
Risk Analysis by Age on the Burden of Meningococcal Disease in Spain

 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data source
2.3. Case Classification
| International
Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM;
Spanish version: Modificación Clínica Clasificación Internacional de
Enfermedades, CIE-10-MC) from 2016 to 2017 |
| A39
Infección meningocócica (meningococcal infection) A39.0 Meningitis meningocócica (meningococcal meningitis) A39.2 Meningococemia aguda (acute meningococcemia) A39.3 Meningococemia crónica (chronic meningococcemia) A39.4 Meningococemia, no especificada (meningococcemia, non-specific) A39.5 Enfermedad cardiaca debida a meningococo (heart disease due to meningococcus) A39.51 Endocarditis meningocócica (meningococcal endocarditis) |
| International
Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM;
Spanish version: Modificación Clínica Clasificación Internacional de Enfermedades,
CIE-9-MC) from 1998 to 2015 |
| 036-Infeccion
Meningococica (meningococcal infection) 036.0-Meningitis Meningococica (meningococcal meningitis) 036.1-Encefalitis Meningococica (meningococcal encephalitis) 036.2-Meningococemia (meningococcemia) 036.3-Sindrome De Waterhouse-Friderichsen, Meningococico (Waterhouse–Friderichsen Syndrome, meningococcal) 036.4-Carditis Meningococica (meningococcal carditis) 036.40-Carditis Meningococica Sin Especificar (meningococcal carditis, unspecified) 036.41-Pericarditis Meningococica (meningococcal pericarditis) 036.42-Endocarditis Meningococica (meningococcal endocarditis) 036.43-Miocarditis Meningococica (meningococcal myocarditis) 036.8-Otras Infecciones Meningococicas Especificadas (other specified meningococcal infections) 036.81-Neuritis Optica Meningococica (meningococcal neuritis optica) 036.82-Artropatia Meningococica (meningococcal arthropathy) |
2.4. Data Analysis
2.5. Ethical Consideration
3. Results
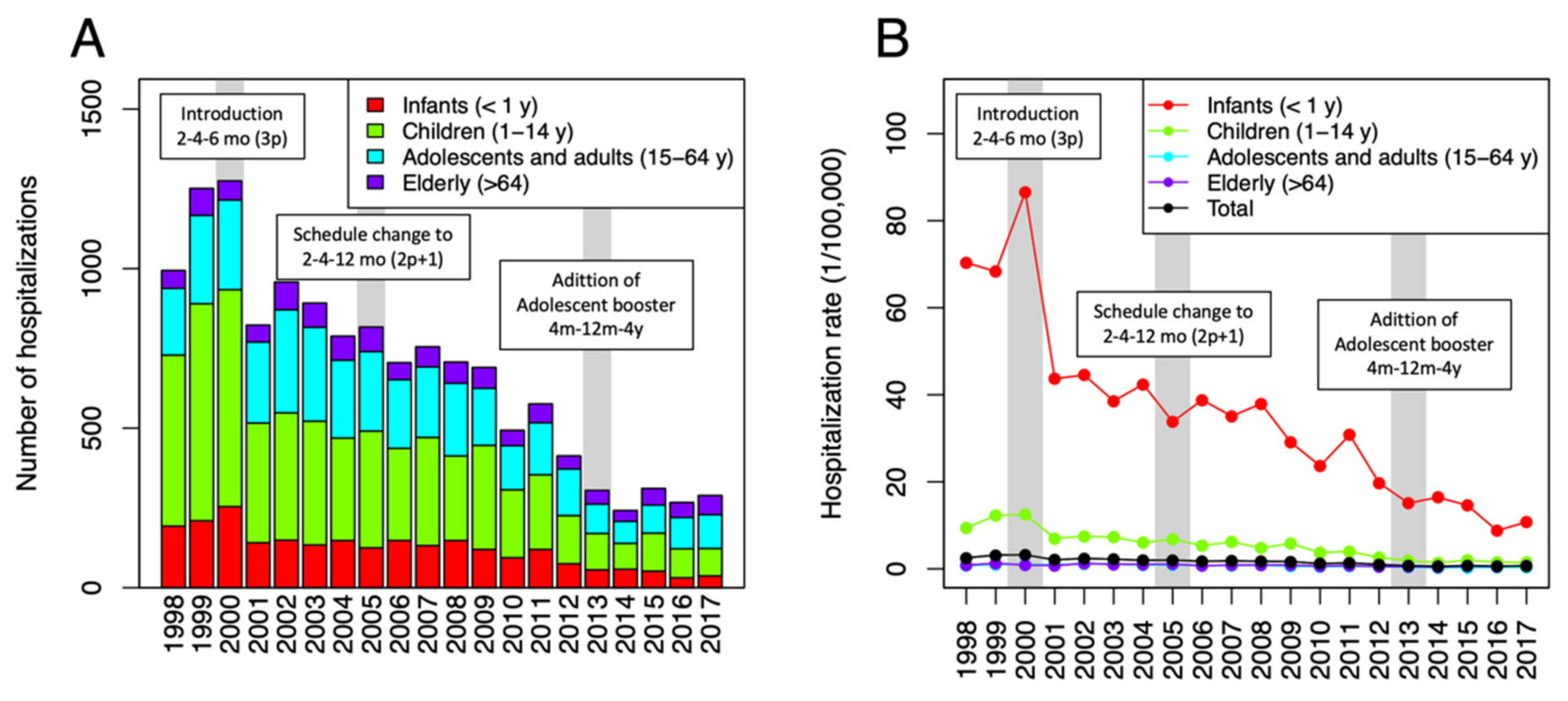
3.1. Meningococcal Disease Hospital Admissions in Spain from 1998 to 2017
3.2. Hospital Admission of Pediatric Age Group
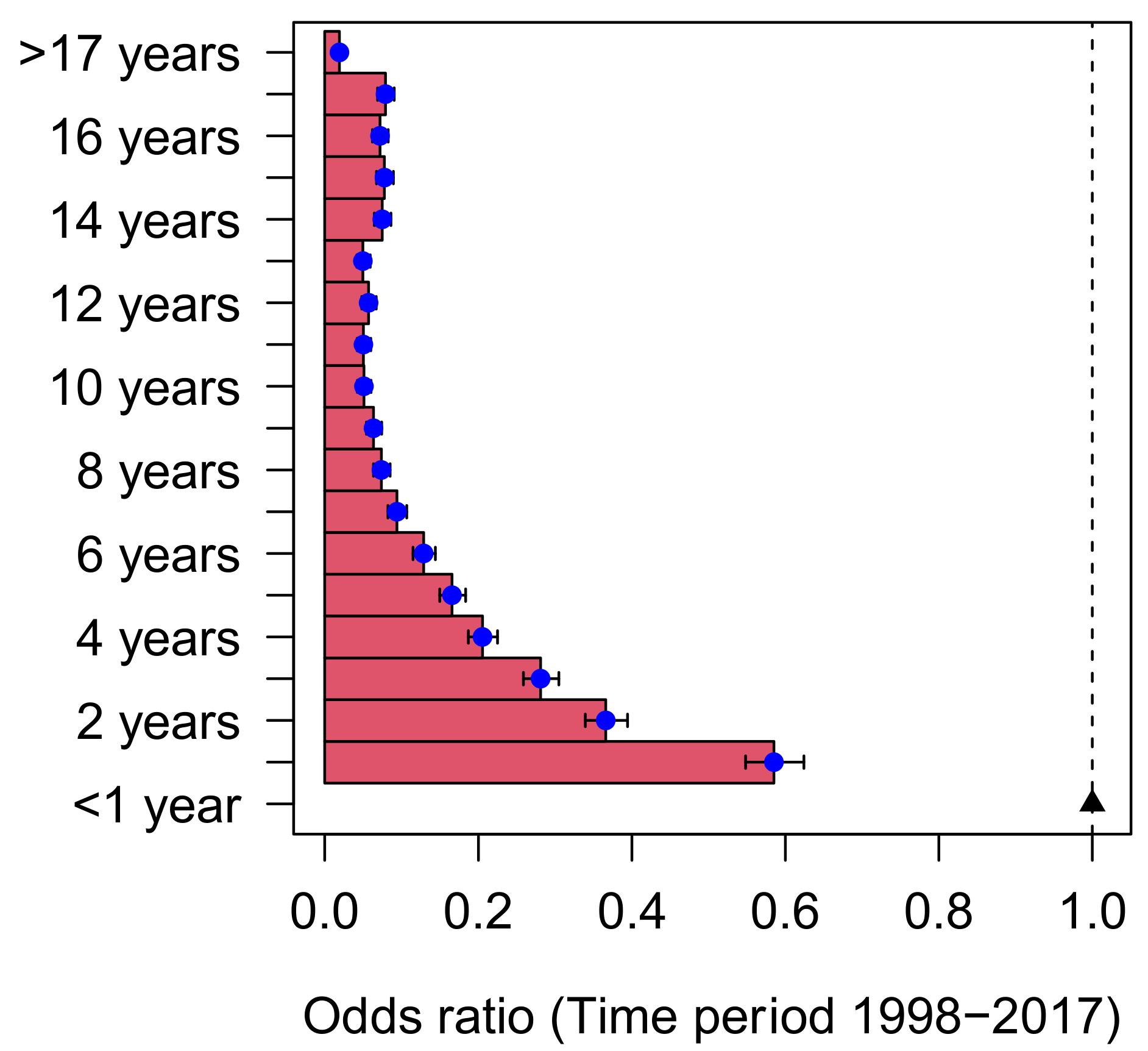
3.3. Risk of Hospital Admission by Age
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grupo de Trabajo Criterios 2011. Criterios de Evaluación para Fundamentar Modificaciones en el Programa de Vacunación en España; Ministerio de Sanidad, Servicios Sociales e Igualidad: Madrid, Spain, 2013.
- Black, S.; Shinefield, H. A routine infant schedule versus an older infant/toddler schedule for Neisseria meningitidis vaccination: What do experience and reason tell us? Expert Rev. Vaccines 2009, 8, 1623–1626. [Google Scholar] [CrossRef] [PubMed]
- Pelton, S.I.; Gilmet, G.P. Expanding prevention of invasive meningococcal disease. Expert Rev. Vaccines 2009, 8, 717–727. [Google Scholar] [CrossRef] [PubMed]
- Grupo de Trabajo de Enfermedad Meningocócica de la Ponencia de Programa y Registro de Vacunación. Situación Actual de la Enfermedad Meningocócica en España: Modificación de la Pauta de Vacunación Frente Meningococo C; Ministerio de Sanidad y Consumo: Madrid, Spain, 2005.
- Larrauri, A.; Cano, R.; Garcia, M.; Mateo, S. Impact and effectiveness of meningococcal C conjugate vaccine following its introduction in Spain. Vaccine 2005, 23, 4097–4100. [Google Scholar] [CrossRef] [PubMed]
- Cano, R.; Larrauri, A.; Mateo, S.; Alcala, B.; Salcedo, C.; Vazquez, J.A. Impact of the meningococcal C conjugate vaccine in Spain: An epidemiological and microbiological decision. Euro Surveill. Bull. Eur. Sur Les Mal. Transm. = Eur. Commun. Dis. Bull. 2004, 9, 5–6. [Google Scholar] [CrossRef]
- Grupo de trabajo MenCC 2012. Revisión del Programa de Vacunación Frente a Enfermedad Meningocócica por Serogrupo C: Ponencia de Programa y Registro de Vacunaciones; Ministerio de Sanidad, Servicios Sociales e Igualidad: Madrid, Spain, 2013.
- Ishola, D.A., Jr.; Borrow, R.; Findlow, H.; Findlow, J.; Trotter, C.; Ramsay, M.E. Prevalence of serum bactericidal antibody to serogroup C Neisseria meningitidis in England a decade after vaccine introduction. Clin. Vaccine Immunol. 2012, 19, 1126–1130. [Google Scholar] [CrossRef] [Green Version]
- Trotter, C.L.; Andrews, N.J.; Kaczmarski, E.B.; Miller, E.; Ramsay, M.E. Effectiveness of meningococcal serogroup C conjugate vaccine 4 years after introduction. Lancet 2004, 364, 365–367. [Google Scholar] [CrossRef]
- Trotter, C.L.; Borrow, R.; Findlow, J.; Holland, A.; Frankland, S.; Andrews, N.J.; Miller, E. Seroprevalence of antibodies against serogroup C meningococci in England in the postvaccination era. Clin. Vaccine Immunol. 2008, 15, 1694–1698. [Google Scholar] [CrossRef] [Green Version]
- Trotter, C.L.; Maiden, M.C.J. Meningococcal vaccines and herd immunity: Lessons learned from serogroup C conjugate vaccination programs. Expert Rev. Vaccines 2014, 8, 851–861. [Google Scholar] [CrossRef] [Green Version]
- Jafri, R.Z.; Ali, A.; Messonnier, N.E.; Tevi-Benissan, C.; Durrheim, D.; Eskola, J.; Fermon, F.; Klugman, K.P.; Ramsay, M.; Sow, S.; et al. Global epidemiology of invasive meningococcal disease. Popul. Health Metr. 2013, 11, 17. [Google Scholar] [CrossRef] [Green Version]
- Halperin, S.A.; Bettinger, J.A.; Greenwood, B.; Harrison, L.H.; Jelfs, J.; Ladhani, S.N.; McIntyre, P.; Ramsay, M.E.; Sáfadi, M.A. The changing and dynamic epidemiology of meningococcal disease. Vaccine 2012, 30 (Suppl. 2), B26–B36. [Google Scholar] [CrossRef]
- Borrow, R.; Alarcón, P.; Carlos, J.; Caugant, D.A.; Christensen, H.; Debbag, R.; De Wals, P.; Echaniz-Aviles, G.; Findlow, J.; Head, C.; et al. The Global Meningococcal Initiative: Global epidemiology, the impact of vaccines on meningococcal disease and the importance of herd protection. Expert Rev. Vaccines 2017, 16, 313–328. [Google Scholar] [CrossRef] [Green Version]
- Informacion Estadisticas Sanitarias. Registro de Altas—CMBD Hospitalización Año 2014; Ministerio de Sanidad, Servicios Sociales e Igualidad: Madrid, Spain, 2016.
- Gil-Prieto, R.; García-García, L.; Álvaro-Meca, A.; González-Escalada, A.; Ester, P.V.; Gil De Miguel, A. The burden of hospitalizations for meningococcal infection in Spain (1997–2008). Vaccine 2011, 29, 5765–5770. [Google Scholar] [CrossRef]
- Ministerio de Sanidad Consumo y Bienestar Social. Coberturas Vacunales en Espana-Ano 2016. Madrid, 2017. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/prevPromocion/vacunaciones/docs/CoberturasVacunacion/Todas_las_tablas.pdf (accessed on 13 December 2019).
- Calle, I.R.; Vilanova-Trillo, L.; Pardo-Seco, J.; Salvado, L.B.; Quinteiro, L.I.; Martinon-Torres, F. The Burden of Pediatric Invasive Meningococcal Disease in Spain (2008–2013). Pediatr. Infect. Dis. J. 2016, 35, 407–413. [Google Scholar] [CrossRef]
- Salleras, L.; Domínguez, A.; Prats, G.; Parron, I.; Muñoz, P. Dramatic decline of serogroup C meningococcal disease incidence in Catalonia (Spain) 24 months after a mass vaccination programme of children and young people. J. Epidemiol. Community Health 2001, 55, 283–287. [Google Scholar] [CrossRef] [Green Version]
- Garrido-Estepa, M.; León-Gómez, I.; Herruzo, R.; Cano, R. Changes in meningococcal C epidemiology and vaccine effectiveness after vaccine introduction and schedule modification. Vaccine 2014, 32, 2604–2609. [Google Scholar] [CrossRef]
- Ordóñez-León, G.Y.; Martínez, E.V.; Herruzo, R.; Garrido-Estepa, M. Updating information about the burden of meningococcal disease hospitalisations in Spain. J. Vaccines Res. Vaccin. 2016, 2, 3. [Google Scholar]
- Fernández, S.; Arreaza, L.; Santiago, I.; Malvar, A.; Berrón, S.; Vazquez, J.A.; Hervada, X.; Gestal, J.J. Carriage of a new epidemic strain of Neisseria meningitidis and its relationship with the incidence of meningococcal disease in Galicia, Spain. Epidemiol. Infect. 1999, 123, 349–357. [Google Scholar] [CrossRef]
- Cardeñosa, N.; Domínguez, A.; Orcau, A.; Pañella, H.; Godoy, P.; Minguell, S.; Camps, N.; Vázquez, J. Carriers of Neisseria meningitidis in household contacts of meningococcal disease cases in Catalonia (Spain). Eur. J. Epidemiol. 2001, 17, 877–884. [Google Scholar] [CrossRef]
- Arteagoitia Axpe, J.M.; García Calabuig, M.A. I Encuesta de Seroprevalencia de la Comunidad Autónoma del País Vasco; Dirección de Salud Publica, Departamento de Sanidad y Consumo: Pais Vasco, Spain, 2011. [Google Scholar]
- Grupo de trabajo MenB Ponencia de Programa y Registro de Vacunaciones. Vacuna Frente a Enfermedad Meningocócica Invasora por Serogrupo B y su Posible Utilización en Salud Pública, Junio de 2013; Ministerio de Sanidad, Servicios Sociales e Igualida: Madrid, Spain, 2015.
- Trotter, C.L.; Edmunds, W.J. Reassessing the cost-effectiveness of meningococcal serogroup C conjugate (MCC) vaccines using a transmission dynamic model. Med. Decis. Mak. Int. J. Soc. Med. Decis. Mak. 2006, 26, 38–47. [Google Scholar] [CrossRef]
- Trotter, C.L.; Gay, N.J.; Edmunds, W.J. Dynamic models of meningococcal carriage, disease, and the impact of serogroup C conjugate vaccination. Am. J. Epidemiol. 2005, 162, 89–100. [Google Scholar] [CrossRef] [Green Version]
- Morgenstern, H. Ecologic studies in epidemiology: Concepts, principles, and methods. Annu. Rev. Pub. Health 1995, 16, 61–81. [Google Scholar] [CrossRef]
- Saunders, C.; Abel, G. Ecological studies: Use with caution. Br. J. Gen. Pract. 2014, 64, 65–66. [Google Scholar] [CrossRef]
- Martinon-Torres, F. Deciphering the Burden of Meningococcal Disease: Conventional and Under-recognized Elements. J. Adolesc. Health Off. Publ. Soc. Adolesc. Med. 2016, 59 (Suppl. 2), S12–S20. [Google Scholar] [CrossRef] [Green Version]
- Grupo de Trabajo de «Uso de 4CMenB en Situaciones Especiales». Recomendaciones de Utilización de la Vacuna Frente a Enfermedad Meningocócica por Serogrupo B; Ministerio de Sanidad, Servicios Sociales e Igualidad: Madrid, Spain, 2015.
- Martinón-Torres, F.; Trilla, A. Meningococcal disease: Can we predict the unpredictable? Med. Clin. (Barc) 2020, 154, 20–22. [Google Scholar] [CrossRef]
- Grupo de trabajo vacunación frente a EMI de la Ponencia de Programa y Registro de Vacunaciones. Recomendaciones de Vacunación Frente a Enfermedad Meningocócica Invasiva; Comisión de Salud Pública del Consejo Interterritorial del Sistema Nacional de Salud. Ministerio de Sanidad: Madrid, Spain, 2019. [Google Scholar]
- Marshall, H.S.; McMillan, M.; Koehler, A.P.; Lawrence, A.; Sullivan, T.R.; MacLennan, J.M.; Maiden, M.C.; Ladhani, S.N.; Ramsay, M.E.; Trotter, C.; et al. Meningococcal B Vaccine and Meningococcal Carriage in Adolescents in Australia. N. Engl. J. Med. 2020, 382, 318–327. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Period | 1998–1999 | 2001–2004 | 2006–2012 | 2014–2017 |
|---|---|---|---|---|
| Vaccination | Pre-routine immunization | Routine immunization of MenC (3p) 1 | Routine immunization of MenC (2p + 1) 1 | Routine immunization of MenC1 (2p + 1 and adolescent booster) |
| Invasive meningococcal disease | ||||
| <1 year | 69.34 | 42.31 | 30.74 | 12.64 |
| 1–14 years | 191.25 | 106.05 | 61.84 | 25.26 |
| 15–64 years | 0.9 | 1.02 | 0.67 | 0.33 |
| >64 years | 1.07 | 1.03 | 0.75 | 0.58 |
| TOTAL | 3.3 | 2.47 | 1.73 | 0.76 |
| Meningococcal meningitis | ||||
| <1 year | 35.66 | 21.9 | 16.7 | 6.9 |
| 1–14 years | 102.24 | 55.48 | 32.24 | 14 |
| 15–64 years | 0.5 | 0.57 | 0.35 | 0.19 |
| >64 years | 0.55 | 0.55 | 0.37 | 0.31 |
| TOTAL | 1.76 | 1.32 | 0.91 | 0.43 |
| Meningococcal sepsis and meningococcemia | ||||
| <1 year | 39.81 | 23.81 | 17.42 | 6.81 |
| 1–14 years | 109.15 | 58.34 | 35.19 | 13.87 |
| 15–64 years | 0.5 | 0.54 | 0.38 | 0.16 |
| >64 years | 0.66 | 0.57 | 0.43 | 0.32 |
| TOTAL | 1.88 | 1.35 | 0.98 | 0.41 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rivero-Calle, I.; Raguindin, P.F.; Pardo-Seco, J.; Martinon-Torres, F. Risk Analysis by Age on the Burden of Meningococcal Disease in Spain. Vaccines 2022, 10, 592. https://doi.org/10.3390/vaccines10040592
Rivero-Calle I, Raguindin PF, Pardo-Seco J, Martinon-Torres F. Risk Analysis by Age on the Burden of Meningococcal Disease in Spain. Vaccines. 2022; 10(4):592. https://doi.org/10.3390/vaccines10040592
Chicago/Turabian StyleRivero-Calle, Irene, Peter Francis Raguindin, Jacobo Pardo-Seco, and Federico Martinon-Torres. 2022. "Risk Analysis by Age on the Burden of Meningococcal Disease in Spain" Vaccines 10, no. 4: 592. https://doi.org/10.3390/vaccines10040592