, Sotirios Roussos, Vasiliki Engeli, Dimitrios Paraskevis, Sotirios Tsiodras, and Angelos Hatzakis. 2022. "Trends in COVID-19 Vaccination Intent, Determinants and Reasons for Vaccine Hesitancy: Results from Repeated Cross-Sectional Surveys in the Adult General Population of Greece during November 2020–June 2021" Vaccines 10, no. 3: 470. https://doi.org/10.3390/vaccines10030470