
The Beneficial Effect of Lomitapide on the Cardiovascular System in LDLr−/− Mice with Obesity
 , , , ,
, , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animal
2.2. Tissue Collection, Plasmatic Levels of Lipids and Glucose
2.3. Oil O Red Staining
2.4. Vascular Reactivity
2.5. Protein Expression
2.6. Gene Expression
2.7. Electrochemiluminescence Multiplex Detection
2.8. Statistical Analysis
3. Results
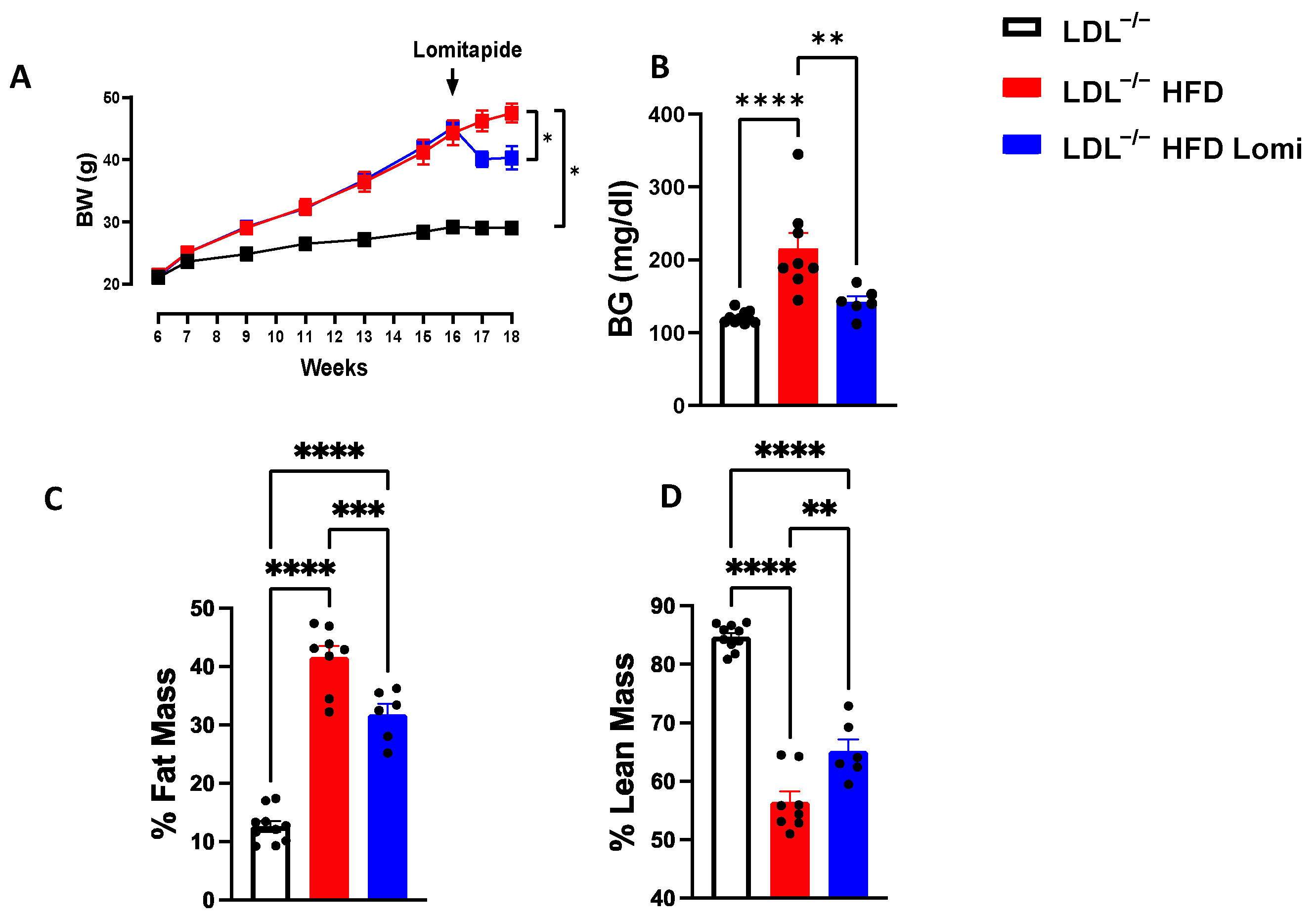
3.1. Treatment with Lomitapide Decreased Body Weight, Reduced Blood Glucose, and Enhanced Body Composition in LDLr−/− Mice on HFD
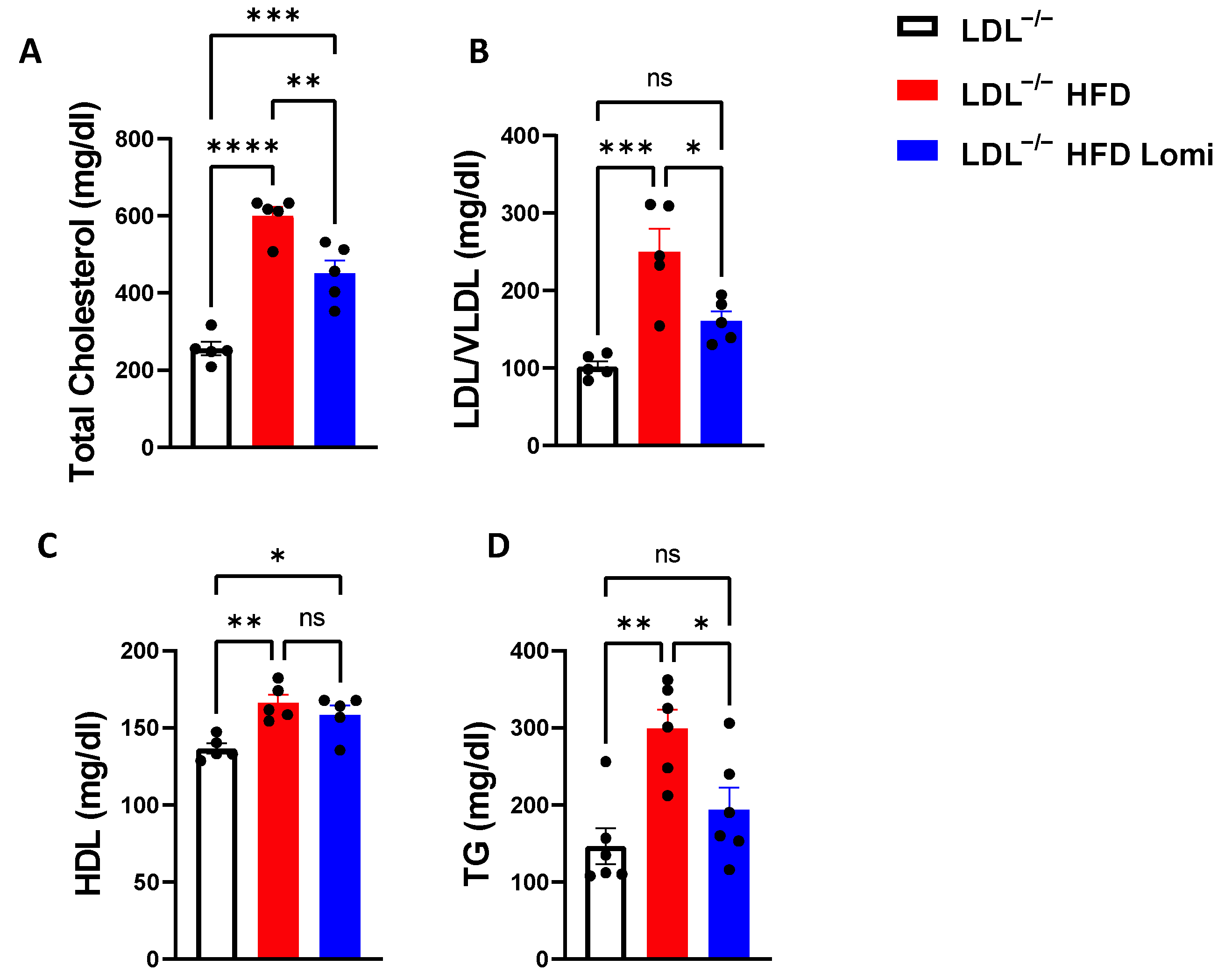
3.2. Lomitapide Treatment Decreased Lipid Profiles in LDLr−/− Mice on HFD
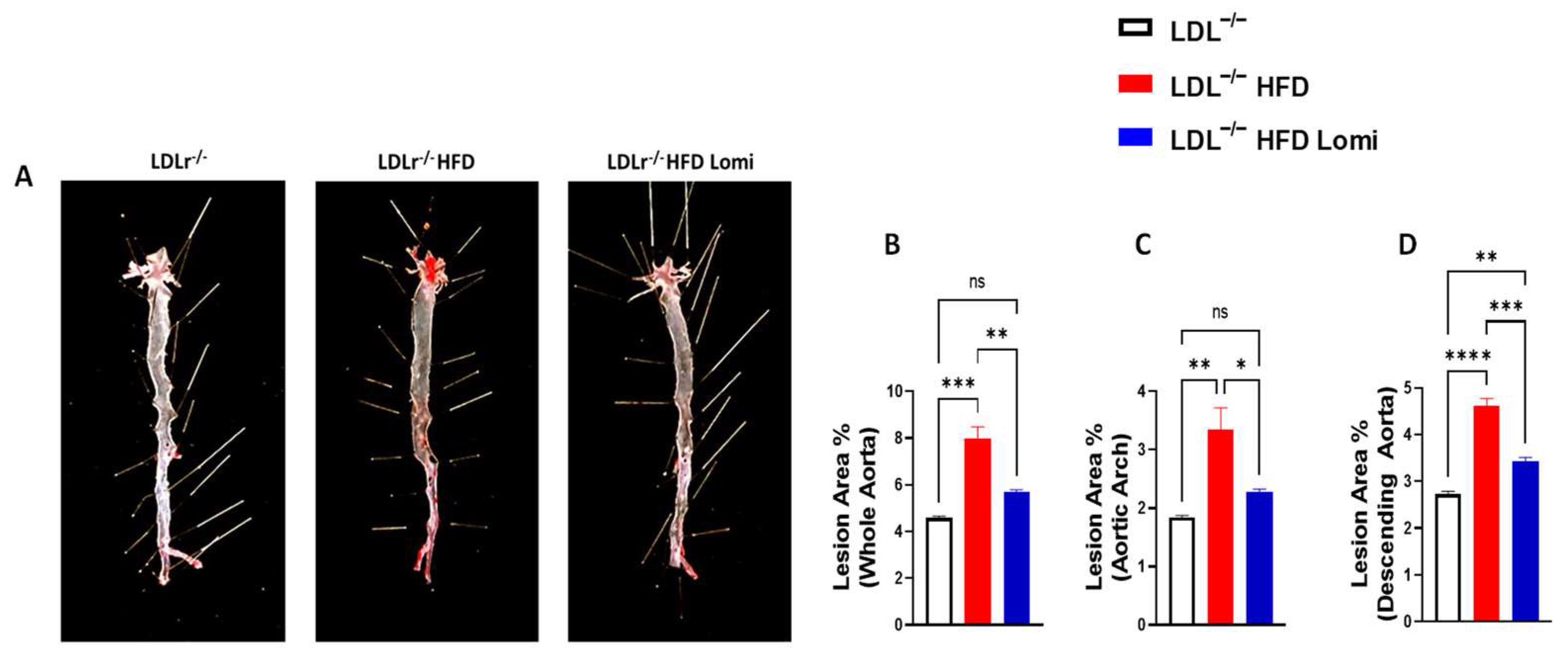
3.3. Lomitapide Decreased Plaque Surface Area in the Thoracic Aorta from LDLr−/− Mice with Obesity
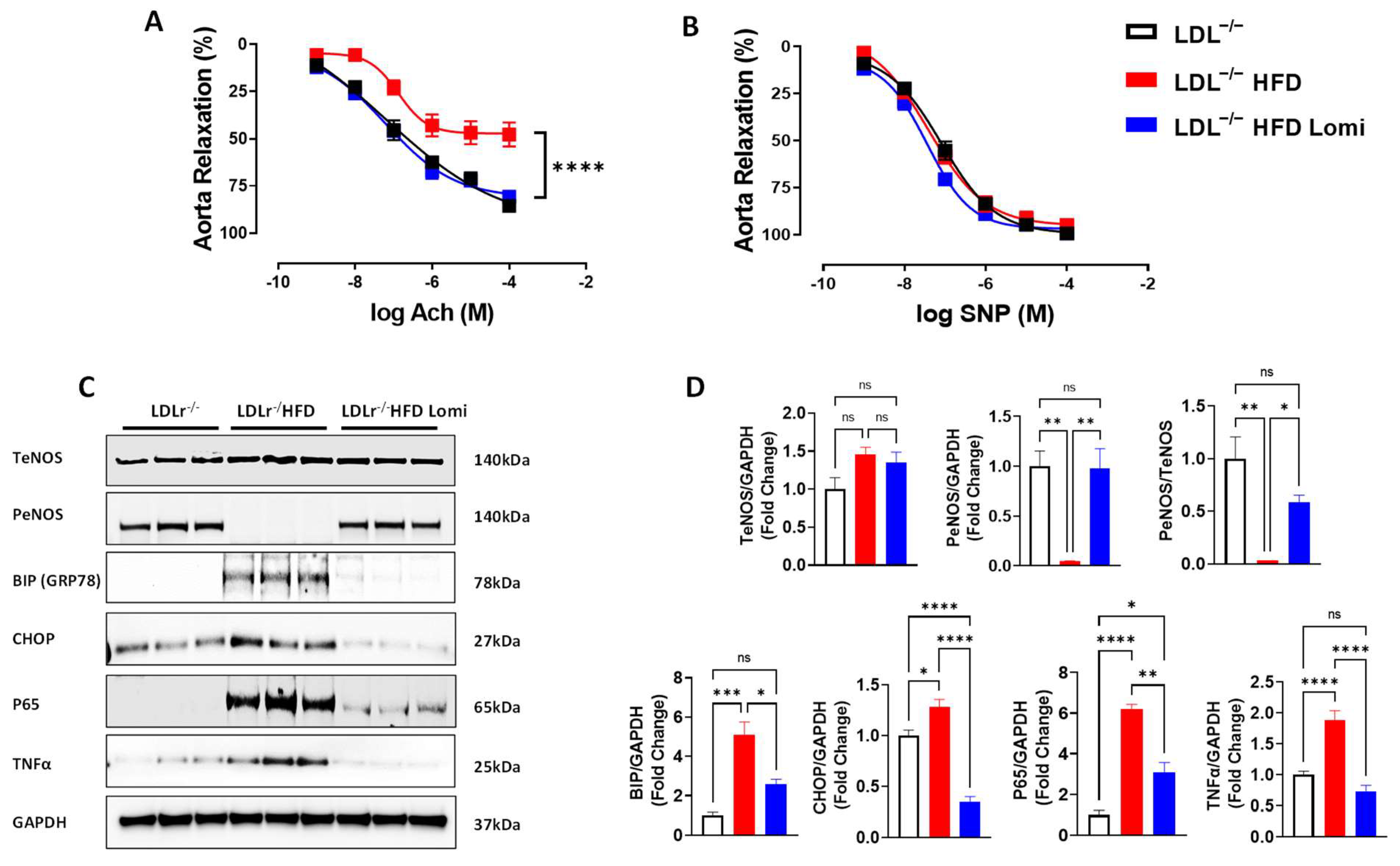
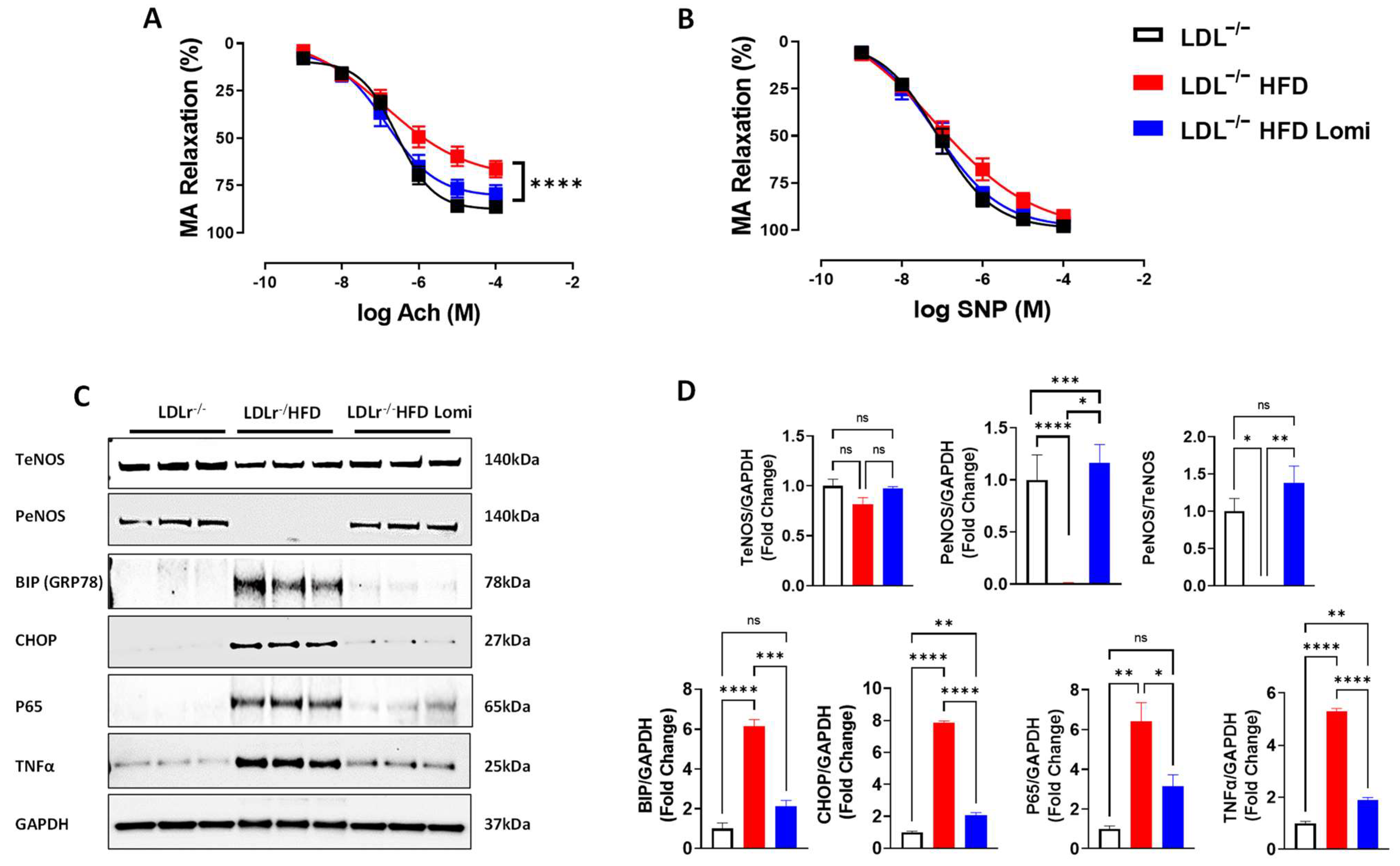
3.4. Lomitapide Improved Vascular Endothelial Function in LDLr−/− Mice on HFD
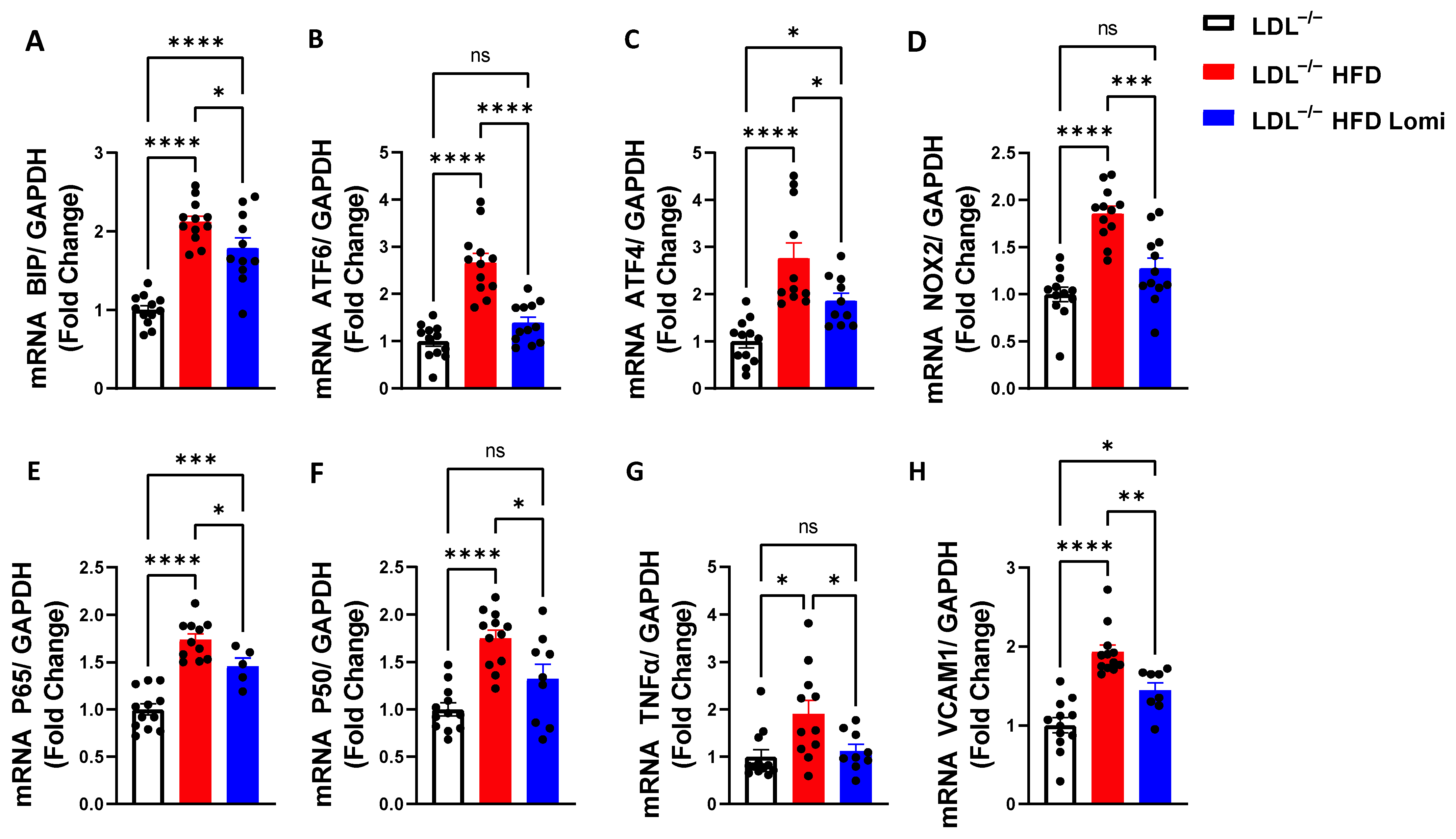
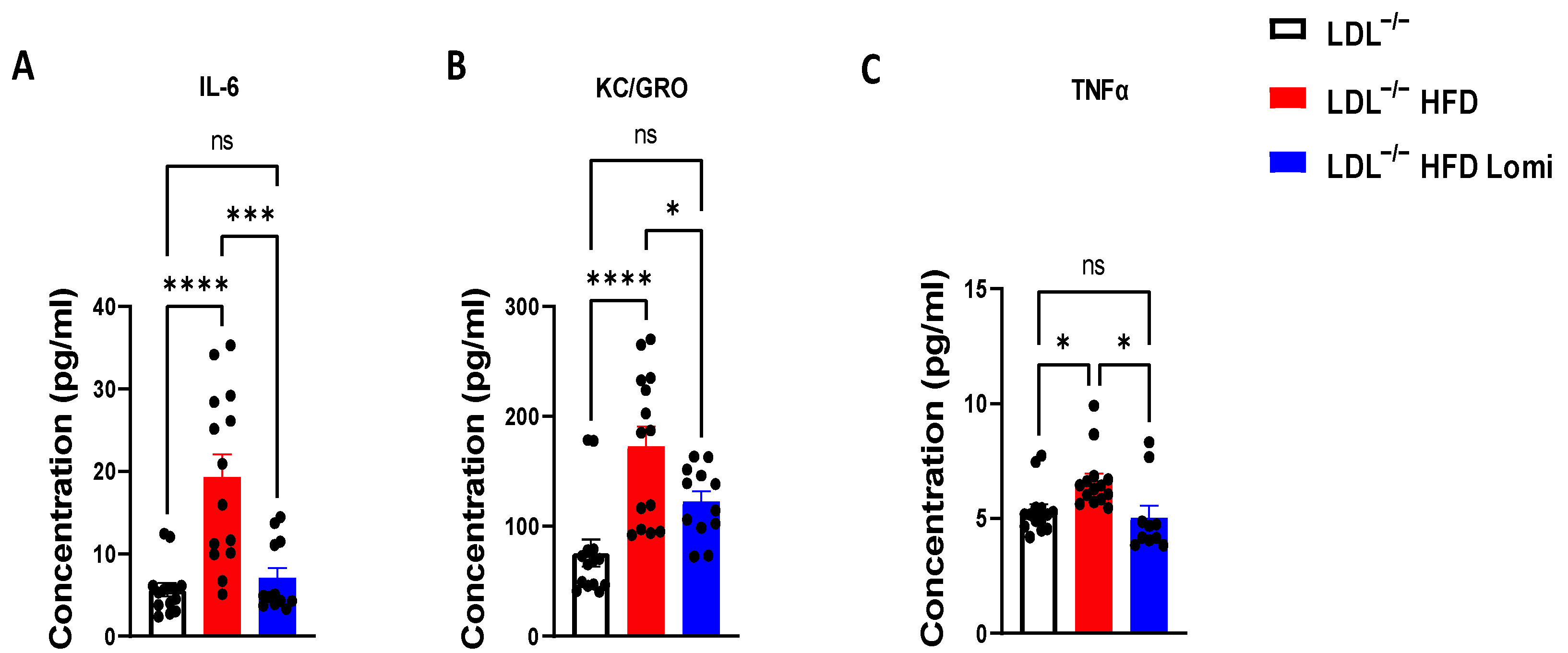
3.5. Lomitapide Beneficial Effect on Oxidative and Endoplasmic Reticulum Stress and Inflammation in LDLr−/− Mice on HFD
4. Discussion
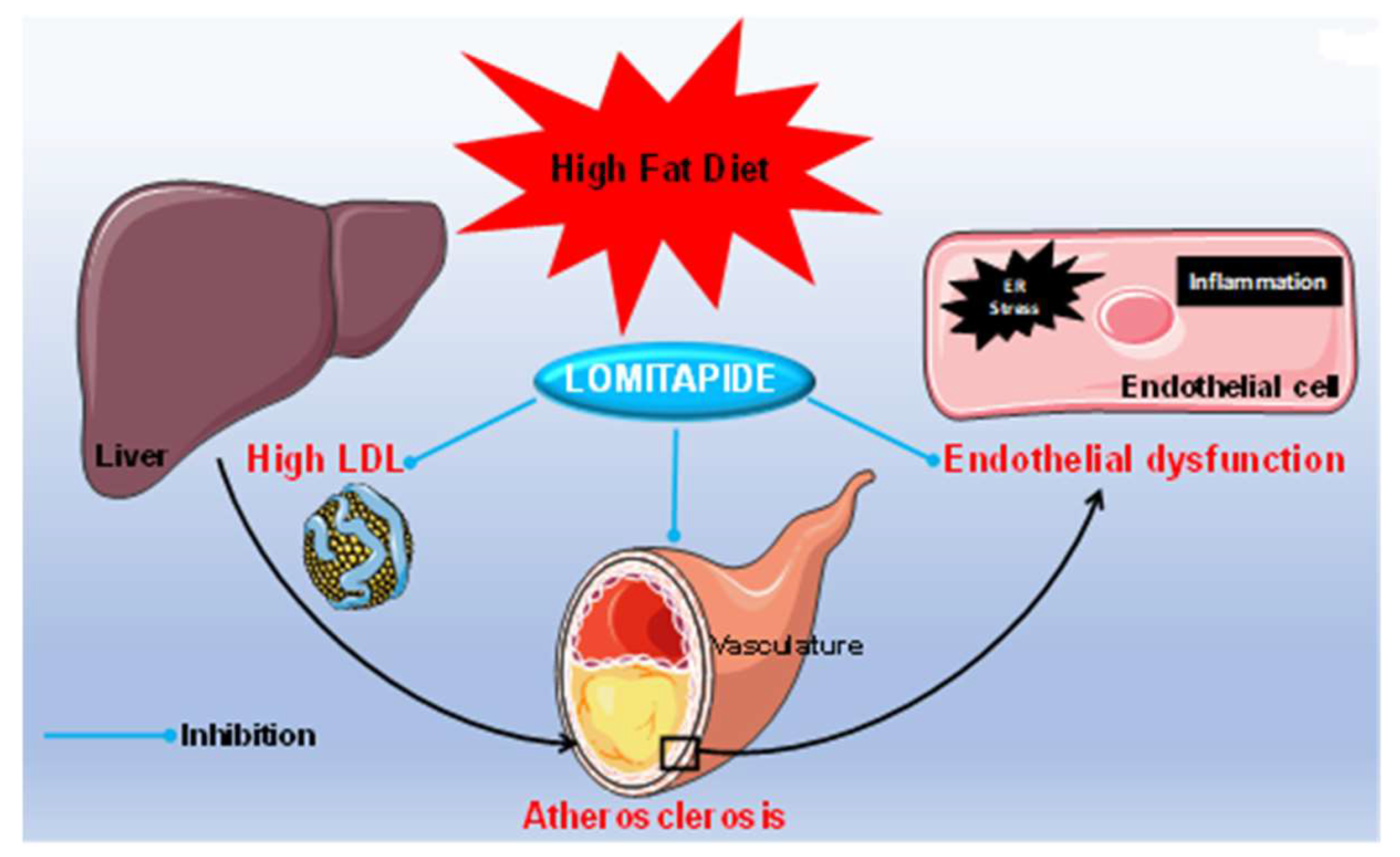
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhang, Y.; Ma, K.L.; Ruan, X.Z.; Liu, B.C. Dysregulation of the Low-Density Lipoprotein Receptor Pathway Is Involved in Lipid Disorder-Mediated Organ Injury. Int. J. Biol. Sci. 2016, 12, 569–579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rader, D.J.; Kastelein, J.J. Lomitapide and mipomersen: Two first-in-class drugs for reducing low-density lipoprotein cholesterol in patients with homozygous familial hypercholesterolemia. Circulation 2014, 129, 1022–1032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stefanutti, C. Lomitapide–A Microsomal Triglyceride Transfer Protein Inhibitor for Homozygous Familial Hypercholesterolemia. Curr. Atheroscler. Rep. 2020, 22, 38. [Google Scholar] [CrossRef] [PubMed]
- Pajkowski, M.; Dudziak, M.; Chlebus, K.; Hellmann, M. Assessment of microvascular function and pharmacological regulation in genetically confirmed familial hypercholesterolemia. Microvasc. Res. 2021, 138, 104216. [Google Scholar] [CrossRef] [PubMed]
- Pejic, R.N. Familial hypercholesterolemia. Ochsner J. 2014, 14, 669–672. [Google Scholar]
- Blom, D.J.; Averna, M.R.; Meagher, E.A.; Theron, H.D.T.; Sirtori, C.R.; Hegele, R.A.; Shah, P.K.; Gaudet, D.; Stefanutti, C.; Vigna, G.B.; et al. Long-Term Efficacy and Safety of the Microsomal Triglyceride Transfer Protein Inhibitor Lomitapide in Patients With Homozygous Familial Hypercholesterolemia. Circulation 2017, 136, 332–335. [Google Scholar] [CrossRef] [Green Version]
- Cuchel, M.; Bruckert, E.; Ginsberg, H.N.; Raal, F.J.; Santos, R.D.; Hegele, R.A.; Wiklund, O. Homozygous familial hypercholesterolaemia: New insights and guidance for clinicians to improve detection and clinical management. A position paper from the Consensus Panel on Familial Hypercholesterolaemia of the European Atherosclerosis Society. Eur. Heart J. 2014, 35, 2146–2157. [Google Scholar] [CrossRef]
- Ison, H.E.; Clarke, S.L.; Knowles, J.W. Familial Hypercholesterolemia. In GeneReviews®; Adam, M.P., Mirzaa, G.M., Pagon, R.A., Wallace, S.E., Bean, L.J., Gripp, K.W., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 1993. [Google Scholar]
- Enas, E.A.; Varkey, B.; Dharmarajan, T.; Pare, G.; Bahl, V.K. Lipoprotein(a): An independent, genetic, and causal factor for cardiovascular disease and acute myocardial infarction. Indian Heart J. 2019, 71, 99–112. [Google Scholar] [CrossRef]
- Tokgozoglu, L.; Kayikcioglu, M. Familial Hypercholesterolemia: Global Burden and Approaches. Curr. Cardiol. Rep. 2021, 23, 151. [Google Scholar] [CrossRef]
- Raal, F.J.; Rosenson, R.S.; Reeskamp, L.F.; Hovingh, G.K.; Kastelein, J.J.; Rubba, P.; Ali, S.; Banerjee, P.; Chan, K.-C.; Gipe, D.A.; et al. Evinacumab for Homozygous Familial Hypercholesterolemia. N. Engl. J. Med. 2020, 383, 711–720. [Google Scholar] [CrossRef]
- Raal, F.J.; Santos, R.D. Homozygous familial hypercholesterolemia: Current perspectives on diagnosis and treatment. Atherosclerosis 2012, 223, 262–268. [Google Scholar] [CrossRef] [PubMed]
- Thompson, G.R. Managing homozygous familial hypercholesterolaemia from cradle to grave. Atheroscler. Suppl. 2015, 18, 16–20. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, A.; Cuchel, M. Homozygous familial hypercholesterolemia: What treatments are on the horizon? Curr. Opin. Lipidol. 2020, 31, 119–124. [Google Scholar] [CrossRef]
- Cesaro, A.; Fimiani, F.; Gragnano, F.; Moscarella, E.; Schiavo, A.; Vergara, A.; Akioyamen, L.; D’erasmo, L.; Averna, M.; Arca, M.; et al. New Frontiers in the Treatment of Homozygous Familial Hypercholesterolemia. Heart Fail. Clin. 2021, 18, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Kayikcioglu, M.; Tokgozoglu, L.; Yilmaz, M.; Kaynar, L.; Aktan, M.; Durmuş, R.B.; Gokce, C.; Temizhan, A.; Ozcebe, O.I.; Akyol, T.K.; et al. A nation-wide survey of patients with homozygous familial hypercholesterolemia phenotype undergoing LDL-apheresis in Turkey (A-HIT 1 registry). Atherosclerosis 2018, 270, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Engin, A. Endothelial Dysfunction in Obesity. Adv. Exp. Med. Biol. 2017, 960, 345–379. [Google Scholar]
- Gamez-Mendez, A.M.; Vargas-Robles, H.; Ríos, A.; Escalante, B. Oxidative Stress-Dependent Coronary Endothelial Dysfunction in Obese Mice. PLoS ONE 2015, 10, e0138609. [Google Scholar] [CrossRef] [Green Version]
- Chen, M.; Masaki, T.; Sawamura, T. LOX-1, the receptor for oxidized low-density lipoprotein identified from endothelial cells: Implications in endothelial dysfunction and atherosclerosis. Pharmacol. Ther. 2002, 95, 89–100. [Google Scholar] [CrossRef]
- Zhang, X.; Sessa, W.C.; Fernández-Hernando, C. Endothelial Transcytosis of Lipoproteins in Atherosclerosis. Front. Cardiovasc. Med. 2018, 5, 130. [Google Scholar] [CrossRef] [Green Version]
- Medina-Leyte, D.J.; Zepeda-García, O.; Domínguez-Pérez, M.; González-Garrido, A.; Villarreal-Molina, T.; Jacobo-Albavera, L. Endothelial Dysfunction, Inflammation and Coronary Artery Disease: Potential Biomarkers and Promising Therapeutical Approaches. Int. J. Mol. Sci. 2021, 22, 3850. [Google Scholar] [CrossRef]
- Austin, R.C.; Lentz, S.R.; Werstuck, G.H. Role of hyperhomocysteinemia in endothelial dysfunction and atherothrombotic disease. Cell Death Differ. 2004, 11 (Suppl. S1), S56–S64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, I.V.G.; de Figueiredo, R.C.; Rios, D.R.A. Effect of Different Classes of Antihypertensive Drugs on Endothelial Function and Inflammation. Int. J. Mol. Sci. 2019, 20, 3458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ron, D. Translational control in the endoplasmic reticulum stress response. J. Clin. Investig. 2002, 110, 1383–1388. [Google Scholar] [CrossRef] [PubMed]
- Marchini, J.F.; Manica, A.; Crestani, P.; Dutzmann, J.; Folco, E.J.; Weber, H.; Libby, P.; Croce, K. Oxidized Low-Density Lipoprotein Induces Macrophage Production of Prothrombotic Microparticles. J. Am. Heart Assoc. 2020, 9, e015878. [Google Scholar] [CrossRef]
- Miyao, M.; Cicalese, S.; Cooper, H.A.; Eguchi, S. Endoplasmic reticulum stress and mitochondrial biogenesis are potential therapeutic targets for abdominal aortic aneurysm. Clin. Sci. 2019, 133, 2023–2028. [Google Scholar] [CrossRef]
- Ghosh, A.; Gao, L.; Thakur, A.; Siu, P.M.; Lai, C.W.K. Role of free fatty acids in endothelial dysfunction. J. Biomed. Sci. 2017, 24, 50. [Google Scholar] [CrossRef] [Green Version]
- Hong, J.; Kim, K.; Park, E.; Lee, J.; Markofski, M.M.; Marrelli, S.P.; Park, Y. Exercise ameliorates endoplasmic reticulum stress-mediated vascular dysfunction in mesenteric arteries in atherosclerosis. Sci. Rep. 2018, 8, 7938. [Google Scholar] [CrossRef] [Green Version]
- Goulooze, S.C.; Cohen, A.F.; Rissmann, R. Lomitapide. Br. J. Clin. Pharmacol. 2015, 80, 179–181. [Google Scholar] [CrossRef] [Green Version]
- Robl, J.A.; Sulsky, R.; Sun, C.-Q.; Simpkins, L.M.; Wang, T.; Dickson, J.K.; Chen, Y.; Magnin, D.R.; Taunk, P.; Slusarchyk, W.A.; et al. A Novel Series of Highly Potent Benzimidazole-Based Microsomal Triglyceride Transfer Protein Inhibitors. J. Med. Chem. 2001, 44, 851–856. [Google Scholar] [CrossRef]
- Chacra, A.P.M.; Ferrari, M.C.; Rocha, V.Z.; Santos, R.D. Case report: The efficacy and safety of lomitapide in a homozygous familial hypercholesterolemic child. J. Clin. Lipidol. 2019, 13, 397–401. [Google Scholar] [CrossRef]
- Cefalù, A.B.; Giammanco, A.; Noto, D.; Spina, R.; Cabibi, D.; Barbagallo, C.M.; Averna, M. Effectiveness and safety of lomitapide in a patient with familial chylomicronemia syndrome. Endocrine 2020, 71, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Lupo, M.G.; Arcidiacono, D.; Zaramella, A.; Fimiani, F.; Calabrò, P.; Cefalù, A.B.; Averna, M.; D’Erasmo, L.; Arca, M.; De Martin, S.; et al. Lomitapide does not alter PCSK9 and Lp(a) levels in homozygous familial hypercholesterolemia patients: Analysis on cytokines and lipid profile. Atheroscler. Plus 2021, 43, 7–9. [Google Scholar] [CrossRef]
- Munkhsaikhan, U.; Kwon, Y.; Sahyoun, A.M.; Ait-Aissa, K.; Kassan, A.; Kassan, M. The Microsomal Triglyceride Transfer Protein Inhibitor, Lomitapide, Improves Vascular Function in Obesity. FASEB J. 2022, 36 (Suppl. S1), 893–901. [Google Scholar] [CrossRef]
- Brautbar, A.; Ballantyne, C.M. Pharmacological strategies for lowering LDL cholesterol: Statins and beyond. Nat. Rev. Cardiol. 2011, 8, 253–265. [Google Scholar] [CrossRef] [PubMed]
- Patel, V.; Joharapurkar, A.; Kshirsagar, S.; Patel, M.; Patel, H.; Savsani, H.; Jain, M. Microsomal triglyceride transfer protein inhibitor lomitapide-induced liver toxicity is ameliorated by Triiodothyronine treatment following improved bile homeostasis and β-oxidation. Toxicol. Appl. Pharmacol. 2021, 434, 115825. [Google Scholar] [CrossRef]
- Nagy, C.; Einwallner, E. Study of In Vivo Glucose Metabolism in High-fat Diet-fed Mice Using Oral Glucose Tolerance Test (OGTT) and Insulin Tolerance Test (ITT). J. Vis. Exp. 2018, 131, e56672. [Google Scholar]
- Andrés-Manzano, M.J.; Andrés, V.; Dorado, B. Oil Red O and Hematoxylin and Eosin Staining for Quantification of Atherosclerosis Burden in Mouse Aorta and Aortic Root. Methods Mol. Biol. 2015, 1339, 85–99. [Google Scholar]
- Bourghardt, J.; Wilhelmson, A.S.K.; Alexanderson, C.; De Gendt, K.; Verhoeven, G.; Krettek, A.; Ohlsson, C.; Tivesten, A. Androgen Receptor-Dependent and Independent Atheroprotection by Testosterone in Male Mice. Endocrinology 2010, 151, 5428–5437. [Google Scholar] [CrossRef] [Green Version]
- Zhao, W.-G.; Zhu, H.-J. [Mechanism, treatment, and evaluation of obesity-induced insulin resistance and type 2 diabetes]. Zhongguo Yi Xue Ke Xue Yuan Xue Bao 2010, 32, 7–12. [Google Scholar] [CrossRef]
- Pathak, P.; Shukla, P.; Kanshana, J.S.; Jagavelu, K.; Sangwan, N.S.; Dwivedi, A.K.; Dikshit, M. Standardized root extract of Withania somnifera and Withanolide A exert moderate vasorelaxant effect in the rat aortic rings by enhancing nitric oxide generation. J. Ethnopharmacol. 2021, 278, 114296. [Google Scholar] [CrossRef]
- Kassan, M.; Vikram, A.; Li, Q.; Kim, Y.-R.; Kumar, S.; Gabani, M.; Liu, J.; Jacobs, J.S.; Irani, K. MicroRNA-204 promotes vascular endoplasmic reticulum stress and endothelial dysfunction by targeting Sirtuin1. Sci. Rep. 2017, 7, 9308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alonso, R.; Cuevas, A.; Mata, P. Lomitapide: A review of its clinical use, efficacy, and tolerability. Core Evid. 2019, 14, 19–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, Y.; Hu, Y.; Han, Z.; Yan, F.; Zhang, S.; Yang, Z.; Zhao, F.; Li, L.; Fan, J.; Wang, R.; et al. Lomitapide ameliorates middle cerebral artery occlusion-induced cerebral ischemia/reperfusion injury by promoting neuronal autophagy and inhibiting microglial migration. CNS Neurosci. Ther. 2022, 28, 2183–2194. [Google Scholar] [CrossRef] [PubMed]
- Pajkowski, M.; Chlebus, K.; Hellmann, M. Microvascular endothelial dysfunction in a young patient with familial hypercholesterolemia. Pol. Arch. Intern. Med. 2020, 130, 679–680. [Google Scholar] [CrossRef]
- Vlahos, A.P.; Naka, K.K.; Bechlioulis, A.; Theoharis, P.; Vakalis, K.; Moutzouri, E.; Miltiadous, G.; Michalis, L.K.; Siamopoulou-Mavridou, A.; Elisaf, M.; et al. Endothelial Dysfunction, But Not Structural Atherosclerosis, Is Evident Early in Children With Heterozygous Familial Hypercholesterolemia. Pediatr. Cardiol. 2014, 35, 63–70. [Google Scholar] [CrossRef]
- Kirchner, H.; Hofmann, S.M.; Fischer-Rosinský, A.; Hembree, J.; Abplanalp, W.; Ottaway, N.; Donelan, E.; Krishna, R.; Woods, S.C.; Müller, T.D.; et al. Caloric Restriction Chronically Impairs Metabolic Programming in Mice. Diabetes 2012, 61, 2734–2742. [Google Scholar] [CrossRef] [Green Version]
- Schreyer, S.A.; Wilson, D.L.; LeBoeuf, R.C. C57BL/6 mice fed high fat diets as models for diabetes-accelerated atherosclerosis. Atherosclerosis 1998, 136, 17–24. [Google Scholar] [CrossRef]
- Kameyama, N.; Maruyama, C.; Kitagawa, F.; Nishii, K.; Uenomachi, K.; Katayama, Y.; Koga, H.; Chikamoto, N.; Kuwata, Y.; Torigoe, J.; et al. Dietary Intake during 56 Weeks of a Low-Fat Diet for Lomitapide Treatment in Japanese Patients with Homozygous Familial Hypercholesterolemia. J. Atheroscler. Thromb. 2019, 26, 72–83. [Google Scholar] [CrossRef] [Green Version]
- Dhote, V.; Joharapurkar, A.; Kshirsagar, S.; Dhanesha, N.; Patel, V.; Patel, A.; Raval, S.; Jain, M. Inhibition of microsomal triglyceride transfer protein improves insulin sensitivity and reduces atherogenic risk in Zucker fatty rats. Clin. Exp. Pharmacol. Physiol. 2011, 38, 338–344. [Google Scholar] [CrossRef]
- Phillips, C.; Owens, D.; Collins, P.; Tomkin, G. Microsomal triglyceride transfer protein: Does insulin resistance play a role in the regulation of chylomicron assembly? Atherosclerosis 2002, 160, 355–360. [Google Scholar] [CrossRef]
- Church, T.; Martin, C.K. The Obesity Epidemic: A Consequence of Reduced Energy Expenditure and the Uncoupling of Energy Intake? Obesity 2018, 26, 14–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McAllister, E.J.; Dhurandhar, N.V.; Keith, S.W.; Aronne, L.J.; Barger, J.; Baskin, M.; Allison, D.B. Ten putative contributors to the obesity epidemic. Crit. Rev. Food Sci. Nutr. 2009, 49, 868–913. [Google Scholar] [CrossRef] [Green Version]
- Rosei, E.A.; Salvetti, M. Management of Hypercholesterolemia, Appropriateness of Therapeutic Approaches and New Drugs in Patients with High Cardiovascular Risk. High Blood Press. Cardiovasc. Prev. 2016, 23, 217–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lairon, D.; Lopez-Miranda, J.; Williams, C. Methodology for studying postprandial lipid metabolism. Eur. J. Clin. Nutr. 2007, 61, 1145–1161. [Google Scholar] [CrossRef] [PubMed]
- Ueshima, K.; Akihisa-Umeno, H.; Nagayoshi, A.; Takakura, S.; Matsuo, M.; Mutoh, S. Implitapide, a Microsomal Triglyceride Transfer Protein Inhibitor, Reduces Progression of Atherosclerosis in Apolipoprotein E Knockout Mice Fed a Western-Type Diet: Involvement of the Inhibition of Postprandial Triglyceride Elevation. Biol. Pharm. Bull. 2005, 28, 247–252. [Google Scholar] [CrossRef] [Green Version]
- Vakkilainen, J.; Mäkimattila, S.; Seppälä-Lindroos, A.; Vehkavaara, S.; Lahdenperä, S.; Groop, P.-H.; Taskinen, M.-R.; Yki-Järvinen, H. Endothelial Dysfunction in Men With Small LDL Particles. Circulation 2000, 102, 716–721. [Google Scholar] [CrossRef] [Green Version]
- Gimbrone, M.A., Jr.; García-Cardeña, G. Endothelial Cell Dysfunction and the Pathobiology of Atherosclerosis. Circ. Res. 2016, 118, 620–636. [Google Scholar] [CrossRef] [Green Version]








Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Munkhsaikhan, U.; Kwon, Y.I.; Sahyoun, A.M.; Galán, M.; Gonzalez, A.A.; Ait-Aissa, K.; Abidi, A.H.; Kassan, A.; Kassan, M. The Beneficial Effect of Lomitapide on the Cardiovascular System in LDLr−/− Mice with Obesity. Antioxidants 2023, 12, 1287. https://doi.org/10.3390/antiox12061287
Munkhsaikhan U, Kwon YI, Sahyoun AM, Galán M, Gonzalez AA, Ait-Aissa K, Abidi AH, Kassan A, Kassan M. The Beneficial Effect of Lomitapide on the Cardiovascular System in LDLr−/− Mice with Obesity. Antioxidants. 2023; 12(6):1287. https://doi.org/10.3390/antiox12061287
Chicago/Turabian StyleMunkhsaikhan, Undral, Young In Kwon, Amal M. Sahyoun, María Galán, Alexis A. Gonzalez, Karima Ait-Aissa, Ammaar H. Abidi, Adam Kassan, and Modar Kassan. 2023. "The Beneficial Effect of Lomitapide on the Cardiovascular System in LDLr−/− Mice with Obesity" Antioxidants 12, no. 6: 1287. https://doi.org/10.3390/antiox12061287