
Gestational Hypertension and High-Density Lipoprotein Function: An Explorative Study in Overweight/Obese Women of the DALI Cohort

 ,
,  , , , , ,
, , , , ,  and
and
Abstract
:1. Introduction
2. Methods
2.1. Definition of GHTN
2.2. Biochemical Analyses
2.3. ApoB-Depletion of Serum
2.4. Cholesterol Efflux Capacity
2.5. Arylesterase (AE)—Activity of Paraoxonase1
2.6. Anti-Oxidative (AO)—Capacity of ApoB-Depleted Serum
2.7. Serum Levels of Apolipoprotein M (apoM)
2.8. Statistical Analyses
3. Results
3.1. Study Cohort Characteristics
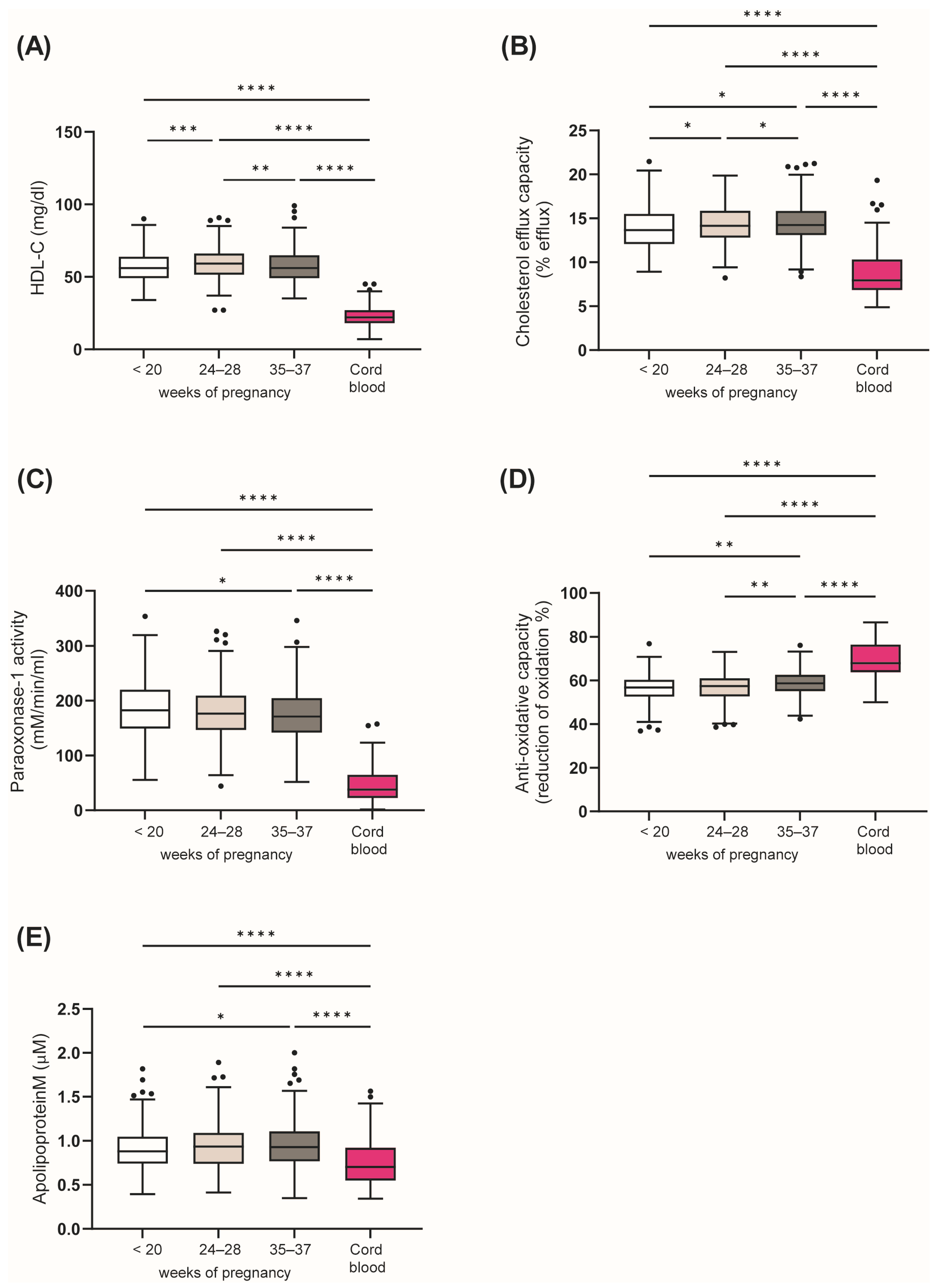
3.2. Changes of HDL-Related Parameters during Pregnancy
3.3. HDL-Related Parameters in Cord Blood
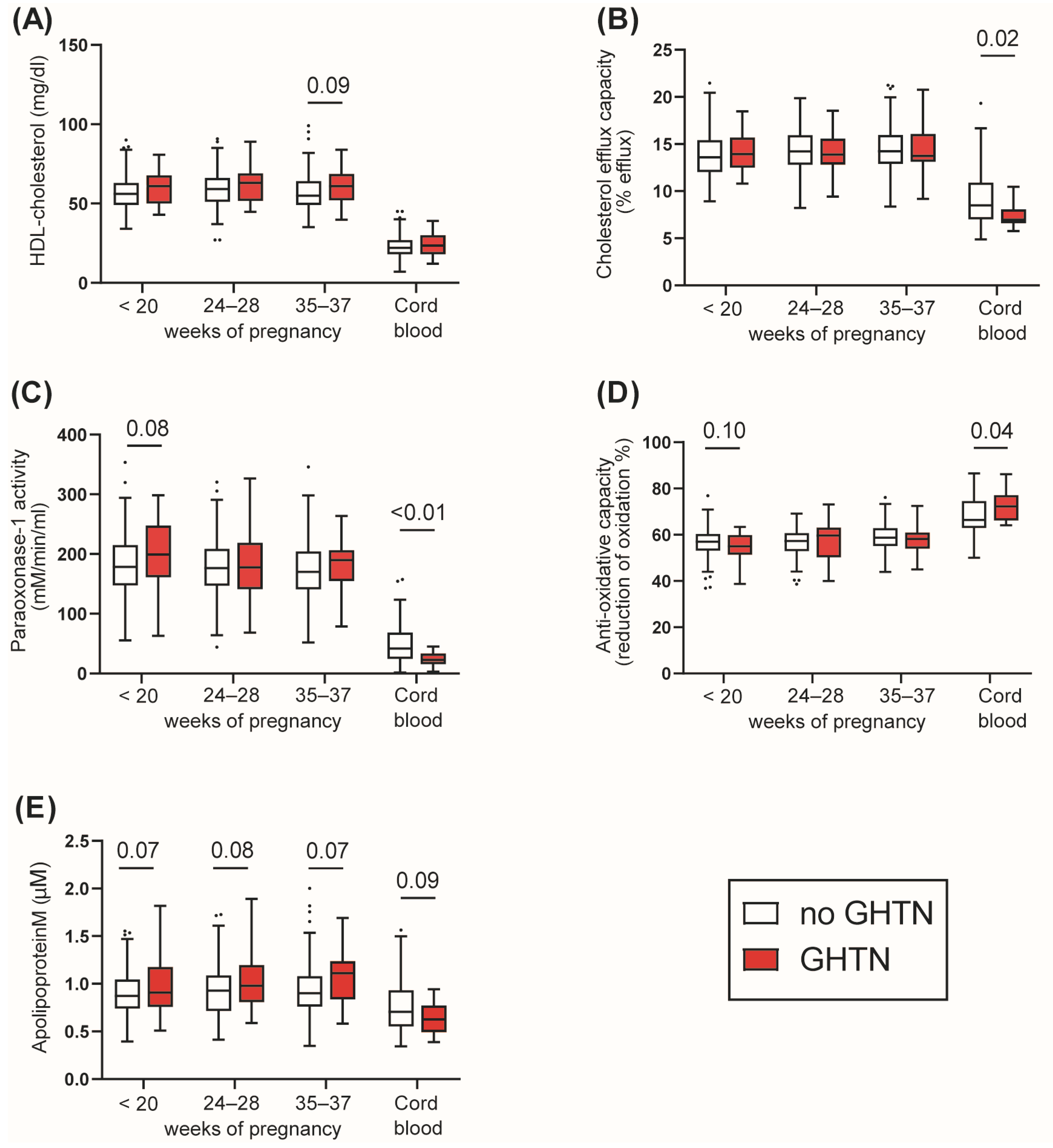
3.4. GHTN-Associated Changes in HDL-Related Parameters in Mothers and Cord Blood
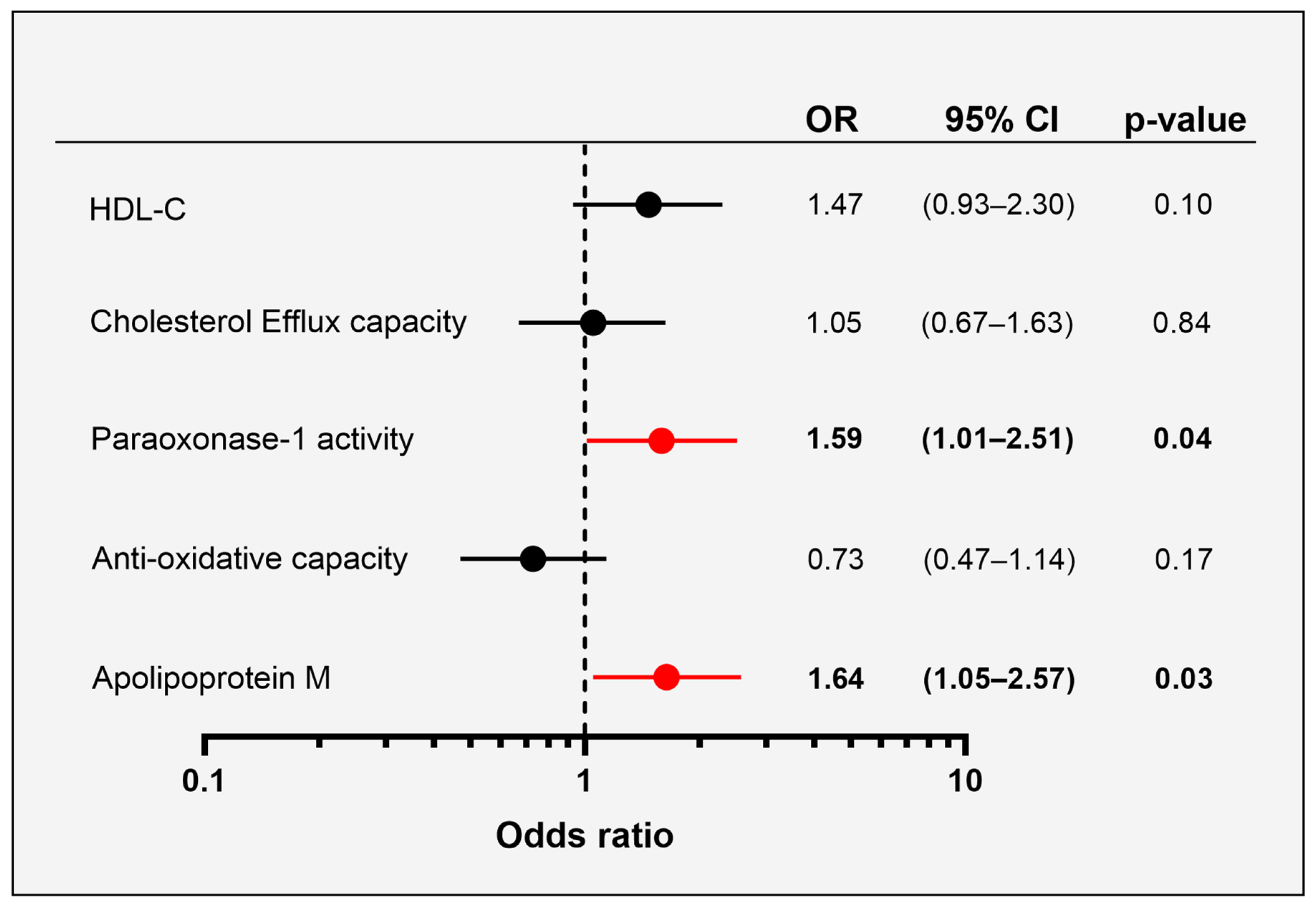
3.5. Association of HDL-Related Parameters with Pregnancy Outcome
3.6. Consequences of Maternal Pregnancy Disorders on HDL-Related Parameters in Cord Blood
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zeng, Z.; Liu, F.; Li, S. Metabolic Adaptations in Pregnancy: A Review. ANM 2017, 70, 59–65. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Recommendations for Prevention and Treatment of Pre-Eclampsia and Eclampsia; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Wildman, K.; Bouvier-Colle, M.-H. MOMS Group Maternal Mortality as an Indicator of Obstetric Care in Europe. BJOG 2004, 111, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Kazemian, E.; Sotoudeh, G.; Dorosty-Motlagh, A.R.; Eshraghian, M.R.; Bagheri, M. Maternal Obesity and Energy Intake as Risk Factors of Pregnancy-Induced Hypertension among Iranian Women. J. Health Popul. Nutr. 2014, 32, 486–493. [Google Scholar] [CrossRef] [PubMed]
- Simmons, D. Epidemiology of Diabetes in Pregnancy. In A Practical Manual of Diabetes in Pregnancy; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2017; pp. 1–16. ISBN 978-1-119-04380-5. [Google Scholar]
- Hollegaard, B.; Lykke, J.A.; Boomsma, J.J. Time from Pre-Eclampsia Diagnosis to Delivery Affects Future Health Prospects of Children. Evol. Med. Public Health 2017, 2017, 53–66. [Google Scholar] [CrossRef] [Green Version]
- Bellamy, L.; Casas, J.-P.; Hingorani, A.D.; Williams, D.J. Pre-Eclampsia and Risk of Cardiovascular Disease and Cancer in Later Life: Systematic Review and Meta-Analysis. BMJ 2007, 335, 974. [Google Scholar] [CrossRef] [Green Version]
- Wu, P.; Haththotuwa, R.; Kwok, C.S.; Babu, A.; Kotronias, R.A.; Rushton, C.; Zaman, A.; Fryer, A.A.; Kadam, U.; Chew-Graham, C.A.; et al. Preeclampsia and Future Cardiovascular Health: A Systematic Review and Meta-Analysis. Circ. Cardiovasc. Qual. Outcomes 2017, 10, e003497. [Google Scholar] [CrossRef]
- Rohatgi, A.; Khera, A.; Berry, J.D.; Givens, E.G.; Ayers, C.R.; Wedin, K.E.; Neeland, I.J.; Yuhanna, I.S.; Rader, D.R.; de Lemos, J.A.; et al. HDL Cholesterol Efflux Capacity and Incident Cardiovascular Events. N. Engl. J. Med. 2014, 371, 2383–2393. [Google Scholar] [CrossRef] [Green Version]
- Trakaki, A.; Marsche, G. Current Understanding of the Immunomodulatory Activities of High-Density Lipoproteins. Biomedicines 2021, 9, 587. [Google Scholar] [CrossRef]
- Barter, P.J.; Nicholls, S.; Rye, K.A.; Anantharamaiah, G.M.; Navab, M.; Fogelman, A.M. Antiinflammatory Properties of HDL. Circ. Res. 2004, 95, 764–772. [Google Scholar] [CrossRef]
- Kontush, A.; Chapman, M.J. Antiatherogenic Function of HDL Particle Subpopulations: Focus on Antioxidative Activities. Curr. Opin. Lipidol. 2010, 21, 312–318. [Google Scholar] [CrossRef]
- Efrat, M.; Aviram, M. Paraoxonase 1 Interactions with HDL, Antioxidants and Macrophages Regulate Atherogenesis—A Protective Role for HDL Phospholipids. Adv. Exp. Med. Biol. 2010, 660, 153–166. [Google Scholar] [CrossRef]
- Del Gaudio, I.; Rubinelli, L.; Sasset, L.; Wadsack, C.; Hla, T.; Di Lorenzo, A. Endothelial Spns2 and ApoM Regulation of Vascular Tone and Hypertension Via Sphingosine-1-Phosphate. J. Am. Heart Assoc. 2021, 10, e021261. [Google Scholar] [CrossRef] [PubMed]
- Christoffersen, C.; Obinata, H.; Kumaraswamy, S.B.; Galvani, S.; Ahnström, J.; Sevvana, M.; Egerer-Sieber, C.; Muller, Y.A.; Hla, T.; Nielsen, L.B.; et al. Endothelium-Protective Sphingosine-1-Phosphate Provided by HDL-Associated Apolipoprotein M. Proc. Natl. Acad. Sci. USA 2011, 108, 9613–9618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Besler, C.; Heinrich, K.; Rohrer, L.; Doerries, C.; Riwanto, M.; Shih, D.M.; Chroni, A.; Yonekawa, K.; Stein, S.; Schaefer, N.; et al. Mechanisms Underlying Adverse Effects of HDL on ENOS-Activating Pathways in Patients with Coronary Artery Disease. J. Clin. Investig. 2011, 121, 2693–2708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, Y.; Kothari, V.; Bornfeldt, K.E. HDL Function in Cardiovascular Disease and Diabetes. Arterioscler. Thromb. Vasc. Biol. 2018, 38, e10–e16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiesa, S.T.; Charakida, M. High-Density Lipoprotein Function and Dysfunction in Health and Disease. Cardiovasc. Drugs 2019, 33, 207–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stadler, J.T.; Marsche, G. Obesity-Related Changes in High-Density Lipoprotein Metabolism and Function. Int. J. Mol. Sci. 2020, 21, 8985. [Google Scholar] [CrossRef] [PubMed]
- Marsche, G.; Heine, G.H.; Stadler, J.T.; Holzer, M. Current Understanding of the Relationship of HDL Composition, Structure and Function to Their Cardioprotective Properties in Chronic Kidney Disease. Biomolecules 2020, 10, 1348. [Google Scholar] [CrossRef]
- Watts, D.H.; Krohn, M.A.; Wener, M.H.; Eschenbach, D.A. C-Reactive Protein in Normal Pregnancy. Obs. Gynecol. 1991, 77, 176–180. [Google Scholar] [CrossRef]
- Melchior, J.T.; Swertfeger, D.K.; Morris, J.; Street, S.E.; Warshak, C.R.; Welge, J.A.; Remaley, A.T.; Catov, J.M.; Davidson, W.S.; Woollett, L.A. Pregnancy Is Accompanied by Larger High Density Lipoprotein Particles and Compositionally Distinct Subspecies. J. Lipid Res. 2021, 62, 100107. [Google Scholar] [CrossRef]
- Litvinov, D.; Mahini, H.; Garelnabi, M. Antioxidant and Anti-Inflammatory Role of Paraoxonase 1: Implication in Arteriosclerosis Diseases. N. Am. J. Med. Sci. 2012, 4, 523–532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao Mattisson, I.; Christoffersen, C. Apolipoprotein M and Its Impact on Endothelial Dysfunction and Inflammation in the Cardiovascular System. Atherosclerosis 2021, 334, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Jelsma, J.G.M.; van Poppel, M.N.M.; Galjaard, S.; Desoye, G.; Corcoy, R.; Devlieger, R.; van Assche, A.; Timmerman, D.; Jans, G.; Harreiter, J.; et al. DALI: Vitamin D and Lifestyle Intervention for Gestational Diabetes Mellitus (GDM) Prevention: An European Multicentre, Randomised Trial—Study Protocol. BMC Pregnancy Childbirth 2013, 13, 142. [Google Scholar] [CrossRef] [Green Version]
- Simmons, D.; Jelsma, J.G.M.; Galjaard, S.; Devlieger, R.; Van Assche, A.; Jans, G.; Corcoy, R.; Adelantado, J.M.; Dunne, F.; Desoye, G.; et al. Results from a European Multicenter Randomized Trial of Physical Activity and/or Healthy Eating to Reduce the Risk of Gestational Diabetes Mellitus: The DALI Lifestyle Pilot. Diabetes Care 2015, 38, 1650–1656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stadler, J.T.; Lackner, S.; Mörkl, S.; Trakaki, A.; Scharnagl, H.; Borenich, A.; Wonisch, W.; Mangge, H.; Zelzer, S.; Meier-Allard, N.; et al. Obesity Affects HDL Metabolism, Composition and Subclass Distribution. Biomedicines 2021, 9, 242. [Google Scholar] [CrossRef] [PubMed]
- Trakaki, A.; Sturm, G.J.; Pregartner, G.; Scharnagl, H.; Eichmann, T.O.; Trieb, M.; Knuplez, E.; Holzer, M.; Stadler, J.T.; Heinemann, A.; et al. Allergic Rhinitis Is Associated with Complex Alterations in High-Density Lipoprotein Composition and Function. Biochim. Biophys. Acta Mol. Cell. Biol. Lipids 2019, 1864, 1280–1292. [Google Scholar] [CrossRef]
- Bosteen, M.H.; Dahlbäck, B.; Nielsen, L.B.; Christoffersen, C. Protein Unfolding Allows Use of Commercial Antibodies in an Apolipoprotein M Sandwich ELISA. J. Lipid Res. 2015, 56, 754–759. [Google Scholar] [CrossRef] [Green Version]
- Elsøe, S.; Ahnström, J.; Christoffersen, C.; Hoofnagle, A.N.; Plomgaard, P.; Heinecke, J.W.; Binder, C.J.; Björkbacka, H.; Dahlbäck, B.; Nielsen, L.B. Apolipoprotein M Binds Oxidized Phospholipids and Increases the Antioxidant Effect of HDL. Atherosclerosis 2012, 221, 91–97. [Google Scholar] [CrossRef]
- Sreckovic, I.; Birner-Gruenberger, R.; Obrist, B.; Stojakovic, T.; Scharnagl, H.; Holzer, M.; Scholler, M.; Philipose, S.; Marsche, G.; Lang, U.; et al. Distinct Composition of Human Fetal HDL Attenuates Its Anti-Oxidative Capacity. Biochim. Biophys. Acta (BBA)-Mol. Cell Biol. Lipids 2013, 1831, 737–746. [Google Scholar] [CrossRef]
- Grimes, S.B.; Wild, R. Effect of Pregnancy on Lipid Metabolism and Lipoprotein Levels. In Endotext; Feingold, K.R., Anawalt, B., Boyce, A., Chrousos, G., de Herder, W.W., Dungan, K., Grossman, A., Hershman, J.M., Hofland, J., Kaltsas, G., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. [Google Scholar]
- Desoye, G.; Schweditsch, M.O.; Pfeiffer, K.P.; Zechner, R.; Kostner, G.M. Correlation of Hormones with Lipid and Lipoprotein Levels during Normal Pregnancy and Postpartum. J. Clin. Endocrinol. Metab. 1987, 64, 704–712. [Google Scholar] [CrossRef]
- Woollett, L.A.; Catov, J.M.; Jones, H.N. Roles of Maternal HDL during Pregnancy. Biochim. Biophys. Acta Mol. Cell. Biol. Lipids 2022, 1867, 159106. [Google Scholar] [CrossRef] [PubMed]
- Einbinder, Y.; Biron-Shental, T.; Agassi-Zaitler, M.; Tzadikevitch-Geffen, K.; Vaya, J.; Khatib, S.; Ohana, M.; Benchetrit, S.; Zitman-Gal, T. High-Density Lipoproteins (HDL) Composition and Function in Preeclampsia. Arch. Gynecol. Obs. 2018, 298, 405–413. [Google Scholar] [CrossRef] [PubMed]
- Mistry, H.D.; Kurlak, L.O.; Mansour, Y.T.; Zurkinden, L.; Mohaupt, M.G.; Escher, G. Increased Maternal and Fetal Cholesterol Efflux Capacity and Placental CYP27A1 Expression in Preeclampsia. J. Lipid Res. 2017, 58, 1186–1195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kockx, M.; Roberts, L.; Wang, J.; Tran, C.; Brown, M.A.; Kritharides, L. Effects of Pre-Eclampsia on HDL-Mediated Cholesterol Efflux Capacity after Pregnancy. Atheroscler. Plus 2022, 48, 12–19. [Google Scholar] [CrossRef]
- Shunmoogam, N.; Naidoo, P.; Chilton, R. Paraoxonase (PON)-1: A Brief Overview on Genetics, Structure, Polymorphisms and Clinical Relevance. Vasc. Health Risk Manag. 2018, 14, 137–143. [Google Scholar] [CrossRef] [Green Version]
- Mackness, M.; Mackness, B. Human Paraoxonase-1 (PON1): Gene Structure and Expression, Promiscuous Activities and Multiple Physiological Roles. Gene 2015, 567, 12–21. [Google Scholar] [CrossRef] [Green Version]
- Elsøe, S.; Christoffersen, C.; Luchoomun, J.; Turner, S.; Nielsen, L.B. Apolipoprotein M Promotes Mobilization of Cellular Cholesterol in Vivo. Biochim. Biophys. Acta (BBA)-Mol. Cell Biol. Lipids 2013, 1831, 1287–1292. [Google Scholar] [CrossRef]
- Wolfrum, C.; Poy, M.N.; Stoffel, M. Apolipoprotein M Is Required for Preβ-HDL Formation and Cholesterol Efflux to HDL and Protects against Atherosclerosis. Nat. Med. 2005, 11, 418–422. [Google Scholar] [CrossRef]
- Liao, J.; Zheng, Y.; Hu, M.; Xu, P.; Lin, L.; Liu, X.; Wu, Y.; Huang, B.; Ye, X.; Li, S.; et al. Impaired Sphingosine-1-Phosphate Synthesis Induces Preeclampsia by Deactivating Trophoblastic YAP (Yes-Associated Protein) Through S1PR2 (Sphingosine-1-Phosphate Receptor-2)-Induced Actin Polymerizations. Hypertension 2022, 79, 399–412. [Google Scholar] [CrossRef]
- Bhattacharyya, T.; Nicholls, S.J.; Topol, E.J.; Zhang, R.; Yang, X.; Schmitt, D.; Fu, X.; Shao, M.; Brennan, D.M.; Ellis, S.G.; et al. Relationship of Paraoxonase 1 (PON1) Gene Polymorphisms and Functional Activity With Systemic Oxidative Stress and Cardiovascular Risk. JAMA 2008, 299, 1265–1276. [Google Scholar] [CrossRef]
- Swertfeger, D.K.; Rebholz, S.; Li, H.; Shah, A.S.; Davidson, W.S.; Lu, L.J. Feasibility of a Plasma Bioassay to Assess Oxidative Protection of Low-Density Lipoproteins by High-Density Lipoproteins. J. Clin. Lipidol. 2018, 12, 1539–1548. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Maternal Characteristics | Total n = 192 | No GHTN n = 161 | GHTN n = 24 | p |
|---|---|---|---|---|
| Age, years | 31.7 ± 5.4 | 31.9 ± 5.3 | 30.4 ± 5.3 | 0.19 |
| Prepregnancy BMI, kg/m2 | 34.1 ± 4.5 | 33.9 ± 4.3 | 36.2 ± 5.8 | 0.07 |
| Gestational weight gain, kg | 8.4 ± 4.8 | 8.3 ± 5.0 | 8.9 ± 4.0 | 0.59 |
| Primiparous | 102 (53%) | 82 (51%) | 16 (67%) | 0.15 |
| Married/living with partner | 181 (94%) | 151 (94%) | 23 (96%) | 0.69 |
| High education | 119 (62%) | 103 (64%) | 14 (58%) | 0.59 |
| European descent | 170 (89%) | 142 (88%) | 22 (92%) | 0.62 |
| Smoking | 18 (9%) | 17 (11%) | 0 (0%) | 0.09 |
| GDM | 55 (29%) | 44 (28%) | 7 (29%) | 0.87 |
| GHTN | 24 (13%) | -- | -- | -- |
| Preeclampsia | 6 (3%) | 5 (3%) | 1 (4%) | 0.78 |
| Neonatal characteristics | ||||
| Gestational age at birth | 39.7 ± 1.4 | 39.7 ± 1.4 | 39.5 ± 1.3 | 0.50 |
| Birthweight | 3575 ± 520 | 3587 ± 527 | 3521 ± 462 | 0.56 |
| Female sex | 90 (47%) | 74 (46%) | 15 (63%) | 0.13 |
| HDL-C B (95% CI) | p | Anti-Oxidative Capacity B (95% CI) | p | Paraoxonase-1 Activity B (95% CI) | p | Cholesterol Efflux Capacity B (95% CI) | p | ApoM B (95% CI) | p | |
|---|---|---|---|---|---|---|---|---|---|---|
| GHTN | 0.04 (−0.06; 0.14) | 0.44 | 5.29 (0.63; 9.95) | 0.03 | −24.88 (−41.87; −7.89) | 0.005 | −2.04 (−3.61; −0.47) | 0.01 | −0.14 (−0.28; 0.003) | 0.055 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stadler, J.T.; van Poppel, M.N.M.; Christoffersen, C.; Hill, D.; Wadsack, C.; Simmons, D.; Desoye, G.; Marsche, G.; DALI Core Investigator Group. Gestational Hypertension and High-Density Lipoprotein Function: An Explorative Study in Overweight/Obese Women of the DALI Cohort. Antioxidants 2023, 12, 68. https://doi.org/10.3390/antiox12010068
Stadler JT, van Poppel MNM, Christoffersen C, Hill D, Wadsack C, Simmons D, Desoye G, Marsche G, DALI Core Investigator Group. Gestational Hypertension and High-Density Lipoprotein Function: An Explorative Study in Overweight/Obese Women of the DALI Cohort. Antioxidants. 2023; 12(1):68. https://doi.org/10.3390/antiox12010068
Chicago/Turabian StyleStadler, Julia T., M. N. M. van Poppel, Christina Christoffersen, David Hill, Christian Wadsack, David Simmons, Gernot Desoye, Gunther Marsche, and DALI Core Investigator Group. 2023. "Gestational Hypertension and High-Density Lipoprotein Function: An Explorative Study in Overweight/Obese Women of the DALI Cohort" Antioxidants 12, no. 1: 68. https://doi.org/10.3390/antiox12010068