
Influence of Isolated Resistance Exercise on Cardiac Remodeling, Myocardial Oxidative Stress, and Metabolism in Infarcted Rats
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Design
2.2. Maximum Load-Carrying Capacity for Resistance Exercise Training
2.3. Exercise Protocol
2.4. Echocardiographic Evaluation
2.5. Tissue Collection
2.6. Histological Analysis
2.7. Metabolic Enzymes Activity
2.8. Antioxidant Enzymes Activity
2.9. Real-Time Quantitative Reverse Transcription Polymerase Chain Reaction (RT-PCR)
2.10. Statistical Analysis
3. Results
3.1. Experimental Groups and Anatomical Variables
3.2. Maximum Load-Carrying Capacity
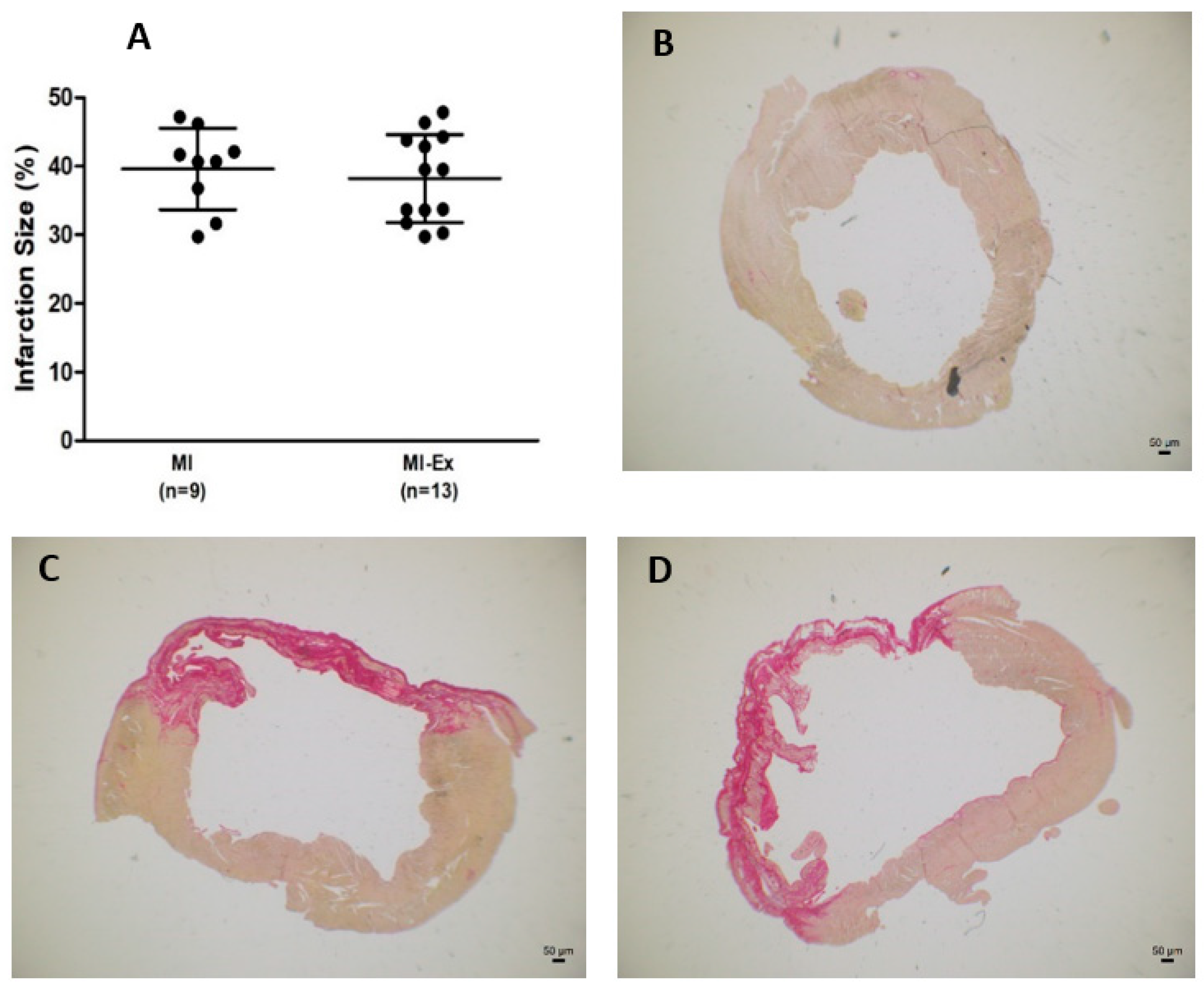
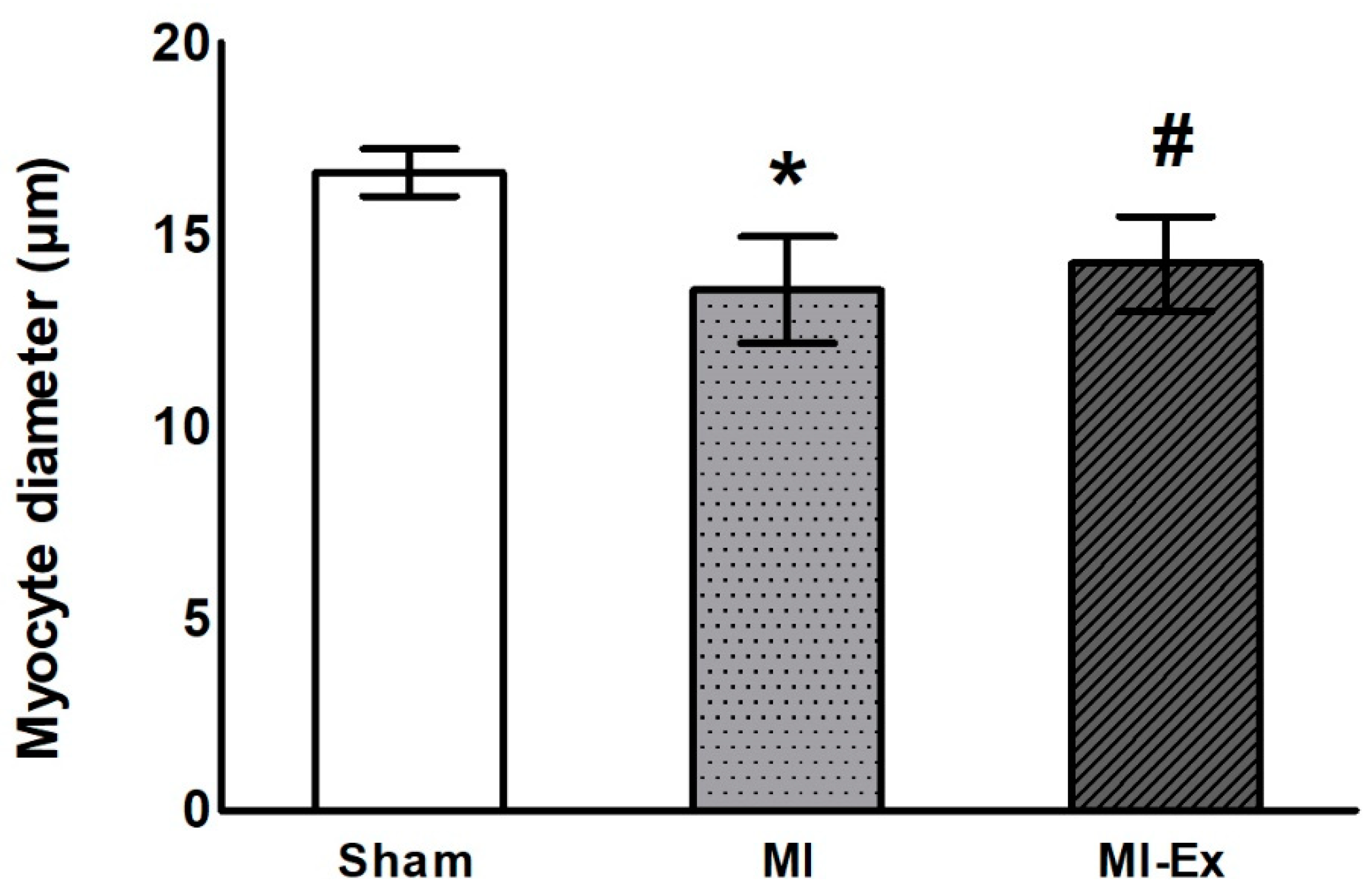
3.3. Morphometric Analysis
3.4. Echocardiographic Evaluation
3.5. Metabolic Enzyme Activity
3.6. Oxidative Stress Evaluation
3.7. Real-Time Quantitative Reverse Transcription Polymerase Chain Reaction (RT-PCR)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Anderson, C.A.M.; Arora, P.; Avery, C.L.; Baker-Smith, C.M.; Beaton, A.Z.; Boehme, A.K.; Buxton, A.E.; et al. Heart disease and stroke statistics—2023 update: A Report from the American Heart Association. Circulation 2023, 147, e93–e621. [Google Scholar] [CrossRef] [PubMed]
- Cohn, J.N.; Ferrari, R.; Sharpe, N. Cardiac remodeling-concepts and clinical implications: A consensus paper from an International Forum on Cardiac Remodeling. J. Am. Coll. Cardiol. 2000, 35, 569–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karwi, Q.G.; Uddin, G.M.; Ho, K.L.; Lopaschuk, G.D. Loss of metabolic flexibility in the failing heart. Front. Cardiovasc. Med. 2018, 5, 68. [Google Scholar] [CrossRef] [Green Version]
- Martinez, P.F.; Bonomo, C.; Guizoni, D.M.; Junior, S.A.; Damatto, R.L.; Cezar, M.D.; Lima, A.R.; Pagan, L.U.; Seiva, F.R.; Bueno, R.T.; et al. Modulation of MAPK and NF-κB signaling pathways by antioxidant therapy in skeletal muscle of heart failure rats. Cell. Physiol. Biochem. 2016, 39, 371–384. [Google Scholar] [CrossRef]
- Reyes, D.R.A.; Gomes, M.J.; Rosa, C.M.; Pagan, L.U.; Zanati, S.G.; Damatto, R.L.; Rodrigues, E.A.; Carvalho, R.F.; Fernandes, A.A.H.; Martinez, P.F.; et al. Exercise during transition from compensated left ventricular hypertrophy to heart failure in aortic stenosis rats. J. Cell. Mol. Med. 2019, 23, 1235–1245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nabeebaccus, A.A.; Reumiller, C.M.; Shen, J.; Zoccarato, A.; Santos, C.X.C.; Shah, A.M. The regulation of cardiac intermediary metabolism by NADPH oxidases. Cardiovasc. Res. 2023, 118, 3305–3319. [Google Scholar] [CrossRef]
- Del Buono, M.G.; Arena, R.; Borlaug, B.A.; Carbone, S.; Canada, J.M.; Kirkman, D.L.; Garten, R.; Rodriguez-Miguelez, P.; Guazzi, M.; Lavie, C.J.; et al. Exercise intolerance in patients with heart failure: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2019, 73, 2209–2225. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- O’Connor, C.M.; Whellan, D.J.; Lee, K.L.; Keteyian, S.J.; Cooper, L.S.; Ellis, S.J.; Leifer, E.S.; Kraus, W.E.; Kitzman, D.W.; Blumenthal, J.A.; et al. Efficacy and safety of exercise training in patients with chronic heart failure. JAMA 2009, 301, 1439–1450. [Google Scholar] [CrossRef]
- Pelliccia, A.; Sharma, S.; Gati, S.; Bäck, M.; Börjesson, M.; Caselli, S.; Collet, J.P.; Corrado, D.; Drezner, J.A.; Halle, M.; et al. 2020 ESC guidelines on sports cardiology and exercise in patients with cardiovascular disease. Eur. Heart J. 2021, 42, 17–96. [Google Scholar] [CrossRef]
- Cai, M.; Wang, Q.; Liu, Z.; Jia, D.; Feng, R.; Tian, Z. Effects of different types of exercise on skeletal muscle atrophy, antioxidant capacity and growth factors expression following myocardial infarction. Life Sci. 2018, 213, 40–49. [Google Scholar] [CrossRef] [PubMed]
- Kemi, O.J.; Høydal, M.A.; Haram, P.M.; Garnier, A.; Fortin, D.; Ventura-Clapier, R.; Ellingsen, O. Exercise training restores aerobic capacity and energy transfer systems in heart failure treated with losartan. Cardiovasc. Res. 2007, 76, 91–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grans, C.F.; Feriani, D.J.; Abssamra, M.E.; Rocha, L.Y.; Carrozzi, N.M.; Mostarda, C.; Figueroa, D.M.; Angelis, K.D.; Irigoyen, M.C.; Rodrigues, B. Resistance training after myocardial infarction in rats: Its role on cardiac and autonomic function. Arq. Bras. Cardiol. 2014, 103, 60–68. [Google Scholar] [CrossRef]
- Garza, M.A.; Wason, E.A.; Cruger, J.R.; Chung, E.; Zhang, J.Q. Strength training attenuates post-infarct cardiac dysfunction and remodeling. J. Physiol. Sci. 2019, 69, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Alves, J.P.; Nunes, R.B.; Ferreira, D.D.C.; Stefani, G.P.; Jaenisch, R.B.; Dal Lago, P. High-intensity resistance training alone or combined with aerobic training improves strength, heart function and collagen in rats with heart failure. Am. J. Transl. Res. 2017, 9, 5432–5441. [Google Scholar]
- Fisher, S.; Smart, N.A.; Pearson, M.J. Resistance training in heart failure patients: A systematic review and meta-analysis. Heart Fail. Rev. 2022, 27, 1665–1682. [Google Scholar] [CrossRef]
- Karlsdottir, A.E.; Foster, C.; Porcari, J.P.; Palmer-McLean, K.; White-Kube, R.; Backes, R.C. Hemodynamic responses during aerobic and resistance exercise. J. Cardiopulm. Rehabil. 2002, 22, 170–177. [Google Scholar] [CrossRef]
- Williams, M.A.; Haskell, W.L.; Ades, P.A.; Amsterdam, E.A.; Bittner, V.; Franklin, B.A.; Gulanick, M.; Laing, S.T.; Stewart, K.J. Resistance exercise in individuals with and without cardiovascular disease: 2007 update: A Scientific Statement from the American Heart Association Council on Clinical Cardiology and Council on Nutrition, Physical Activity, and Metabolism. Circulation 2007, 116, 572–584. [Google Scholar] [CrossRef] [Green Version]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: Executive summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2022, 79, 1757–1780. [Google Scholar] [CrossRef]
- Gomes, M.J.; Pagan, L.; Lima, A.R.R.; Reyes, D.R.A.; Martinez, P.F.; Damatto, F.C.; Pontes, T.H.D.; Rodrigues, E.A.; Souza, L.M.; Tosta, I.F.; et al. Effects of aerobic and resistance exercise on cardiac remodelling and skeletal muscle oxidative stress of infarcted rats. J. Cell. Mol. Med. 2020, 24, 5352–5362. [Google Scholar] [CrossRef] [Green Version]
- Okoshi, K.; Ribeiro, H.B.; Okoshi, M.P.; Matsubara, B.B.; Gonçalves, G.; Barros, R.; Cicogna, A.C. Improved systolic ventricular function with normal myocardial mechanics in compensated cardiac hypertrophy. Jpn. Heart J. 2004, 45, 647–656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lima, A.R.; Martinez, P.F.; Damatto, R.L.; Cezar, M.D.; Guizoni, D.M.; Bonomo, C.; Oliveira, S.A., Jr.; Dal-Pai Silva, M.; Zornoff, L.A.; Okoshi, K.; et al. Heart failure-induced diaphragm myopathy. Cell. Physiol. Biochem. 2014, 34, 333–345. [Google Scholar] [CrossRef] [PubMed]
- Sugizaki, M.M.; Carvalho, R.F.; Aragon, F.F.; Padovani, C.R.; Okoshi, K.; Okoshi, M.P.; Zanati, S.G.; Pai-Silva, M.D.; Novelli, E.L.; Cicogna, A.C. Myocardial dysfunction induced by food restriction is related to morphological damage in normotensive middle-aged rats. J. Biomed. Sci. 2005, 12, 641–649. [Google Scholar] [CrossRef]
- Souza, L.M.; Gomes, M.J.; Brandao, B.B.; Pagan, L.U.; Gatto, M.; Damatto, F.C.; Rodrigues, E.A.; Pontes, T.H.D.; Borim, P.A.; Fernandes, A.A.H.; et al. Effects of resistance exercise on slow-twitch soleus muscle of infarcted rats. Antioxidants 2023, 12, 291. [Google Scholar] [CrossRef]
- Cezar, M.D.M.; Damatto, R.L.; Martinez, P.F.; Lima, A.R.R.; Campos, D.H.S.; Rosa, C.M.; Guizoni, D.M.; Bonomo, C.; Cicogna, A.C.; Gimenes, R.; et al. Aldosterone blockade reduces mortality without changing cardiac remodeling in spontaneously hypertensive rats. Cell. Physiol. Biochem. 2013, 32, 1275–1287. [Google Scholar] [CrossRef] [PubMed]
- Gimenes, C.; Gimenes, R.; Rosa, C.M.; Xavier, N.P.; Campos, D.H.; Fernandes, A.A.; Cezar, M.D.; Guirado, G.N.; Cicogna, A.C.; Takamoto, A.H.; et al. Low intensity physical exercise attenuates cardiac remodeling and myocardial oxidative stress and dysfunction in diabetic rats. J. Diabetes Res. 2015, 2015, 457848. [Google Scholar] [CrossRef] [Green Version]
- Gimenes, R.; Gimenes, C.; Rosa, C.M.; Xavier, N.P.; Campos, D.H.S.; Fernandes, A.A.H.; Cezar, M.D.M.; Guirado, G.N.; Pagan, L.U.; Chaer, I.D.; et al. Influence of apocynin on cardiac remodeling in rats with streptozotocin-induced diabetes mellitus. Cardiovasc. Diabetol. 2018, 17, 15. [Google Scholar] [CrossRef]
- Okoshi, K.; Fioretto, J.R.; Okoshi, M.P.; Cicogna, A.C.; Aragon, F.F.; Matsubara, L.S.; Matsubara, B.B. Food restriction induces in vivo ventricular dysfunction in spontaneously hypertensive rats without impairment of in vitro myocardial contractility. Braz. J. Med. Biol. Res. 2004, 37, 607–613. [Google Scholar] [CrossRef] [Green Version]
- Martinez, P.F.; Bonomo, C.; Guizoni, D.M.; Junior, S.A.; Damatto, R.L.; Cezar, M.D.; Lima, A.R.; Pagan, L.U.; Seiva, F.R.; Fernandes, D.C.; et al. Influence of N-acetylcysteine on oxidative stress in slow-twitch soleus muscle of heart failure rats. Cell. Physiol. Biochem. 2015, 35, 148–159. [Google Scholar] [CrossRef]
- Souza, L.M.; Okoshi, M.P.; Gomes, M.J.; Gatto, M.; Rodrigues, E.A.; Pontes, T.H.D.; Damatto, F.C.; Oliveira, L.R.S.; Borim, P.A.; Lima, A.R.R.; et al. Effects of late aerobic exercise on cardiac remodeling of rats with small-sized myocardial infarction. Arq. Bras. Cardiol. 2021, 116, 784–792. [Google Scholar] [CrossRef]
- Gomes, M.J.; Martinez, P.F.; Campos, D.H.; Pagan, L.U.; Bonomo, C.; Lima, A.R.; Damatto, R.L.; Cezar, M.D.; Damatto, F.C.; Rosa, C.M.; et al. Beneficial effects of physical exercise on functional capacity and skeletal muscle oxidative stress in rats with aortic stenosis-induced heart failure. Oxid. Med. Cell. Longev. 2016, 2016, 8695716. [Google Scholar] [CrossRef] [Green Version]
- Reyes, D.R.A.; Gomes, M.J.; Rosa, C.M.; Pagan, L.U.; Damatto, F.C.; Damatto, R.L.; Depra, I.; Campos, D.H.S.; Fernandez, A.A.H.; Martinez, P.F.; et al. N-acetylcysteine influence on oxidative stress and cardiac remodeling in rats during transition from compensated left ventricular hypertrophy to heart failure. Cell. Physiol. Biochem. 2017, 44, 2310–2321. [Google Scholar] [CrossRef]
- Okoshi, K.; Cezar, M.D.M.; Polin, M.A.M.; Paladino, J.R., Jr.; Martinez, P.F.; Oliveira, S.A., Jr.; Lima, A.R.R.; Damatto, R.L.; Paiva, S.A.R.; Zornoff, L.A.M.; et al. Influence of intermittent fasting on myocardial infarction-induced cardiac remodeling. BMC Cardiovasc. Disord. 2019, 19, 126. [Google Scholar] [CrossRef]
- Guizoni, D.M.; Oliveira-Junior, S.A.; Noor, S.L.; Pagan, L.U.; Martinez, P.F.; Lima, A.R.; Gomes, M.J.; Damatto, R.L.; Cezar, M.D.; Bonomo, C.; et al. Effects of late exercise on cardiac remodeling and myocardial calcium handling proteins in rats with moderate and large size myocardial infarction. Int. J. Cardiol. 2016, 221, 406–412. [Google Scholar] [CrossRef] [Green Version]
- Minicucci, M.F.; Azevedo, P.S.; Martinez, P.F.; Lima, A.R.; Bonomo, C.; Guizoni, D.M.; Polegato, B.F.; Okoshi, M.P.; Okoshi, K.; Matsubara, B.B.; et al. Critical infarct size to induce ventricular remodeling, cardiac dysfunction and heart failure in rats. Int. J. Cardiol. 2011, 151, 242–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindsey, M.L.; Brunt, K.R.; Kirk, J.A.; Kleinbongard, P.; Calvert, J.W.; de Castro Brás, L.E.; DeLeon-Pennell, K.Y.; Del Re, D.P.; Frangogiannis, N.G. Guidelines for in vivo mouse models of myocardial infarction. Am. J. Physiol. Circ. Physiol. 2021, 32, H1056–H1073. [Google Scholar] [CrossRef]
- Suzuki, T.; Palus, S.; Springer, J. Skeletal muscle wasting in chronic heart failure. ESC Heart Fail. 2018, 5, 1099–1107. [Google Scholar] [CrossRef]
- Okoshi, M.P.; Romeiro, F.G.; Paiva, S.A.R.; Okoshi, K. Heart failure-induced cachexia. Arq. Bras. Cardiol. 2013, 100, 476–482. [Google Scholar] [CrossRef] [PubMed]
- Kitagawa, T.; Hiraya, K.; Denda, T.; Yamamoto, S. A comparison of different exercise intensities for improving bone mineral density in postmenopausal women with osteoporosis: A systematic review and meta-analysis. Bone Rep. 2022, 17, 101631. [Google Scholar] [CrossRef] [PubMed]
- Correia, R.R.; Veras, A.S.C.; Tebar, W.R.; Rufino, J.C.; Batista, V.R.G.; Teixeira, G.R. Strength training for arterial hypertension treatment: A systematic review and meta-analysis of randomized clinical trials. Sci. Rep. 2023, 13, 201. [Google Scholar] [CrossRef] [PubMed]
- Guirado, G.N.; Damatto, R.L.; Matsubara, B.B.; Roscani, M.G.; Fusco, D.R.; Cicchetto, L.A.; Seki, M.M.; Teixeira, A.S.; Valle, A.P.; Okoshi, K.; et al. Combined exercise training in asymptomatic elderly with controlled hypertension: Effects on functional capacity and cardiac diastolic function. Med. Sci. Monit. 2012, 18, CR461–CR465. [Google Scholar] [CrossRef] [Green Version]
- Zornoff, L.A.M.; Paiva, S.A.R.; Duarte, D.R.; Spadaro, J. Remodelação ventricular pós-infarto do miocárdio: Conceitos e implicações clínicas. Arq. Bras. Cardiol. 2009, 92, 157–164. [Google Scholar] [CrossRef] [Green Version]
- Sanchis-Gomar, F.; Lavie, C.J.; Marín, J.; Perez-Quilis, C.; Eijsvogels, T.M.H.; O’Keefe, J.H.; Perez, M.V.; Blair, S.N. Exercise effects on cardiovascular disease: From basic aspects to clinical evidence. Cardiovasc. Res. 2022, 118, 2253–2266. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.; Addetia, K.; Singh, A. Echocardiographic evaluation of the athlete’s heart: Focused review and update. Curr. Cardiol. Rep. 2022, 24, 1907–1916. [Google Scholar] [CrossRef] [PubMed]
- Mascia, G.; Arbelo, E.; Porto, I.; Brugada, R.; Brugada, J. The arrhythmogenic right ventricular cardiomyopathy in comparison to the athletic heart. J. Cardiovasc. Electrophysiol. 2020, 31, 1836–1843. [Google Scholar] [CrossRef] [PubMed]
- Bae, J.; Paltzer, W.G.; Mahmoud, A.I. The role of metabolism in heart failure and regeneration. Front. Cardiovasc. Med. 2021, 8, 702920. [Google Scholar] [CrossRef]
- Lopaschuk, G.D.; Karwi, Q.G.; Tian, R.; Wende, A.R.; Abel, E.D. Cardiac energy metabolism in heart failure. Circ. Res. 2021, 128, 1487–1513. [Google Scholar] [CrossRef] [PubMed]
- Gibb, A.A.; Hill, B.G. Metabolic coordination of physiological and pathological cardiac remodeling. Circ. Res. 2018, 123, 107–128. [Google Scholar] [CrossRef] [PubMed]
- Pagan, L.U.; Gomes, M.J.; Gatto, M.; Mota, G.A.F.; Okoshi, K.; Okoshi, M.P. The role of oxidative stress in the aging heart. Antioxidants 2022, 11, 336. [Google Scholar] [CrossRef]
- Gupta, A.; Akki, A.; Wang, Y.; Leppo, M.K.; Chacko, V.P.; Foster, D.B.; Caceres, V.; Shi, S.; Kirk, J.A.; Su, J.; et al. Creatine kinase–mediated improvement of function in failing mouse hearts provides causal evidence the failing heart is energy starved. J. Clin. Investig. 2012, 122, 291–302. [Google Scholar] [CrossRef] [Green Version]
- Altenhöfer, S.; Radermacher, K.A.; Kleikers, P.W.M.; Wingler, K.; Schmidt, H.H.H.W. Evolution of NADPH oxidase inhibitors: Selectivity and mechanisms for target engagement. Antioxid. Redox Signal. 2015, 23, 406–427. [Google Scholar] [CrossRef] [PubMed]
- Powers, S.K.; Goldstein, E.; Schrager, M.; Ji, L.L. Exercise training and skeletal muscle antioxidant enzymes: An update. Antioxidants 2022, 12, 39. [Google Scholar] [CrossRef] [PubMed]
- Gomes, M.J.; Martinez, P.F.; Pagan, L.U.; Damatto, R.L.; Cezar, M.D.M.; Lima, A.R.R.; Okoshi, K.; Okoshi, M.P. Skeletal muscle aging: Influence of oxidative stress and physical exercise. Oncotarget 2017, 8, 20428–20440. [Google Scholar] [CrossRef] [Green Version]
- Liu, F.; Fan, L.M.; Geng, L.; Li, J.M. p47phox-dependent oxidant signalling through ASK1, MKK3/6 and MAPKs in angiotensin II-induced cardiac hypertrophy and apoptosis. Antioxidants 2021, 10, 1363. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Frequency (n, %) | ||
|---|---|---|
| MI (n = 9) | MI-Ex (n = 13) | |
| Atria thrombi | 11.1 (1) | 23.1 (3) |
| Pleuro-pericardial effusion | 11.1 (1) | 30.8 (4) |
| Hepatic congestion | 33.3 (3) | 23.1 (3) |
| Right ventricular hypertrophy | 33.3 (3) | 30.8 (4) |
| Ascites | 22.2 (2) | 15.4 (2) |
| Sham (n = 14) | MI (n = 9) | MI-Ex (n = 13) | |
|---|---|---|---|
| BW (g) | 552 (527–582) | 531 (511–572) | 526 (476–570) |
| RV (g) | 0.24 (0.21–0.26) | 0.36 (0.30–0.43) * | 0.34 (0.30–0.50) * |
| RV/BW (mg/g) | 0.43 (0.41–0.45) | 0.71 (0.52–0.86) * | 0.65 (0.56–0.94) * |
| Atria (mg) | 0.10 (0.09–0.14) | 0.15 (0.11–0.31) * | 0.16 (0.14–0.19) * |
| Atria/BW (mg/g) | 0.19 (0.16–0.32) | 0.32 (0.22–0.54) * | 0.33 (0.24–0.49) * |
| Lung (g) | 1.98 ± 0.68 | 2.98 ± 0.89 * | 2.64 ± 0.70 |
| Lung/BW (mg/g) | 3.65 (3.19–3.70) | 5.18 (4.43–7.24) * | 4.82 (3.77–5.27) |
| Sham (n = 4) | MI (n = 7) | MI-Ex (n = 13) | |
|---|---|---|---|
| Initial (g) | 416 ± 90 | 281 ± 70 * | 342 ± 81 |
| Final (g) | 306 ± 144 | 349 ± 143 | 617 ± 169 *,#,& |
| Sham (n = 14) | MI (n = 9) | MI-Ex (n = 13) | |
|---|---|---|---|
| BW (g) | 471 ± 47 | 458 ± 43 | 447 ± 47 |
| LVDD (mm) | 8.07 ± 0.44 | 10.53 ± 0.69 * | 10.16 ± 1.07 * |
| LVDD/BW (mm/kg) | 17.3 ± 1.39 | 23.2 ± 2.68 * | 22.8 ± 2.56 * |
| LVSD (mm) | 4.10 (3.81–4.30) | 8.16 (7.99–8.62) * | 7.89 (7.23–8.55) * |
| DPWT (mm) | 1.33 (1.27–1.37) | 1.65 (1.54–1.95) * | 1.65 (1.49–1.74) * |
| AO (mm) | 4.01 (3.83–4.01) | 3.94 (3.78–4.01) | 3.83 (3.61–4.01) |
| LA (mm) | 5.29 (5.11–5.66) | 7.66 (6.70–8.27) * | 6.75 (6.27–7.41) * |
| LA/AO | 1.35 (1.32–1.39) | 1.94 (1.67–2.27) * | 1.80 (1.55–1.99) * |
| LA/BW (mm/kg) | 11.6 (10.4–12.3) | 17.4 (13.9–19.5) * | 15.3 (13.3–17.5) * |
| End-diast. area (mm2) | 44.2 ± 7.43 | 89.5 ± 14.7 * | 80.5 ± 14.3 * |
| End-sist. area (mm2) | 15.6 (12.5–18.0) | 61.6 (55.6–72.1) * | 52.2 (43.1–58.9) * |
| Sham (n = 14) | MI (n = 9) | MI-Ex (n = 13) | |
|---|---|---|---|
| HR (bpm) | 292 ± 25 | 295 ± 26 | 275 ± 24 |
| EF | 0.86 (0.84–0.89) | 0.51 (0.43–0.57) * | 0.50 (0.42–0.58) * |
| PWSV (mm/s) | 40.5 ± 5.58 | 24.5 ± 7.67* | 28.6 ± 8.37 * |
| Tei index | 0.47 (0.44–0.53) | 0.74 (0.63–0.89) * | 0.76 (0.63–0.81) * |
| FAC (%) | 65.7 ± 5.52 | 28.6 ± 8.19 * | 33.7 ± 7.59 * |
| Mitral E (cm/s) | 80.3 ± 7.53 | 99.1 ± 16.5 * | 88.5 ± 18.3 |
| Mitral A (cm/s) | 47 (45–55) | 44 (21–64) | 42 (23–58) |
| E/A | 1.65 (1.47–1.82) | 2.02 (1.44–5.27) | 1.63 (1.41–4.70) |
| IVRT (ms) | 26 (22–26) | 30 (26–33) | 30 (25–32) |
| TDI S’ (average, cm/s) | 3.47 ± 0.33 | 3.13 ± 0.36 | 2.90 ± 0.46 * |
| TDI E’ (average, cm/s) | 4.15 ± 0.72 | 4.10 ± 0.52 | 3.76 ± 0.50 |
| E/TDI E’ (average) | 19.8 ± 3.69 | 24.5 ± 5.38 * | 24.5 ± 6.44 * |
| Sham (n = 14) | MI (n = 9) | MI-Ex (n = 13) | |
|---|---|---|---|
| LVDD (mm) | 8.34 ± 0.43 | 11.1 ± 0.88 * | 10.9 ± 0.82 * |
| LVDD/BW (mm/kg) | 15.1 (14.3–15.9) | 21.5 (18.5–22.2) * | 20.8 (19.8–22.3) * |
| LVSD (mm) | 4.09 ± 0.38 | 8.96 ± 1.33 * | 8.62 ± 1.16 * |
| DPWT (mm) | 1.42 (1.38–1.43) | 1.80 (1.64–2.01) * | 1.69 (1.60–1.73) * |
| AO (mm) | 4.21 ± 0.15 | 4.01 ± 0.23 | 4.06 ± 0.27 |
| LA (mm) | 5.68 ± 0.46 | 8.23 ± 1.30 * | 7.80 ± 1.26 * |
| LA/AO | 1.38 (1.24–1.44) | 2.22 (1.63–2.34) * | 1.86 (1.78–2.23) * |
| LA/BW (mm/kg) | 10.1 (9.21–11.1) | 15.9 (12.0–17.5) * | 14.7 (12.8–17.1) * |
| End-diast. area (mm2) | 49 (47–51) | 90 (85–96) * | 94 (80–106) * |
| End-sist. area (mm2) | 15 (14–18) | 65 (56–72) * | 60 (47–76) * |
| Sham (n = 14) | MI (n = 9) | MI-Ex (n = 13) | |
|---|---|---|---|
| HR (bpm) | 280 ± 39 | 300 ± 32 | 292 ± 21 |
| EF | 0.88 (0.87–0.90) | 0.46 (0.40–0.54) * | 0.53 (0.42–0.59) * |
| PWSV (mm/s) | 42 ± 6.2 | 25 ± 9.4 * | 28 ± 6.2 * |
| Tei index | 0.47 ± 0.06 | 0.62 ± 0.14 * | 0.66 ± 0.12 * |
| FAC (%) | 67.3 ± 4.90 | 29.6 ± 8.92 * | 34.4 ± 12.2 * |
| Mitral E (cm/s) | 77 (74–86) | 102 (79–120) | 78 (72–121) |
| Mitral A (cm/s) | 51 ± 15 | 39 ± 28 | 47 ± 21 |
| E/A | 1.71 (1.41–1.80) | 4.27 (1.30–5.99) | 1.41 (1.24–5.53) |
| IVRT (ms) | 25 ± 3.7 | 27 ± 5.2 | 27 ± 4.3 |
| TDI S’ (average, cm/s) | 3.55 ± 0.36 | 2.80 ± 0.49 * | 2.93 ± 0.45 * |
| TDI E’ (average, cm/s) | 4.16 ± 0.68 | 4.18 ± 0.76 | 3.92 ± 0.56 |
| E/TDI E’ (average) | 18 (16–21) | 23 (20–25) | 22 (19–28) |
| Sham (n = 9) | MI (n = 9) | MI-Ex (n = 10) | |
|---|---|---|---|
| PFK (nmol/min·g of protein) | 23.7 (20.5–28.3) | 22.1 (15.0–27.9) | 25.3 (22.9–28.3) |
| PK (nmol/min·g of protein) | 235 ± 38.8 | 204 ± 23.1 | 225 ± 40.6 |
| LDH (nmol/min·g of protein) | 1241 ± 131 | 1034 ± 112 * | 1129 ± 157 |
| CS (umol/min·g of protein) | 293 ± 33 | 207 ± 48 * | 232 ± 55 * |
| CK (nmol/min·g of protein) | 30.8 ± 4.93 | 24.8 ± 4.91 * | 28.8 ± 3.86 |
| CPT1 (nmol/min·g of protein) | 16.8 ± 4.46 | 22.2 ± 6.56 | 22.6 ± 6.76 |
| Sham (n = 7) | MI (n = 8) | MI-Ex (n = 8) | |
|---|---|---|---|
| Superoxide dismutase (nmol/g of tissue) | 7.49 (6.22–8.87) | 6.67 (5.67–7.25) | 5.78 (5.36–6.13) |
| Catalase (µmol/g of tissue) | 54.2 ± 8.31 | 47.3 ± 10.34 * | 40.8 ± 6.97 * |
| Glutathione peroxidase (nmol/g of protein) | 30.0 ± 5.70 | 29.3 ± 6.95 | 29.7 ± 7.66 |
| Sham (n = 7) | MI (n = 8) | MI-Ex (n = 8) | |
|---|---|---|---|
| Malondialdehyde (nmol/mg of protein) | 4.98 (4.77–5.29) | 5.46 (3.71–7.89) | 4.88 (4.36–9.82) |
| Protein carbonylation (nmol/mg of protein) | 3.12 (3.05–3.26) | 3.02 (2.82–3.14) | 3.14 (3.10–3.21) |
| Lipid hydroperoxide (nmol/g of tissue) | 160 (128–187) | 204 (182–244) | 128 (118–152) # |
| Sham (n = 8) | MI (n = 6) | MI-Ex (n = 8) | |
|---|---|---|---|
| Nox2 | 0.98 (0.87–1.07) | 1.43 (1.19–2.30) | 1.96 (1.05–2.76) * |
| Nox4 | 0.97 ± 0.43 | 1.60 ± 0.41 * | 1.57 ± 0.58 * |
| p22phox | 0.99 (0.96–1.03) | 1.06 (0.89–1.20) | 1.32 (1.02–1.51) * |
| p47phox | 0.98 (0.78–1.12) | 0.66 (0.60–0.68) * | 0.81 (0.58–0.95) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodrigues, E.A.; Lima, A.R.R.; Gomes, M.J.; Souza, L.M.; Pontes, T.H.D.; Pagan, L.U.; Murata, G.M.; Damatto, F.C.; Carvalho Depra, I.; Rego, A.B.G.C.; et al. Influence of Isolated Resistance Exercise on Cardiac Remodeling, Myocardial Oxidative Stress, and Metabolism in Infarcted Rats. Antioxidants 2023, 12, 896. https://doi.org/10.3390/antiox12040896
Rodrigues EA, Lima ARR, Gomes MJ, Souza LM, Pontes THD, Pagan LU, Murata GM, Damatto FC, Carvalho Depra I, Rego ABGC, et al. Influence of Isolated Resistance Exercise on Cardiac Remodeling, Myocardial Oxidative Stress, and Metabolism in Infarcted Rats. Antioxidants. 2023; 12(4):896. https://doi.org/10.3390/antiox12040896
Chicago/Turabian StyleRodrigues, Eder Anderson, Aline Regina Ruiz Lima, Mariana Janini Gomes, Lidiane Moreira Souza, Thierres Hernani Dias Pontes, Luana Urbano Pagan, Gilson Masahiro Murata, Felipe Cesar Damatto, Igor Carvalho Depra, Amanda Bergamo Gonçalves Castro Rego, and et al. 2023. "Influence of Isolated Resistance Exercise on Cardiac Remodeling, Myocardial Oxidative Stress, and Metabolism in Infarcted Rats" Antioxidants 12, no. 4: 896. https://doi.org/10.3390/antiox12040896