
Immunogenicity of a Heterologous Prime-Boost COVID-19 Vaccination with mRNA and Inactivated Virus Vaccines Compared with Homologous Vaccination Strategy against SARS-CoV-2 Variants

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Procedures
2.3. Outcomes
2.4. Statistics
3. Results
3.1. Subjects
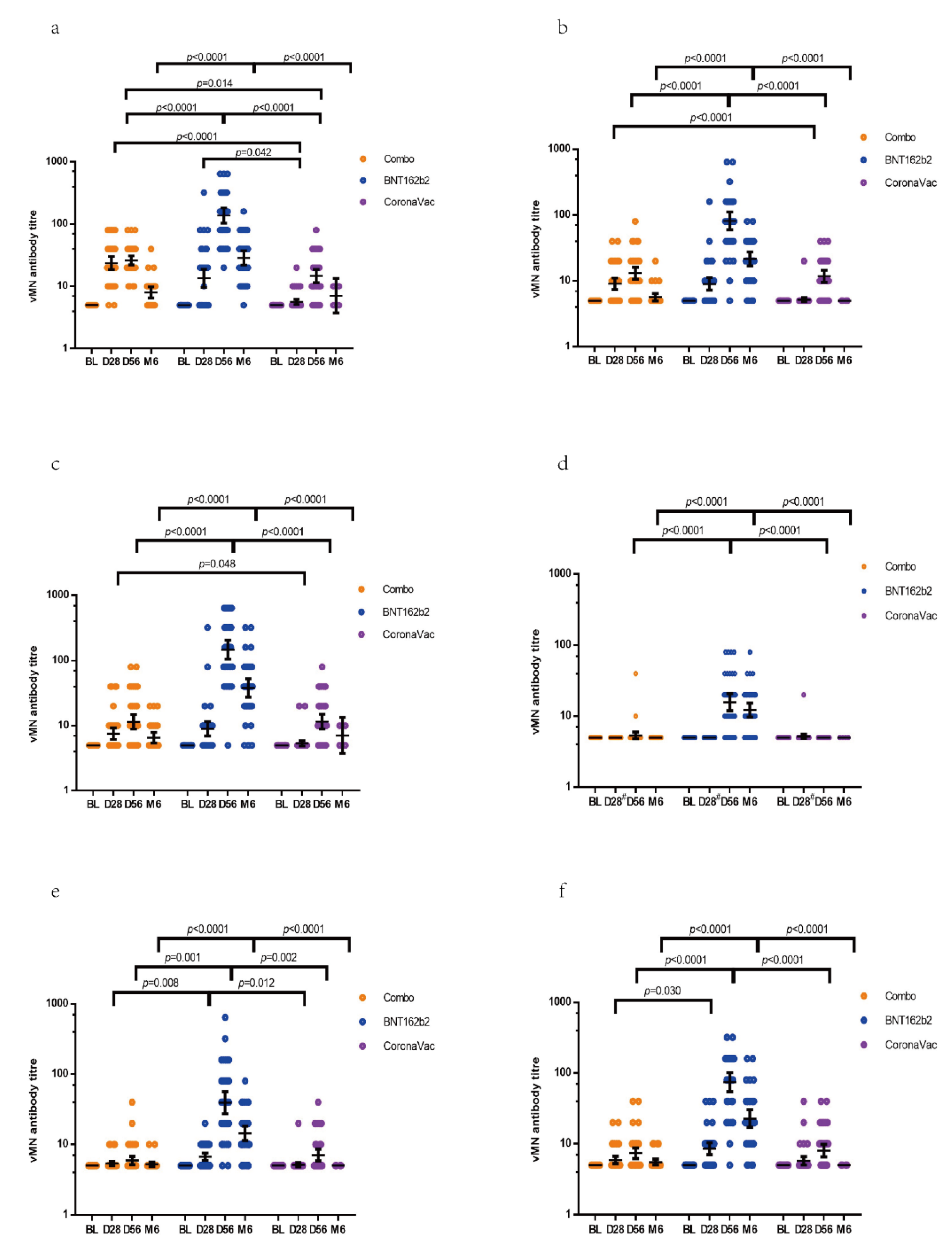
3.2. Immunogenicity of Vaccines Determined by vMN
3.3. Immunogenicity of Vaccines Determined by Surrogate NAb Test
3.4. Safety
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease 2019 (COVID-19) Situation Report. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 23 November 2021).
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Tanriover, M.D.; Doğanay, H.L.; Akova, M.; Güner, H.R.; Azap, A.; Akhan, S.; Köse, Ş.; Erdinç, F.; Akalın, E.H.; Tabak, Ö.F.; et al. Efficacy and safety of an inactivated whole-virion SARS-CoV-2 vaccine (CoronaVac): Interim results of a double-blind, randomised, placebo-controlled, phase 3 trial in Turkey. Lancet 2021, 398, 213–222. [Google Scholar] [CrossRef]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Heath, P.T.; Galiza, E.P.; Baxter, D.N.; Boffito, M.; Browne, D.; Burns, F.; Chadwick, D.R.; Clark, R.; Cosgrove, C.; Galloway, J.; et al. Safety and Efficacy of NVX-CoV2373 COVID-19 Vaccine. N. Engl. J. Med. 2021, 385, 1172–1183. [Google Scholar] [CrossRef]
- Tregoning, J.S.; Flight, K.E.; Higham, S.L.; Wang, Z.; Pierce, B.F. Progress of the COVID-19 vaccine effort: Viruses, vaccines and variants versus efficacy, effectiveness and escape. Nat. Rev. Immunol. 2021, 21, 626–636. [Google Scholar] [CrossRef]
- Tartof, S.Y.; Slezak, J.M.; Fischer, H.; Hong, V.; Ackerson, B.K.; Ranasinghe, O.N.; Frankland, T.B.; Ogun, O.A.; Zamparo, J.M.; Gray, S.; et al. Effectiveness of mRNA BNT162b2 COVID-19 vaccine up to 6 months in a large integrated health system in the USA: A retrospective cohort study. Lancet 2021, 398, 1407–1416. [Google Scholar] [CrossRef]
- Thomas, S.J.; Moreira, E.D., Jr.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Perez Marc, G.; Polack, F.P.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine through 6 Months. N. Engl. J. Med. 2021, 385, 1761–1773. [Google Scholar] [CrossRef] [PubMed]
- Hou, Y.J.; Chiba, S.; Halfmann, P.; Ehre, C.; Kuroda, M.; Dinnon, K.H., 3rd; Leist, S.R.; Schäfer, A.; Nakajima, N.; Takahashi, K.; et al. SARS-CoV-2 D614G variant exhibits efficient replication ex vivo and transmission in vivo. Science 2020, 370, 1464–1468. [Google Scholar] [CrossRef]
- Gómez, C.E.; Perdiguero, B.; Esteban, M. Emerging SARS-CoV-2 Variants and Impact in Global Vaccination Programs against SARS-CoV-2/COVID-19. Vaccines 2021, 9, 243. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, M.; Shayestehpour, M.; Mirzaei, H. The impact of spike mutated variants of SARS-CoV2 [Alpha, Beta, Gamma, Delta, and Lambda] on the efficacy of subunit recombinant vaccines. Braz. J. Infect. Dis. 2021, 25, 101606. [Google Scholar] [CrossRef]
- Shinde, V.; Bhikha, S.; Hoosain, Z.; Archary, M.; Bhorat, Q.; Fairlie, L.; Lalloo, U.; Masilela, M.S.L.; Moodley, D.; Hanley, S.; et al. Efficacy of NVX-CoV2373 COVID-19 Vaccine against the B.1.351 Variant. N. Engl. J. Med. 2021, 384, 1899–1909. [Google Scholar] [CrossRef]
- Madhi, S.A.; Baillie, V.; Cutland, C.L.; Voysey, M.; Koen, A.L.; Fairlie, L.; Padayachee, S.D.; Dheda, K.; Barnabas, S.L.; Bhorat, Q.E.; et al. Efficacy of the ChAdOx1 nCoV-19 COVID-19 Vaccine against the B.1.351 Variant. N. Engl. J. Med. 2021, 384, 1885–1898. [Google Scholar] [CrossRef] [PubMed]
- Lustig, Y.; Zuckerman, N.; Nemet, I.; Atari, N.; Kliker, L.; Regev-Yochay, G.; Sapir, E.; Mor, O.; Alroy-Preis, S.; Mendelson, E.; et al. Neutralising capacity against Delta (B.1.617.2) and other variants of concern following Comirnaty (BNT162b2, BioNTech/Pfizer) vaccination in health care workers, Israel. Eurosurveill 2021, 26, 2100557. [Google Scholar] [CrossRef]
- Pollard, A.J.; Launay, O.; Lelievre, J.D.; Lacabaratz, C.; Grande, S.; Goldstein, N.; Robinson, C.; Gaddah, A.; Bockstal, V.; Wiedemann, A.; et al. Safety and immunogenicity of a two-dose heterologous Ad26.ZEBOV and MVA-BN-Filo Ebola vaccine regimen in adults in Europe (EBOVAC2): A randomised, observer-blind, participant-blind, placebo-controlled, phase 2 trial. Lancet Infect. Dis. 2021, 21, 493–506. [Google Scholar] [CrossRef]
- Ledford, H. Could mixing COVID vaccines boost immune response? Nature 2021, 590, 375–376. [Google Scholar] [CrossRef]
- Hillus, D.; Schwarz, T.; Tober-Lau, P.; Vanshylla, K.; Hastor, H.; Thibeault, C.; Jentzsch, S.; Helbig, E.T.; Lippert, L.J.; Tscheak, P.; et al. Safety, reactogenicity, and immunogenicity of homologous and heterologous prime-boost immunisation with ChAdOx1 nCoV-19 and BNT162b2: A prospective cohort study. Lancet Respir. Med. 2021. [Google Scholar] [CrossRef]
- Chan, K.H.; Leung, K.Y.; Zhang, R.R.; Liu, D.; Fan, Y.; Chen, H.; Yuen, K.Y.; Hung, I.F. Performance of a Surrogate SARS-CoV-2-Neutralizing Antibody Assay in Natural Infection and Vaccination Samples. Diagnostics 2021, 11, 1757. [Google Scholar] [CrossRef]
- Park, J.W.; Lagniton, P.N.P.; Liu, Y.; Xu, R.H. mRNA vaccines for COVID-19: What, why and how. Int. J. Biol. Sci. 2021, 17, 1446–1460. [Google Scholar] [CrossRef]
- Zhang, Y.; Zeng, G.; Pan, H.; Li, C.; Hu, Y.; Chu, K.; Han, W.; Chen, Z.; Tang, R.; Yin, W.; et al. Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine in healthy adults aged 18-59 years: A randomised, double-blind, placebo-controlled, phase 1/2 clinical trial. Lancet Infect. Dis. 2021, 21, 181–192. [Google Scholar] [CrossRef]
- Walsh, E.E.; Frenck, R.W., Jr.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and Immunogenicity of Two RNA-Based COVID-19 Vaccine Candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef]
- Vasileiou, E.; Simpson, C.R.; Shi, T.; Kerr, S.; Agrawal, U.; Akbari, A.; Bedston, S.; Beggs, J.; Bradley, D.; Chuter, A.; et al. Interim findings from first-dose mass COVID-19 vaccination roll-out and COVID-19 hospital admissions in Scotland: A national prospective cohort study. Lancet 2021, 397, 1646–1657. [Google Scholar] [CrossRef]
- Zhang, R.; Khong, K.W.; Leung, K.Y.; Liu, D.; Fan, Y.; Lu, L.; Chan, P.C.; Chen, L.; Kelvin Kai-Wang To, K.K.W.; Chen, H.; et al. Antibody Response of BNT162b2 and CoronaVac Platforms in Recovered Individuals Previously Infected by COVID-19 against SARS-CoV-2 Wild Type and Delta Variant. Vaccines 2021, 9, 1442. [Google Scholar] [CrossRef]
- Kon, E.; Elia, U.; Peer, D. Principles for designing an optimal mRNA lipid nanoparticle vaccine. Curr. Opin. Biotechnol. 2021, 73, 329–336. [Google Scholar] [CrossRef]
- Thomas, S.J.; Moreira, E.D., Jr.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Polack, F.P.; Zerbini, C.; et al. Six Month Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. MedRxiv 2021, 21. [Google Scholar] [CrossRef]
- Miron, O.; Wilf-Miron, R.; Davidovitch, N. Effectiveness of COVID-19 vaccines BNT162b2 and mRNA-1273 by days from vaccination: A reanalysis of clinical trial data. SSRN 2021, 14. [Google Scholar] [CrossRef]
- Fernández, J.; Bruneau, N.; Fasce, R.; Martín, H.S.; Balanda, M.; Bustos, P.; Ulloa, S.; Mora, J.; Ramírez, E. Neutralization of alpha, gamma, and D614G SARS-CoV-2 variants by CoronaVac vaccine-induced antibodies. J. Med. Virol. 2021, 94, 399–403. [Google Scholar] [CrossRef]
- Xie, X.; Liu, Y.; Liu, J.; Zhang, X.; Zou, J.; Fontes-Garfias, C.R.; Xia, H.; Swanson, K.A.; Cutler, M.; Cooper, D.; et al. Neutralization of SARS-CoV-2 spike 69/70 deletion, E484K and N501Y variants by BNT162b2 vaccine-elicited sera. Nat. Med. 2021, 27, 620–621. [Google Scholar] [CrossRef] [PubMed]
- Wibmer, C.K.; Ayres, F.; Hermanus, T.; Madzivhandila, M.; Kgagudi, P.; Oosthuysen, B.; Lambson, B.E.; de Oliveira, T.; Vermeulen, M.; van der Berg, K.; et al. SARS-CoV-2 501Y.V2 escapes neutralization by South African COVID-19 donor plasma. Nat. Med. 2021, 27, 622–625. [Google Scholar] [CrossRef]
- Lopez Bernal, J.; Andrews, N.; Gower, C.; Gallagher, E.; Simmons, R.; Thelwall, S.; Stowe, J.; Tessier, E.; Groves, N.; Dabrera, G.; et al. Effectiveness of COVID-19 Vaccines against the B.1.617.2 (Delta) Variant. N. Engl. J. Med. 2021, 385, 585–594. [Google Scholar] [CrossRef] [PubMed]
- Iacobucci, G.; Mahase, E. COVID-19 vaccination: What’s the evidence for extending the dosing interval? Bmj 2021, 372, n18. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Combo (n = 42) | CoronaVac (n = 41) | BNT162b2 (n = 40) | p2 | |
|---|---|---|---|---|
| Median age (years) | 44.5 (36–50.5) 1 | 49 (39.5–54.5) | 47 (33–51.75) | 0.232 |
| Male/Female (%) | 24/18 (57.1/42.8) | 13/28 (31.7/68.3) | 19/21(47.5/52.5) | 0.065 |
| Combo (n = 42) | BNT162b2 (n = 40) | CoronaVac (n = 41) | p9 | |
|---|---|---|---|---|
| WT | ||||
| Baseline | ||||
| GMT 1 | 5 (5–5) | 5 (5–5) | 5 (5–5) | |
| Day 21 2/Day 28 | ||||
| GMT | 23.7 (18.8–29.9) | 13.4 (9.7–18.7) | 5.6 (5.1–6.2) | 0.002 |
| GMT fold increase | 4.7 (3.8–6.0) 3 | 2.7 (1.9–3.7) | 1.1 (1.0–1.2) 6 | 0.002 |
| Day 56 | ||||
| GMT | 26.2 (22.3–30.9) | 136.9 (104.2–179.7) | 14.7 (11.6–18.6) | <0.0001 |
| GMT fold increase | 5.2 (4.5–6.2) | 27.4 (20.8–36.0) | 2.9 (2.3–3.7) 7 | <0.0001 |
| Month 6 | ||||
| GMT | 8.0 (6.6–9.8) | 28.8 (22.3–37.2) | 7.1(4.8–10.5) | <0.0001 |
| GMT fold increase | 1.6 (1.3–2.0) 4 | 5.8 (4.5–7.4) 5 | 1.4 (1.0–2.1) 8 | <0.0001 |
| D614G | ||||
| Baseline | ||||
| GMT | 5 (5–5) | 5 (5–5) | 5 (5–5) | |
| Day 21/Day 28 | ||||
| GMT | 9.0 (7.5–11.0) | 9.0 (7.3–11.2) | 5.2 (4.8–5.5) | 0.050 |
| GMT fold increase | 1.8 (1.5–2.2) | 1.8 (1.5–2.2) | 1.0 (1.0–1.1) | 0.050 |
| D614G | ||||
| Day 56 | ||||
| GMT | 13.1 (10.7–16.1) | 81.4 (60.0–110.5) | 11.8 (9.6–14.5) | <0.0001 |
| GMT fold increase | 2.6 (2.1–3.2) | 16.3 (12.0–22.1) | 2.4 (1.9–2.9) | <0.0001 |
| Month 6 | ||||
| GMT | 5.7 (5.0–6.4) | 21.5 (17.0–27.2) | 5 (5–5) | <0.0001 |
| GMT fold increase | 1.1 (1.0–1.3) | 4.3 (3.4–5.4) | 1.0 (1.0–1.0) | <0.0001 |
| Alpha | ||||
| Baseline | ||||
| GMT | 5 (5–5) | 5 (5–5) | 5 (5–5) | |
| Day 21/Day 28 | ||||
| GMT | 7.5 (6.1–9.2) | 9.0 (7.1–11.5) | 5.4 (4.9–5.9) | 0.177 |
| GMT fold increase | 1.5 (1.2–1.8) | 1.8 (1.4–2.3) | 1.1 (1.0–1.2) | 0.177 |
| Day 56 | ||||
| GMT | 11.5 (8.9–14.7) | 146.7 (106.2–202.7) | 11.6 (9.0–15.0) | <0.0001 |
| GMT fold increase | 2.3 (1.8–2.9) | 29.3 (21.2–40.5) | 2.3 (1.8–3.0) | <0.0001 |
| Month 6 | ||||
| GMT | 6.6 (5.5–7.8) | 37.9 (27.7–51.8) | 7.1 (4.8–10.5) | <0.0001 |
| GMT fold increase | 1.3 (1.1–1.6) | 7.6 (5.5–10.4) | 1.4 (1.0–2.1) | <0.0001 |
| Beta | ||||
| Baseline | ||||
| GMT | 5 (5–5) | 5 (5–5) | 5 (5–5) | |
| Day 21/Day 28 | ||||
| GMT | 5 (5–5) | 5 (5–5) | 5.2 (4.8–5.5) | 0.366 |
| GMT fold increase | 1.0 (1.0–1.0) | 1.0 (1.0–1.0) | 1.0 (1.0–1.1) | 0.366 |
| Day 56 | ||||
| GMT | 5.4 (4.8–5.9) | 15.7 (12.0–20.5) | 5 (5–5) | <0.0001 |
| GMT fold increase | 1.1 (1.0–1.2) | 3.1 (2.4–4.1) | 1.0 (1.0–1.0) | <0.0001 |
| Month 6 | ||||
| GMT | 5 (5–5) | 12.2 (9.8–15.2) | 5 (5–5) | <0.0001 |
| GMT fold increase | 1.0 (1.0–1.0) | 2.4 (2.0–3.0) | 1.0 (1.0–1.0) | <0.0001 |
| Theta | ||||
| Baseline | ||||
| GMT | 5 (5–5) | 5 (5–5) | 5 (5–5) | |
| Day 21/Day 28 | ||||
| GMT | 5.4 (5.0–5.7) | 6.7 (6.0–7.6) | 5.2 (4.8–5.5) | 0.001 |
| GMT fold increase | 1.1 (1.0–1.1) | 1.3 (1.2–1.5) | 1.0 (1.0–1.1) | 0.001 |
| Day 56 | ||||
| GMT | 5.9 (5.2–6.8) | 39.3 (27.6–55.9) | 7.1 (5.9–8.6) | <0.0001 |
| GMT fold increase | 1.2 (1.0–1.4) | 7.9 (5.5–11.2) | 1.4 (1.2–1.7) | <0.0001 |
| Theta | ||||
| Month 6 | ||||
| GMT | 5.3 (4.9–5.6) | 14.4 (11.5–18.1) | 5 (5–5) | <0.0001 |
| GMT fold increase | 1.1 (1.0–1.1) | 2.9 (2.3–3.6) | 1.0 (1.0–1.0) | <0.0001 |
| Delta | ||||
| Baseline | ||||
| GMT | 5 (5–5) | 5 (5–5) | 5 (5–5) | |
| Day 21/Day 28 | ||||
| GMT | 5.9 (5.3–6.6) | 8.6 (7.1–10.3) | 5.7 (5.0–6.5) | 0.008 |
| GMT fold increase | 1.2 (1.1–1.3) | 1.7 (1.4–2.1) | 1.1 (1.0–1.3) | 0.008 |
| Day 56 | ||||
| GMT | 7.4 (6.2–8.8) | 74.6 (55.4–100.7) | 8.0 (6.6–9.8) | <0.0001 |
| GMT fold increase | 1.5 (1.2–1.8) | 14.9 (11.1–20.1) | 1.6 (1.3–2.0) | <0.0001 |
| Month 6 | ||||
| GMT | 5.5 (5.0–6.1) | 22.7 (17.3–29.9) | 5 (5–5) | <0.0001 |
| GMT fold increase | 1.1 (1.0–1.2) | 4.5 (3.5–6.0) | 1.0 (1.0–1.0) | <0.0001 |
| Combo (n = 42) | BNT162b2 (n = 40) | CoronaVac (n = 41) | p9 | |
|---|---|---|---|---|
| Surrogate NAb Mean (AU/mL) 1 | ||||
| Baseline | 4.1 (3.9–4.3) | 4.0 (4.0–4.0) | 4.1 (3.9–4.4) | 0.610 |
| Day21 2/Day28 | 37.1 (27.6–46.6) 3 | 70.6 (30.3–110.8) | 5.5 (4.7–6.4) 6 | 0.001 |
| Day 56 | 40.5 (24.6–56.4) | 594.7 (509.9–679.5) | 38.8 (27.9–49.6) 7 | <0.0001 |
| Month 6 | 8.6 (7.2–9.9) 4 | 138.5 (80.5–196.6) 5 | 9.2 (3.5–14.9) 8 | 0.001 |
| Anti-N IgG Mean (AU/mL) 1 | ||||
| Baseline | 1.4 (1.0–1.9) | 1.7 (0.6–2.8) | 0.8 (0.6–1.0) | 0.166 |
| Day21 2/Day28 | 1.4 (0.9–1.8) 3 | 1.6 (0.6–2.6) | 1.6 (1.1–2.0) 6 | 0.904 |
| Day 56 | 1.4 (0.9–1.8) | 1.3 (0.4–2.2) | 21.8 (15.8–27.8) 7 | <0.0001 |
| Month 6 | 1.3 (0.7–1.9) 4 | 1.3 (0.4–2.2) 5 | 5.9 (-4.8–16.7) 8 | 0.007 |
| Combo (n = 42) | BNT162b2 (n = 33) | CoronaVac (n = 35) | p2 | |
|---|---|---|---|---|
| Post first dose System reactions | 19 (45.2%) | 15 (45.5%) | 13 (37.1%) | 0.761 |
| Fever | 2 (4.8%) | 1 (3.0%) | 0 (0) | 0.636 |
| Chills | 0 (0) | 0 (0) | 2 (5.7%) | 0.187 |
| Headache | 6 (14.3%) | 6 (18.2%) | 4 (11.4%) | 0.702 |
| Tiredness | 12 (31.0%) | 11 (33.3%) | 9 (25.7%) | 0.807 |
| Nausea | 1 (2.4%) | 1 (3.0%) | 3 (8.6%) | 0.516 |
| Vomit | 0 (0) | 0 (0) | 0 (0) | - |
| Diarrhea | 1 (2.4%) | 2 (6.1%) | 2 (5.7%) | 0.732 |
| Muscle pain | 7 (16.7%) | 9 (27.3%) | 6 (17.1%) | 0.500 |
| Joint pain | 1 (2.4%) | 4 (12.1%) | 2 (5.7%0 | 0.255 |
| Skin rash | 3 (7.1%) | 1 (3.0%) | 1 (2.9%) | 0.624 |
| SAE 1 | 0 (0) | 0 (0) | 0 (0) | - |
| Local symptoms | 41 (97.6%) | 27 (81.8%) | 12 (34.3%) | <0.0001 |
| Pain | 41 (97.6%) | 25 (75.8%) | 12 (34.3%) | <0.0001 |
| Redness | 3 (7.1%) | 7 (21.2%) | 0 (0) | 0.005 |
| Swelling | 6 (14.3%) | 12 (36.4%) | 0 (0) | <0.0001 |
| Ecchymosis | 4 (9.5%) | 3 (9.1%) | 0 (0) | 0.200 |
| Itching | 2 (4.8%) | 3 (9.1%) | 1 (2.9%) | 0.200 |
| Post second dose System reactions | 13 (31.0%) | 22 (66.7%) | 8 (22.9%) | <0.0001 |
| Fever | 0 (0) | 2 (6.1%) | 0 (0) | 0.088 |
| Chills | 0 (0) | 6 (18.2%) | 1 (2.9%) | 0.002 |
| Headache | 6 (14.3%) | 9 (27.3%) | 3 (8.6%) | 0.107 |
| Tiredness | 10 (23.8%) | 17 (51.5%) | 3 (8.6%) | <0.0001 |
| Nausea | 2 (4.8%) | 5 (15.2%) | 2 (5.7%) | 0.233 |
| Vomit | 0 (0) | 1 (3.0%) | 1 (2.9%) | 0.524 |
| Diarrhea | 0 (0) | 3 (9.1%) | 3 (8.6%) | 0.157 |
| Muscle pain | 3 (7.1%) | 16 (48.5%) | 3 (8.6%) | <0.0001 |
| Joint pain | 1 (2.4%) | 5 (15.2%) | 1 (2.9%) | 0.046 |
| Skin rash | 0 (0) | 1 (3.0%) | 0 (0) | 0.300 |
| SAE 1 | 0 (0) | 0 (0) | 0 (0) | - |
| Local symptoms | 15 (35.7%) | 25 (75.8%) | 7 (20.0%) | <0.0001 |
| Pain | 15 (35.7%) | 23 (69.7%) | 7 (20.0%) | <0.0001 |
| Redness | 2 (4.8%) | 9 (27.3%) | 1 (2.9%) | 0.001 |
| Swelling | 2 (4.8%) | 11 (33.3%) | 0 (0) | <0.0001 |
| Ecchymosis | 0 (0) | 1 (3.0%) | 0 (0) | 0.300 |
| Itching | 0 (0) | 5 (15.2%) | 0 (0) | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, R.; Liu, D.; Leung, K.-Y.; Fan, Y.; Lu, L.; Chan, P.-C.; To, K.K.-W.; Chen, H.; Yuen, K.-Y.; Chan, K.-H.; et al. Immunogenicity of a Heterologous Prime-Boost COVID-19 Vaccination with mRNA and Inactivated Virus Vaccines Compared with Homologous Vaccination Strategy against SARS-CoV-2 Variants. Vaccines 2022, 10, 72. https://doi.org/10.3390/vaccines10010072
Zhang R, Liu D, Leung K-Y, Fan Y, Lu L, Chan P-C, To KK-W, Chen H, Yuen K-Y, Chan K-H, et al. Immunogenicity of a Heterologous Prime-Boost COVID-19 Vaccination with mRNA and Inactivated Virus Vaccines Compared with Homologous Vaccination Strategy against SARS-CoV-2 Variants. Vaccines. 2022; 10(1):72. https://doi.org/10.3390/vaccines10010072
Chicago/Turabian StyleZhang, Ruiqi, Danlei Liu, Ka-Yi Leung, Yujing Fan, Lu Lu, Pui-Chun Chan, Kelvin Kai-Wang To, Honglin Chen, Kwok-Yung Yuen, Kwok-Hung Chan, and et al. 2022. "Immunogenicity of a Heterologous Prime-Boost COVID-19 Vaccination with mRNA and Inactivated Virus Vaccines Compared with Homologous Vaccination Strategy against SARS-CoV-2 Variants" Vaccines 10, no. 1: 72. https://doi.org/10.3390/vaccines10010072