
Plasmatic Oxidative and Metabonomic Profile of Patients with Different Degrees of Biliary Acute Pancreatitis Severity

 , ,
, ,  , , ,
, , ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
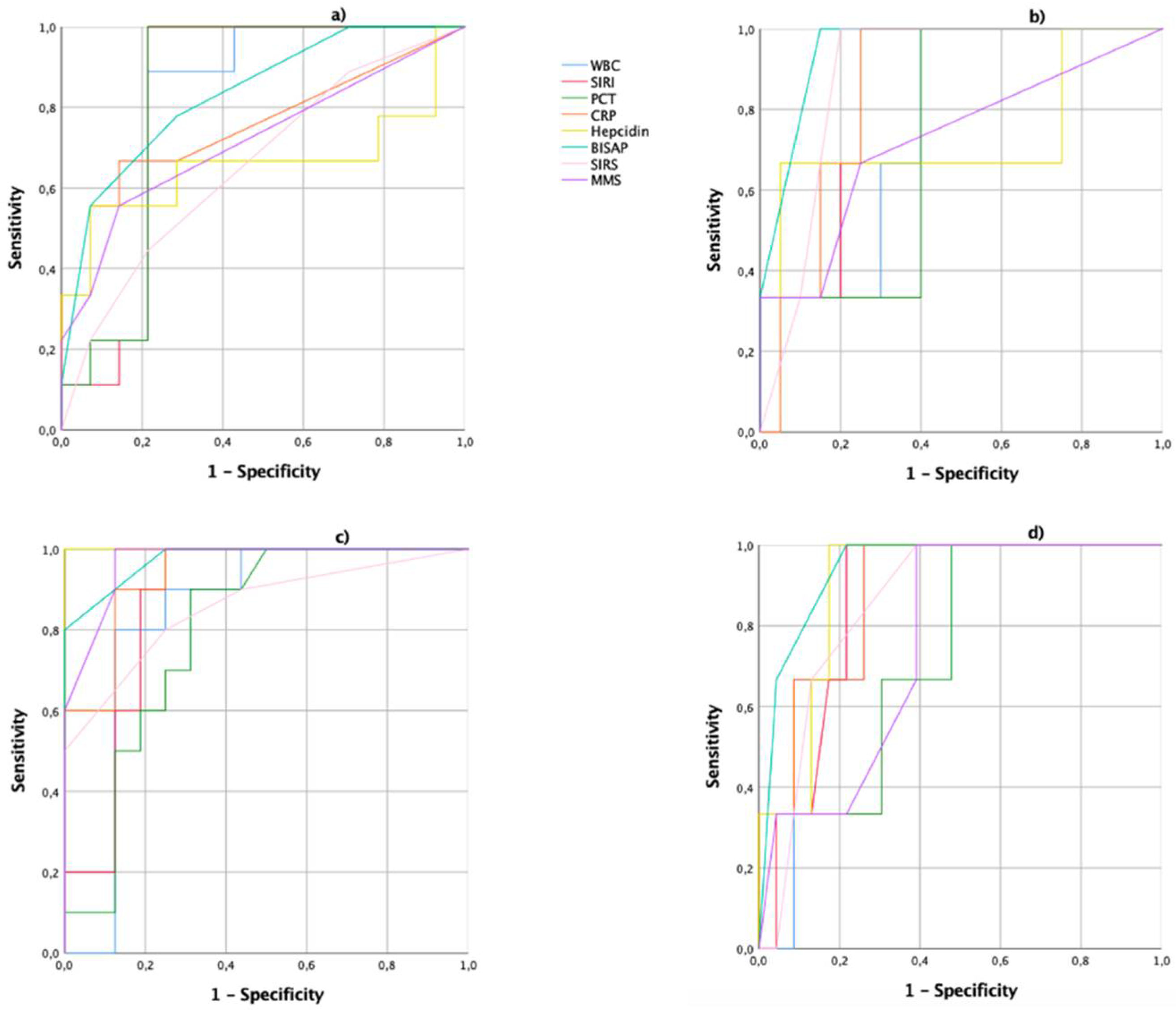
2.3. Analysis of Biomarkers and Scores Systems
2.4. Oxidative Stress Evaluation
2.5. Proton NMR (1H-NMR) Spectroscopy
2.6. Statistical Analysis
3. Results
3.1. Clinical Data
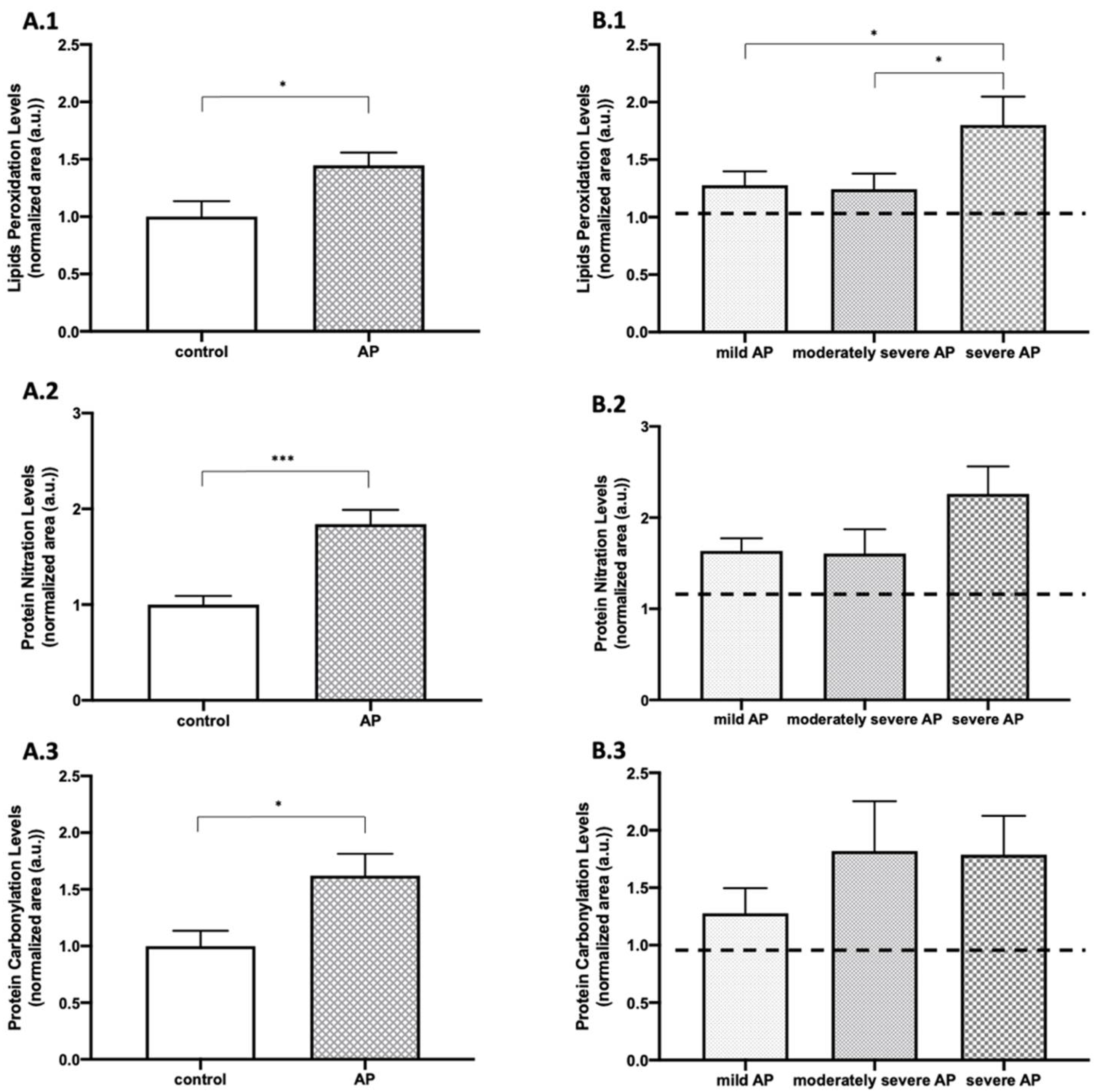
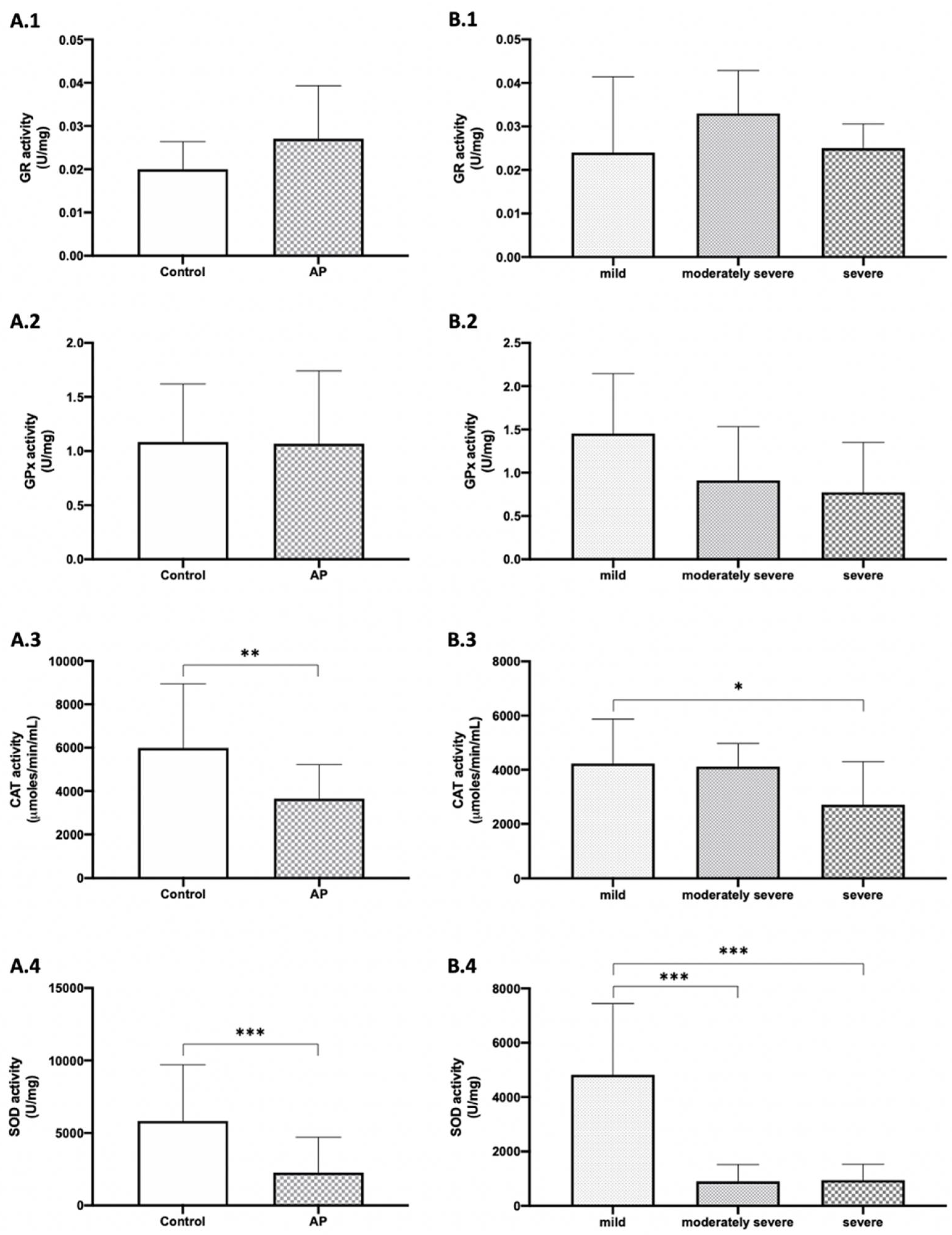
3.2. Patients with Biliary AP Presented Increased Levels of Plasma OS-Related Markers and Lower CAT and SOD Activities Than Healthy Subjects and Increased Levels of Lipid Peroxidation and Lower Levels of CAT and SOD in Severe Biliary AP
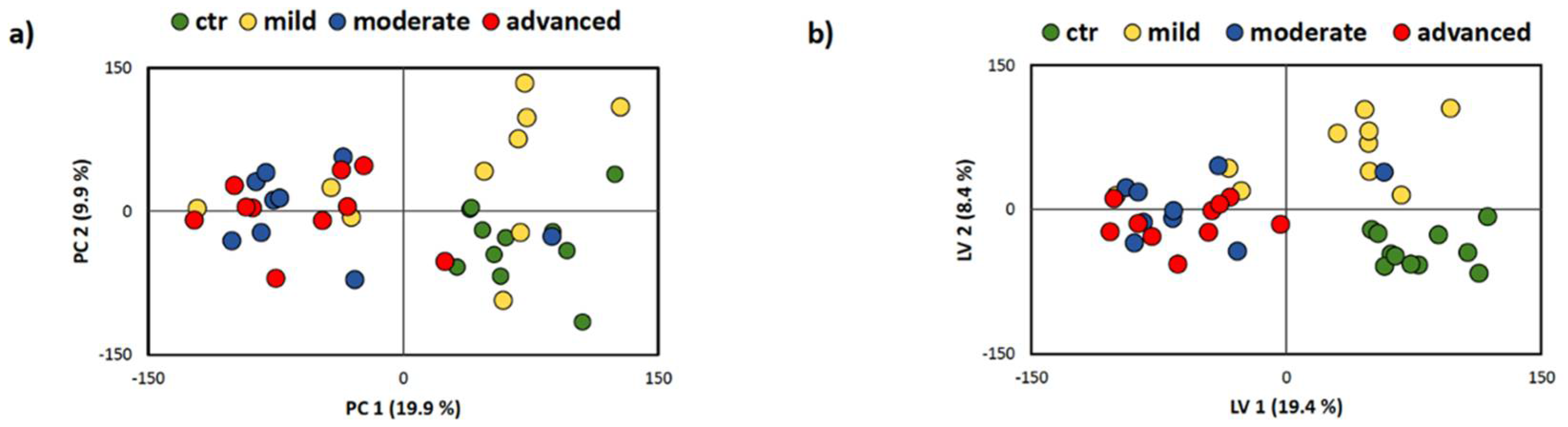
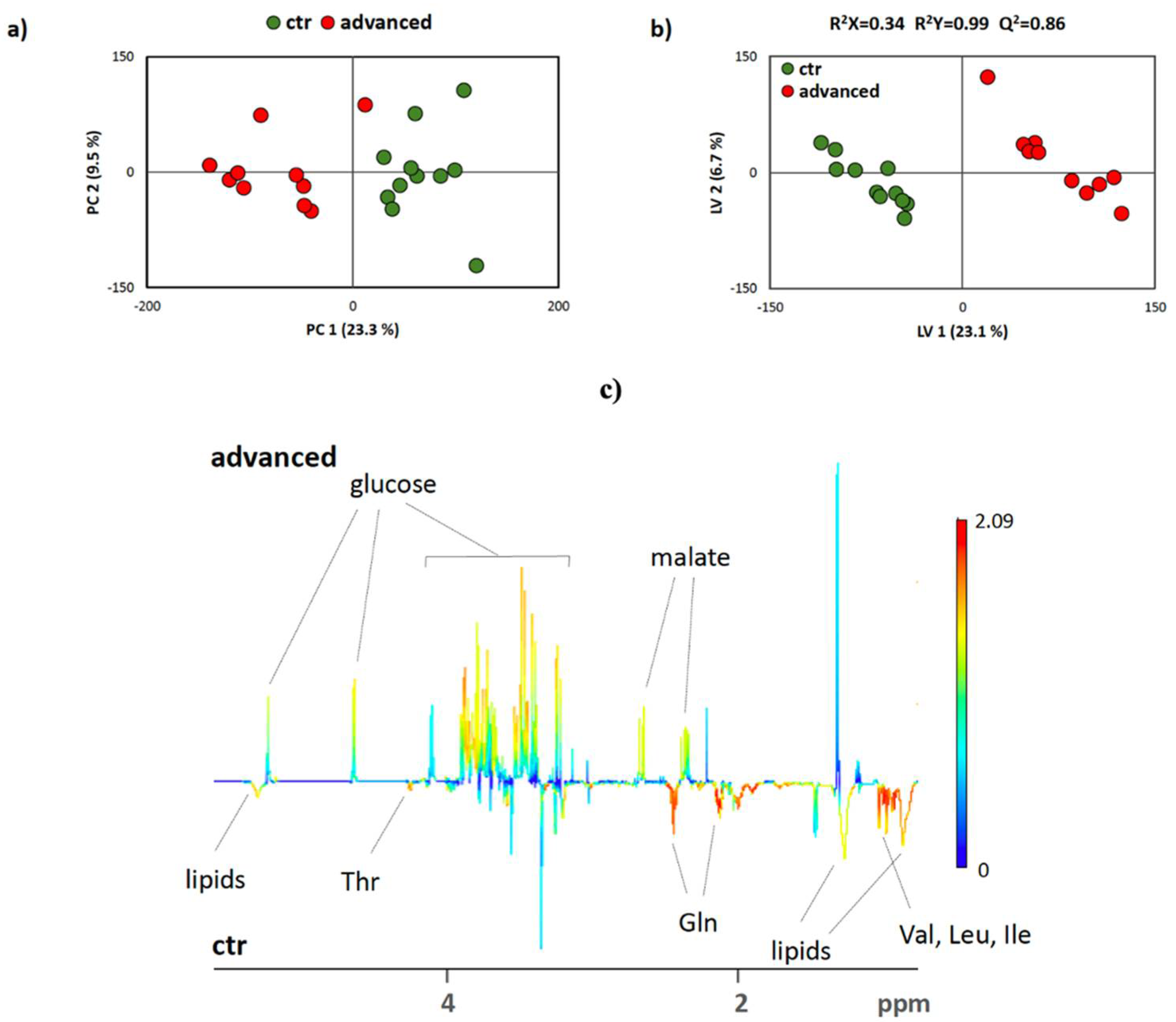
3.3. NMR-Based Metabonomics Analysis of Plasma Samples from AP Patients
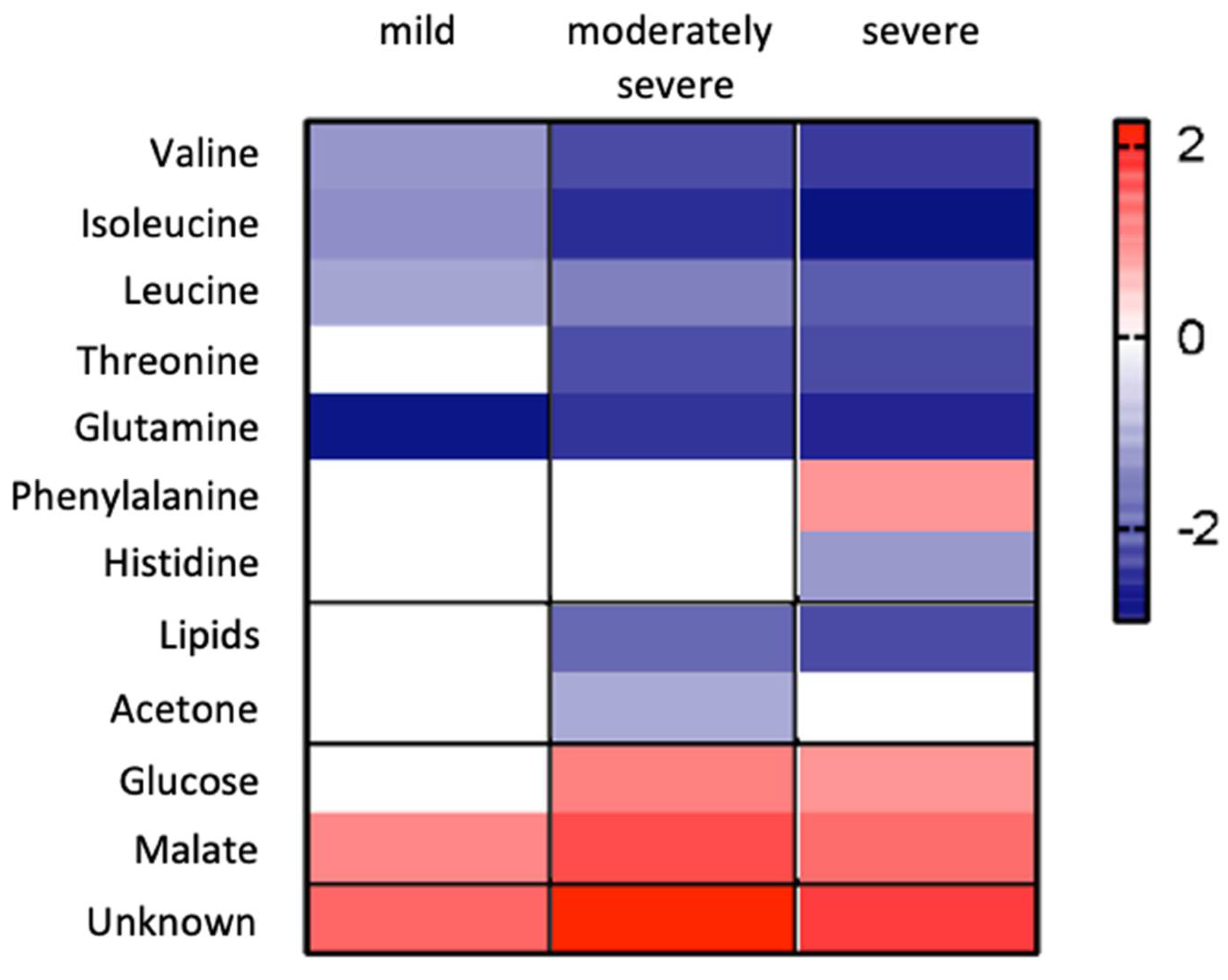
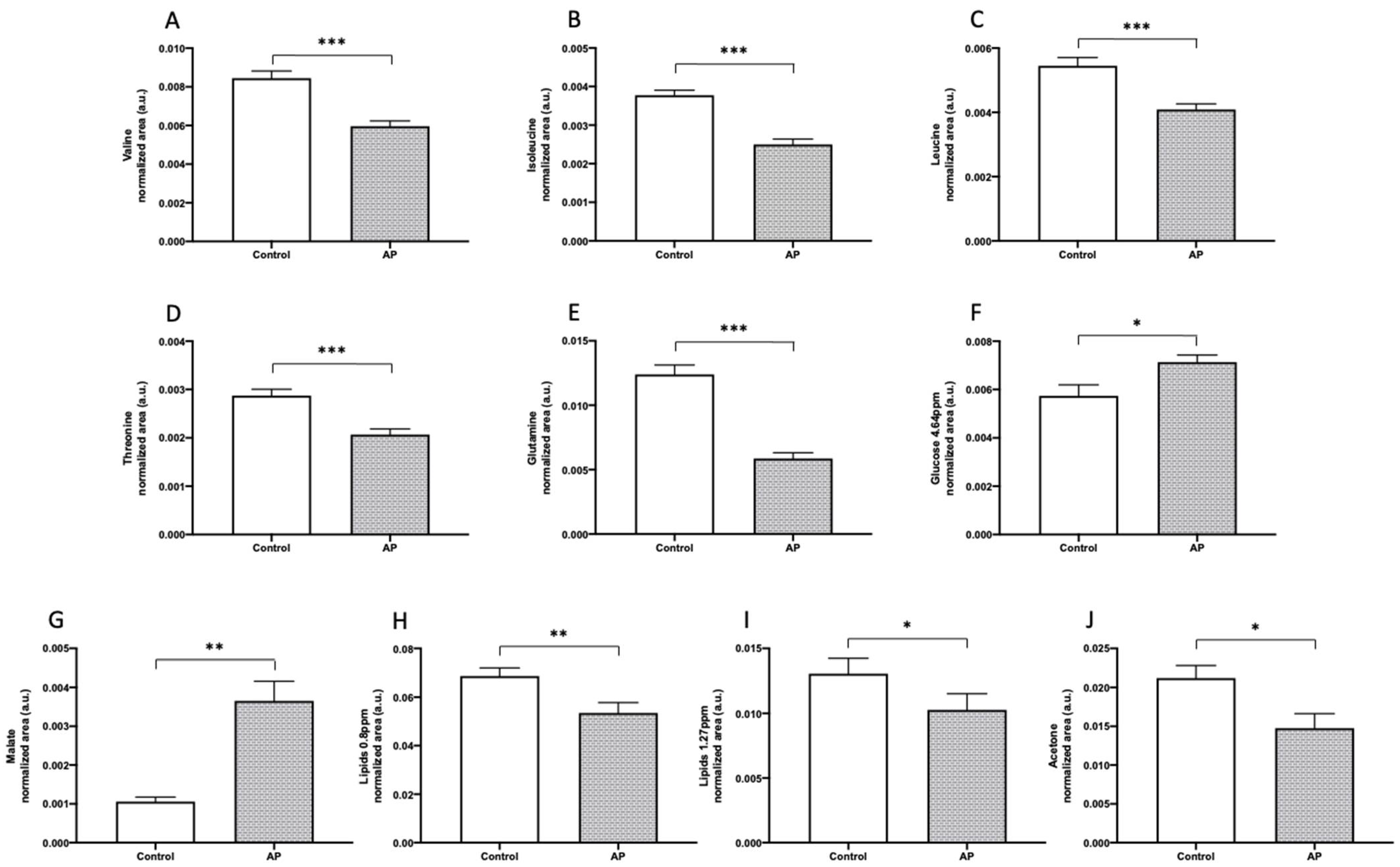
3.4. Plasma Metabolic Profiles Show Differential Response to AP Diagnosis and Prognosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kaplan, M.; Ates, I.; Akpinar, M.Y.; Yuksel, M.; Kuzu, U.B.; Kacar, S.; Coskun, O.; Kayacetin, E. Predictive value of C-reactive protein/albumin ratio in acute pancreatitis. Hepatobiliary Pancreat. Dis. Int. 2017, 16, 424–430. [Google Scholar] [CrossRef]
- Lu, J.D.; Cao, F.; Ding, Y.X.; Wu, Y.D.; Guo, Y.L.; Li, F. Timing, distribution, and microbiology of infectious complications after necrotizing pancreatitis. World J. Gastroenterol. 2019, 25, 5162–5173. [Google Scholar] [CrossRef] [PubMed]
- Singh, V.K.; Bollen, T.L.; Wu, B.U.; Repas, K.; Maurer, R.; Yu, S.; Mortele, K.J.; Conwell, D.L.; Banks, P.A. An assessment of the severity of interstitial pancreatitis. Clin. Gastroenterol. Hepatol. 2011, 9, 1098–1103. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.-J.; Bae, G.-S.; Jo, I.-J.; Choi, S.-B.; Kim, D.-G.; Jung, H.-J.; Song, H.-J.; Park, S.-J. Fraxinellone inhibits inflammatory cell infiltration during acute pancreatitis by suppressing inflammasome activation. Int. Immunopharmacol. 2019, 69, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Hagjer, S.; Kumar, N. Evaluation of the BISAP scoring system in prognostication of acute pancreatitis—A prospective observational study. Int. J. Surg. 2018, 54, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Samanta, J.; Dhaka, N.; Gupta, P.; Singh, A.K.; Yadav, T.D.; Gupta, V.; Sinha, S.K.; Kochhar, R. Comparative study of the outcome between alcohol and gallstone pancreatitis in a high-volume tertiary care center. JGH Open 2019, 3, 338–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva-Vaz, P.; Abrantes, A.M.; Castelo-Branco, M.; Gouveia, A.; Botelho, M.F.; Tralhão, J.G. Murine Models of Acute Pancreatitis: A Critical Appraisal of Clinical Relevance. Int. J. Mol. Sci. 2019, 20, 2794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roberts, S.E.; Morrison-Rees, S.; John, A.; Williams, J.G.; Brown, T.H.; Samuel, D.G. The incidence and aetiology of acute pancreatitis across Europe. Pancreatology 2017, 17, 155–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, G.J.; Gao, C.F.; Wei, D.; Wang, C.; Ding, S.Q. Acute pancreatitis: Etiology and common pathogenesis. World J. Gastroenterol. 2009, 15, 1427–1430. [Google Scholar] [CrossRef] [PubMed]
- Saluja, A.; Dudeja, V.; Dawra, R.; Sah, R.P. Early Intra-Acinar Events in Pathogenesis of Pancreatitis. Gastroenterology 2019, 156, 1979–1993. [Google Scholar] [CrossRef] [PubMed]
- Mayer, A.; McMahon, M.; Bowen, M.; Cooper, E. C reactive protein: An aid to assessment and monitoring of acute pancreatitis. J. Clin. Pathol. 1984, 37, 207–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arabul, M.; Celik, M.; Aslan, O.; Torun, S.; Beyazit, Y.; Alper, E.; Kandemir, A.; Ünsal, B. Hepcidin as a predictor of disease severity in acute pancreatitis: A single center prospective study. Hepatogastroenterology 2013, 60, 595–600. [Google Scholar] [PubMed]
- Silva-Vaz, P.; Abrantes, A.M.; Morgado-Nunes, S.; Castelo-Branco, M.; Gouveia, A.; Botelho, M.F.; Tralhão, J.G. Evaluation of Prognostic Factors of Severity in Acute Biliary Pancreatitis. Int. J. Mol. Sci. 2020, 21, 4300. [Google Scholar] [CrossRef] [PubMed]
- Woo, S.M.; Noh, M.H.; Kim, B.G.; Hsing, C.T.; Han, J.S.; Ryu, S.H.; Seo, J.M.; Yoon, H.A.; Jang, J.S.; Choi, S.R.; et al. Comparison of serum procalcitonin with Ranson, APACHE-II, Glasgow and Balthazar CT severity index scores in predicting severity of acute pancreatitis. Korean J. Gastroenterol. Taehan Sohwagi Hakhoe Chi 2011, 58, 31–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, B.U.; Johannes, R.S.; Sun, X.; Tabak, Y.; Conwell, D.L.; Banks, P.A. The early prediction of mortality in acute pancreatitis: A large population-based study. Gut 2008, 57, 1698–1703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mofidi, R.; Duff, M.; Wigmore, S.; Madhavan, K.; Garden, O.; Parks, R. Association between early systemic inflammatory response, severity of multiorgan dysfunction and death in acute pancreatitis. Br. J. Surg. 2006, 93, 738–744. [Google Scholar] [CrossRef] [PubMed]
- Banks, P.A.; Bollen, T.L.; Dervenis, C.; Gooszen, H.G.; Johnson, C.D.; Sarr, M.G.; Tsiotos, G.G.; Vege, S.S. Classification of acute pancreatitis—2012: Revision of the Atlanta classification and definitions by international consensus. Gut 2013, 62, 102–111. [Google Scholar] [CrossRef] [PubMed]
- Criddle, D.N. Reactive oxygen species, Ca(2+) stores and acute pancreatitis; a step closer to therapy? Cell Calcium 2016, 60, 180–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, B.K.; Chung, J.B.; Lee, J.H.; Suh, J.H.; Park, S.W.; Song, S.Y.; Kim, H.; Kim, K.H.; Kang, J.K. Role of oxygen free radicals in patients with acute pancreatitis. World J. Gastroenterol. 2003, 9, 2266–2269. [Google Scholar] [CrossRef] [PubMed]
- Closa, D. Free radicals and acute pancreatitis: Much ado about...something. Free Radic. Res. 2013, 47, 934–940. [Google Scholar] [CrossRef] [PubMed]
- Booth, D.M.; Mukherjee, R.; Sutton, R.; Criddle, D.N. Calcium and reactive oxygen species in acute pancreatitis: Friend or foe? Antioxid. Redox Signal. 2011, 15, 2683–2698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Que, R.S.; Cao, L.P.; Ding, G.P.; Hu, J.A.; Mao, K.J.; Wang, G.F. Correlation of nitric oxide and other free radicals with the severity of acute pancreatitis and complicated systemic inflammatory response syndrome. Pancreas 2010, 39, 536–540. [Google Scholar] [CrossRef] [PubMed]
- Vayssier-Taussat, M.; Kreps, S.E.; Adrie, C.; Dall’Ava, J.; Christiani, D.; Polla, B.S. Mitochondrial membrane potential: A novel biomarker of oxidative environmental stress. Environ. Health Perspect. 2002, 110, 301–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trumbeckaite, S.; Kuliaviene, I.; Deduchovas, O.; Kincius, M.; Baniene, R.; Virketyte, S.; Bukauskas, D.; Jansen, E.; Kupcinskas, L.; Borutaite, V.; et al. Experimental acute pancreatitis induces mitochondrial dysfunction in rat pancreas, kidney and lungs but not in liver. Pancreatology 2013, 13, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Rau, B.; Poch, B.; Gansauge, F.; Bauer, A.; Nüssler, A.K.; Nevalainen, T.; Schoenberg, M.H.; Beger, H.G. Pathophysiologic role of oxygen free radicals in acute pancreatitis: Initiating event or mediator of tissue damage? Ann. Surg. 2000, 231, 352–360. [Google Scholar] [CrossRef] [PubMed]
- Gu, W.; Tong, Z. Clinical Application of Metabolomics in Pancreatic Diseases: A Mini-Review. Lab. Med. 2020, 51, 116–121. [Google Scholar] [CrossRef] [PubMed]
- Villasenor, A.; Kinross, J.M.; Li, J.V.; Penney, N.; Barton, R.H.; Nicholson, J.K.; Darzi, A.; Barbas, C.; Holmes, E. 1H NMR global metabolic phenotyping of acute pancreatitis in the emergency unit. J. Proteome Res. 2014, 13, 5362–5375. [Google Scholar] [CrossRef] [PubMed]
- Lusczek, E.R.; Paulo, J.A.; Saltzman, J.R.; Kadiyala, V.; Banks, P.A.; Beilman, G.; Conwell, D.L. Urinary 1H-NMR metabolomics can distinguish pancreatitis patients from healthy controls. JOP J. Pancreas 2013, 14, 161–170. [Google Scholar]
- Xu, H.; Zhang, L.; Kang, H.; Zhang, J.; Liu, J.; Liu, S. Serum Metabonomics of Mild Acute Pancreatitis. J. Clin. Lab. Anal. 2016, 30, 990–998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, H.; Huang, J.-h.; Zhang, X.-w.; Ahmed, R.; Xie, Q.-l.; Li, B.; Zhu, Y.-m.; Cai, X.; Peng, Q.-h.; Qin, Y.-h. Identification of potential diagnostic biomarkers of acute pancreatitis by serum metabolomic profiles. Pancreatology 2017, 17, 543–549. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.H.; He, D.; Chen, L.; Dong, C.Y.; Zhang, S.H.; Qin, Y.H.; Yu, R.; Ahmed, R.; Kuang, J.J.; Zhang, X.W. GC-MS based metabolomics strategy to distinguish three types of acute pancreatitis. Pancreatology 2019, 19, 630–637. [Google Scholar] [CrossRef] [PubMed]
- Weitz, G.; Woitalla, J.; Wellhöner, P.; Schmidt, K.J.; Büning, J.; Fellermann, K. Comorbidity in acute pancreatitis relates to organ failure but not to local complications. Z. Gastroenterol. 2016, 54, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Brusselaers, N.; Lagergren, J. The Charlson Comorbidity Index in Registry-based Research. Methods Inf. Med. 2017, 56, 401–406. [Google Scholar] [PubMed]
- Dias, T.R.; Alves, M.G.; Bernardino, R.L.; Martins, A.D.; Moreira, A.C.; Silva, J.; Barros, A.; Sousa, M.; Silva, B.M.; Oliveira, P.F. Dose-dependent effects of caffeine in human Sertoli cells metabolism and oxidative profile: Relevance for male fertility. Toxicology 2015, 328, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, P.F.; Tomas, G.D.; Dias, T.R.; Martins, A.D.; Rato, L.; Alves, M.G.; Silva, B.M. White tea consumption restores sperm quality in prediabetic rats preventing testicular oxidative damage. Reprod. Biomed. Online 2015, 31, 544–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, M.A.; Cerniglia, G.J.; Zaman, A. Microtiter plate assay for the measurement of glutathione and glutathione disulfide in large numbers of biological samples. Anal. Biochem. 1990, 190, 360–365. [Google Scholar] [CrossRef]
- Oguntibeju, O.O.; Meyer, S.; Aboua, Y.G.; Goboza, M. Hypoxis hemerocallidea Significantly Reduced Hyperglycaemia and Hyperglycaemic-Induced Oxidative Stress in the Liver and Kidney Tissues of Streptozotocin-Induced Diabetic Male Wistar Rats. Evid. Based Complementary Altern. Med. 2016, 2016, 8934362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alves, M.G.; Oliveira, P.J.; Carvalho, R.A. Substrate selection in hearts subjected to ischemia/reperfusion: Role of cardioplegic solutions and gender. NMR Biomed. 2011, 24, 1029–1037. [Google Scholar] [CrossRef] [PubMed]
- Wishart, D.S.; Feunang, Y.D.; Marcu, A.; Guo, A.C.; Liang, K.; Vazquez-Fresno, R.; Sajed, T.; Johnson, D.; Li, C.; Karu, N.; et al. HMDB 4.0: The human metabolome database for 2018. Nucleic Acids Res. 2018, 46, D608–D617. [Google Scholar] [CrossRef] [PubMed]
- Jarak, I.; Carrola, J.; Barros, A.S.; Gil, A.M.; Pereira, M.L.; Corvo, M.L.; Duarte, I.F. From the Cover: Metabolism Modulation in Different Organs by Silver Nanoparticles: An NMR Metabolomics Study of a Mouse Model. Toxicol. Sci. 2017, 159, 422–435. [Google Scholar] [CrossRef] [Green Version]
- Savorani, F.; Tomasi, G.; Engelsen, S.B. icoshift: A versatile tool for the rapid alignment of 1D NMR spectra. J. Magn. Reson. 2010, 202, 190–202. [Google Scholar] [CrossRef] [PubMed]
- Dieterle, F.; Ross, A.; Schlotterbeck, G.; Senn, H. Probabilistic quotient normalization as robust method to account for dilution of complex biological mixtures. Application in 1H NMR metabonomics. Anal. Chem. 2006, 78, 4281–4290. [Google Scholar] [CrossRef] [PubMed]
- Triba, M.N.; Le Moyec, L.; Amathieu, R.; Goossens, C.; Bouchemal, N.; Nahon, P.; Rutledge, D.N.; Savarin, P. PLS/OPLS models in metabolomics: The impact of permutation of dataset rows on the K-fold cross-validation quality parameters. Mol. Biosyst. 2015, 11, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Berben, L.; Sereika, S.M.; Engberg, S. Effect size estimation: Methods and examples. Int. J. Nurs. Stud. 2012, 49, 1039–1047. [Google Scholar] [CrossRef] [PubMed]
- van Dijk, S.M.; Hallensleben, N.D.; van Santvoort, H.C.; Fockens, P.; van Goor, H.; Bruno, M.J.; Besselink, M.G. Acute pancreatitis: Recent advances through randomised trials. Gut 2017, 66, 2024–2032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva-Vaz, P.; Abrantes, A.M.; Castelo-Branco, M.; Gouveia, A.; Botelho, M.F.; Tralhao, J.G. Multifactorial Scores and Biomarkers of Prognosis of Acute Pancreatitis: Applications to Research and Practice. Int. J. Mol. Sci. 2020, 21, 338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cartwright, S.L.; Knudson, M.P. Evaluation of acute abdominal pain in adults. Am. Fam. Physician 2008, 77, 971–978. [Google Scholar] [PubMed]
- Li, J.; Zhu, S.F.; Zhao, X.L.; Liu, Y.X.; Wan, M.H.; Guo, H.; Liu, Y.L.; Gong, H.L.; Chen, G.Y.; Tang, W.F. Metabolomic profiles illuminate the efficacy of Chinese herbal Da-Cheng-Qi decoction on acute pancreatitis in rats. Pancreatology 2015, 15, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Chen, D.Z.; Lang, R.; Jin, Z.K.; Fan, H.; Wu, T.M.; Li, X.L.; He, Q. Enhanced recovery in the management of mild gallstone pancreatitis: A prospective cohort study. Surg. Today 2013, 43, 643–647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khanna, A.K.; Meher, S.; Prakash, S.; Tiwary, S.K.; Singh, U.; Srivastava, A.; Dixit, V. Comparison of Ranson, Glasgow, MOSS, SIRS, BISAP, APACHE-II, CTSI Scores, IL-6, CRP, and procalcitonin in predicting severity, organ failure, pancreatic necrosis, and mortality in acute pancreatitis. HPB Surg. 2013, 2013, 367581. [Google Scholar] [CrossRef] [PubMed]
- Al-Nawas, B.; Krammer, I.; Shah, P.M. Procalcitonin in diagnosis of severe infections. Eur. J. Med. Res. 1996, 1, 331–333. [Google Scholar] [PubMed]
- Gu, L.; Ma, X.; Wang, L.; Li, H.; Chen, L.; Li, X.; Zhang, Y.; Xie, Y.; Zhang, X. Prognostic value of a systemic inflammatory response index in metastatic renal cell carcinoma and construction of a predictive model. Oncotarget 2017, 8, 52094–52103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.; Kong, X.; Wang, Z.; Wang, X.; Fang, Y.; Wang, J. Pretreatment Systemic Inflammation Response Index in Patients with Breast Cancer Treated with Neoadjuvant Chemotherapy as a Useful Prognostic Indicator. Cancer Manag. Res. 2020, 12, 1543–1567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardoso, F.S.; Ricardo, L.B.; Oliveira, A.M.; Horta, D.V.; Papoila, A.L.; Deus, J.R.; Canena, J. C-Reactive Protein at 24 Hours after Hospital Admission may have Relevant Prognostic Accuracy in Acute Pancreatitis: A Retrospective Cohort Study. GE Port. J. Gastroenterol. 2015, 22, 198–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kulaksiz, H.; Fein, E.; Redecker, P.; Stremmel, W.; Adler, G.; Cetin, Y. Pancreatic b-cells express hepcidin, an iron-uptake regulatory peptide. J. Endocrinol. 2008, 197, 241–250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babitt, J.L.; Huang, F.W.; Wrighting, D.M.; Xia, Y.; Sidis, Y.; Samad, T.A.; Campagna, J.A.; Chung, R.T.; Schneyer, A.L.; Woolf, C.J. Bone morphogenetic protein signaling by hemojuvelin regulates hepcidin expression. Nat. Genet. 2006, 38, 531. [Google Scholar] [CrossRef] [PubMed]
- Perez, S.; Pereda, J.; Sabater, L.; Sastre, J. Redox signaling in acute pancreatitis. Redox Biol. 2015, 5, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, J.Y.; Lim, J.W.; Kim, H.; Morio, T.; Kim, K.H. Oxidative stress induces nuclear loss of DNA repair proteins Ku70 and Ku80 and apoptosis in pancreatic acinar AR42J cells. J. Biol. Chem. 2003, 278, 36676–36687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abu-Hilal, M.; McPhail, M.J.; Marchand, L.; Johnson, C.D. Malondialdehyde and superoxide dismutase as potential markers of severity in acute pancreatitis. JOP J. Pancreas 2006, 7, 185–192. [Google Scholar]
- Marek, G.; Ściskalska, M.; Grzebieniak, Z.; Milnerowicz, H. Decreases in Paraoxonase-1 Activities Promote a Pro-inflammatory Effect of Lipids Peroxidation Products in Non-smoking and Smoking Patients with Acute Pancreatitis. Int. J. Med. Sci. 2018, 15, 1619–1630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sajewicz, W.; Milnerowicz, S.; Nabzdyk, S. Blood plasma antioxidant defense in patients with pancreatitis. Pancreas 2006, 32, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Abreu, F.F.; Souza, A.C.A.; Teixeira, S.A.; Soares, A.G.; Teixeira, D.F.; Soares, R.C.; Santana, M.T.; Lauton Santos, S.; Costa, S.K.P.; Muscará, M.N.; et al. Elucidating the role of oxidative stress in the therapeutic effect of rutin on experimental acute pancreatitis. Free Radic. Res. 2016, 50, 1350–1360. [Google Scholar] [CrossRef] [PubMed]
- Bopanna, S.; Nayak, B.; Prakash, S.; Shalimar; Mahapatra, S.J.; Garg, P.K. Increased oxidative stress and deficient antioxidant levels may be involved in the pathogenesis of idiopathic recurrent acute pancreatitis. Pancreatology 2017, 17, 529–533. [Google Scholar] [CrossRef] [PubMed]
- Jarak, I.; Almeida, S.; Carvalho, R.A.; Sousa, M.; Barros, A.; Alves, M.G.; Oliveira, P.F. Senescence and declining reproductive potential: Insight into molecular mechanisms through testicular metabolomics. Biochim. Biophys. Acta Mol. Basis Dis. 2018, 1864, 3388–3396. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Ma, C.; Liao, Z.; Tian, B.; Lu, J.P. Study on chronic pancreatitis and pancreatic cancer using MRS and pancreatic juice samples. World J. Gastroenterol. 2011, 17, 2126–2130. [Google Scholar] [CrossRef] [PubMed]
- Jeurnink, S.M.; Nijs, M.M.; Prins, H.A.; Greving, J.P.; Siersema, P.D. Antioxidants as a treatment for acute pancreatitis: A meta-analysis. Pancreatology 2015, 15, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Kim, H. Glutamine as an immunonutrient. Yonsei Med. J. 2011, 52, 892–897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grimble, R.F. The Interaction Between Nutrition and Inflammatory Stress Throughout the Life Cycle. In Nutrients, Stress and Medical Disorders; Yehuda, S., Mostofsky, D.I., Eds.; Humana Press: Totowa, NJ, USA, 2005; pp. 387–424. [Google Scholar]
- Tang, M.; Hu, G.; Zhao, Y.; Su, M.; Wang, Y.; Jia, W.; Qiu, Y.; Liu, G.; Wang, X. A serum metabolomic investigation on lipoprotein lipase-deficient mice with hyperlipidemic pancreatitis using gas chromatography/mass spectrometry. Biomed. Rep. 2013, 1, 469–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dong, Y.W.; Jiang, W.D.; Liu, Y.; Wu, P.; Jiang, J.; Kuang, S.Y.; Tang, L.; Tang, W.N.; Zhang, Y.A.; Zhou, X.Q.; et al. Threonine deficiency decreased intestinal immunity and aggravated inflammation associated with NF-kappaB and target of rapamycin signalling pathways in juvenile grass carp (Ctenopharyngodon idella) after infection with Aeromonas hydrophila. Br. J. Nutr. 2017, 118, 92–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, S.S.; Lin, J.Y.; Chen, W.S.; Liu, M.H.; Cheng, C.W.; Cheng, M.L.; Wang, C.H. Phenylalanine- and leucine-defined metabolic types identify high mortality risk in patients with severe infection. Int. J. Infect. Dis. 2019, 85, 143–149. [Google Scholar] [CrossRef] [Green Version]
- Biczo, G.; Vegh, E.T.; Shalbueva, N.; Mareninova, O.A.; Elperin, J.; Lotshaw, E.; Gretler, S.; Lugea, A.; Malla, S.R.; Dawson, D.; et al. Mitochondrial Dysfunction, Through Impaired Autophagy, Leads to Endoplasmic Reticulum Stress, Deregulated Lipid Metabolism, and Pancreatitis in Animal Models. Gastroenterology 2018, 154, 689–703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szymanska, E.; Frydenvang, K.; Pickering, D.S.; Krintel, C.; Nielsen, B.; Kooshki, A.; Zachariassen, L.G.; Olsen, L.; Kastrup, J.S.; Johansen, T.N. Studies on Aryl-Substituted Phenylalanines: Synthesis, Activity, and Different Binding Modes at AMPA Receptors. J. Med. Chem. 2016, 59, 448–461. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control (n = 11) | Sample (n = 29) | p | Mild AP (n = 10) | Moderately Severe AP (n = 9) | Severe AP (n = 10) | p | |
|---|---|---|---|---|---|---|---|
| Age (years) | 69 14.6 | 65 18.9 | 0.65 ‡ | 54 16.8 | 69 17.2 | 73 18.7 | 0.53 ‡‡‡ |
| Female sex | 6 (54.5%) | 20 (69%) | 0.41 ‡‡ | 8 (80%) | 6 (66.7%) | 6 (60%) | 0.39 ‡‡ |
| BMI (kg/m2) | 26.7 3.0 | 26.7 3.8 | 0.98 ‡ | 27.0 2.9 | 26.4 4.6 | 26.6 4.0 | 0.92 ‡‡‡ |
| BMI 30 kg/m2 | 2 (18.2%) | 6 (20.7%) | 0.91 ‡‡ | 2 (20%) | 2 (22.2%) | 2 (20%) | 0.91 ‡‡ |
| CCI | 3 (1–4) | 3 (1–4) | 0.49 ‡ | 1 (0–2) | 3 (2–4) | 3 (1–4) | 0.49 ‡‡‡ |
| Hospital stay (days) | 12 7.8 | - | 6 2.5 | 11 5.0 | 18 8.7 | - | |
| Mortality | 3 (10.3%) | 3 (30%) |
| Controls (n = 11) | Time | Sample (n = 29) | Mild AP (n = 10) | Moderately Severe AP (n = 9) | Severe AP (n = 10) | p‡ | |
|---|---|---|---|---|---|---|---|
| WBC | 6.5 1.6 | Admission | 14.5 5.4 | 11.2 4.5 | 15.0 5.6 | 17.4 4.1 | 0.017 |
| 48 h | 12.1 6.3 | 6.9 3.5 | 12.7 7.5 | 14.9 2.8 | 0.002 | ||
| Neutrophils | 4.8 0.9 | Admission | 12.4 5.5 | 8.6 4.5 | 13.2 5.3 | 15.7 3.6 | 0.011 |
| 48 h | 10.0 6.2 | 4.7 3.2 | 10.4 6.9 | 13.2 2.7 | 0.001 | ||
| SIRI | Aission | 7.4 6.3 | 3.6 3.9 | 8.8 7.5 | 11.4 4.9 | 0.022 | |
| 48 h | 6.6 6.4 | 1.6 2.3 | 5.9 6.4 | 10.6 5.7 | 0.001 | ||
| PCT | Admission | 2.9 6.9 | 0.7 0.9 | 4.5 5.8 | 5.9 10.9 | 0.001 | |
| 48 h | 4.1 7.3 | 0.6 0.1 | 6.6 9.1 | 7.9 8.8 | <0.001 | ||
| CRP | 5.3 1.1 | Admission | 42.8 82.7 | 5.4 1.2 | 33.0 51.5 | 88.9 22.0 | 0.032 |
| 48 h | 170.7 152.6 | 15.9 14.0 | 180.6 107.2 | 316.6 107.9 | <0.001 | ||
| Hepcidin | Admission | 64.2 69.6 | 20.4 12.2 | 69.9 37.9 | 100.7 90.5 | 0.047 | |
| 48 h | 136.7 138.7 | 26.4 27.2 | 56.6 51.9 | 286.7 87.3 | <0.001 | ||
| Calcium | Admission | 9.0 0.6 | 8.9 0.5 | 9.1 0.4 | 8.9 0.9 | NS | |
| 48 h | 8.5 0.8 | 8.9 0.3 | 8.7 0.5 | 7.9 1.0 | 0.014 | ||
| Albumin | Admission | 3.7 0.5 | 3.8 0.4 | 3.7 0.4 | 3.5 0.5 | NS | |
| 48 h | 3.1 0.5 | 3.5 0.3 | 3.2 0.3 | 2.7 0.6 | 0.001 | ||
| Total proteins | Admission | 6.5 0.6 | 6.7 0.5 | 6.7 0.5 | 6.3 0.6 | NS | |
| 48 h | 5.9 0.6 | 6.4 0.4 | 6.0 0.3 | 5.3 0.6 | 0.001 | ||
| BISAP | Admission | 1 (1–3) | 1 (0–1) | 1 (1–2) | 3 (2–3) | <0.001 | |
| 48 h | 2 (1–4) | 1 (0–1) | 1 (1–3) | 4 (4–5) | <0.001 | ||
| SIRS | Admission | 1 (1–2) | 1 (0–1) | 2 (1–2) | 2 (1–2) | 0.045 | |
| 48 h | 1 (0–2) | 0 (0–1) | 1 (0–2) | 3 (2–3) | 0.001 | ||
| MMS | Admission | 0 (0–1) | 0 (0–0) | 0 (0–2) | 1 (0–2) | 0.017 | |
| 48 h | 0 (0–2) | 0 (0–0) | 0 (0–2) | 3 (2–3) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva-Vaz, P.; Jarak, I.; Rato, L.; Oliveira, P.F.; Morgado-Nunes, S.; Paulino, A.; Castelo-Branco, M.; Botelho, M.F.; Tralhão, J.G.; Alves, M.G.; et al. Plasmatic Oxidative and Metabonomic Profile of Patients with Different Degrees of Biliary Acute Pancreatitis Severity. Antioxidants 2021, 10, 988. https://doi.org/10.3390/antiox10060988
Silva-Vaz P, Jarak I, Rato L, Oliveira PF, Morgado-Nunes S, Paulino A, Castelo-Branco M, Botelho MF, Tralhão JG, Alves MG, et al. Plasmatic Oxidative and Metabonomic Profile of Patients with Different Degrees of Biliary Acute Pancreatitis Severity. Antioxidants. 2021; 10(6):988. https://doi.org/10.3390/antiox10060988
Chicago/Turabian StyleSilva-Vaz, Pedro, Ivana Jarak, Luís Rato, Pedro F. Oliveira, Sara Morgado-Nunes, Aida Paulino, Miguel Castelo-Branco, Maria Filomena Botelho, José Guilherme Tralhão, Marco G. Alves, and et al. 2021. "Plasmatic Oxidative and Metabonomic Profile of Patients with Different Degrees of Biliary Acute Pancreatitis Severity" Antioxidants 10, no. 6: 988. https://doi.org/10.3390/antiox10060988