
Oxidative Potential in Exhaled Air (OPEA) as a Tool for Predicting Certain Respiratory Disorders in the General Adult Population: Cross-Sectional Analysis Nested in the Swiss Health Study
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Sample
2.3. Data Collection and Management
2.4. Pulmonary Functional Test
2.5. SARS-CoV-2 Serology Test
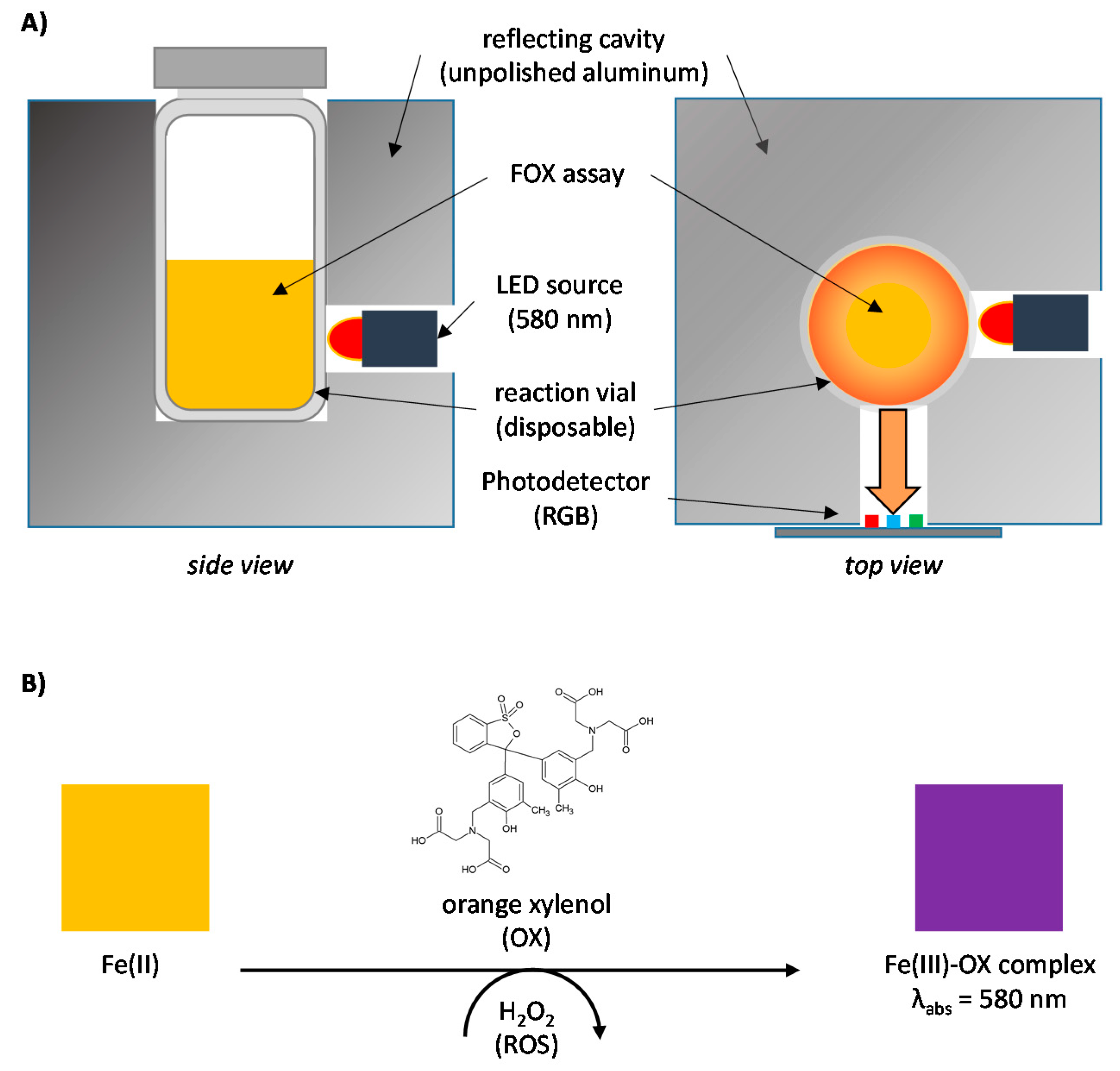
2.6. OPEA Measurement
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Frijhoff, J.; Winyard, P.G.; Zarkovic, N.; Davies, S.S.; Stocker, R.; Cheng, D.; Knight, A.R.; Taylor, E.L.; Oettrich, J.; Ruskovska, T.; et al. Clinical Relevance of Biomarkers of Oxidative Stress. Antioxid. Redox Signal. 2015, 23, 1144–1170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halliwell, B. Free radicals and antioxidants: A personal view. Nutr. Rev. 1994, 52, 253–265. [Google Scholar] [CrossRef] [PubMed]
- Sies, H. Oxidative stress: A concept in redox biology and medicine. Redox. Biol. 2015, 4, 180–183. [Google Scholar] [CrossRef] [Green Version]
- Suarez, G.; Santschi, C.; Plateel, G.; Martin, O.J.F.; Riediker, M. Absorbance enhancement in microplate wells for improved-sensitivity biosensors. Biosens. Bioelectron. 2014, 56, 198–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suarez, G.; Santschi, C.; Slaveykova, V.I.; Martin, O.J.F. Sensing the dynamics of oxidative stress using enhanced absorption in protein-loaded random media. Sci. Rep. 2013, 3, 3447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goekce, S.; Concha-Lozano, N.; Sauvain, J.-J.; Hemmendinger, M.; Portela, A.; Sergent, E.; Andujar, P.; Pairon, J.-C.; Wild, P.; Suárez, G. Multiscattering-enhanced absorbance to enable the sensitive analysis of extremely diluted biological samples: Determination of oxidative potential in exhaled air. Med. Nov. Technol. Devices 2022, 14, 100120. [Google Scholar] [CrossRef]
- Dagher, G.; Becker, K.-F.; Bonin, S.; Foy, C.; Gelmini, S.; Kubista, M.; Kungl, P.; Oelmueller, U.; Parkes, H.; Pinzani, P.; et al. Pre-analytical processes in medical diagnostics: New regulatory requirements and standards. New Biotechnol. 2019, 52, 121–125. [Google Scholar] [CrossRef]
- Ozarda, Y. Reference intervals: Current status, recent developments and future considerations. Biochem. Med. (Zagreb) 2016, 26, 5–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ozarda, Y.; Ichihara, K.; Jones, G.; Streichert, T.; Ahmadian, R. Comparison of reference intervals derived by direct and indirect methods based on compatible datasets obtained in Turkey. Clin. Chim. Acta 2021, 520, 186–195. [Google Scholar] [CrossRef] [PubMed]
- FOPH. Swiss Health Survey: Pilot Phase to Be Continued. Available online: https://www.bag.admin.ch/bag/en/home/das-bag/aktuell/news/news-15-09-2020.html (accessed on 23 August 2022).
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Harris, P.A.; Delacqua, G.; Taylor, R.; Pearson, S.; Fernandez, M.; Duda, S.N. The REDCap Mobile Application: A data collection platform for research in regions or situations with internet scarcity. JAMIA Open 2021, 4, ooab078. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Tan, W.C.; Bourbeau, J.; O’Donnell, D.; Aaron, S.; Maltais, F.; Marciniuk, D.; Hernandez, P.; Cowie, R.; Chapman, K.; Sonia Buist, A.; et al. Quality assurance of spirometry in a population-based study -predictors of good outcome in spirometry testing. J. Chronic Obstr. Pulm. Dis. 2014, 11, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, D.M.; Jurdi, R.; Roberts, C.A.; Hernandez, M.; Horne, R.; Chan, A. A Review of Portable Electronic Spirometers: Implications for Asthma Self-Management. Curr. Allergy Asthma. Rep. 2018, 18, 53. [Google Scholar] [CrossRef] [PubMed]
- Sekerel, B.E.; Unsal, H.; Sahiner, U.M.; Uysal Soyer, O.; Damadoglu, E.; Karakaya, G.; Kalyoncu, A.F. Clinical Validation of the Spirohome Clinic Ultrasonic Spirometer in Child and Adolescent Patients. J. Asthma. Allergy 2022, 15, 219–229. [Google Scholar] [CrossRef] [PubMed]
- Singh, D.; Agusti, A.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Celli, B.R.; Criner, G.J.; Frith, P.; Halpin, D.M.G.; Han, M.; et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease: The GOLD science committee report 2019. Eur. Respir. J. 2019, 53, 1900164. [Google Scholar] [CrossRef]
- Quanjer, P.H.; Stanojevic, S.; Cole, T.J.; Baur, X.; Hall, G.L.; Culver, B.H.; Enright, P.L.; Hankinson, J.L.; Ip, M.S.; Zheng, J.; et al. Multi-ethnic reference values for spirometry for the 3-95-yr age range: The global lung function 2012 equations. Eur. Respir. J. 2012, 40, 1324–1343. [Google Scholar] [CrossRef] [PubMed]
- Lytras. Available online: https://cran.r-project.org/web/packages/rspiro/index.html (accessed on 30 May 2022).
- Blankenberger, J.; Kaufmann, M.; Albanese, E.; Amati, R.; Anker, D.; Camerini, A.-L.; Chocano-Bedoya, P.; Cullati, S.; Cusini, A.; Fehr, J.; et al. Is living in a household with children associated with SARS-CoV-2 seropositivity in adults? Results from the Swiss national seroprevalence study Corona Immunitas. BMC Med. 2022, 20, 233. [Google Scholar] [CrossRef]
- Fenwick, C.; Croxatto, A.; Coste, A.T.; Pojer, F.; André, C.; Pellaton, C.; Farina, A.; Campos, J.; Hacker, D.; Lau, K. Changes in SARS-CoV-2 antibody responses impact the estimates of infections in population-based seroprevalence studies. MedRxiv 2020. [Google Scholar] [CrossRef]
- CLSI; IFCC. Defining, Establishing and Verifying Reference Intervals in the Clinical Laboratory: Approved Guideline; Clinical and Laboratory Standards Institute and International Federation of Clinical Chemistry: Wayne, PA, USA, 2008; pp. 1–76. [Google Scholar]
- Coisnon, C.; Mitchell, M.A.; Rannou, B.; Le Boedec, K. Subjective assessment of frequency distribution histograms and consequences on reference interval accuracy for small sample sizes: A computer-simulated study. Vet. Clin. Pathol. 2021, 50, 427–441. [Google Scholar] [CrossRef] [PubMed]
- Tukey, J.W. Exploratory Data Analysis; Addison-Wesely: Boston, MA, USA, 1977. [Google Scholar]
- Ammer, T.; Schützenmeister, A.; Prokosch, H.U.; Rauh, M.; Rank, C.M.; Zierk, J. refineR: A Novel Algorithm for Reference Interval Estimation from Real-World Data. Sci. Rep. 2021, 11, 16023. [Google Scholar] [CrossRef] [PubMed]
- Guseva Canu, I.; Hemmendinger, M.; Sauvain, J.J.; Suarez, G.; Hopf, N.B.; Pralong, J.A.; Ben Rayana, T.; Besançon, S.; Sakthithasan, K.; Jouannique, V.; et al. Respiratory Disease Occupational Biomonitoring Collaborative Project (ROBoCoP): A longitudinal pilot study and implementation research in the Parisian transport company. J. Occup. Med. Toxicol. 2021, 16, 22. [Google Scholar] [CrossRef] [PubMed]
- Guseva Canu, I.; Plys, E.; Crézé, C.; Fito, C.; Hopf, N.B.; Progiou, A.; Riganti, C.; Sauvain, J.J.; Squillacioti, G.; Suarez, G.; et al. A harmonized protocol for an international multicenter prospective study of nanotechnology workers: The NanoExplore cohort. Nanotoxicology 2022, in press. [Google Scholar]
- Ozarda, Y.; Sikaris, K.; Streichert, T.; Macri, J. Distinguishing reference intervals and clinical decision limits—A review by the IFCC Committee on Reference Intervals and Decision Limits. Crit. Rev. Clin. Lab. Sci. 2018, 55, 420–431. [Google Scholar] [CrossRef] [PubMed]
- Firmann, M.; Mayor, V.; Vidal, P.M.; Bochud, M.; Pécoud, A.; Hayoz, D.; Paccaud, F.; Preisig, M.; Song, K.S.; Yuan, X.; et al. The CoLaus study: A population-based study to investigate the epidemiology and genetic determinants of cardiovascular risk factors and metabolic syndrome. BMC Cardiovasc. Disord 2008, 8, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, B.W.; Ackermann-Liebrich, U.; Leuenberger, P.; Künzli, N.; Stutz, E.Z.; Keller, R.; Zellweger, J.-P.; Wüthrich, B.; Monn, C.; Blaser, K.; et al. SAPALDIA: Methods and participation in the cross-sectional part of the Swiss Study on Air Pollution and Lung Diseases in Adults. Soz. -Und Präventivmedizin 1997, 42, 67–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henny, J.; Nadif, R.; Got, S.L.; Lemonnier, S.; Ozguler, A.; Ruiz, F.; Beaumont, K.; Brault, D.; Sandt, E.; Goldberg, M.; et al. The CONSTANCES Cohort Biobank: An Open Tool for Research in Epidemiology and Prevention of Diseases. Front. Public Health 2020, 8, 605133. [Google Scholar] [CrossRef] [PubMed]
- Alwan, H.; Pruijm, M.; Ponte, B.; Ackermann, D.; Guessous, I.; Ehret, G.; Staessen, J.A.; Asayama, K.; Vuistiner, P.; Younes, S.E.; et al. Epidemiology of Masked and White-Coat Hypertension: The Family-Based SKIPOGH Study. PLoS ONE 2014, 9, e92522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ichihara, K. Statistical considerations for harmonization of the global multicenter study on reference values. Clin. Chim. Acta. 2014, 432, 108–118. [Google Scholar] [CrossRef] [PubMed]
- STATVD. Population Résidante Permanente Étrangère Par Nationalité, Vaud, 2000–2021. Statistique annuelle de la population. 2022. Available online: https://www.vd.ch/themes/etat-droit-finances/statistique/publications/annuaire-statistique/tableaux-de-lannuaire-statistique/ (accessed on 30 August 2022).
- Guseva Canu, I.; Crézé, C.; Hemmendinger, M.; Ben Rayana, T.; Besançon, S.; Jouannique, V.; Debatisse, A.; Wild, P.; Sauvain, J.J.; Suárez, G.; et al. Particle and metal exposure in Parisian subway: Relationship between exposure biomarkers in air, exhaled breath condensate, and urine. Int. J. Hyg. Environ. Health 2021, 237, 113837. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.; Rapold, R.; Brunner, B.; Blozik, E.; Wieser, S. Asthma and COPD in Switzerland: Prevalence and direct medical costs according to health insurance claims data and a large population survey. In Proceedings of the Wennberg International Collaborative Spring Policy Meeting 2018, Zürich, Switzerland, 12–13 April 2018; pp. 12–13. [Google Scholar]



{kind=link}
{kind=link}
| Sociodemographic Characteristics | n | % | Health Characteristics | n | % |
|---|---|---|---|---|---|
| Sex | Self-declared health status | ||||
| Female | 150 | 60.73 | Healthy | 221 | 89.47 |
| Male | 97 | 39.27 | Unhealthy | 26 | 10.53 |
| Age category (years) | SARS-CoV-2 serology | ||||
| 20–29 | 53 | 21.46 | Positive | 51 | 20.65 |
| 30–39 | 48 | 19.43 | Negative | 173 | 70.04 |
| 40–49 | 43 | 17.41 | Unknown | 23 | 9.31 |
| 50–59 | 56 | 22.67 | FEV1 | ||
| 60–71 | 47 | 19.03 | Normal | 217 | 87.85 |
| Diet status | <LLN(GLI) | 21 | 8.5 | ||
| Omnivor | 182 | 73.68 | Unknown | 9 | 3.64 |
| Vegetarian | 33 | 13.36 | FVC | ||
| Vegan | 29 | 11.74 | Normal | 231 | 93.52 |
| Unknown | 3 | 1.21 | <LLN(GLI) | 7 | 2.83 |
| Smoking status | Unknown | 9 | 3.64 | ||
| Non-smoker | 134 | 54.25 | FEV1/FVC | ||
| Smoker | 28 | 11.34 | Normal | 225 | 91.09 |
| Ex-smoker | 85 | 34.41 | <LLN(GLI) | 13 | 5.26 |
| BMI | Unknown | 9 | 3.64 | ||
| ≤25 | 139 | 56.28 | FEF25-75 | ||
| 25–30 | 73 | 29.55 | Normal | 220 | 89.07 |
| ≥30 | 24 | 9.72 | <LLN(GLI) | 18 | 7.29 |
| Unknown | 11 | 4.45 | Unknown | 9 | 3.64 |
| Characteristic | Category | Observed Mean | 95% Conf. | Interval | p-Value |
|---|---|---|---|---|---|
| Sex | Female | −0.0390 | −0.0730 | −0.0051 | 0.51 |
| Male | −0.0399 | −0.0821 | 0.0023 | ||
| Age (y) | 20–29 | −0.0289 | −0.0862 | 0.0284 | 0.93 |
| 30–39 | −0.0514 | −0.1117 | 0.0089 | ||
| 40–49 | −0.0279 | −0.0916 | 0.0358 | ||
| 50–59 | −0.0564 | −0.1122 | −0.0006 | ||
| 60–71 | −0.0290 | −0.0899 | 0.0319 | ||
| Diet | Omnivore | −0.0451 | −0.0759 | −0.0143 | 0.15 |
| Vegetarian | 0.0237 | −0.0487 | 0.0960 | ||
| Vegan | −0.0721 | −0.1493 | 0.0050 | ||
| BMI | ≤25 | −0.0409 | −0.0753 | −0.0065 | 0.24 |
| 25–30 | −0.0482 | −0.0957 | −0.0007 | ||
| ≥30 | 0.0315 | −0.0514 | 0.1143 | ||
| Smoking | Non-smoker | −0.0274 | −0.0633 | 0.0085 | 0.62 |
| Smoker | −0.0587 | −0.1372 | 0.0199 | ||
| Ex-smoker | −0.0518 | −0.0969 | −0.0068 | ||
| Self-declared health | Healthy | −0.0349 | −0.0629 | −0.0070 | 0.83 |
| Unhealthy | −0.0768 | −0.1582 | 0.0046 | ||
| SARS-CoV-2 serology | Negative | −0.0561 | −0.0875 | −0.0247 | 0.03 |
| Positive | 0.0096 | −0.0483 | 0.0674 | ||
| FEV1 | Normal | −0.0372 | −0.0649 | −0.0094 | 0.23 |
| <LLN(GLI) | −0.0027 | −0.0920 | 0.0867 | ||
| FVC | Normal | −0.0331 | −0.0601 | −0.0062 | 0.66 |
| <LLN(GLI) | −0.0666 | −0.2214 | 0.0883 | ||
| FEV1/FVC | Normal | −0.0400 | −0.0671 | −0.0128 | 0.04 |
| <LLN(GLI) | 0.0671 | −0.0458 | 0.1800 | ||
| FEF25–75 | Normal | −0.0374 | −0.0650 | −0.0098 | 0.20 |
| <LLN(GLI) | 0.0064 | −0.0900 | 0.1029 |
| Estimated Statistics | OPEA |
|---|---|
| Mean | −0.0280414 |
| Standard deviation | 0.0120425 |
| Lower level | −0.0516443 |
| 90%-IC | [−0.0734537; −0.0316189] |
| Upper level | −0.0044385 |
| 90%-IC | [−0.0224059; 0.0153129] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guseva Canu, I.; Hemmendinger, M.; Toto, A.; Wild, P.; Veys-Takeuchi, C.; Bochud, M.; Suárez, G. Oxidative Potential in Exhaled Air (OPEA) as a Tool for Predicting Certain Respiratory Disorders in the General Adult Population: Cross-Sectional Analysis Nested in the Swiss Health Study. Antioxidants 2022, 11, 2079. https://doi.org/10.3390/antiox11102079
Guseva Canu I, Hemmendinger M, Toto A, Wild P, Veys-Takeuchi C, Bochud M, Suárez G. Oxidative Potential in Exhaled Air (OPEA) as a Tool for Predicting Certain Respiratory Disorders in the General Adult Population: Cross-Sectional Analysis Nested in the Swiss Health Study. Antioxidants. 2022; 11(10):2079. https://doi.org/10.3390/antiox11102079
Chicago/Turabian StyleGuseva Canu, Irina, Maud Hemmendinger, Antonio Toto, Pascal Wild, Caroline Veys-Takeuchi, Murielle Bochud, and Guillaume Suárez. 2022. "Oxidative Potential in Exhaled Air (OPEA) as a Tool for Predicting Certain Respiratory Disorders in the General Adult Population: Cross-Sectional Analysis Nested in the Swiss Health Study" Antioxidants 11, no. 10: 2079. https://doi.org/10.3390/antiox11102079