
The Association of Previous Vaccination with Live-Attenuated Varicella Zoster Vaccine and COVID-19 Positivity: An Israeli Population-Based Study

 , , and
, , and
Abstract
:1. Introduction
2. Methods
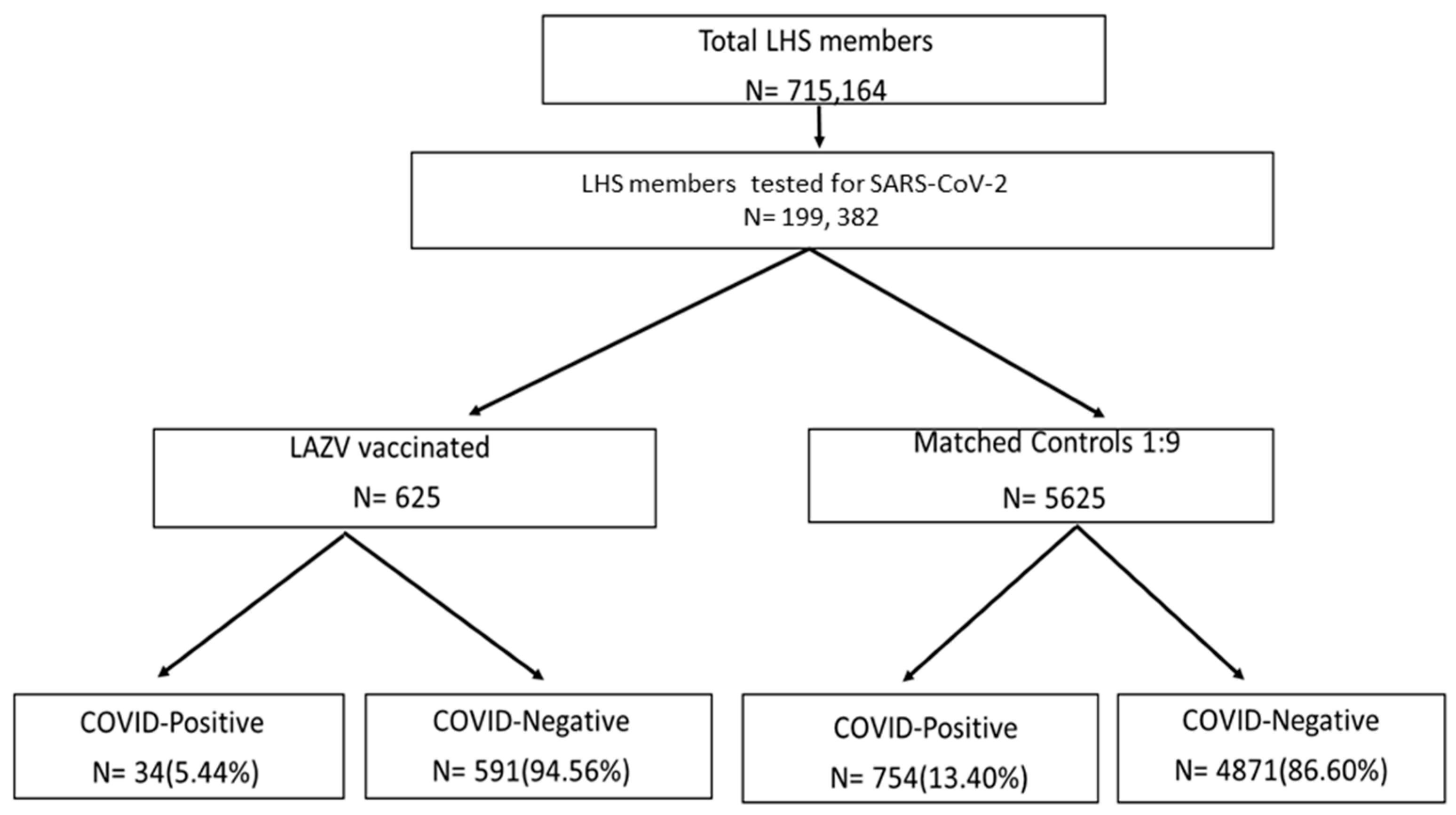
2.1. Study Subjects
2.2. Definitions
2.3. Statistical Analysis
3. Results
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Mina, M. Measles, immune suppression and vaccination: Direct and indirect nonspecific vaccine benefits. J. Infect. 2017, 74 (Suppl. 1), S10–S17. [Google Scholar] [CrossRef]
- Mina, M.J.; Metcalf, C.J.E.; de Swart, R.L.; Osterhaus, A.D.M.E.; Grenfell, B.T. Long-term measles-induced immunomodulation increases overall childhood infectious disease mortality. Science 2015, 348, 694–699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aaby, P.; Roth, A.; Ravn, H.; Napirna, B.M.; Rodrigues, A.; Lisse, I.M.; Stensballe, L.G.; Diness, B.R.; Lausch, K.R.; Lund, N.; et al. Randomized Trial of BCG Vaccination at Birth to Low-Birth-Weight Children: Beneficial Nonspecific Effects in the Neonatal Period? J. Infect. Dis. 2011, 204, 245–252. [Google Scholar] [CrossRef] [PubMed]
- de Castro, M.J.; Pardo-Seco, J.; Martinón-Torres, F. Nonspecific (heterologous) protection of neonatal BCG vaccination against hospitalization due to respiratory infection and sepsis. Clin. Infect. Dis. 2015, 60, 1611–1619. [Google Scholar] [CrossRef] [Green Version]
- Näslund, C. Resultats des Experiences de Vaccination par le BCG Poursuivies dans le NORRBOTTEN (Suède) (Septembre 1927–Décembre 1931). In Vaccination Preventative de Tuberculose, Rapports et Documents; Institut Pasteur: Paris, France, 1932. [Google Scholar]
- Stensballe, L.G.; Nante, E.; Jensen, I.P.; Kofoed, P.-E.; Poulsen, A.; Jensen, H.; Newport, M.; Marchant, A.; Aaby, P. Acute lower respiratory tract infections and respiratory syncytial virus in infants in Guinea-Bissau: A beneficial effect of BCG vaccination for girls: Community based case–control study. Vaccine 2005, 23, 1251–1257. [Google Scholar] [CrossRef] [PubMed]
- Wardhana, D.E.; Sultana, A.; Mandang, V.V.; Jim, E. The efficacy of Bacillus Calmette-Guerin vaccinations for the prevention of acute upper respiratory tract infection in the elderly. Acta Med. Indones. 2011, 43, 185–190. [Google Scholar] [PubMed]
- Escobar, L.E.; Molina-Cruz, A.; Barillas-Mury, C. BCG vaccine protection from severe coronavirus disease 2019 (COVID-19). Proc. Natl. Acad. Sci. USA 2020, 117, 17720–17726. [Google Scholar] [CrossRef] [PubMed]
- Murdoch Childrens Research Institute. BCG Vaccination to Protect Healthcare Workers against COVID-19 (BRACE). Clinicaltrials.gov. Available online: https://www.clinicaltrials.gov/ct2/show/NCT04327206 (accessed on 28 February 2021).
- Bonten, M.J.M. Reducing Health Care Workers Absenteeism in COVID-19 Pandemic through BCG Vaccine (BCG-CORONA). Available online: https://clinicaltrials.gov/ct2/show/NCT04328441 (accessed on 28 February 2021).
- Green, I.; Ashkenazi, S.; Merzon, E.; Vinker, S.; Golan-Cohen, A. The association of previous influenza vaccination and coronavirus disease-2019. Hum. Vaccines Immunother. 2021, 17, 2169–2175. [Google Scholar] [CrossRef] [PubMed]
- Netea, M.G.; Latz, E.; Mills, K.; O’Neill, L. Innate immune memory: A paradigm shift in understanding host defense. Nat. Immunol. 2015, 16, 675–679. [Google Scholar] [CrossRef] [PubMed]
- Netea, M.G.; Joosten, L.A.B.; Latz, E.; Mills, K.H.G.; Natoli, G.; Stunnenberg, H.G.; O’Neill, L.A.J.; Xavier, R.J. Trained immunity: A program of innate immune memory in health and disease. Science 2016, 352, aaf1098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mantovani, A.; Netea, M.G. Trained Innate Immunity, Epigenetics, and COVID-19. N. Engl. J. Med. 2020, 383, 1078–1080. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, J.; Franz, K. Innate defence: Evidence for memory in invertebrate immunity. Nature 2003, 425, 37–38. [Google Scholar] [CrossRef] [PubMed]
- de Laval, B.; Maurizio, J.; Kandalla, P.K.; Brisou, G.; Simonnet, L.; Huber, C.; Gimenez, G.; Matcovitch-Natan, O.; Reinhardt, S.; David, E.; et al. C/EBPβ-Dependent epigenetic memory induces trained immunity in hematopoietic stem cells. Cell Stem Cell 2020, 26, 793. [Google Scholar] [CrossRef] [PubMed]
- Cirovic, B.; de Bree, L.C.J.; Groh, L.; Blok, B.A.; Chan, J.; van der Velden, W.J.; Bremmers, M.; van Crevel, R.; Händler, K.; Picelli, S.; et al. BCG Vaccination in Humans Elicits Trained Immunity via the Hematopoietic Progenitor Compartment. Cell Host Microbe 2020, 28, 322–334.e5. [Google Scholar] [CrossRef] [PubMed]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef]
- Onder, G.; Rezza, G.; Brusaferro, S. Case-Fatality Rate and Characteristics of Patients Dying in Relation to COVID-19 in Italy. JAMA 2020, 323, 1775–1776. [Google Scholar] [CrossRef] [PubMed]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; Northwell COVID-19 Research Consortium. Presenting Characteristics, Comorbidities, and Outcomes Among 5700 Patients Hospitalized with COVID-19 in the New York City Area. JAMA 2020, 323, 2052–2059. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, A.; Zhang, J.H.; Oxman, M.N.; Johnson, G.R.; Hayward, A.R.; Caulfield, M.J.; Irwin, M.R.; Clair, J.; Smith, J.G.; Stanley, H.; et al. Varicella-Zoster Virus–Specific Immune Responses to Herpes Zoster in Elderly Participants in a Trial of a Clinically Effective Zoster Vaccine. J. Infect. Dis. 2009, 200, 1068–1077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levin, M.J.; Oxman, M.N.; Zhang, J.H.; Johnson, G.R.; Stanley, H.; Hayward, A.R.; Caulfield, M.J.; Irwin, M.; Smith, J.G.; Clair, J.; et al. Varicella-Zoster Virus–Specific Immune Responses in Elderly Recipients of a Herpes Zoster Vaccine. J. Infect. Dis. 2008, 197, 825–835. [Google Scholar] [CrossRef] [Green Version]
- Pringle, M.; Ward, P.; Chilvers, C. Assessment of the completeness and accuracy of computer medical records in four practices committed to recording data on computer. Br. J. Gen. Pract. 1995, 45, 537–541. [Google Scholar]
- Rennert, G.; Peterburg, Y. Prevalence of selected chronic diseases in Israel. Isr. Med. Assoc. J. 2001, 3, 404–408. [Google Scholar] [PubMed]
- Shalev, V.; Chodick, G.; Goren, I.; Silber, H.; Kokia, E.; Heymann, A.D. The use of an automated patient registry to manage and monitor cardiovascular conditions and related outcomes in a large health organization. Int. J. Cardiol. 2011, 152, 345–349. [Google Scholar] [CrossRef] [PubMed]
- Chodick, G.; Heymann, A.D.; Shalev, V.; Kookia, E. The epidemiology of diabetes in a large Israeli HMO. Eur. J. Epidemiol. 2002, 18, 1143–1146. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Laboratory Testing for 2019 Novel Coronavirus (2019-nCoV) in Suspected Human Cases. Interim Guidance. March 2020. Available online: https://apps.who.int/iris/bitstream/handle/10665/331501/WHO-COVID-19-laboratory-2020 (accessed on 1 December 2021).
- Adams, M.L.; Katz, D.L.; Grandpre, J. Population-Based Estimates of Chronic Conditions Affecting Risk for Complications from Coronavirus Disease, United States. Emerg. Infect. Dis. 2020, 26, 1831–1833. [Google Scholar] [CrossRef] [PubMed]
- Merzon, E.; Manor, I.; Rotem, A.; Schneider, T.; Vinker, S.; Cohen, A.G.; Lauden, A.; Weizman, A.; Green, I. ADHD as a Risk Factor for Infection With COVID-19. J. Atten. Disord. 2021, 25, 1783–1790. [Google Scholar] [CrossRef] [PubMed]
- Merzon, E.; Green, I.; Shpigelman, M.; Vinker, S.; Raz, I.; Golan-Cohen, A.; Eldor, R. Hemoglobin A1C is a Predictor of COVID-19 Severity in Patients with Diabetes. Diabetes Metab. Res. Rev. 2020, 27, e3398. [Google Scholar]
- Green, I.; Merzon, E.; Vinker, S.; Golan-Cohen, A.; Magen, E. Potential protective effect of asthma on COVID-19 susceptibility. J. Allergy Clin. Immunol. Pract. 2020, 23. S2213-2198(20)31240-X. [Google Scholar] [CrossRef]
- Merzon, E.; Green, I.; Vinker, S.; Golan-Cohen, A.; Gorohovski, A.; Avramovich, E.; Frenkel-Morgenstern, M.; Magen, E. The use of aspirin for primary prevention of cardiovascular disease is associated with a lower likelihood of COVID-19 infection. FEBS J. 2021, 288, 5179–5189. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Demographics | LAZV-Vaccinated N = 625 | Matched Control Group N = 5625 | p-Value | |
|---|---|---|---|---|
| Mean age (years ± SD) | 69.35 ± 10.04 | 69.31 ± 13.15 | 0.751 * | |
| Gender, N (%) | Male | 272 (43.52%) | 2446 (43.48%) | 0.986 ** |
| Female | 353 (56.48%) | 3179 (56.52%) | ||
| SES, N (%) | Low | 179 (28.64%) | 2603 (46.28%) | <0.001 ** |
| Middle–High | 445 (71.2%) | 2679 (47.63%) | ||
| Missing Data | 1 (0.16%) | 343 (6.1%) | ||
| Smoking, N (%) | Never | 535 (85.6%) | 4093 (72.76%) | <0.001 ** |
| Current | 57 (9.12%) | 688 (12.23%) | ||
| Past | 33 (5.28%) | 844 (15%) | ||
| BMI, Mean (SD) | 27.77 ± 4.66 | 28.28 ± 5.37 | 0.022 * | |
| Hemoglobin A1C, Mean (SD) | 5.77 ± 0.85 | 5.79 ± 1.27 | 0.738 * | |
| Obesity, N (%) | 175 (28.18%) | 1713 (30.45%) | 0.124 ** | |
| Diabetes Mellitus, N (%) | 271 (43.36%) | 2465 (43.82%) | 0.964 ** | |
| HTN, N (%) | 366 (58.56%) | 3292 (58.52%) | 0.925 ** | |
| IHD, N (%) | 179 (28.64%) | 1598 (28.41%) | 0.918 ** | |
| Asthma, N (%) | 73 (11.68%) | 654 (11.63%) | 0.741 ** | |
| COPD, N (%) | 107 (17.1%) | 961 (17.08%) | 0.643 ** | |
| Malignancy, N (%) | 0 | 4 (0.07%) | 0.504 ** | |
| Depression, N (%) | 65 (10.40%) | 673 (11.96%) | 0.2502 ** | |
| ADHD, N (%) | 18 (2.88%) | 112 (1.99%) | 0.1396 ** | |
| Aspirin, N (%) | 224 (35.84%) | 1803 (32.05%) | 0.073 ** | |
| Statins, N (%) | 370 (59.2%) | 2251 (40.02%) | <0.001 ** | |
| ACEIs, N (%) | 134 (21.44%) | 1134 (20.16%) | 0.450 ** | |
| ARBs, N (%) | 94 (15.04%) | 595 (10.58%) | <0.001 ** | |
| Flu vaccine (2019–2020), N (%) | 486 (77.76%) | 2544 (45.23%) | <0.001 ** | |
| Hospitalizations d/t COVID-19, N (%) | 1 (0.16%) | 21 (0.37%) | <0.001 ** | |
| Demographics | COVID-19-Positive N = 788 (12.61%) | COVID-19-Negative N = 5462 (87.39%) | p-Value | |
|---|---|---|---|---|
| Mean age (years ± SD) | 66.50 ± 12.34 | 69.74 ± 12.73 | <0.001 * | |
| Gender, N (%) | Male | 386 (48.98%) | 2332 (42.69%) | <0.001 ** |
| Female | 402 (51.02%) | 3130 (57.31%) | ||
| SES, N (%) | Low | 524 (69.13%) | 2258 (43.86%) | <0.001 ** |
| Middle-High | 234 (30.87%) | 2890 (56.14%) | ||
| Smoking, N (%) | Never | 609 (77.28%) | 4019 (73.58%) | <0.001 ** |
| Current | 60 (7.61%) | 685 (12.54%) | ||
| Past | 119 (15.10%) | 758 (13.88%) | ||
| BMI, Mean (SD) | 28.96 ± 5.32 | 28.12 ± 5.29 | <0.001 * | |
| Hemoglobin A1C, Mean (SD) | 5.85 ± 1.35 | 5.78 ± 1.22 | 0.192 * | |
| Obesity, N (%) | 277 (35.15%) | 1611 (29.49%) | <0.001 ** | |
| Diabetes Mellitus, N (%) | 348 (44.16%) | 2388 (43.72%) | 0.815 ** | |
| HTN, N (%) | 414 (52.54%) | 3244 (59.39%) | <0.001 ** | |
| IHD, N (%) | 171 (21.70%) | 1606 (29.40%) | <0.001 ** | |
| Asthma, N (%) | 63 (7.99%) | 664 (12.16%) | 0.741 ** | |
| COPD, N (%) | 113 (14.34%) | 953 (17.45%) | 0.0301 ** | |
| Malignancy, N (%) | 1 (0.13%) | 3 (0.05%) | <0.001 ** | |
| Depression, N (%) | 74 (9.39%) | 664 (12.16%) | 0.024 ** | |
| ADHD, N (%) | 21 (2.66%) | 109 (2%) | 0.218 ** | |
| Aspirin, N (%) | 193 (24.49%) | 1834 (33.58%) | <0.001 ** | |
| Statins, N (%) | 260 (32.99%) | 2359 (43.19%) | <0.001 ** | |
| ACEIs, N (%) | 160 (20.30%) | 1108 (20.29%) | 0.990 ** | |
| ARSs, N (%) | 57 (7.23%) | 632 (11.57%) | <0.001 ** | |
| Flu vaccine (2019–2020), N (%) | 304 (38.58%) | 2726 (49.91%) | <0.001 ** | |
| LAZV vaccine, N (%) | 34 (4.31%) | 591 (10.82%) | <0.001 ** | |
| Variable | Crude OR | 95% CI | p-Value | Adjusted * OR | 95% CI | p-Value | VIF When All Covariates Are in the Model |
|---|---|---|---|---|---|---|---|
| Age | 0.97 | 0.97–0.98 | <0.001 | 0.99 | 0.98–1.00 | 0.130 | 1.03 |
| Male gender | 1.28 | 1.10–1.49 | 0.001 | 1.51 | 1.28–1.80 | <0.001 | 1.76 |
| Low SES | 2.86 | 2.43–3.37 | <0.001 | 2.58 | 2.16–3.09 | <0.001 | 1.56 |
| Smoking (current vs. never) | 0.57 | (0.40; 0.77) | <0.05 | 0.94 | 0.82–1.07 | 0.382 | 1.73 |
| Diabetes Mellitus | 1.01 | 0.87–1.18 | 0.815 | 1.22 | 1.00–1.50 | 0.043 | 1.45 |
| Hemoglobin A1C | 1.04 | 0.97–1.10 | 0.192 | 1.03 | 0.95–1.11 | 0.392 | 1.64 |
| Obesity | 1.29 | 1.10–1.51 | 0.002 | 1.27 | 1.06–1.52 | 0.007 | 1.89 |
| HTN | 0.74 | 0.64–0.86 | <0.001 | 0.98 | 0.79–1.21 | 0.869 | 1.78 |
| IHD | 0.66 | 0.55–0.79 | <0.001 | 0.73 | 0.59–0.90 | 0.005 | 2.01 |
| Asthma | 0.62 | 0.47–0.82 | 0.001 | 0.59 | 0.39–0.91 | 0.018 | 1.52 |
| COPD | 0.79 | 0.64–0.97 | 0.03 | 1.14 | 0.81–1.59 | 0.432 | 1.02 |
| Malignancy | 2.31 | 0.24–22.25 | 0.468 | 3.00 | 0.27–32.58 | 0.366 | 2.08 |
| Depression | 0.75 | 0.58–1.02 | 0.052 | 0.91 | 0.69–1.21 | 0.428 | 1.23 |
| ADHD | 1.34 | 0.84–2.16 | 0.220 | 1.31 | 0.76–2.22 | 0.337 | 1.11 |
| Aspirin | 0.64 | 0.54–0.76 | <0.001 | 0.78 | 0.63–0.97 | 0.03 | 2.03 |
| Statins | 0.64 | 0.55–0.75 | <0.001 | 0.85 | 0.70–1.04 | 0.134 | 2.56 |
| ACEIs | 1.00 | 0.83–1.20 | 0.990 | 1.02 | 0.81–1.28 | 0.833 | 1.34 |
| ARBs | 0.59 | 0.44–0.79 | <0.001 | 0.65 | 0.47–0.90 | <0.001 | 2.42 |
| Flu vaccine (2019–2020) | 0.63 | 0.54–0.73 | <0.001 | 0.83 | 0.69–0.99 | 0.048 | 1.05 |
| LAZV vaccine | 0.37 | 0.26–0.52 | <0.001 | 0.47 | 0.32–0.69 | <0.001 | 1.94 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Merzon, E.; Green, I.; Somekh, E.; Vinker, S.; Golan-Cohen, A.; Israel, A.; Gorohovski, A.; Frenkel-Morgenstern, M.; Stein, M. The Association of Previous Vaccination with Live-Attenuated Varicella Zoster Vaccine and COVID-19 Positivity: An Israeli Population-Based Study. Vaccines 2022, 10, 74. https://doi.org/10.3390/vaccines10010074
Merzon E, Green I, Somekh E, Vinker S, Golan-Cohen A, Israel A, Gorohovski A, Frenkel-Morgenstern M, Stein M. The Association of Previous Vaccination with Live-Attenuated Varicella Zoster Vaccine and COVID-19 Positivity: An Israeli Population-Based Study. Vaccines. 2022; 10(1):74. https://doi.org/10.3390/vaccines10010074
Chicago/Turabian StyleMerzon, Eugene, Ilan Green, Eli Somekh, Shlomo Vinker, Avivit Golan-Cohen, Ariel Israel, Alessandro Gorohovski, Milana Frenkel-Morgenstern, and Michal Stein. 2022. "The Association of Previous Vaccination with Live-Attenuated Varicella Zoster Vaccine and COVID-19 Positivity: An Israeli Population-Based Study" Vaccines 10, no. 1: 74. https://doi.org/10.3390/vaccines10010074