
Inclusive Education for Health: Analysis of the Mandatory Nature of Vaccination and Its Regulation by Administrations, and Implications and Considerations for Vaccination against COVID

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population and Sample
2.2. Instrument
2.3. Variables
- Sex—dichotomous independent variable with 2 possibilities: male and female.
- Age—polytomous independent variable with 4 possibilities: less than 30, between 30 and 44, between 45 and 59, greater than 60.
- Sector—polytomous independent variable with 3 possibilities: health, education, economy.
- Country—polytomous independent variable with 76 possibilities: Albania, Germany, Andorra, Angola, Saudi Arabia, Algeria, Argentina, Australia, Austria, Bangladesh, Belgium, Bolivia, Bosnia–Herzegovina, Botswana, Brazil, Bulgaria, Cape Verde, Cameroon, Canada, Chile, China, Cyprus, Colombia, Ivory Coast, Cuba, Denmark, Ecuador, United Arab Emirates, Spain, U.S.A., Estonia, Philippines, Finland, France, Gabon, Gambia, Georgia, Greece, Guatemala, Equatorial Guinea, Haiti, Honduras, India, Ireland, Iceland, Israel, Italy, Jamaica, Japan, Jordan, Latvia, Lebanon, Liberia, Luxembourg, Morocco, Mauritius, Mauritania, Mexico, Montenegro, Mozambique, Paraguay, Peru, Poland, Portugal, United Kingdom, Russia, South Africa, Sweden, Switzerland, Thailand, Tanzania, Turkey, Ukraine, Uganda, Venezuela, Zimbabwe.
- Human Development Index (HDI)—polytomous independent variable with 4 possibilities: very high, high, medium, low.
- Continent—polytomous independent variable with 5 possibilities: Europe, America, Asia, Africa, Oceania.
2.4. Procedure
2.5. Data Analysis
3. Results
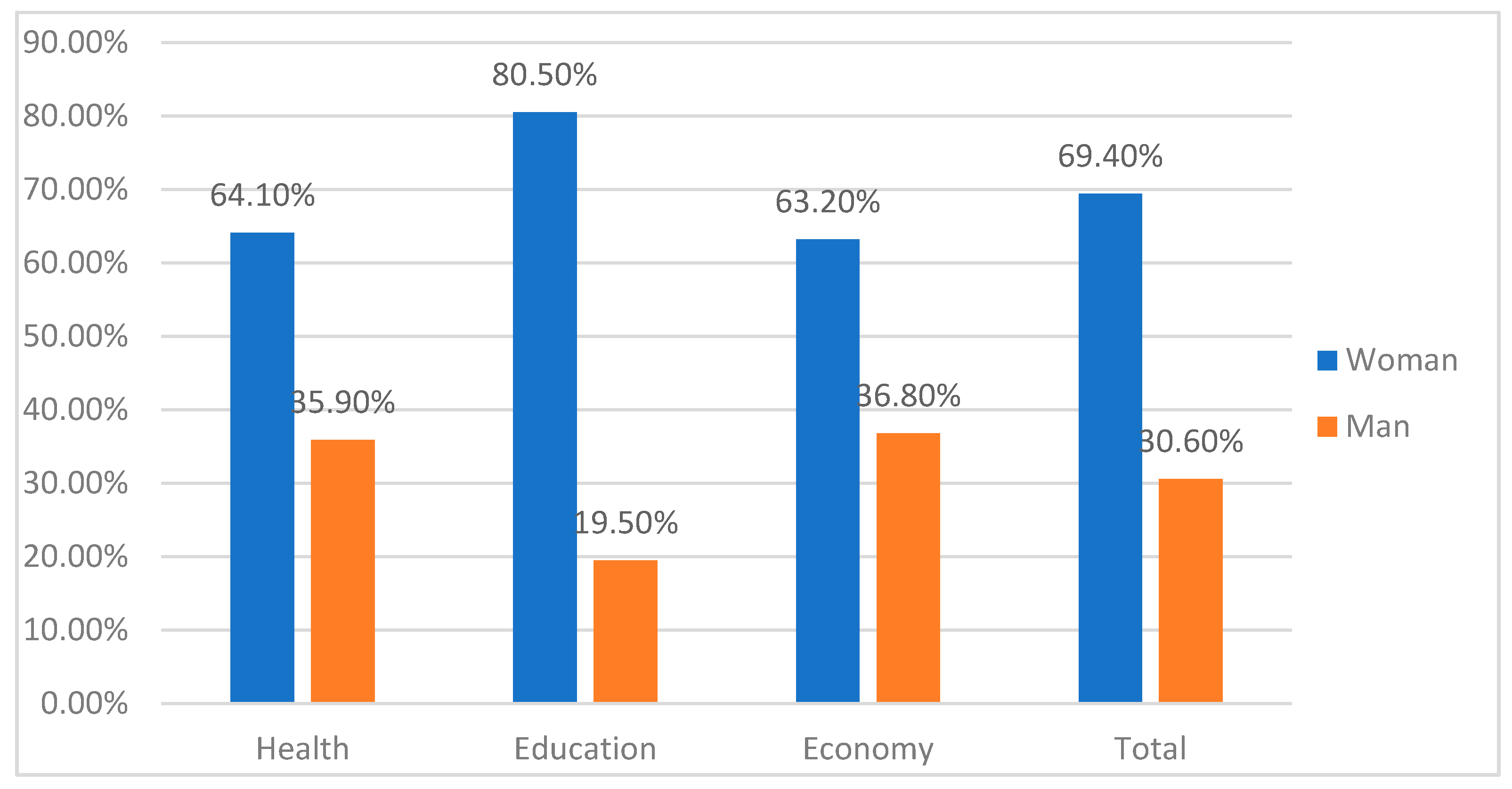
3.1. Analysis of the Incidence of Sex
3.2. Analysis of the Incidence of Age
3.3. Analysis of the Incidence of Sector
3.4. Analysis of the Incidence by Human Development Index (HDI)
3.5. Analysis of the Incidence by Continent
3.6. Analysis of the Incidence by Country
3.7. Correlational Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gothefors, L. El impacto de las vacunas en países con bajos ingresos y países con altos ingresos. Ann. Nestlé 2008, 66, 55–69, 517. [Google Scholar] [CrossRef]
- García-Toledano, E.; Palomares-Ruiz, A.; Cebrián-Martínez, A.; López-Parra, E. Obligatoriedad de la vacunación y su incidencia en la comunidad educativa. In Educar y Forma A la Generación Z: Experiencias Derivadas de la Investigación; Trujillo, J.M., Cáceres, M.P., Marín, J.A., Moreno, A.J., Eds.; Octaedro: Barcelona, Spain, 2021; pp. 89–102. [Google Scholar]
- World Health Organization @WHO. Media Briefing on #COVID19 with @DrTedros. #coronavirus. Available online: https://twitter.com/WHO/status/1237774421307228160 (accessed on 11 March 2020).
- Urbiztondo, L.; Borràs, E.; Mirada, G. Coronavirus vaccines. Vacunas 2020, 21, 69–72. [Google Scholar] [CrossRef] [PubMed]
- Casino, G.; Horstmann, L.; Juste, P. Las Vacunas En España. Situación Actual Y Perspectivas De Futuro; Deloitte: Barcelona, Spain, 2018; pp. 1–125. Available online: https://www2.deloitte.com/content/dam/Deloitte/es/Documents/sanidad/Deloitte-ES-sanidad-estudio-vacunas-2017.pdf (accessed on 3 February 2021).
- Thomas, N.H.; Thomas, H.; David, H. Global Alliance for Vaccines and Immunization. In Immunization and the Sustainable Development Goals; GAVI: Geneva, Switzerland, 2019; Available online: https://bit.ly/3sbphd7 (accessed on 29 June 2021).
- European Commission. European Pillar of Social Rights; European Commission: Brussels, Belgium, 2017. [Google Scholar] [CrossRef]
- Ramos, F. El Pilar Europeo De Derechos Sociales. La Última Oportunidad Para La Europa Social; Fundación Alternativas: Madrid, Spain, 2018; Available online: https://www.fundacionalternativas.org/public/storage/fundacion_documentos_archivos/78475dc8e0e318bab051e4e75f076082.pdf (accessed on 29 June 2021).
- United Nations Educational Scientific and Cultural Organization. Education 2030: Incheon Declaration and Framework for Action for the Implementation of Sustainable Development Goal 4: Ensure Inclusive and Equitable Quality Education and Promote Lifelong learning Opportunities for All; UNESCO: Paris, France, 2016; Available online: https://unesdoc.unesco.org/ark:/48223/pf0000245656 (accessed on 28 June 2021).
- World Health Organization. Vaccine Hesitancy: A Growing Challenge for Immunization Programmes; World Health Organization: Geneve, Switzerland, 2015; Available online: https://www.who.int/news/item/18-08-2015-vaccine-hesitancy-a-growing-challenge-for-immunization-programmes (accessed on 30 July 2021).
- De Lorenzo, R. Responsabilidad porno vacunación. Redacción Médica. 2013. Available online: https://www.redaccionmedica.com/opinion/ricardo-de-lorenzo/responsabilidad-por-no-vacunacion-7037 (accessed on 28 June 2021).
- Agencia Española de Medicamentos y Productos Sanitarios. Vacunas COVID-19. Informe De Farmacovigilancia; AEMPS: Madrid, Spain, 2021. Available online: https://www.aemps.gob.es/laAEMPS/docs/informe-farmacovigilancia-marzo-2021.pdf?x10382 (accessed on 25 July 2021).
- Ministry of Health; Ministry of Education and Vocational Training. Medidas de Prevención, Higiene y Promoción de la Salud Frente a COVID-19 Para Centros EDUCATIVOS en el Curso 2020–2021; Government of Spain: Madrid, Spain, 2021. Available online: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/documentos/COVID19_16.03.2021_Medidas_centros_educativos_Curso_2020_2021.pdf (accessed on 29 May 2021).
- Martínez-Santos, A.E.; Tizón-Bouza, E.; Fernández-Morante, C.; Casal-Otero, L.; Cebreiro, B. La enfermería escolar: Contenidos y percepciones sobre su pertinencia en las escuelas inclusivas. Enferm. Glob. 2019, 18, 291–323. [Google Scholar] [CrossRef]
- Delgado, T.; Hernández, N.; Martínez, S.; Ruiz, B.; Gargallo, J.; Mallén, S. La figura de la enfermera escolar. Rev. Sanit. Inves. [online] 2021, 2. Available online: https://www.revistasanitariadeinvestigacion.com/la-figura-de-la-enfermera-escolar (accessed on 23 June 2021).
- ElDiario.es. Letonia autoriza el despido de trabajadores que se nieguen a vacunarse contra la COVID-19. Available online: https://www.eldiario.es/sociedad/ultima-hora-coronavirus-actualidad-politica-4-noviembre_6_8457842_1080721.html (accessed on 5 November 2021).
- BBC News Mundo. COVID-19: Costa Rica se Convierte en el Primer País que Hace Obligatoria la Vacuna Para Niños. Available online: https://www.bbc.com/mundo/noticias-america-latina-59188277 (accessed on 7 November 2021).
- Cruz, M.; Rodríguez, A.; Hortal, J.; Padilla, J. Reticencia vacunal: Análisis del discurso de madres y padres con rechazo total o parcial a las vacunas. Gac. Sanit. 2019, 33, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Gallè, F.; Sabella, E.; Roma, P.; De Giglio, O.; Caggiano, G.; Tafuri, S.; Da Molin, G.; Ferrcuti, S.; Montagna, M.T.; Liguori, G.; et al. Napoli, Christian. Knowledge and Acceptance of COVID-19 Vaccination among Undergraduate Students from Central and Southern Italy. Vaccines 2021, 9, 638. [Google Scholar] [CrossRef] [PubMed]
- Quintero, E.; De la Mella, S.; Gómez, L. La promoción de la salud y su vínculo con la prevención primaria. Mediocent. Electron. 2017, 21, 101–111. Available online: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S102930432017000200003&lng=es (accessed on 21 May 2021).
- Hernández-Sarmiento, J.M.; Jaramillo-Jaramillo, L.; Villegas-Alzate, J.; Álvarez-Hernández, L.; Roldán-Tabares, M.; Ruiz-Mejía, C.; Calle-Estrada, M.; Ospina-Jiménez, M.; Martínez-Sánchez, L. Health education as an important promotion and prevention strategy. Arch. Med. 2020, 20, 490–504. [Google Scholar] [CrossRef]
- Rodríguez Torres, Á.F.; Rodríguez Alvear, J.C.; Guerrero, H.I.; Arias, E.R.; Paredes, A.E.; Chávez, V.A. Beneficios de la actividad física para niños y adolescentes en el contexto escolar. Rev. Cub. Medic. Gen. Integ. 2020, 36, e1535. Available online: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0864-21252020000200010 (accessed on 23 June 2021).
- Van der Heide, I.; Wang, J.; Droomers, M.; Spreeuwenberg, P.; Rademakers, J.; Uiters, E. The relationship between health, education, and health literacy: Results from the Dutch Adult Literacy and Life Skills Survey. J. Health Commun. 2013, 18, 172–184. [Google Scholar] [CrossRef] [Green Version]
- Díaz, Y.; Pérez, J.L.; Báez, F.; Conde, M. Generalidades sobre promoción y educación para la salud. Rev. Cubana Med. Gen. Integr. 2012, 28, 299–308. Available online: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S0864-21252012000300009 (accessed on 5 February 2021).
- García-Toledano, E.; Palomares-Ruiz, A.; Cebrián-Martínez, A.; López-Parra, E. Design and validation of an instrument for evaluating training and education of health and proper use of vaccines “VACUNASEDUCA”. Int. J. Environ. Res. Public Health 2021, 18, 7321. [Google Scholar] [CrossRef] [PubMed]
- Kerlinger, F.N.; Lee, H.B. Investigación del Comportamiento, 4th ed.; Pineda, L., Mora, T.I., Eds.; McGraw-Hill-Interamericana: Ciudad de México, México, 2002. [Google Scholar]
- Pelea, L.P. ¿Cómo proceder ante el incumplimiento de las premisas de los métodos paramétricos? O ¿cómo trabajar con variables biológicas no normales? Rev. Jardín Botánico Nac. 2018, 39, 1–12. Available online: https://www.jstor.org/stable/26600674 (accessed on 22 July 2021).
- Ledesma, R. Introducción al Bootstrap. Desarrollo de un ejemplo acompañado de software de aplicación. Tutor. Quantit. Meth. Psych. 2008, 4, 51–60. [Google Scholar] [CrossRef]
- Simon, J.L.; Bruce, P. Resampling: A Tool for Everyday Statistical Work. Chance 1991, 4, 22–32. [Google Scholar] [CrossRef]
- Simon, J.L. Resampling: The New Statistics; Resampling Stats: Arlington, VA, USA, 1997. [Google Scholar]
- Chernick, M.R. Bootstrap Methods: A Guide for Practitioners and Researchers, 2nd ed.; Wiley and Sons: Hoboken, NJ, USA, 2008f. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Science; Academic Press: New York, NY, USA, 1977. [Google Scholar] [CrossRef]
- Martínez, M.; Rodríguez, I.; Velásquez, G. Infancia Confinada ¿Cómo Vive La Situación De Confinamiento Niñas, Niños y Adolescentes? Enclave: Madrid, Spain, 2020; Available online: https://www.observatoriodelainfancia.es/ficherosoia/documentos/7073_d_informe-infancia-confinada.pdf (accessed on 21 May 2021).
- Bartlett, J.; Griffin, J.; Thomson, D. Resources for Supporting Children’s Emotional Well-Being during the COVID-19 Pandemic; Child Trends: 2020. Available online: https://www.childtrends.org/publications/resources-for-supporting-childrens-emotional-well-being-during-the-covid-19-pandemic (accessed on 23 July 2021).
- Dalton, L.; Rapa, E.; Stein, A. Protecting the psychological health of children through effective communication about COVID-19. Lancet Child Adolesc. Health 2020, 4, 346–347. [Google Scholar] [CrossRef]
- Gómez-Luna, L.M. El desafío ambiental: Enseñanzas a partir de la COVID-19. Rev. Med. Sant. Cuba 2020, 24, 728–742. Available online: http://www.medisan.sld.cu/index.php/san/article/view/3188 (accessed on 24 June 2021).
- Cabana, J.; Pedra, C.; Ciruzzi, M.S.; Garategaray, M.; Cutri, A.; Lorenzo, C. Percepciones y Sentimientos De Niños Argentinos Frente A La Cuarentena COVID-19. Resultados Preliminares; Sociedad Argentina de Pediatría: Buenos Aires, Argentina, 2020; Available online: https://www.sap.org.ar/uploads/archivos/general/files_doc-percepciones-y-sentimientos-de-ninos-argentinos-frente-a-la-cuarentena-covid-19_1606056649.pdf (accessed on 28 July 2021).
- Erades, N.; Morales, A. Impacto psicológico del confinamiento por la COVID-19 en niños españoles: Un estudio transversal. Rev. Psicol. Clin. Niños Adolesc. 2020, 7, 27–34. [Google Scholar] [CrossRef]
- United Nations International Children’s Emergency Fund. Encuesta COVID-19. Encuesta De Percepción y Actitudes de la Población. Impacto de la Pandemia COVID-19 y Las Medidas Adoptadas Por el Gobierno Sobre la Vida Cotidiana; UNICEF Argentina: Buenos Aires, Argentina, 2020; Available online: https://www.unicef.org/argentina/media/8056/file/Covid19-EncuestaRapidaInformeEducacion.pdf (accessed on 7 May 2021).
- Valadez, M.D.; López-Aymes, G.; Ruvalcaba, N.A.; Flores, F.; Ortiz, G.; Rodríguez, C.; Borges, Á. Emotions and reactions to the confinement by COVID-19 of children and adolescents with high abilities and community samples: A mixed methods research study. Front. Psychol. 2020, 11, 1–14. [Google Scholar] [CrossRef]
- Navarro, I.; Real-Fernández, M.; Juárez, R.; Costa-López, B.; Sánchez, M.; Lavigne, R. Consequences of Confinement due to COVID-19 in Spain on Anxiety, sleep and executive functioning of children and adolescents with ADHD. Sustainability 2021, 13, 2487. [Google Scholar] [CrossRef]
- De Alba-Villegas, E.; Castro-Gámez, T.; Corona-Padilla, S.; González-Suárez, H.; Valadez-Sierra, M.D. Comparación de la calidad de vida en niños con trastorno por déficit de la atención e hiperactividad y niños con altas capacidades ante el confinamiento por COVID-19. Talincrea 2021, 7, 52–58. Available online: http://www.talincrea.cucs.udg.mx/sites/default/files/adjuntos/07_14/08_comparacion.pdf (accessed on 14 October 2021).
- Zhang, J.; Shuai, L.; Yu, H.; Wang, Z.; Qiu, M.; Lu, L.; Cao, X.; Xia, W.; Wang, Y.; Chen, R. Acute stress, behavioural symptoms and mood states among school-age children with attention-deficit/hyperactive disorder during the COVID-19 outbreak. Asian J. Psych. 2020, 51, 102077. [Google Scholar] [CrossRef]
- Baweja, R.; Brown, S.L.; Edwards, E.M.; Murray, M.J. COVID-19 Pandemic and Impact on Patients with Autism Spectrum Disorder. J. Autism Dev. Disord. 2021, 10, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Amend, E.R.; Koehler, J.; Peters, M.P.; Joerg, M.; Nilles, K. Supporting Your Gifted Child during COVID-19. National Association for Gifted Children. Available online: https://www.nagc.org/sites/default/files/Publication%20PHP/NAGC_TIP-Sheet_COVID-19_With%20Strategies%20by%20Development%20Level_April%202020.pdf (accessed on 20 July 2021).
- López-Aymes, G.; Valadez, M.D.; Rodríguez-Naveiras, E.; Castellanos-Simons, D.; Aguirre, T.; Borges, Á. A mixed methods research study of parental perception of physical activity and quality of life of children under home lock down in the COVID-19 pandemic. Front. Psychol. 2021, 12, 649481. [Google Scholar] [CrossRef]
- Cross, J.R.; Cross, T.L. Clinical and mental health issues in counseling the gifted individual. J. Couns. Dev. 2015, 93, 163–172. [Google Scholar] [CrossRef] [Green Version]
- Duraku, H.Z.; Hoxha, N. The impact of COVID-19, school closure, and social isolation on gifted students’ wellbeing and attitudes toward remote (online) learning. In Impact of the COVID-19 Pandemic on Education and Wellbeing; Duraku, Z.H., Ed.; University of Prishtina “Hasan Prishtina”: Pristina, Kosovo, 2020; pp. 130–169. Available online: https://cutt.ly/MUDieJc (accessed on 24 May 2021).
- Ducoing, W. Una expresión de la desigualdad en educación básica durante la emergencia sanitaria: El caso de una alumna. In Educación y Pandemia: Una Visión Académica; Casanova, H., Ed.; Universidad Autónoma de México: Ciudad de México, México, 2020; pp. 55–64. Available online: http://132.248.192.241:8080/xmlui/bitstream/handle/IISUE_UNAM/539/DucoingP_2020_Una_expresi%C3%B3n_de_la_desigualdad.pdf?sequence=1&isAllowed=y (accessed on 24 May 2021).
- Quiroz-Reyes, C. Pandemia COVID-19 e inequidad territorial: El agravamiento de las desigualdades en Chile. Rev. Intern. Educ. Justicia Soc. 2020, 9, 1–6. Available online: https://revistas.uam.es/riejs/article/view/12143 (accessed on 25 May 2021).
- Matesanz, R. Vacunas Anti-COVID: Lo individual frente a lo colectivo. Redac. Méd. 2021. Available online: https://www.redaccionmedica.com/opinion/rafael-matesanz/vacunas-anti-covid-lo-individual-frente-a-lo-colectivo-4492 (accessed on 7 May 2021).
- Javierre, A.P.; Álvarez, M.J. Reticencia vacunal: Argumentos y consejos para confrontar las dudas sobre las vacunas. Form. Méd. Contin. Atenc. Prim. 2021, 28, 36–45. [Google Scholar] [CrossRef]
- Aquino-Canchari, C.; Guillen, K. Vaccine refusal as an increasing most frequent practice in the world. Rev. Cub. Investig. Biomed. 2020, 39, e406. Available online: https://www.medigraphic.com/pdfs/revcubinvbio/cib-2020/cib201b.pdf (accessed on 22 July 2021).
- Fernández-Niño, J.; Baquero, H. El movimiento anti-vacunas y la anti-ciencia como amenaza para la Salud Pública. Salud UIS 2019, 51, 103–106. [Google Scholar] [CrossRef]
- Pan American Health Organization. Educación Para la Salud Con Enfoque Integral; Pan American Health Organization: Washington, DC, USA, 2017; Available online: https://www.paho.org/hq/dmdocuments/2017/promocion-salud-intersectorialidad-concurso-2017-educacion.pdf (accessed on 24 June 2021).


{kind=link}
| Dimensions | Items |
|---|---|
| D1 = Awareness and regulation | 1–2 |
| D2 = Education and teachers | 3–4 to 5–6 |
| D3 = Regulation and obligation | 7–8 |
| D4 = Consequences and risks | 9–10–11–12 |
| Scale (n) | 95% CI | 95% CI | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Dimension (D) | Item | 1 | 2 | 3 | n | M | Lower | Upper | SD | Lower | Upper |
| P01 | 26 | 174 | 800 | 1000 | 2.77 | 2.75 | 2.80 | 0.48 | 0.44 | 0.51 | |
| P02 | 14 | 132 | 854 | 1000 | 2.84 | 2.81 | 2.86 | 0.40 | 0.37 | 0.44 | |
| D1 = Awareness and regulation | D1t | 2.81 | 2.78 | 2.83 | 0.36 | 0.34 | 0.38 | ||||
| P03 | 34 | 131 | 835 | 1000 | 2.80 | 2.77 | 2.83 | 0.48 | 0.44 | 0.52 | |
| P04 | 27 | 152 | 821 | 1000 | 2.79 | 2.77 | 2.82 | 0.47 | 0.43 | 0.50 | |
| P05 | 35 | 139 | 826 | 1000 | 2.79 | 2.76 | 2.82 | 0.49 | 0.44 | 0.52 | |
| P06 | 35 | 74 | 891 | 1000 | 2.86 | 2.83 | 2.88 | 0.44 | 0.40 | 0.49 | |
| D2 = Education and teachers | D2t | 2.81 | 2.79 | 2.83 | 0.31 | 0.28 | 0.33 | ||||
| P07 | 616 | 183 | 201 | 1000 | 1.59 | 1.53 | 1.64 | 0.80 | 0.78 | 0.83 | |
| P08 | 701 | 240 | 59 | 1000 | 1.36 | 1.32 | 1.40 | 0.59 | 0.56 | 0.62 | |
| D3 = Regulation and obligation | D3t | 1.47 | 1.44 | 1.51 | 0.59 | 0.56 | 0.61 | ||||
| P09 | 791 | 174 | 35 | 1000 | 1.24 | 1.21 | 1.28 | 0.50 | 0.47 | 0.54 | |
| P10 | 828 | 149 | 23 | 1000 | 1.20 | 1.17 | 1.22 | 0.45 | 0.41 | 0.48 | |
| P11 | 840 | 143 | 17 | 1000 | 1.18 | 1.15 | 1.20 | 0.42 | 0.39 | 0.46 | |
| P12 | 836 | 147 | 17 | 1000 | 1.18 | 1.16 | 1.21 | 0.43 | 0.39 | 0.46 | |
| D4 = Consequences and risks | D4t | 1.20 | 1.18 | 1.23 | 0.41 | 0.37 | 0.44 | ||||
| Total | S3t | 2.05 | 2.04 | 2.06 | 0.22 | 0.20 | 0.23 | ||||
| SEX | ||||||||
|---|---|---|---|---|---|---|---|---|
| Man n = 306 = 30.6% | Woman n = 694 = 69.4% | |||||||
| Dimension (D) | Item | 1 | 2 | 3 | 1 | 2 | 3 | n |
| D3 = Regulation and obligation | P07 | 157 | 60 | 89 | 459 | 123 | 112 | 1000 |
| P08 | 193 | 87 | 26 | 508 | 153 | 33 | 1000 | |
| Man | 95% CI | Woman | 95% CI | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Dimension (D) | Item | M | Lower-Upper | SD | Lower-Upper | M | Lower-Upper | SD | Lower-Upper | F | p | Eta2 | Direction |
| P07 | 1.78 | 1.68–1.88 | 0.87 | 0.83–0.90 | 1.50 | 1.44–1.56 | 0.76 | 0.72–0.79 | 26.02 | <0.01 | 0.03 | W < M | |
| P08 | 1.45 | 1.39–1.53 | 0.65 | 0.59–0.70 | 1.32 | 1.28–1.36 | 0.56 | 0.52–0.60 | 11.86 | <0.01 | 0.01 | W < M | |
| D3 = Regulation and obligation | D3t | 1.62 | 1.55–1.69 | 0.64 | 0.60–0.68 | 1.41 | 1.37–1.45 | 0.55 | 0.52–0.58 | 27.17 | <0.01 | 0.03 | W < M |
| AGE | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Less than 30 n = 363 = 36.3% | Between 30 and 44 n = 348 = 34.8% | Between 45 and 59 n = 267 = 26.76% | Greater than 60 n = 22 = 2.2% | |||||||||||
| Dimension (D) | 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 | n | |
| D3 = Regulation and obligation | P07 | 297 | 26 | 40 | 188 | 83 | 77 | 120 | 71 | 76 | 11 | 3 | 8 | 1000 |
| P08 | 315 | 36 | 12 | 232 | 94 | 22 | 141 | 102 | 24 | 13 | 8 | 1 | 1000 | |
| Item | M | E1 = <30 L-U | SD | 95% CI | M | E2 = 30–44 L-U | SD | 95% CI | p | Eta2 | Direction |
|---|---|---|---|---|---|---|---|---|---|---|---|
| P07 | 1.29 | 1.22–1.36 | 0.65 | 0.58–0.72 | 1.68 | 1.60–1.77 | 0.81 | 0.77–0.85 | 0.00 | 0.08 | E1 < E2.E3 |
| P08 | 1.17 | 1.12–1.21 | 0.45 | 0.38–0.52 | 1.40 | 1.33–1.46 | 0.61 | 0.55–0.65 | 0.00 | 0.07 | E1 < E2 < E3 |
| D3t | 1.23 | 1.18–1.28 | 0.46 | 0.40–0.51 | 1.54 | 1.48–1.60 | 0.59 | 0.55–0.62 | 0.00 | 0.11 | E1 < E2 < E3.E4 |
| Item | M | E3 = 45–59 L-U | SD | 95% CI | M | E4 = >60 L-U | SD | 95% CI | p | Eta2 | Direction |
| P07 | 1.84 | 1.73–1.93 | 0.84 | 0.80–0.87 | 1.86 | 1.45–2.29 | 0.94 | 0.76–1.00 | 0.00 | 0.08 | E1 < E2.E3 |
| P08 | 1.56 | 1.48–1.64 | 0.65 | 0.60–0.70 | 1.45 | 1.22–1.73 | 0.60 | 0.43–0.75 | 0.00 | 0.07 | E1 < E2 < E3 |
| D3t | 1.70 | 1.62–1.78 | 0.63 | 0.59–0.67 | 1.66 | 1.39–1.96 | 0.64 | 0.48–0.77 | 0.00 | 0.11 | E1 < E2 < E3.E4 |
| Sector | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Health n = 554 = 55.4% | Education n = 329 = 32.9% | Economy n = 117 = 11.7% | |||||||||
| Dimension (D) | Item | 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 | n |
| D3 = Regulation and obligation | P07 | 302 | 123 | 129 | 255 | 32 | 42 | 59 | 28 | 30 | 1000 |
| P08 | 356 | 159 | 39 | 279 | 44 | 6 | 66 | 37 | 14 | 1000 | |
| Item | M | Health L-U | SD | 95% CI L-U | p | Eta2 | Direction |
|---|---|---|---|---|---|---|---|
| P07 | 1.69 | 1.62–1.76 | 0.83 | 0.79–0.85 | 0.00 | 0.04 | S2 > S1.S3 |
| P08 | 1.43 | 1.38–1.48 | 0.62 | 0.58–0.66 | 0.00 | 0.05 | S2 > S1.S3 |
| D3t | 1.56 | 1.51–1.61 | 0.60 | 0.57–0.63 | 0.00 | 0.06 | S2 > S1.S3 |
| Item | M | Education L-U | SD | 95% CI L-U | p | Eta2 | Direction |
| P03 | 1.35 | 1.28–1.43 | 0.70 | 0.62–0.76 | 0.00 | 0.04 | S2 > S1.S3 |
| P04 | 1.17 | 1.13–1.22 | 0.42 | 0.36–0.48 | 0.00 | 0.05 | S2 > S1.S3 |
| D3t | 1.26 | 1.21–1.31 | 0.47 | 0.42–0.52 | 0.00 | 0.06 | S2 > S1.S3 |
| Item | M | Economy L-U | SD | 95% CI L-U | p | Eta2 | Direction |
| P03 | 1.75 | 1.60–1.91 | 0.84 | 0.77–0.89 | 0.00 | 0.04 | S2 > S1.S3 |
| P04 | 1.56 | 1.43–1.68 | 0.70 | 0.61–0.77 | 0.00 | 0.05 | S2 > S1.S3 |
| D3t | 1.65 | 1.53–1.77 | 0.66 | 0.59–0.72 | 0.00 | 0.06 | S2 > S1.S3 |
| HDI | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Very high n = 873 = 87.3% | High n = 85 = 8.5% | Medium n = 31 = 3.1% | Low n = 11 = 1.1% | |||||||||||
| Dimension (D) | 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 | n | |
| D3 = Regulation and obligation | P07 | 564 | 157 | 152 | 36 | 18 | 31 | 14 | 4 | 13 | 2 | 4 | 5 | 1000 |
| P08 | 638 | 190 | 45 | 37 | 38 | 10 | 21 | 6 | 4 | 5 | 6 | 0 | 1000 | |
| Item | M | Very high L-U | SD | 95% CI L-U | M | High L-U | SD | 95% CI L-U | p | Eta2 | Direction |
|---|---|---|---|---|---|---|---|---|---|---|---|
| P07 | 1.53 | 1.48–1.58 | 0.77 | 0.74–0.80 | 1.94 | 1.74–2.13 | 0.89 | 0.83–0.94 | 0.00 | 0.04 | I1 < I2 < I3 < I4 |
| P08 | 1.32 | 1.28–1.36 | 0.57 | 0.53–0.61 | 1.68 | 1.54–1.83 | 0.68 | 0.58–0.75 | 0.00 | 0.03 | I1 < I3 < I4 < I2 |
| D3t | 1.42 | 1.39–1.47 | 0.57 | 0.54–0.60 | 1.81 | 1.68–1.94 | 0.60 | 0.53–0.66 | 0.00 | 0.05 | I1 < I3 < I2 < I4 |
| Item | M | Medium L-U | SD | 95% CI L-U | M | Low L-U | SD | 95% CI L-U | p | Eta2 | Direction |
| P07 | 1.97 | 1.65–2.29 | 0.95 | 0.84–1.00 | 2.27 | 1.80–2.73 | 0.79 | 0.45–0.98 | 0.00 | 0.04 | I1 < I2 < I3 < I4 |
| P08 | 1.45 | 1.22–1.70 | 0.72 | 0.51–0.87 | 1.55 | 1.25–1.86 | 0.52 | 0.38–0.55 | 0.00 | 0.03 | I1 < I3 < I4 < I2 |
| D3t | 1.71 | 1.50–1.92 | 0.62 | 0.48–0.72 | 1.91 | 1.55–2.25 | 0.58 | 0.32–0.71 | 0.00 | 0.05 | I1 < I3 < I2 < I4 |
| Continent | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Europe n = 830 = 83% | America n = 93 = 9.3% | Asia n = 40 = 4% | Africa n = 35 = 3.5% | Oceania n = 2 = 2% | |||||||||||||
| Dimension (D) | 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 | n | |
| D3 = Regulation and obligation | P07 | 558 | 146 | 126 | 29 | 24 | 40 | 14 | 5 | 21 | 14 | 8 | 13 | 1 | 0 | 1 | 1000 |
| P08 | 624 | 169 | 37 | 38 | 43 | 12 | 18 | 14 | 8 | 20 | 14 | 1 | 1 | 0 | 1 | 1000 | |
| Item | M | Europe L-U | SD | 95% CI L-U | M | America L-U | SD | 95% CI L-U | p | Eta2 | Direction |
|---|---|---|---|---|---|---|---|---|---|---|---|
| P07 | 1.48 | 1.43–1.53 | 0.74 | 0.71–0.78 | 2.12 | 1.94–2.29 | 0.86 | 0.79–0.91 | 0.00 | 0.09 | C1 < C2.C3.C4 |
| P08 | 1.29 | 1.26–1.33 | 0.54 | 0.51–0.58 | 1.72 | 1.59–1.86 | 0.68 | 0.60–0.75 | 0.00 | 0.07 | C1 < C2.C3 |
| D3t | 1.39 | 1.35–1.42 | 0.54 | 0.51–0.57 | 1.92 | 1.80–2.05 | 0.64 | 0.56–0.69 | 0.00 | 0.11 | C1 < C2.C3.C4 |
| Item | M | Asia L-U | SD | 95% CI L-U | M | Africa L-U | SD | 95% CI L-U | p | Eta2 | Direction |
| P07 | 2.18 | 1.87–2.45 | 0.93 | 0.83–0.98 | 1.97 | 1.68–2.29 | 0.89 | 0.78–0.96 | 0.00 | 0.09 | C1 < C2.C3.C4 |
| P08 | 1.75 | 1.51–2.00 | 0.78 | 0.63–0.87 | 1.46 | 1.27–1.66 | 0.56 | 0.46–0.66 | 0.00 | 0.07 | C1 < C2.C3 |
| D3t | 1.96 | 1.74–2.15 | 0.64 | 0.52–0.74 | 1.71 | 1.51–1.92 | 0.60 | 0.51–0.66 | 0.00 | 0.11 | C1 < C2.C3.C4 |
| Number of Respondents by Country | |||||||
|---|---|---|---|---|---|---|---|
| Country | n | Country | n | Country | n | Country | n |
| Albania | 3 | Chile | 4 | Guatemala | 3 | Mexico | 10 |
| Germany | 28 | China | 6 | Guinea Equatorial | 4 | Montenegro | 2 |
| Andorra | 2 | Cyprus | 4 | Haiti | 1 | Mozambique | 1 |
| Angola | 5 | Colombia | 13 | Honduras | 2 | Paraguay | 2 |
| Arabia Saudi | 4 | Ivory Coast | 2 | India | 6 | Peru | 2 |
| Argelia | 2 | Cuba | 3 | Ireland | 9 | Poland | 1 |
| Argentina | 6 | Denmark | 8 | Islandic | 2 | Portugal | 19 |
| Australia | 2 | Ecuador | 6 | Israel | 3 | United Kingdom | 21 |
| Austria | 6 | United Arab Emirates | 1 | Italy | 27 | Russia | 2 |
| Bangladesh | 2 | Spain | 596 | Jamaica | 3 | South Africa | 3 |
| Belgium | 6 | USA | 17 | Japan | 4 | Sweden | 2 |
| Bolivia | 5 | Estonia | 1 | Jordanian | 2 | Switzerland | 11 |
| Bosnia- Herzegovina | 1 | Philippines | 5 | Leetonia | 1 | Thailand | 3 |
| Botswana | 1 | Finland | 4 | Lebanon | 3 | Tanzania | 1 |
| Brazil | 8 | France | 49 | Liberia | 2 | Turkey | 2 |
| Bulgaria | 6 | Gabon | 1 | Luxemburg | 6 | Ukraine | 1 |
| Cape Verde | 1 | Gambia | 1 | Morocco | 1 | Uganda | 2 |
| Cameroon | 4 | Georgia | 2 | Mauritius | 1 | Venezuela | 2 |
| Canada | 6 | Greece | 8 | Mauritania | 1 | Zimbabwe | 3 |
| Dimension (D) | Item | Country | n | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| D3 = Regulation and obligation | Germany n = 28 = 2.8% | Spain n = 596 = 59.6% | France n = 49 = 4.9% | ||||||||
| 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 | |||
| P07 | 12 | 9 | 7 | 454 | 78 | 64 | 20 | 17 | 12 | 673 | |
| P08 | 14 | 11 | 3 | 502 | 87 | 7 | 29 | 16 | 4 | 673 | |
| Italy n = 27 = 2.7% | Portugal n = 19 = 1.9% | United Kingdom n = 59 = 5.9% | |||||||||
| 1 | 2 | 3 | 1 | 2 | 3 | 1 | 2 | 3 | |||
| P07 | 12 | 11 | 4 | 11 | 4 | 4 | 12 | 6 | 3 | 67 | |
| P08 | 15 | 10 | 2 | 11 | 6 | 2 | 15 | 6 | 0 | 67 | |
| U.S.A. n = 17 = 1.7% | |||||||||||
| 1 | 2 | 3 | |||||||||
| P07 | 2 | 3 | 12 | 17 | |||||||
| P08 | 5 | 6 | 6 | 17 | |||||||
| P07 | TOTAL | 757 | |||||||||
| P08 | TOTAL | 757 | |||||||||
| Item | M | Germany L-U | SD | 95% CI L-U | M | Spain L-U | SD | 95% CI L-U | p | Eta2 | Direction |
|---|---|---|---|---|---|---|---|---|---|---|---|
| P07 | 1.821 | 1.50–2.15 | 0.82 | 0.64–0.92 | 1.346 | 1.30–1.40 | 0.66 | 0.61–0.71 | 0.00 | 0.11 | E < R < P < I < A.F < U |
| P08 | 1.607 | 1.36–1.88 | 0.69 | 0.50–0.81 | 1.169 | 1.14–1.20 | 0.41 | 0.36–0.45 | 0.00 | 0.13 | E < R < F < I.P < A < U |
| D3t | 1.714 | 1.45–1.98 | 0.70 | 0.56–0.79 | 1.258 | 1.22–1.29 | 0.44 | 0.40–0.47 | 0.00 | 0.16 | E < R < P < I < F < A < U |
| Item | M | France L-U | SD | 95% CI L-U | M | Italy L-U | SD | 95% CI L-U | p | Eta2 | Direction |
| P07 | 1.837 | 1.62–2.08 | 0.80 | 0.70–0.88 | 1.704 | 1.43–1.97 | 0.72 | 0.56–0.85 | 0.00 | 0.11 | E < R < P < I < A.F < U |
| P08 | 1.490 | 1.32–1.70 | 0.65 | 0.51–0.77 | 1.519 | 1.27–1.77 | 0.64 | 0.46–0.78 | 0.00 | 0.13 | E < R < F < I.P < A < U |
| D3t | 1.663 | 1.50–1.84 | 0.58 | 0.48–0.67 | 1.611 | 1.40–1.84 | 0.56 | 0.40–0.68 | 0.00 | 0.16 | E < R < P < I < F < A < U |
| Item | M | Portugal L-U | SD | 95% CI L-U | M | United Kingdom L-U | SD | 95% CI L-U | p | Eta2 | Direction |
| P07 | 1.632 | 1.27–2.00 | 0.83 | 0.52–0.97 | 1.571 | 1.25–1.94 | 0.75 | 0.47–0.91 | 0.00 | 0.11 | E < R < P < I < A.F < U |
| P08 | 1.526 | 1.24–1.83 | 0.70 | 0.45–0.86 | 1.286 | 1.10–1.50 | 0.46 | 0.31–0.51 | 0.00 | 0.13 | E < R < F < I.P < A < U |
| D3t | 1.579 | 1.29–1.89 | 0.67 | 0.45–0.80 | 1.429 | 1.22–1.66 | 0.51 | 0.31–0.62 | 0.00 | 0.16 | E < R < P < I < F < A < U |
| Item | M | USA L-U | SD | 95% CI L-U | p | Eta2 | Direction | ||||
| P07 | 2.588 | 2.22–2.92 | 0.71 | 0.29–0.93 | 0.00 | 0.11 | E < R < P < I < A.F < U | ||||
| P08 | 2.059 | 1.64–2.46 | 0.83 | 0.62–0.94 | 0.00 | 0.13 | E < R < F < I.P < A < U | ||||
| D3t | 2.324 | 1.97–2.65 | 0.71 | 0.43–0.86 | 0.00 | 0.16 | E < R < P < I < F < A < U |
| Age | Sex | HDI | Continent | Sector | Country | ||
|---|---|---|---|---|---|---|---|
| Age | Correlation Coefficient | 1.000 | 0.234 ** | 0.206 ** | 0.256 ** | −0.209 ** | 0.014 |
| Sig. (2-tailed) | <0.001 | <0.001 | <0.001 | <0.001 | 0.666 | ||
| Sex | Correlation Coefficient | 0.234 ** | 1.000 | 0.120 ** | 0.127 ** | −0.096 ** | −0.005 |
| Sig. (2-tailed) | <0.001 | <0.001 | <0.001 | 0.002 | 0.879 | ||
| HDI | Correlation Coefficient | 0.206 ** | 0.120 ** | 1.000 | 0.813 ** | −0.193 ** | 0.011 |
| Sig. (2-tailed) | <0.001 | <0.001 | <0.001 | <0.001 | 0.725 | ||
| Continent | Correlation Coefficient | 0.256 ** | 0.127 ** | 0.813 ** | 1.000 | −0.211 ** | <0.001 |
| Sig. (2-tailed) | <0.001 | <0.001 | <0.001 | <0.001 | 1.000 | ||
| Sector | Correlation Coefficient | −0.209 ** | −0.096 ** | −0.193 ** | −0.211 ** | 1.000 | −0.042 |
| Sig. (2-tailed) | <0.001 | 0.002 | <0.001 | <0.001 | 0.189 | ||
| Country | Correlation Coefficient | 0.014 | −0.005 | 0.011 | <0.001 | −0.042 | 1.000 |
| Sig. (2-tailed) | 0.666 | 0.879 | 0.725 | 1.000 | 0.189 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Toledano, E.; López-Parra, E.; Cebrián-Martínez, A.; Palomares-Ruiz, A. Inclusive Education for Health: Analysis of the Mandatory Nature of Vaccination and Its Regulation by Administrations, and Implications and Considerations for Vaccination against COVID. Vaccines 2022, 10, 73. https://doi.org/10.3390/vaccines10010073
García-Toledano E, López-Parra E, Cebrián-Martínez A, Palomares-Ruiz A. Inclusive Education for Health: Analysis of the Mandatory Nature of Vaccination and Its Regulation by Administrations, and Implications and Considerations for Vaccination against COVID. Vaccines. 2022; 10(1):73. https://doi.org/10.3390/vaccines10010073
Chicago/Turabian StyleGarcía-Toledano, Eduardo, Emilio López-Parra, Antonio Cebrián-Martínez, and Ascensión Palomares-Ruiz. 2022. "Inclusive Education for Health: Analysis of the Mandatory Nature of Vaccination and Its Regulation by Administrations, and Implications and Considerations for Vaccination against COVID" Vaccines 10, no. 1: 73. https://doi.org/10.3390/vaccines10010073