
Effect of Melatonin Plus Zinc Supplementation on Fatigue Perception in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: A Randomized, Double-Blind, Placebo-Controlled Trial

 ,
,  , , and
, , and
Abstract
:
1. Introduction
2. Materials and Methods
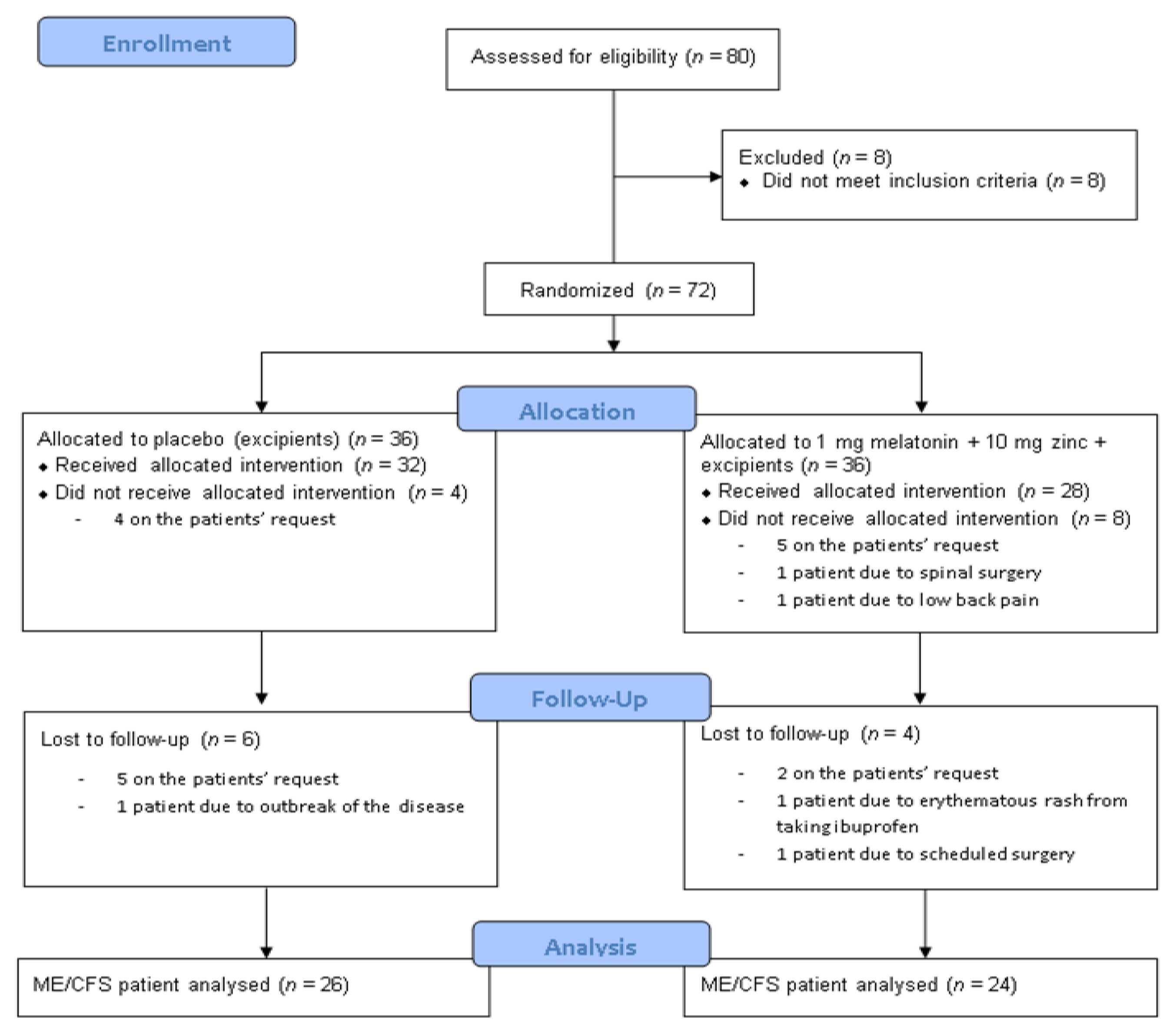
2.1. Study Participants
2.2. Intervention
2.3. Tested Product
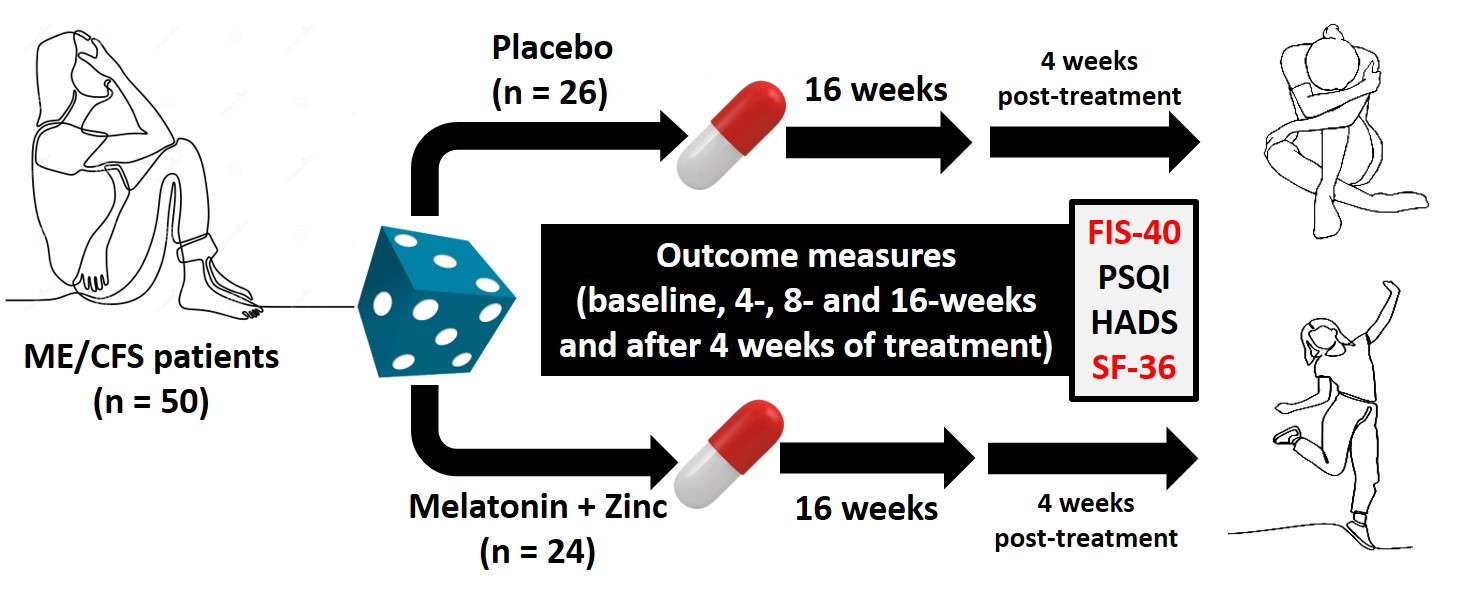
2.4. Study Design
2.5. Primary Outcome Measure
2.6. Secondary Outcome Measures
2.6.1. The Short-Form 36-Item Health Survey
2.6.2. Pittsburgh Sleep Quality Index
2.6.3. Anxiety and Depression
2.7. Measurement of Melatonin and Zinc
2.7.1. Specimen Collection and Processing
2.7.2. Measurements of 6-Sulphatoxymelatonin and Zinc
2.8. Sample Size Estimation
2.9. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics of the Study Population
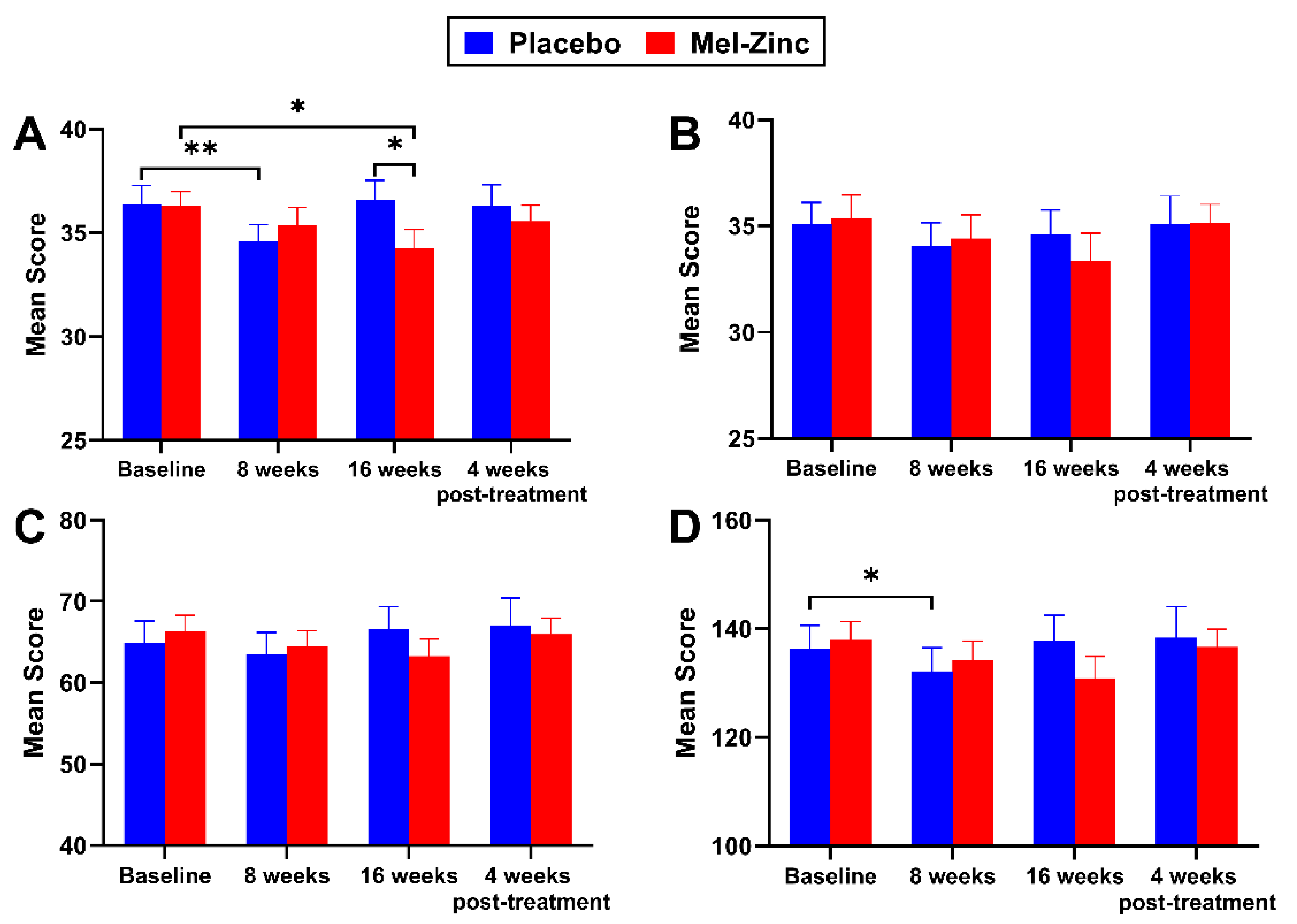
3.2. Primary Outcome Measure
3.3. Secondary Outcome Measures
3.3.1. The Short-Form 36-Item Health Survey
3.3.2. Pittsburgh Sleep Quality Index
3.3.3. Anxiety and Depression
3.3.4. Levels of 6-Sulphatoxymelatonin and Zinc among the Participants
3.3.5. Safety and Tolerability
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nishishinya, B.; Requeijo, C.; Roque, M.; Salas, C.; Urrutia, G. Centro Cochrane Iberoamericano y Agència de Qualitat i Avaluació Sanitàries de Catalunya. In Evaluación y Abordaje de Síndrome de Fatiga Crónica. Actualización de Las Evidencias Científicas; Agència de Qualitat i Avaluació Sanitàries de Catalunya. Departament de Salut. Generalitat de Catalunya: Barcelona, Spain, 2017. [Google Scholar]
- Castro-Marrero, J.; Zaragozá, M.C.; González-Garcia, S.; Aliste, L.; Sáez-Francàs, N.; Romero, O.; Ferré, A.; Fernandez de Sevilla, T.; Alegre, J. Poor self-reported sleep quality and health-related quality of life in patients with chronic fatigue syndrome/myalgic encephalomyelitis. J. Sleep Res. 2018, 27, e12703. [Google Scholar] [CrossRef]
- Fisk, J.D.; Ritvo, P.G.; Ross, L.; Haase, D.A.; Marrie, T.J.; Schlech, W.F. Measuring the functional impact of fatigue: Initial validation of the fatigue impact scale. Clin. Infect. Dis. 1994, 18, S79–S83. [Google Scholar] [CrossRef]
- Alonso, J.; Prieto, L.; Antó, J.M. La versión española del SF-36 Health Survey (Cuestionario de Salud SF-36): Un instrumento para la medida de los resultados clínicos. Med. Clin. 1995, 104, 771–776. [Google Scholar]
- Herrero, M.J.; Blanch, J.; Peri, J.M.; De Pablo, J.; Pintor, L.; Bulbena, A. A validation study of the hospital anxiety and depression scale (HADS) in a Spanish population. Gen. Hosp. Psychiatr. 2003, 25, 277–283. [Google Scholar] [CrossRef]
- Castro-Marrero, J.; Sáez-Francàs, N.; Santillo, D.; Alegre, J. Treatment and management of chronic fatigue syndrome/myalgic encephalomyelitis: All roads lead to Rome. Br. J. Pharmacol. 2017, 174, 345–369. [Google Scholar] [CrossRef] [Green Version]
- Maes, M.; Twisk, F.N. Why myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) may kill you: Disorders in the inflammatory and oxidative and nitrosative stress (IO&NS) pathways may explain cardiovascular disorders in ME/CFS. Neuroendocrinol. Lett. 2009, 30, 677–693. [Google Scholar]
- Werbach, M.R. Nutritional Strategies for Treating Chronic Fatigue Syndrome. Altern Med. Rev. 2000, 52, 93–108. [Google Scholar]
- Alraek, T.; Lee, M.S.; Choi, T.Y.; Cao, H.; Liu, J. Complementary and alternative medicine for patients with CFS: A systematic review. BMC Complement. Altern. Med. 2011, 11, 87. [Google Scholar] [CrossRef] [Green Version]
- Castro-Marrero, J.; Zaragozá, M.C.; Domingo, J.C.; Martinez-Martinez, A.; Alegre, J.; von Schacky, C. Low omega-3 index and polyunsaturated fatty acid status in patients with chronic fatigue syndrome/myalgic encephalomyelitis Prostaglandins Leukot. Essent. Fatty Acids 2018, 139, 20–24. [Google Scholar] [CrossRef]
- Sánchez, A.; Calpena, A.C.; Clares, B. Evaluating the oxidative stress in inflammation: Role of melatonin. Int. J. Mol. Sci. 2015, 16, 16981–17004. [Google Scholar] [CrossRef] [Green Version]
- Cambras, T.; Castro-Marrero, J.; Zaragozá, M.C.; Díez-Noguera, A.; Alegre, J. Circadian rhythm abnormalities and autonomic dysfunction in patients with chronic fatigue syndrome/myalgic encephalomyelitis. PLoS ONE 2018, 13, e0198106. [Google Scholar] [CrossRef]
- Bonaventura, P.; Benedetti, G.; Albarède, F.; Miossec, P. Zinc and its role in immunity and inflammation. Autoimmun. Rev. 2015, 14, 277–285. [Google Scholar] [CrossRef]
- Prasad, A.S. Zinc is an antioxidant and anti-inflammatory agent: Its role in human health. Front. Nutr. 2014, 1, 14. [Google Scholar] [CrossRef] [Green Version]
- Nowak, G.; Szewczyk, B.; Pilc, A. Zinc and depression. An update. Pharmac. Rep. 2005, 57, 713–719. [Google Scholar]
- Maksoud, R.; Balinas, C.; Holden, S.; Cabanas, H.; Staines, D.; Marshall-Gradisnik, S. A systematic review of nutraceutical interventions for mitochondrial dysfunctions in myalgic encephalomyelitis/chronic fatigue syndrome. J. Transl. Med. 2021, 19, 81. [Google Scholar] [CrossRef]
- Bjørklund, G.; Dadar, M.; Pen, J.J.; Chirumbolo, S.; Aaseth, J. Chronic fatigue syndrome: Suggestions for a nutritional treatment in the therapeutic approach. Biomed. Pharmacother. 2019, 109, 1000–1007. [Google Scholar] [CrossRef]
- Fukuda, K.; Strauss, S.E.; Hickie, I.; Sharpe, M.C.; Dobbins, J.G.; Komaroff, A. The chronic fatigue syndrome: A comprehensive approach to its definition and study. Ann. Intern. Med. 1994, 121, 953–959. [Google Scholar] [CrossRef]
- Milton, J.S. Estadística para Biología y Ciencias de la Salud, 2nd ed.; Interamericana-McGraw-Hill: Madrid, Spain, 1994; p. 466. [Google Scholar]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kuepfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Marrugat, J.; Vila, J.; Pavesi, M.; Sanz, F. Estimación del tamaño de la muestra en la investigación clínica y epidemiológica. Med. Clin. 1998, 111, 267–276. [Google Scholar]
- Foley, H.M.; Steel, A.E. Adverse events associated with oral administration of melatonin: A critical systematic review of clinical evidence. Complement. Ther. Med. 2019, 42, 65–81. [Google Scholar] [CrossRef]
- Cummings, J.E.; Kovacic, J.P. The ubiquitous role of zinc in health and disease. J. Vet. Emerg. Crit. Care 2009, 19, 215–240. [Google Scholar] [CrossRef]
- Swardfager, W.; Herrmann, N.; Mazereeuw, G.; Goldberger, K.; Harimoto, T.; Lanctôt, K.L. Zinc in depression: A meta-analysis. Biol. Psychiatry 2013, 74, 872–878. [Google Scholar] [CrossRef] [PubMed]
- Maes, M.; Mihaylova, I.; De Ruyter, M. Lower serum zinc in chronic fatigue syndrome: Relationships to immune dysfunction and relevance for the oxidative stress status in CFS. J. Affect. Disord. 2006, 90, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Acuna-Castroviejo, D.; Escames, G.; Reiter, R.J. Melatonin therapy in fibromyalgia. J. Pineal Res. 2006, 40, 98–99. [Google Scholar] [CrossRef]
- La Rubia, M.; Rus, A.; Molina, F.; del Moral, M.L. Is fibromyalgia-related oxidative stress implicated in the decline of physical and mental health status. Clin. Exp. Rheumatol. 2013, 31, S121–S127. [Google Scholar] [PubMed]
- Korszun, A.; Sackett-Lundeen, L.; Papadopoulus, E.; Brucksch, C.; Masterson, L.; Engelberg, N.C.; Haus, E.; Demitrack, M.A.; Crofford, L. Melatonin levels in women with fibromyalgia and chronic fatigue syndrome. J. Rheumatol. 1999, 26, 2675–2680. [Google Scholar]
- Castro-Marrero, J.; Sáez-Francàs, N.; Segundo, M.J.; Calvo, N.; Faro, M.; Aliste, L.; Fernández de Sevilla, T.; Alegre, J. Effect of coenzyme Q10 plus nicotinamide adenine dinucleotide supplementation on maximum heart rate after exercise testing in chronic fatigue syndrome: A randomized, controlled, double-blind trial. Clin. Nutr. 2016, 35, 826–834. [Google Scholar] [CrossRef] [Green Version]
- van Heukelom, R.O.; Prins, J.B.; Smits, M.G.; Bleijenberg, G. Influence of melatonin on fatigue severity in patients with chronic fatigue syndrome and late melatonin secretion. Eur. J. Neurol. 2006, 13, 55–60. [Google Scholar] [CrossRef]
- Pardini, M.; Cordano, C.; Benassi, F.; Mattei, C.; Sassos, D.; Guida, S.; Serrati, C.; Primavera, A.; Amore, M.; Cocito, L.; et al. Agomelatine but not melatonin improves fatigue perception: A longitudinal proof-of-concept study. Eur. Neuropsychopharmacol. 2014, 24, 939–944. [Google Scholar] [CrossRef]
- Starreveld, D.E.J.; Daniels, L.A.; Valdimarsdottir, H.B.; Redd, W.H.; de Geus, J.L.; Ancoli-Israel, S.; Lutgendorf, S.; Korse, C.M.; Kieffer, J.M.; van Leeuwen, F.E.; et al. Light therapy as a treatment of cancer-related fatigue in (non-) Hodgkin lymphoma survivors (SPARKLE trial): Study protocol of a multicenter randomized controlled trial. BMC Cancer 2018, 18, 880. [Google Scholar] [CrossRef]
- Steur, L.M.H.; Kaspers, G.J.L.; Van Someren, E.J.W.; Van Eijkelenburg, N.K.A.; Van der Sluis, I.M.; Dors, N.; Van den Bos, C.; Tissing, W.J.E.; Grootenhuis, M.A.; Van Litsenburg, R.R.L. Sleep-wake rhythm disruption is associated with cancer-related fatigue in paediatric acute lymphoblastic leukaemia. Sleep 2020, 43, zsz320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hemati, K.; Kadijani, A.A.; Sayehmiri, F.; Mehrzadi, S.; Zabihiyeganeh, M.; Hosseinzadeh, A.; Mirzaei, A. Melatonin in the treatment of fibromyalgia symptoms: A systematic review. Complement. Ther. Clin. Pract. 2020, 38, 101072. [Google Scholar] [CrossRef]
- Adamczyk-Sowa, M.; Sowa, P.; Adamczyk, J.; Niedziela, N.; Misiolek, H.; Owczarek, M.; Zwirska-Korczala, K. Effect of melatonin supplementation on plasma lipid hydroperoxides, homocysteine concentrations and chronic fatigue syndrome in multiple sclerosis patients treated with interferons-beta and mitoxantrone. J. Physiol. Pharmacol. 2016, 67, 235–242. [Google Scholar]
- Adamczyk-Sowa, M.; Pierzchala, K.; Sowa, P.; Polaniak, R.; Kukla, M.; Hartel, M. Influence of melatonin supplementation on serum antioxidative properties and impact of the quality of life in multiple sclerosis patients. J. Physiol. Pharmacol. 2014, 65, 543–550. [Google Scholar]
- de Figueiredo Ribeiro, S.M.; Moreno Braga, C.B.; Maris Peria, F.; Zangiacomi Martinez, E.; Ribeiro da Rocha, J.J.; Carvalho Cunha, S.F. Effects of zinc supplementation on fatigue and quality of life in patients with colorectal cancer. Einstein 2017, 15, 24–28. [Google Scholar] [CrossRef] [Green Version]
- Rondanelli, M.; Opizzi, A.; Monteferrario, F.; Antoniello, N.; Manni, R.; Klersy, C. The effect of melatonin, magnesium and zinc on primary insomnia in long-term care facility residents in Italy: A double-blind, placebo-controlled clinical trial. J. Am. Geriatr. Soc. 2011, 59, 82–90. [Google Scholar] [CrossRef]
- Celer, M.; Mogulkoc, R.; Baltaci, A.K.; Dervis Dasdelen, D. The effects of zinc and melatonin on muscle ischaemia-reperfusion injury in rat. Cell. Mol. Biol. 2018, 64, 1–4. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Placebo (n = 26) | Mel-Zinc (n = 24) | p-Value |
|---|---|---|---|
| Age (years) | 53.7 ± 9.6 | 51.0 ± 10.2 | 0.339 |
| Marital status | 0.473 | ||
| Married | 15 (58) | 16 (70) | |
| Single | 7 (27) | 6 (26) | |
| Separated/divorced | 4 (15) | 1 (4) | |
| BMI (kg/m2) | 28 ± 0.1 | 26 ± 0.3 | 0.651 |
| Systolic BP (mmHg) | 118 ± 17.1 | 114 ± 13.7 | 0.291 |
| Diastolic BP (mmHg) | 78 ± 11.9 | 72 ± 9.1 | 0.088 |
| Heart rate (bpm) | 75 ± 8 | 76 ± 12 | 0.680 |
| Illness duration (years) | 0.201 | ||
| >10 | 17 (65) | 19 (79) | |
| ≤10 | 6 (23) | 4 (17) | |
| History of chronic pain | 25 (96) | 24 (100) | 0.319 |
| Illness-affected relatives | 11 (42) | 5 (21) | 0.135 |
| Concomitant drugs | |||
| Anticonvulsants | 13 (50) | 18 (75) | 0.217 |
| Antidepressants | 19 (73) | 24 (85) | 0.065 |
| Anxiolytics | 5 (19) | 6 (25) | 0.302 |
| NSAID | 12 (46) | 11 (46) | 0.720 |
| Opioids | 9 (34) | 12 (50) | 0.547 |
| SF-36 Domains | Placebo (n = 26) | Mel-Zinc (n = 24) | p-Value 1 |
|---|---|---|---|
| Physical functioning | |||
| Baseline | 23.96 ± 3.84 | 22.92 ± 3.43 | 0.893 |
| 8 weeks | 26.04 ± 4.15 | 21.04 ± 3.24 | 0.534 |
| 16 weeks | 21.75 ± 3.84 | 26.09 ± 3.46 | 0.316 |
| 4 weeks post-treatment | 26.14 ± 4.21 | 19.77 ± 3.29 * | 0.421 |
| Physical role functioning | |||
| Baseline | 0.00 ± 0.00 | 1.04 ± 1.02 | 0.298 |
| 8 weeks | 6.00 ± 2.99 | 1.09 ± 1.04 | 0.179 |
| 16 weeks | 3.41 ± 3.20 | 8.70 ± 5.14 | 0.323 |
| 4 weeks post-treatment | 2.08 ± 1.41 | 4.35 ± 3.25 | 0.930 |
| Bodily pain | |||
| Baseline | 14.35 ± 3.36 | 13.50 ± 2.75 | 0.848 |
| 8 weeks | 20.08 ± 3.72 * | 16.79 ± 2.52 | 0.797 |
| 16 weeks | 17.35 ± 3.14 | 17.22 ± 3.41 | 0.847 |
| 4 weeks post-treatment | 15.17 ± 3.33 | 13.78 ± 2.26 | 0.886 |
| General health perception | |||
| Baseline | 14.50 ± 2.64 | 22.91 ± 2.23 | 0.015 |
| 8 weeks | 21.23 ± 4.12 * | 24.04 ± 2.98 | 0.197 |
| 16 weeks | 15.55 ± 3.33 | 25.77 ± 3.29 | 0.017 |
| 4 weeks post-treatment | 19.18 ± 3.29 | 22.05 ± 2.89 | 0.308 |
| Vitality | |||
| Baseline | 18.59 ± 4.57 | 12.99 ± 2.83 | 0.678 |
| 8 weeks | 23.40 ± 5.00 | 15.83 ± 3.81 | 0.370 |
| 16 weeks | 16.01 ± 4.19 | 19.28 ± 4.65 | 0.482 |
| 4 weeks post-treatment | 20.00 ± 4.79 | 18.64 ± 4.47 | 0.935 |
| Social role functioning | |||
| Baseline | 32.69 ± 6.00 | 28.65 ± 3.57 | 0.835 |
| 8 weeks | 41.35 ± 5.33 * | 29.69 ± 3.89 | 0.154 |
| 16 weeks | 31.52 ± 4.99 | 34.24 ± 4.14 | 0.488 |
| 4 weeks post-treatment | 35.94 ± 6.48 | 32.07 ± 4.87 | 0.838 |
| Emotional role functioning | |||
| Baseline | 46.15 ± 9.06 | 42.03 ± 8.81 | 0.790 |
| 8 weeks | 41.03 ± 9.67 | 25.76 ± 7.68 * | 0.403 |
| 16 weeks | 46.97 ± 10.01 | 36.23 ± 8.74 | 0.507 |
| 4 weeks post-treatment | 43.06 ± 9.92 | 28.99 ± 8.60 | 0.304 |
| Mental health status | |||
| Baseline | 48.00 ± 4.26 | 47.63 ± 3.27 | 0.815 |
| 8 weeks | 50.15 ± 4.93 | 45.13 ± 3.44 | 0.553 |
| 16 weeks | 47.43 ± 4.14 | 50.43 ± 3.82 | 0.447 |
| 4 weeks post-treatment | 47.91 ± 4.63 | 40.91 ± 3.78 ** | 0.368 |
| Physical component summary | |||
| Baseline | 20.77 ± 1.14 | 22.53 ± 1.00 | 0.210 |
| 8 weeks | 24.48 ± 1.30 ** | 24.25 ± 1.16 * | 0.856 |
| 16 weeks | 21.29 ± 1.58 | 25.12 ± 1.20 * | 0.070 |
| 4 weeks post-treatment | 22.85 ± 1.21 | 24.38 ± 1.21 | 0.335 |
| Mental component summary | |||
| Baseline | 38.76 ± 2.66 | 35.94 ± 2.10 | 0.455 |
| 8 weeks | 38.14 ± 2.85 | 33.61 ± 2.04 | 0.329 |
| 16 weeks | 37.33 ± 2.83 | 35.95 ± 2.40 | 0.778 |
| 4 weeks post-treatment | 38.52 ± 2.95 | 32.55 ± 2.55 | 0.201 |
| PSQI Domains | Placebo (n = 26) | Mel-Zinc (n = 24) | p-Value 1 |
|---|---|---|---|
| Subjective sleep quality | |||
| Baseline | 2.46 ± 0.12 | 2.50 ± 0.13 | 0.692 |
| 8 weeks | 1.92 ± 0.17 ** | 1.96 ± 0.20 | 0.791 |
| 16 weeks | 1.96 ± 0.24 * | 1.83 ± 0.20 * | 0.540 |
| 4 weeks post-treatment | 2.21 ± 0.16 | 1.91 ± 0.21 | 0.412 |
| Sleep latency | |||
| Baseline | 2.46 ± 0.14 | 2.08 ± 0.17 | 0.096 |
| 8 weeks | 1.88 ± 0.19 ** | 1.75 ± 0.18 | 0.589 |
| 16 weeks | 2.00 ± 0.20 ** | 1.58 ± 0.19 ** | 0.128 |
| 4 weeks post-treatment | 2.29 ± 0.18 | 1.83 ± 0.20 * | 0.080 |
| Sleep duration | |||
| Baseline | 1.92 ± 0.21 | 1.63 ± 0.24 | 0.366 |
| 8 weeks | 1.54 ± 0.24 * | 1.46 ± 0.23 | 0.817 |
| 16 weeks | 1.70 ± 0.21 | 1.25 ± 0.25 | 0.172 |
| 4 weeks post-treatment | 1.83 ± 0.23 | 1.91 ± 0.22 ** | 0.791 |
| Habitual sleep efficiency | |||
| Baseline | 2.31 ± 0.19 | 1.83 ± 0.24 | 0.169 |
| 8 weeks | 1.50 ± 0.25 *** | 1.75 ± 0.25 | 0.466 |
| 16 weeks | 1.91 ± 0.27 | 1.58 ± 0.28 | 0.524 |
| 4 weeks post-treatment | 2.17 ± 0.21 | 2.04 ± 0.23 | 0.768 |
| Sleep disturbances | |||
| Baseline | 2.31 ± 0.14 | 2.04 ± 0.11 | 0.110 |
| 8 weeks | 1.92 ± 0.15 ** | 2.00 ± 0.10 | 0.642 |
| 16 weeks | 2.09 ± 0.16 | 1.88 ± 0.12 | 0.312 |
| 4 weeks post-treatment | 2.13 ± 0.17 | 2.22 ± 0.10 ** | 0.825 |
| Sleeping medication use | |||
| Baseline | 2.00 ± 0.26 | 1.83 ± 0.28 | 0.664 |
| 8 weeks | 2.19 ± 0.26 | 1.58 ± 0.28 | 0.118 |
| 16 weeks | 1.70 ± 0.28 | 1.38 ± 0.29 | 0.487 |
| 4 weeks post-treatment | 2.25 ± 0.24 | 2.04 ± 0.27 ** | 0.722 |
| Daytime dysfunction | |||
| Baseline | 2.38 ± 0.17 | 2.58 ± 0.14 | 0.404 |
| 8 weeks | 2.00 ± 0.17 ** | 2.32 ± 0.15 | 0.158 |
| 16 weeks | 2.13 ± 0.22 | 2.21 ± 0.19 | 0.991 |
| 4 weeks post-treatment | 2.33 ± 0.15 | 2.48 ± 0.15 | 0.476 |
| Global PSQI score | |||
| Baseline | 15.85 ± 0.64 | 14.50 ± 0.63 | 0.101 |
| 8 weeks | 12.96 ± 0.90 ** | 12.83 ± 0.74 * | 0.755 |
| 16 weeks | 13.48 ± 1.07 ** | 11.71 ± 0.94 ** | 0.178 |
| 4 weeks post-treatment | 15.04 ± 0.94 * | 14.43 ± 0.84 ** | 0.448 |
| HADS Domains | Placebo (n = 26) | Mel-Zinc (n = 24) | p-Value 1 |
|---|---|---|---|
| Anxiety | |||
| Baseline | 13.12 ± 0.95 | 11.92 ± 0.77 | 0.163 |
| 8 weeks | 11.08 ± 0.90 ** | 12.46 ± 0.78 | 0.275 |
| 16 weeks | 13.00 ± 1.06 | 11.67 ± 0.80 | 0.124 |
| 4 weeks post-treatment | 12.50 ± 1.06 * | 12.48 ± 0.73 | 0.543 |
| Depression | |||
| Baseline | 11.62 ± 1.04 | 11.71 ± 0.67 | 0.718 |
| 8 weeks | 10.77 ± 1.01 | 11.58 ± 0.86 | 0.907 |
| 16 weeks | 11.87 ± 1.03 | 11.08 ± 0.81 | 0.353 |
| 4 weeks post-treatment | 11.54 ± 0.96 | 11.74 ± 0.81 | 0.535 |
| Total HADS | |||
| Baseline | 25.92 ± 1.38 | 21.92 ± 1.67 | 0.062 |
| 8 weeks | 21.85 ± 1.81 * | 24.04 ± 1.44 | 0.613 |
| 16 weeks | 24.87 ± 1.99 | 22.75 ± 1.41 | 0.201 |
| 4 weeks post-treatment | 24.04 ± 1.94 | 24.22 ± 1.34 | 0.400 |
| Melatonin (as aMT6s), ng/mL urine | Placebo (n = 26) | Mel-Zinc (n = 24) | p-Value 1 |
|---|---|---|---|
| Baseline | 16.55 ± 2.39 | 24.91 ± 3.43 | 0.063 |
| 8 weeks | 16.68 ± 2.44 | 283.50 ± 8.47 *** | <0.0001 |
| 16 weeks | 14.85 ± 2.14 | 284.20 ± 8.45 *** | <0.0001 |
| 4 weeks after treatment | 13.21 ± 2.18 | 26.45 ± 5.61 *** | 0.078 |
| Zinc, µg/dL | Placebo (n = 26) | Mel-Zinc (n = 24) | p-Value 1 |
| Baseline | 114.73 ± 3.94 | 122.04 ± 6.34 | 0.676 |
| 8 weeks | 114.42 ± 4.26 | 120.96 ± 4.92 | 0.336 |
| 16 weeks | 126.62 ± 4.74 | 129.21 ± 6.28 | 0.641 |
| 4 weeks after treatment | 121.45 ± 3.18 | 127.87 ± 5.18 | 0.735 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castro-Marrero, J.; Zaragozá, M.-C.; López-Vílchez, I.; Galmés, J.L.; Cordobilla, B.; Maurel, S.; Domingo, J.C.; Alegre-Martín, J. Effect of Melatonin Plus Zinc Supplementation on Fatigue Perception in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: A Randomized, Double-Blind, Placebo-Controlled Trial. Antioxidants 2021, 10, 1010. https://doi.org/10.3390/antiox10071010
Castro-Marrero J, Zaragozá M-C, López-Vílchez I, Galmés JL, Cordobilla B, Maurel S, Domingo JC, Alegre-Martín J. Effect of Melatonin Plus Zinc Supplementation on Fatigue Perception in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: A Randomized, Double-Blind, Placebo-Controlled Trial. Antioxidants. 2021; 10(7):1010. https://doi.org/10.3390/antiox10071010
Chicago/Turabian StyleCastro-Marrero, Jesús, Maria-Cleofé Zaragozá, Irene López-Vílchez, José Luis Galmés, Begoña Cordobilla, Sara Maurel, Joan Carles Domingo, and José Alegre-Martín. 2021. "Effect of Melatonin Plus Zinc Supplementation on Fatigue Perception in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: A Randomized, Double-Blind, Placebo-Controlled Trial" Antioxidants 10, no. 7: 1010. https://doi.org/10.3390/antiox10071010