
Effectiveness of BNT162b2 and mRNA-1273 Vaccines against COVID-19 Infection: A Meta-Analysis of Test-Negative Design Studies


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategies
2.2. Data Extraction and Study Quality Assessment
2.3. Data Synthesis and Analysis
3. Results
3.1. Literature Research and Study Characteristics
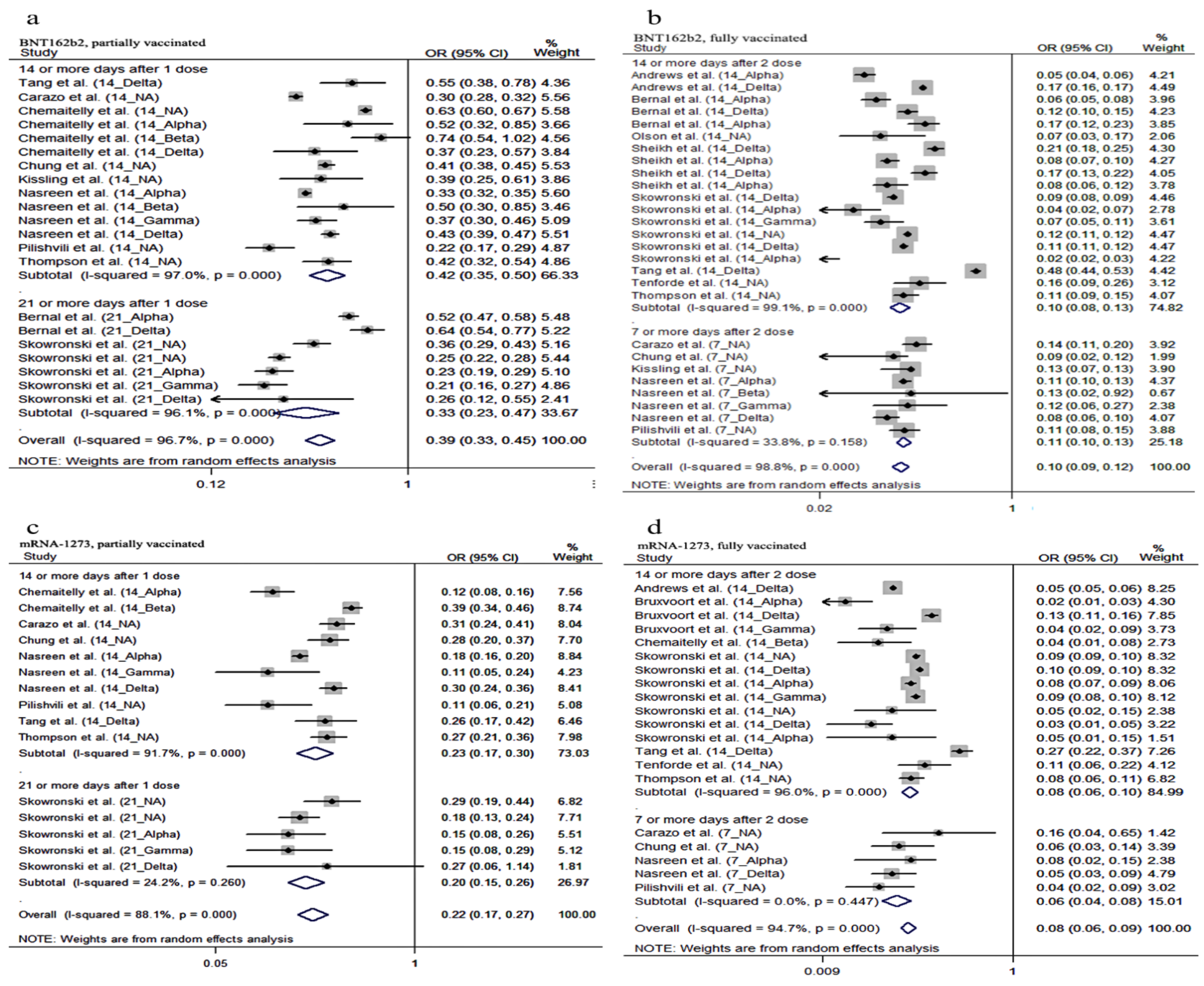
3.2. Pooled VE of BNT162b2 and mRNA-1273 against COVID-19 Infection
3.3. Pooled VE against VOC
3.4. Pooled VE by Different Time Points after Vaccination
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | 14 or More Days after 1 Dose | 21 or More Days after 1 Dose | 7 or More Days after 2 Doses | 14 or More Days after 2 Doses | Variant | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cases | Controls | Cases | Controls | Cases | Controls | Cases | Controls | ||||||||||
| V* | UV* | V | UV | V | UV | V | UV | V | UV | V | UV | V | UV | V | UV | ||
| Chung [17] | 636 | 51,220 | 7483 | 251,541 | 51 | 51,220 | 3275 | 25,154 | NA | ||||||||
| Bernal [20] | 450 | 7313 | 8641 | 96,371 | 49 | 7313 | 15,749 | 96,371 | Alpha | ||||||||
| 137 | 4043 | 8641 | 96,371 | 122 | 4043 | 15,749 | 96,371 | Delta | |||||||||
| Pilishvili [23] | NA | NA | NA | NA | NA | NA | NA | NA | |||||||||
| Thompson [21] | 88 | 2847 | 824 | 8965 | 105 | 2847 | 3484 | 8965 | NA | ||||||||
| Tenforde [26] | 28 | 454 | 69 | 144 | NA | ||||||||||||
| Bernal [27] | 42 | 37,320 | 672 | 89,377 | |||||||||||||
| Sheikh [29] | 208 | 3672 | 53,471 | 113,591 | Delta | ||||||||||||
| 104 | 5828 | 53,471 | 113,591 | Alpha | |||||||||||||
| 75 | 2439 | 4326 | 38,065 | Delta | |||||||||||||
| 34 | 3977 | 4394 | 38,065 | Alpha | |||||||||||||
| Chemaitelly [35] | 2358 | 3567 | 111,472 | 110,263 | NA | ||||||||||||
| 27 | 1581 | 50 | 1558 | Alpha | |||||||||||||
| 72 | 3000 | 95 | 2977 | Beta | |||||||||||||
| 27 | 2134 | 72 | 2089 | Delta | |||||||||||||
| Skowronski [31] | 215 | 475 | 5408 | 4067 | NA | ||||||||||||
| Nascreen [22] | 2484 | 37,621 | 60,775 | 440,391 | 138 | 37,621 | 32,292 | 440,391 | Alpha | ||||||||
| 17 | 331 | 60,758 | 373,364 | - | - | 32,292 | 373,364 | Beta | |||||||||
| 104 | 1678 | 60,758 | 373,364 | - | - | 32,292 | 373,364 | Gamma | |||||||||
| 657 | 1832 | 54,770 | 155,232 | 87 | 1832 | 28,335 | 155,232 | Delta | |||||||||
| Skowronski [32] | 4876 | 18,809 | 168,831 | 76,621 | NA | ||||||||||||
| 2501 | 11,500 | 168,831 | 76,621 | Delta | |||||||||||||
| 10 | 728 | 168,831 | 76,621 | Alpha | |||||||||||||
| 24 | 708 | 168,831 | 76,621 | Gamma | |||||||||||||
| 3707 | 11,366 | 387,968 | 212,918 | NA | |||||||||||||
| 2489 | 6349 | 397,968 | 212,918 | Delta | |||||||||||||
| 32 | 1589 | 387,968 | 212,918 | Alpha | |||||||||||||
| Carazo [30] | 1202 | 3424 | 24,589 | 18,663 | 48 | 3424 | 1954 | 18,663 | NA | ||||||||
| Kissling [33] | 30 | 505 | 433 | 2345 | 14 | 505 | 512 | 2345 | NA | ||||||||
| Skowronski [18] | 299 | 5258 | 7959 | 35,358 | NA | ||||||||||||
| 93 | 5802 | 774 | 12,194 | Alpha | |||||||||||||
| 64 | 5802 | 591 | 12,194 | Gamma | |||||||||||||
| 9 | 5802 | 50 | 12,194 | Delta | |||||||||||||
| Tang [17] | Delta | ||||||||||||||||
| Andrews [34] | - | - | - | - | Alpha | ||||||||||||
| - | - | - | - | Delta | |||||||||||||
| Olson [25] | 6 | 173 | 93 | 192 | NA | ||||||||||||
| Study | 14 or More Days after 1 Dose | 21 or More Days after 1 Dose | 7 Or More Days After 2 Doses | 14 or More Days after 2 Doses | Variant | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cases | Controls | Cases | Controls | Cases | Controls | Cases | Controls | ||||||||||
| V * | UV * | V | UV | V | UV | V | UV | V | UV | V | UV | V | UV | V | UV | ||
| Chung [19] | 49 | 51,220 | 962 | 251,541 | 6 | 51,220 | 542 | 251,541 | NA | ||||||||
| Pilishvili [23] | - | - | - | - | - | - | - | - | NA | ||||||||
| Thompson [21] | 49 | 2847 | 2427 | 8965 | NA | ||||||||||||
| Tenforde [26] | 17 | 454 | 46 | 144 | NA | ||||||||||||
| Skowronski [31] | 28 | 475 | 913 | 4067 | NA | ||||||||||||
| Narseen [22] | 282 | 37,621 | 13,750 | 440,391 | - | 37,621 | 8608 | 440,391 | Alpha | ||||||||
| 6 | 1678 | 13,750 | 373,364 | Gamma | |||||||||||||
| 117 | 1832 | 12,955 | 155,232 | 14 | 1832 | 7807 | 155,232 | Delta | |||||||||
| Skowronski [32] | 1209 | 18,809 | 41,889 | 76,621 | NA | ||||||||||||
| 573 | 11,500 | 41,889 | 76,621 | Delta | |||||||||||||
| 3 | 728 | 41,889 | 76,621 | Alpha | |||||||||||||
| 3 | 708 | 41,889 | 76,621 | Gamma | |||||||||||||
| 796 | 11,366 | 109,861 | 212,918 | NA | |||||||||||||
| 517 | 6349 | 109,861 | 212,918 | Delta | |||||||||||||
| 9 | 1589 | 109,861 | 212,918 | Alpha | |||||||||||||
| Carazo [30] | 64 | 3424 | 1529 | 18,663 | 2 | 3424 | 126 | 18,663 | NA | ||||||||
| Bruxvoort [24] | 13 | 1409 | 1734 | 5376 | Alpha | ||||||||||||
| 232 | 1795 | 4588 | 5547 | Delta | |||||||||||||
| 9 | 340 | 552 | 1193 | Gamma | |||||||||||||
| Tang [17] | 150 | 2797 | 1568 | 10,583 | Delta | ||||||||||||
| Andrews [34] | - | - | - | - | Delta | ||||||||||||
| Chemaitelly [28] | 44 | 23,860 | 365 | 23,539 | Alpha | ||||||||||||
| 419 | 47,872 | 1067 | 47,224 | 6 | 44,731 | 165 | 44,572 | Beta | |||||||||
| Study | Vaccine Type | After 1 Dose (days) | OR | After 2 Doses (days) | OR | Variants |
|---|---|---|---|---|---|---|
| Tang et al. [17] | BNT162b2 | ≥14 | 0.203 (0.026–1.595) | ≥14 | 0.066 (0.03–0.146) | Delta |
| mRNA-1273 | ≥14 | 0.133 (0.017–1.014) | ≥14 | 0.039 (0.005–0.284) | Delta | |
| Nasreen et al. [22] | BNT162b2 | ≥14 | 0.14 (0.13–0.16) | ≥7 | 0.32 (0.25–0.41) | Alpha |
| mRNA-1273 | ≥14 | 0.116 (0.13–0.20) | ≥7 | 0.04 (0.02–0.07) | Alpha | |
| BNT162b2 | ≥14 | 0.28 (0.13–0.63) | ≥7 | 0.122 (0.01–0.94) | Beta | |
| BNT162b2 | ≥14 | 0.14 (0.09–0.22) | ≥7 | 0.10 (0.02–0.40) | Gamma | |
| mRNA-1273 | ≥14 | 0.07 (0.02–0.27) | — | — | Gamma | |
| BNT162b2 | ≥14 | 0.17 (0.09–0.30) | ≥7 | 0.05 (0.01–0.21) | Non-VOC | |
| mRNA-1273 | ≥14 | 0.17 (0.05–0.56) | — | — | Non-VOC | |
| Bruxvoort et al. [24] | mRNA-1273 | — | — | ≥14 | 0.025 (0.008–0.073) | Delta |
| mRNA-1273 | — | — | ≥14 | 0.034 (0.011–0.105) | NA | |
| Skiwronski et al. [32] | BNT162b2 | — | — | ≥14 | 0.02 (0.02–0.03) | Delta |
| BNT162b2 | — | — | ≥14 | 0.04 (0.01–0.17) | Alpha | |
| BNT162b2 | — | — | ≥14 | 0.03 (0.01–0.07) | Gamma | |
| mRNA-1273 | — | — | ≥14 | 0.03 (0.02–0.04) | Delta | |
| BNT162b2 | — | — | ≥14 | 0.03 (0.02–0.04) | Delta | |
| mRNA-1273 | — | — | ≥14 | 0.02 (0.01–0.04) | Delta | |
| mRNA-1273 | — | — | ≥14 | 0.13 (0.04–0.44) | Alpha | |
| Skiwronski et al. [31] | BNT162b2 | ≥21 | 0.19 (0.15–0.25) | — | — | NA |
| mRNA-1273 | ≥21 | 0.15 (0.09–0.24) | — | — | NA | |
| Andrews et al. [34] | BNT162b2 | — | — | ≥14 | 0.021 (0.005–0.086) | Alpha |
| BNT162b2 | — | — | ≥14 | 0.033 (0.03–0.037) | Delta |

References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. 2021. Available online: https://covid19.who.int/ (accessed on 22 November 2021).
- Frenck, R.W., Jr.; Klein, N.P.; Kitchin, N.; Gurtman, A.; Absalon, J.; Lockhart, S.; Perez, J.L.; Walter, E.B.; Senders, S.; Bailey, R.; et al. Safety, Immunogenicity, and Efficacy of the BNT162b2 COVID-19 Vaccine in Adolescents. N. Engl. J. Med. 2021, 385, 239–250. [Google Scholar] [CrossRef] [PubMed]
- Hall, V.G.; Ferreira, V.H.; Ku, T.; Ierullo, M.; Majchrzak-Kita, B.; Chaparro, C.; Selzner, N.; Schiff, J.; McDonald, M.; Tomlinson, G.; et al. Randomized Trial of a Third Dose of mRNA-1273 Vaccine in Transplant Recipients. N. Engl. J. Med. 2021, 385, 1244–1246. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- El Sahly, H.M.; Baden, L.R.; Essink, B.; Doblecki-Lewis, S.; Martin, J.M.; Anderson, E.J.; Campbell, T.B.; Clark, J.; Jackson, L.A.; Fichtenbaum, C.J.; et al. Efficacy of the mRNA-1273 SARS-CoV-2 Vaccine at Completion of Blinded Phase. N. Engl. J. Med. 2021, 385, 1774–1785. [Google Scholar] [CrossRef]
- Walensky, R.P.; Walke, H.T.; Fauci, A.S. SARS-CoV-2 Variants of Concern in the United States-Challenges and Opportunities. JAMA 2021, 325, 1037–1038. [Google Scholar] [CrossRef]
- Garcia-Beltran, W.F.; Lam, E.C.; St Denis, K.; Nitido, A.D.; Garcia, Z.H.; Hauser, B.M.; Feldman, J.; Pavlovic, M.N.; Gregory, D.J.; Poznansky, M.C.; et al. Multiple SARS-CoV-2 variants escape neutralization by vaccine-induced humoral immunity. Cell 2021, 184, 2523. [Google Scholar] [CrossRef]
- Planas, D.; Veyer, D.; Baidaliuk, A.; Staropoli, I.; Guivel-Benhassine, F.; Rajah, M.M.; Planchais, C.; Porrot, F.; Robillard, N.; Puech, J.; et al. Reduced sensitivity of SARS-CoV-2 variant Delta to antibody neutralization. Nature 2021, 596, 276–280. [Google Scholar] [CrossRef]
- Hoffmann, M.; Arora, P.; Gross, R.; Seidel, A.; Hornich, B.F.; Hahn, A.S.; Krüger, N.; Graichen, L.; Hofmann-Winkler, H.; Kempf, A.; et al. SARS-CoV-2 variants B.1.351 and P.1 escape from neutralizing antibodies. Cell 2021, 184, 2384–2393.e12. [Google Scholar] [CrossRef]
- Jackson, M.L.; Nelson, J.C. The test-negative design for estimating influenza vaccine effectiveness. Vaccine 2013, 31, 2165–2168. [Google Scholar] [CrossRef]
- Ranzani, O.T.; Hitchings, M.D.T.; Dorion, M.; D’Agostini, T.L.; de Paula, R.C.; de Paula, O.F.P.; Villela, E.F.M.; Torres, M.S.S.; de Oliveira, S.B.; Schulz, W.; et al. Effectiveness of the CoronaVac vaccine in older adults during a gamma variant associated epidemic of COVID-19 in Brazil: Test negative case-control study. BMJ 2021, 374, n2015. [Google Scholar] [CrossRef] [PubMed]
- Li, X.N.; Huang, Y.; Wang, W.; Jing, Q.L.; Zhang, C.H.; Qin, P.Z.; Guan, W.J.; Gan, L.; Li, Y.L.; Liu, W.H.; et al. Effectiveness of inactivated SARS-CoV-2 vaccines against the Delta variant infection in Guangzhou: A test-negative case-control real-world study. Emerg. Microbes Infect. 2021, 10, 1751–1759. [Google Scholar] [CrossRef] [PubMed]
- Dean, N.E.; Hogan, J.W.; Schnitzer, M.E. COVID-19 Vaccine Effectiveness and the Test-Negative Design. N. Engl. J. Med. 2021, 385, 1431–1433. [Google Scholar] [CrossRef] [PubMed]
- Evans, S.J.W.; Jewell, N.P. Vaccine Effectiveness Studies in the Field. N. Engl. J. Med. 2021, 385, 650–651. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.; Shea, B.; O’Connell, D.; Pereson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses, Ottawa Hospital Research Institute. 2011. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 22 November 2021).
- Tang, P.; Hasan, M.R.; Chemaitelly, H.; Yassine, H.M.; Benslimane, F.M.; Al Khatib, H.A.; AlMukdad, S.; Coyle, P.; Ayoub, H.H.; Al Kanaani, Z.; et al. BNT162b2 and mRNA-1273 COVID-19 vaccine effectiveness against the SARS-CoV-2 Delta variant in Qatar. Nat. Med. 2021, 27, 2136–2143. [Google Scholar] [CrossRef] [PubMed]
- Skowronski, D.M.; Setayeshgar, S.; Zou, M.; Prystajecky, N.; Tyson, J.R.; Sbihi, H.; Fjell, C.D.; Galanis, E.; Naus, M.; Patrick, D.M.; et al. Comparative single-dose mRNA and ChAdOx1 vaccine effectiveness against SARS-CoV-2, including early variants of concern: A test-negative design, British Columbia, Canada. medRxiv 2021, jiac023. [Google Scholar] [CrossRef]
- Chung, H.; He, S.; Nasreen, S.; Sundaram, M.E.; Buchan, S.A.; Wilson, S.E.; Chen, B.; Calzavara, A.; Fell, D.B.; Austin, P.C.; et al. Effectiveness of BNT162b2 and mRNA-1273 COVID-19 vaccines against symptomatic SARS-CoV-2 infection and severe COVID-19 outcomes in Ontario, Canada: Test negative design study. BMJ 2021, 374, n1943. [Google Scholar] [CrossRef]
- Bernal, J.L.; Andrews, N.; Gower, C.; Gallagher, E.; Simmons, R.; Thelwall, S.; Stowe, J.; Tessier, E.; Groves, N.; Dabrera, G.; et al. Effectiveness of COVID-19 Vaccines against the B.1.617.2 (Delta) Variant. N. Engl. J. Med. 2021, 385, 585–594. [Google Scholar] [CrossRef]
- Thompson, M.G.; Stenehjem, E.; Grannis, S.; Ball, S.W.; Naleway, A.L.; Ong, T.C.; DeSilva, M.B.; Natarajan, K.; Bozio, C.H.; Lewis, N.; et al. Effectiveness of COVID-19 vaccines in ambulatory and inpatient care settings. N. Engl. J. Med. 2021, 385, 1355–1371. [Google Scholar] [CrossRef]
- Nasreen, S.; Chung, H.; He, S.; Brown, K.A.; Gubbay, J.B.; Buchan, S.A.; Fell, D.B.; Austin, P.C.; Schwartz, K.L.; Sundaram, M.E.; et al. Effectiveness of mRNA and ChAdOx1 COVID-19 vaccines against symptomatic SARS-CoV-2 infection and severe outcomes with variants of concern in Ontario. medRxiv 2021. [Google Scholar] [CrossRef]
- Pilishvili, T.; Gierke, R.; Fleming-Dutra, K.E.; Farrar, J.L.; Mohr, N.M.; Talan, D.A.; Krishnadasan, A.; Harland, K.K.; Smithline, H.A.; Hou, P.C.; et al. Effectiveness of mRNA COVID-19 Vaccine among U.S. Health Care Personnel. N. Engl. J. Med. 2021, 385, e90. [Google Scholar] [CrossRef] [PubMed]
- Bruxvoort, K.J.; Sy, L.S.; Qian, L.; Ackerson, B.K.; Luo, Y.; Lee, G.S.; Tian, Y.; Florea, A.; Aragones, M.; Tubert, J.E.; et al. Effectiveness of mRNA-1273 against Delta, Mu, and other emerging variants. medRxiv 2021. [Google Scholar] [CrossRef]
- Olson, S.M.; Newhams, M.M.; Halasa, N.B.; Price, A.M.; Boom, J.A.; Sahni, L.C.; Irby, K.; Walker, T.C.; Schwartz, S.P.; Pannaraj, P.S.; et al. Effectiveness of Pfizer-BioNTech mRNA Vaccination against COVID-19 Hospitalization among Persons Aged 12–18 Years-United States, June–September 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1483–1488. [Google Scholar] [CrossRef] [PubMed]
- Tenforde, M.W.; Patel, M.M.; Ginde, A.A.; Douin, D.J.; Talbot, H.K.; Casey, J.D.; Mohr, N.M.; Zepeski, A.; Gaglani, M.; McNeal, T.; et al. Effectiveness of SARS-CoV-2 mRNA Vaccines for Preventing COVID-19 Hospitalizations in the United States. Clin. Infect. Dis. 2021, ciab687. [Google Scholar] [CrossRef] [PubMed]
- Bernal, J.L.; Andrews, N.; Gower, C.; Robertson, C.; Stowe, J.; Tessier, E.; Simmons, R.; Cottrell, S.; Roberts, R.; O’Doherty, M.; et al. Effectiveness of the Pfizer-BioNTech and Oxford-AstraZeneca vaccines on COVID-19 related symptoms, hospital admissions, and mortality in older adults in England: Test negative case-control study. BMJ-Br. Med. J. 2021, 373, n1088. [Google Scholar] [CrossRef] [PubMed]
- Chemaitelly, H.; Yassine, H.M.; Benslimane, F.M.; Al Khatib, H.A.; Tang, P.; Hasan, M.R.; Malek, J.A.; Coyle, P.; Ayoub, H.H.; Al Kanaani, Z.; et al. mRNA-1273 COVID-19 vaccine effectiveness against the B.1.1.7 and B.1.351 variants and severe COVID-19 disease in Qatar. Nat. Med. 2021, 27, 1614–1621. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, A.; McMenamin, J.; Taylor, B.; Robertson, C. SARS-CoV-2 Delta VOC in Scotland: Demographics, risk of hospital admission, and vaccine effectiveness. Lancet 2021, 397, 2461–2462. [Google Scholar] [CrossRef]
- Carazo, S.; Talbot, D.; Boulianne, N.; Brisson, M.; Gilca, R.; Deceuninck, G.; Brousseau, N.; Drolet, M.; Ouakki, M.; Sauvageau, C.; et al. Single-dose mRNA vaccine effectiveness against SARS-CoV-2 in healthcare workers extending 16 weeks post-vaccination: A test-negative design from Quebec, Canada. Clin. Infect. Dis. 2021, ciab739. [Google Scholar] [CrossRef]
- Skowronski, D.M.; Setayeshgar, S.; Zou, M.; Prystajecky, N.; Tyson, J.R.; Galanis, E.; Naus, M.; Patrick, D.M.; Sbihi, H.; El Adam, S.; et al. Single-dose mRNA vaccine effectiveness against SARS-CoV-2, including Alpha and Gamma variants: A test-negative design in adults 70 years and older in British Columbia, Canada. Clin. Infect. Dis. 2021, ciab616. [Google Scholar] [CrossRef]
- Skowronski, D.M.; Setayeshgar, S.; Febriani, Y.; Ouakki, M.; Zou, M.; Talbot, D.; Prystajecky, N.; Tyson, J.R.; Gilca, R.; Brousseau, N.; et al. Two-dose SARS-CoV-2 vaccine effectiveness with mixed schedules and extended dosing intervals: Test-negative design studies from British Columbia and Quebec, Canada. medRxiv 2021. [Google Scholar] [CrossRef]
- Kissling, E.; Hooiveld, M.; Martin, V.S.; Martinez-Baz, I.; William, N.; Vilcu, A.M.; Mazagatos, C.; Domegan, L.; de Lusignan, S.; Meijer, A.; et al. Vaccine effectiveness against symptomatic SARS-CoV-2 infection in adults aged 65 years and older in primary care: I-MOVE-COVID-19 project, Europe, December 2020 to May 2021. Eurosurveillance 2021, 26, 2100670. [Google Scholar] [CrossRef] [PubMed]
- Andrews, N.; Tessier, E.; Stowe, J.; Gower, C.; Kirsebom, F.; Simmons, R.; Gallagher, E.; Chand, M.; Brown, K.; Ladhani, S.N.; et al. Vaccine effectiveness and duration of protection of Comirnaty, Vaxzevria and Spikevax against mild and severe COVID-19 in the UK. medRxiv 2021. [Google Scholar] [CrossRef]
- Chemaitelly, H.; Tang, P.; Hasan, M.R.; AlMukdad, S.; Yassine, H.M.; Benslimane, F.M.; Al Khatib, H.A.; Coyle, P.; Ayoub, H.H.; Al Kanaani, Z.; et al. Waning of BNT162b2 Vaccine Protection against SARS-CoV-2 Infection in Qatar. N. Engl. J. Med. 2021, 385, e83. [Google Scholar] [CrossRef] [PubMed]
- Bajema, K.L.; Dahl, R.M.; Prill, M.M.; Meites, E.; Rodriguez-Barradas, M.C.; Marconi, V.C.; Beenhouwer, D.O.; Brown, S.T.; Holodniy, M.; Lucero-Obusan, C.; et al. Effectiveness of COVID-19 mRNA Vaccines Against COVID-19-Associated Hospitalization-Five Veterans Affairs Medical Centers, United States, 1 February–6 August 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1294–1299. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, E.S.; Holtgrave, D.R.; Dorabawila, V.; Conroy, M.; Greene, D.; Lutterloh, E. New COVID-19 Cases and Hospitalizations Among Adults, by Vaccination Status—New York, 3 May–25 July 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1150–1155. [Google Scholar] [CrossRef]
- Seppälä, E.; Veneti, L.; Starrfelt, J.; Danielsen, A.S.; Bragstad, K.; Hungnes, O.; Taxt, A.M.; Watle, S.V.; Meijerink, H. Vaccine effectiveness against infection with the Delta (B.1.617.2) variant, Norway, April to August 2021. Eurosurveillance 2021, 26, 2100793. [Google Scholar] [CrossRef]
- Edara, V.V.; Pinsky, B.A.; Suthar, M.S.; Lai, L.; Davis-Gardner, M.E.; Floyd, K.; Flowers, M.W.; Wrammert, J.; Hussaini, L.; Ciric, C.R.; et al. Infection and Vaccine-Induced Neutralizing-Antibody Responses to the SARS-CoV-2 B.1.617 Variants. N. Engl. J. Med. 2021, 385, 664–666. [Google Scholar] [CrossRef]
- Hoffmann, M.; Hofmann-Winkler, H.; Krüger, N.; Kempf, A.; Nehlmeier, I.; Graichen, L.; Arora, P.; Sidarovich, A.; Moldenhauer, A.S.; Winkler, M.S.; et al. SARS-CoV-2 variant B.1.617 is resistant to bamlanivimab and evades antibodies induced by infection and vaccination. Cell Rep. 2021, 36, 109415. [Google Scholar] [CrossRef]
- Swift, M.D.; Breeher, L.E.; Tande, A.J.; Tommaso, C.P.; Hainy, C.M.; Chu, H.; Murad, M.H.; Berbari, E.F.; Virk, A. Effectiveness of Messenger RNA Coronavirus Disease 2019 (COVID-19) Vaccines Against Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Infection in a Cohort of Healthcare Personnel. Clin. Infect. Dis. 2021, 73, e1376–e1379. [Google Scholar] [CrossRef]
- Paris, C.; Perrin, S.; Hamonic, S.; Bourget, B.; Roué, C.; Brassard, O.; Tadié, E.; Gicquel, V.; Bénézit, F.; Thibault, V.; et al. Effectiveness of mRNA-BNT162b2, mRNA-1273, and ChAdOx1 nCoV-19 vaccines against COVID-19 in healthcare workers: An observational study using surveillance data. Clin. Microbiol. Infect. 2021, 27, e5–e99. [Google Scholar] [CrossRef]
- Flacco, M.E.; Soldato, G.; Acuti Martellucci, C.; Carota, R.; Di Luzio, R.; Caponetti, A.; Manzoli, L. Interim Estimates of COVID-19 Vaccine Effectiveness in a Mass Vaccination Setting: Data from an Italian Province. Vaccines 2021, 9, 628. [Google Scholar] [CrossRef] [PubMed]
- Nanduri, S.; Pilishvili, T.; Derado, G.; Soe, M.M.; Dollard, P.; Wu, H.; Li, Q.; Bagchi, S.; Dubendris, H.; Link-Gelles, R.; et al. Effectiveness of Pfizer-BioNTech and Moderna Vaccines in Preventing SARS-CoV-2 Infection among Nursing Home Residents before and during Widespread Circulation of the SARS-CoV-2 B.1.617.2 (Delta) Variant-National Healthcare Safety Network, 1 March–1 August 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1163–1166. [Google Scholar] [CrossRef] [PubMed]
- Steensels, D.; Pierlet, N.; Penders, J.; Mesotten, D.; Heylen, L. Comparison of SARS-CoV-2 Antibody Response Following Vaccination with BNT162b2 and mRNA-1273. JAMA 2021, 326, 1533–1535. [Google Scholar] [CrossRef] [PubMed]
- Self, W.H.; Tenforde, M.W.; Rhoads, J.P.; Gaglani, M.; Ginde, A.A.; Douin, D.J.; Olson, S.M.; Talbot, H.K.; Casey, J.D.; Mohr, N.M.; et al. Comparative Effectiveness of Moderna, Pfizer-BioNTech, and Janssen (Johnson & Johnson) Vaccines in Preventing COVID-19 Hospitalizations among Adults Without Immunocompromising Conditions-United States, March–August 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1337–1343. [Google Scholar] [CrossRef]




| Study/Country | Study Period | Study Population | Number of Cases/Controls | Age (Years) | Female (%) | Vaccine Type | Point Time of Assessing VE | Variants | NOS | |
|---|---|---|---|---|---|---|---|---|---|---|
| Days after 1 Dose | Days after 2 Dose | |||||||||
| Tang et al./Qatar [17] | 23 March 2021 – 7 July 2021 | Resident population | 12,357/50,616 | 0–70+ | 21,095 (33.4) | BNT162b2, mRNA-1273 | ≥14 | ≥14 | Delta | 8 |
| Skowronski et al./Canada [18] | 4 April 2021 – 2 October 2021 | Adults in British Columbia | 3040/49,477 | 50–69 | 27,877 (53) | BNT162b2, mRNA-1273 | ≥21 | — | NA Alpha, Gamma, Delta | 6 |
| Chung et al./Canada [19] | 14 December 2020 – 19 April 2021 | Community dwelling people who had symptoms of COVID-19 | 53,270/270,763 | ≥18 | 185,539 (57.3) | BNT162b2, mRNA-1273 | ≥14 | ≥7 | NA | 8 |
| Bernal et al./UK [20] | October 2020 – May 2021 | Symptomatic persons who underwent COVID-19 testing in England | 11,356/96,371 | ≥16 | NA | BNT162b2 | ≥21 | ≥14 | Alpha, Delta | 8 |
| Thompson et al./US [21] | 1 January 2021 – 22 June 2021 | Laboratory-confirmed SARS-CoV-2 and COVID-19-like illness | 3251/18,271 | ≥50 | NA | BNT162b2, mRNA-1273 | ≥14 | ≥14 | NA | 8 |
| Nasreen et al./Canada [22] | 14 December 2020 – 3 August 2021 | Symptomatic community-dwelling individuals | 82,880/599,591 | ≥16 | 376,607 (55) | BNT162b2, mRNA-1273 | ≥14 | ≥7 | Alpha, Beta, Gamma, Delta | 7 |
| Pilishvili et al./US [23] | 28 December 2020 – 19 May 2021 | Health care personnel across 25 U.S. states | 1482/3449 | ≥18 | 4107 (83) | BNT162b2, mRNA-1273 | ≥14 | ≥7 | Delta | 6 |
| Bruxvoort et al./US [24] | 1 March 2021 – 27 September 2021 | KPSCa membership | 2027/10,135 | ≥18 | 5364 (44.1) | mRNA-1273 | — | ≥14 | Alpha, Gamma, Delta | 7 |
| Olson et al./US [25] | 1 June2021 – 30 September 2021 | Adolescent patients | 179/285 | 12–18 | 210 (45.3) | BNT162b2 | — | ≥14 | NA | 6 |
| Tenforde et al./US [26] | 11 March 2021 – 5 May 2021 | US adults | 590/620 | ≥18 | 613 (50.7) | BNT162b2, mRNA-1273 | — | ≥14 | NA | 6 |
| Bernal et al./UK [27] | 8 December 2020 – 19 February 2021 | Adults who reported symptoms | 44,590/112,340 | ≥70 | 87,066 (55.5) | BNT162b2 | — | ≥14 | Alpha | 7 |
| Chemaitelly et al./Qatar [28] | 1 February 2021 – 10 May 2021 | Resident population | 66,042/66,042 | 19–39 | 40,298 (30.5) | mRNA-1273 | ≥14 | ≥14 | Alpha, Beta | 8 |
| Sheikh et al./UK [29] | 1 April 2021 – 6 June 2021 | Individuals who have a PCR test for SARS-CoV-2 in study period | 10,827/195,000 | 0–90+ | NA | BNT162b2 | — | ≥14 | Alpha, Delta | 8 |
| Carazo et al./Canada [30] | 17 January 2021 – 5 June 2021 | Healthcare workers | 5316/53,160 | 18–74 | 48,513 (83) | BNT162b2, mRNA-1273 | ≥14 | ≥7 | NA | 6 |
| Skowronski et al./Canada [31] | 4 April 2021 – 1 May 2021 | Community-dwelling adults in British Columbia | 1226/15,767 | ≥70 | 8657 (50.9) | BNT162b2, mRNA-1273 | ≥21 | — | NA | 6 |
| Skowronski et al./Canada [32] | 3 May 2021 – 2 October 2021 | Community-dwelling adults in British Columbia and Quebec | British:27,439/353,093 Quebec:17,234/837,681 | ≥18 | British:211,999 (56) Quebee:511,620 (60) | BNT162b2, mRNA-1273 | — | ≥14 | NA, Alpha, Gamma, Delta | 7 |
| Kissling et al. [33] | 10 December 2021 – 31 May 2021 | Adults in 8 European countries | 592/4372 | ≥65 | 2933 (60) | BNT162b2 | ≥14 | ≥7 | NA | 6 |
| Andrews et al./UK [34] | 8 December 2020 – 3 September 2021 | Symptomatic adults | 1475,391/3757,981 | ≥16 | 2,928,972 (56) | BNT162b2, mRNA-1273 | — | ≥14 | Alpha, Delta | 8 |
| Chemaitelly et al./Qatar [35] | 1 January 2021 – 5 September 2021 | Resident population | 142,300/848,240 | 0–70+ | NA | BNT162b2 | ≥21 | — | NA Alpha, Beta, Delta | 8 |
| First Author | BNT162b2 OR 1 | Variant | |||
|---|---|---|---|---|---|
| 14 Days after 1 Dose | 21 Days after 1 Dose | 7 Days after 2 Doses | 14 Days after 2 Doses | ||
| Chung et al. [19] | 0.41 (0.38–0.45) | — | 0.09 (0.02–0.12) | NA | NA |
| Bernal et al. [20] | — | 0.525 (0.472–0.584) | — | 0.063 (0.047–0.084) | Alpha |
| — | 0.644 (0.536–0.773) | — | 0.12 (0.099–0.147) | Delta | |
| Pilishvili et al. [23] | 0.161 (0.121–0.213) | — | 0.085 (0.06–0.121) | — | Delta |
| Thompson et al. [21] | 0.42 (0.32–0.54) | — | — | 0.11 (0.09–0.15) | NA |
| Tenforde et al. [26] | — | — | — | 0.155 (0.091–0.262) | NA |
| Bernal et al. [27] | — | — | — | 0.17 (0.12–0.23) | Alpha |
| Sheikh et al. [29] | — | — | — | 0.21 (0.18–0.25) | Delta |
| — | — | — | 0.08 (0.07–0.10) | Alpha | |
| — | — | — | 0.17 (0.13–0.22) | Delta | |
| — | — | — | 0.08 (0.06–0.12) | Alpha | |
| Chemaitelly et al. [35] | 0.632 (0.598–0.668) | — | — | — | NA |
| 0.521 (0.321–0.845) | — | — | — | Alpha | |
| 0.742 (0.539–1.02) | — | — | — | Beta | |
| 0.366 (0.234–0574) | — | — | — | Delta | |
| Skowronski et al. [31] | NA | 0.36 (0.29–0.43) | — | — | NA |
| Nasreen et al. [22] | 0.33 (0.32–0.35) | — | 0.11 (0.10–0.13) | — | Alpha |
| 0.5 (0.30–0.85) | — | 0.13 (0.02–0.92) | — | Beta | |
| 0.37 (0.30–0.46) | — | 0.12 (0.06–0.27) | — | Gamma | |
| 0.43 (0.39–0.47) | — | 0.08 (0.06–0.10) | — | Delta | |
| Skowronski et al. [32] | — | — | — | 0.09 (0.08–0.09) | Delta |
| — | — | — | 0.04 (0.02–0.07) | Alpha | |
| — | — | — | 0.07 (0.05–0.11) | Gamma | |
| — | — | — | 0.12 (0.11–0.12) | NA | |
| — | — | — | 0.11 (0.11–0.12) | Delta | |
| — | — | — | 0.02 (0.02–0.03) | Alpha | |
| Carazo et al. [30] | 0.297 (0.276–0.319) | — | 0.145 (0.107–0.196) | — | NA |
| Kissling et al. [33] | 0.39 (0.25–0.61) | — | 0.13 (0.07–0.13) | — | NA |
| Skowronski et al. [18] | NA | 0.25 (0.22–0.28) | — | — | NA |
| NA | 0.23 (0.19–0.29) | — | — | Alpha | |
| NA | 0.21 (0.16–0.27) | — | — | Gamma | |
| NA | 0.26 (0.12–0.55) | — | — | Delta | |
| Tang et al. [17] | 0.547 (0.384–0.78) | — | — | 0.481 (0.436–0.53) | Delta |
| Andrews et al. [34] | — | — | — | 0.05 (0.041–0.062) | Alpha |
| — | — | — | 0.165 (0.164–0.167) | Delta | |
| Olson et al. [25] | — | — | — | 0.07 (0.03–0.17) | NA |
| First Author | mRNA-1273 OR 1 | Variants | |||
|---|---|---|---|---|---|
| 14 Days after 1 Dose | 21 Days after 1 Dose | 7 Days after 2 Doses | 14 Days after 2 Doses | ||
| Chung et al. [19] | 0.28 (0.20–0.37) | — | 0.06 (0.03–0.14) | — | NA |
| Pilishvili et al. [23] | 0.163 (0.124–0.214) | — | 0.08 (0.057–0.113) | — | Delta |
| Thompson et al. [21] | 0.27 (0.21–0.36) | — | — | 0.08 (0.06–0.11) | NA |
| Tenforde et al. [26] | — | — | — | 0.113 (0.059–0.215) | NA |
| Skowronski et al. [31] | — | 0.29 (0.19–0.44) | — | — | NA |
| Nasreen et al. [22] | 0.18 (0.16–0.20) | — | 0.08 (0.02–0.15) | — | Alpha |
| 0.11 (0.05–0.24) | — | — | — | Gamma | |
| 0.30 (0.24–0.36) | — | 0.05 (0.03–0.09) | — | Delta | |
| Skowronski et al. [32] | — | — | — | 0.09 (0.09–0.10) | NA |
| — | — | — | 0.10 (0.09–0.10) | Delta | |
| — | — | — | 0.08 (0.07–0.09) | Alpha | |
| — | — | — | 0.09 (0.08–0.10) | Gamma | |
| — | — | — | 0.05 (0.02–0.15) | NA | |
| — | — | — | 0.03 (0.01–0.05) | Delta | |
| — | — | — | 0.05 (0.01–0.15) | Alpha | |
| Carazo et al. [30] | 0.313 (0.241–0.405) | — | 0.159 (0.039–0.651) | — | NA |
| Bruxvoort et al. [24] | — | — | — | 0.016 (0.009–0.031) | Alpha |
| — | — | — | 0.133 (0.113–0.157) | Delta | |
| — | — | — | 0.045 (0.022–0.091) | Gamma | |
| Skowronski et al. [18] | — | 0.18 (0.13–0.24) | — | — | NA |
| — | 0.15 (0.08–0.26) | — | — | Alpha | |
| — | 0.15 (0.08–0.29) | — | — | Gamma | |
| — | 0.27 (0.06–1.14) | — | — | Delta | |
| Tang et al. [17] | 0.263 (0.165–0.419) | — | — | 0.269 (0.222–0.325) | Delta |
| Andrews et al. [34] | — | — | — | 0.052 (0.048–0.056) | Delta |
| Chemaitelly et al. [28] | 0.119 (0.085–0.163) | — | — | — | Alpha |
| 0.387 (0.345–0.455) | — | — | 0.036 (0.013–0.081) | Beta | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, S.; Liu, H.; Wu, J.; Xiao, W.; Chen, S.; Qiu, S.; Duan, G.; Song, H.; Zhang, R. Effectiveness of BNT162b2 and mRNA-1273 Vaccines against COVID-19 Infection: A Meta-Analysis of Test-Negative Design Studies. Vaccines 2022, 10, 469. https://doi.org/10.3390/vaccines10030469
Chang S, Liu H, Wu J, Xiao W, Chen S, Qiu S, Duan G, Song H, Zhang R. Effectiveness of BNT162b2 and mRNA-1273 Vaccines against COVID-19 Infection: A Meta-Analysis of Test-Negative Design Studies. Vaccines. 2022; 10(3):469. https://doi.org/10.3390/vaccines10030469
Chicago/Turabian StyleChang, Shuailei, Hongbo Liu, Jian Wu, Wenwei Xiao, Sijia Chen, Shaofu Qiu, Guangcai Duan, Hongbin Song, and Rongguang Zhang. 2022. "Effectiveness of BNT162b2 and mRNA-1273 Vaccines against COVID-19 Infection: A Meta-Analysis of Test-Negative Design Studies" Vaccines 10, no. 3: 469. https://doi.org/10.3390/vaccines10030469