
Clivus-Cervical Stabilization through Transoral Approach in Patients with Craniocervical Tumor: Three Cases and Surgical Technical Note

 and
and
Abstract
:1. Introduction
2. Design/Methods
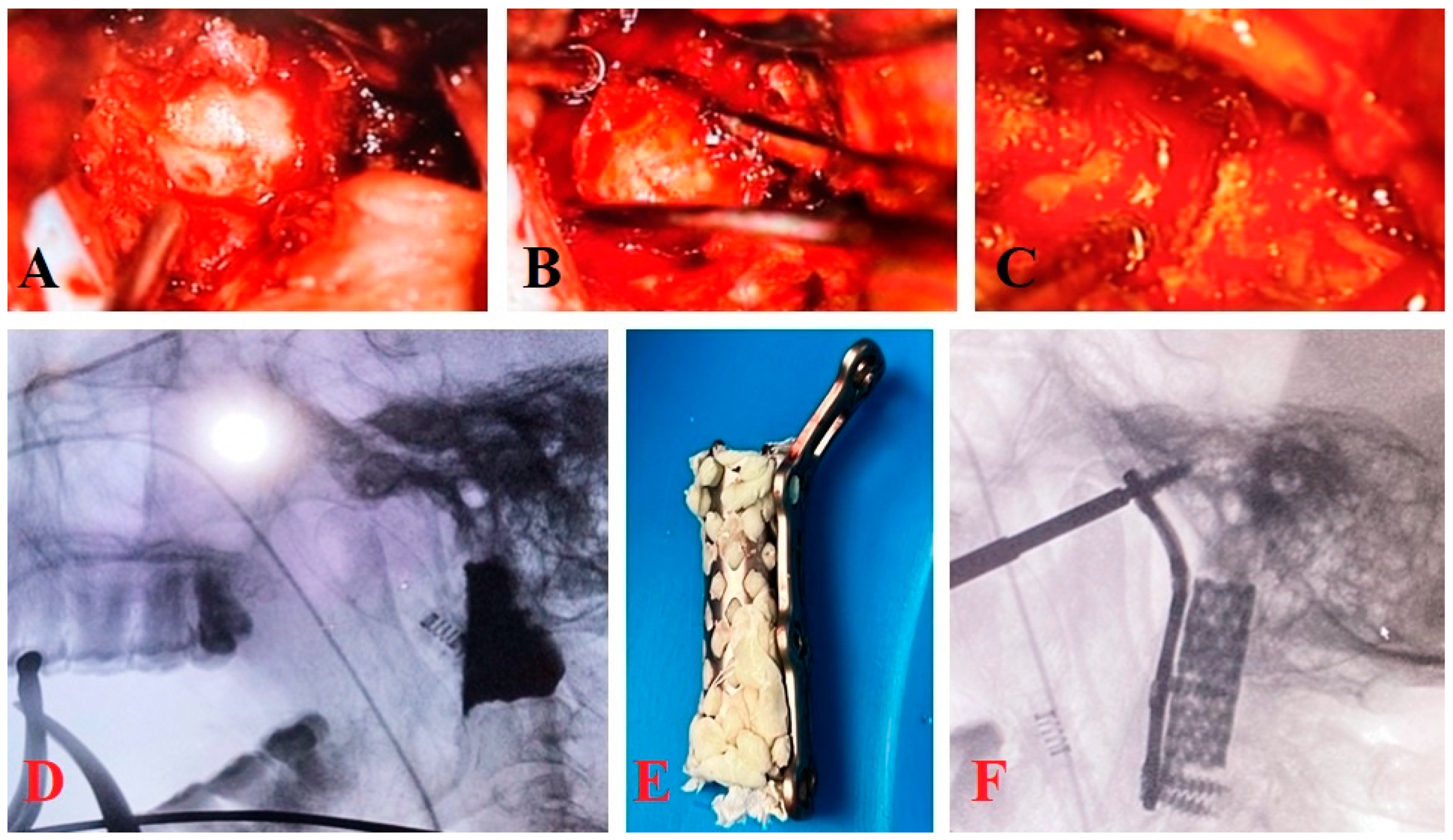
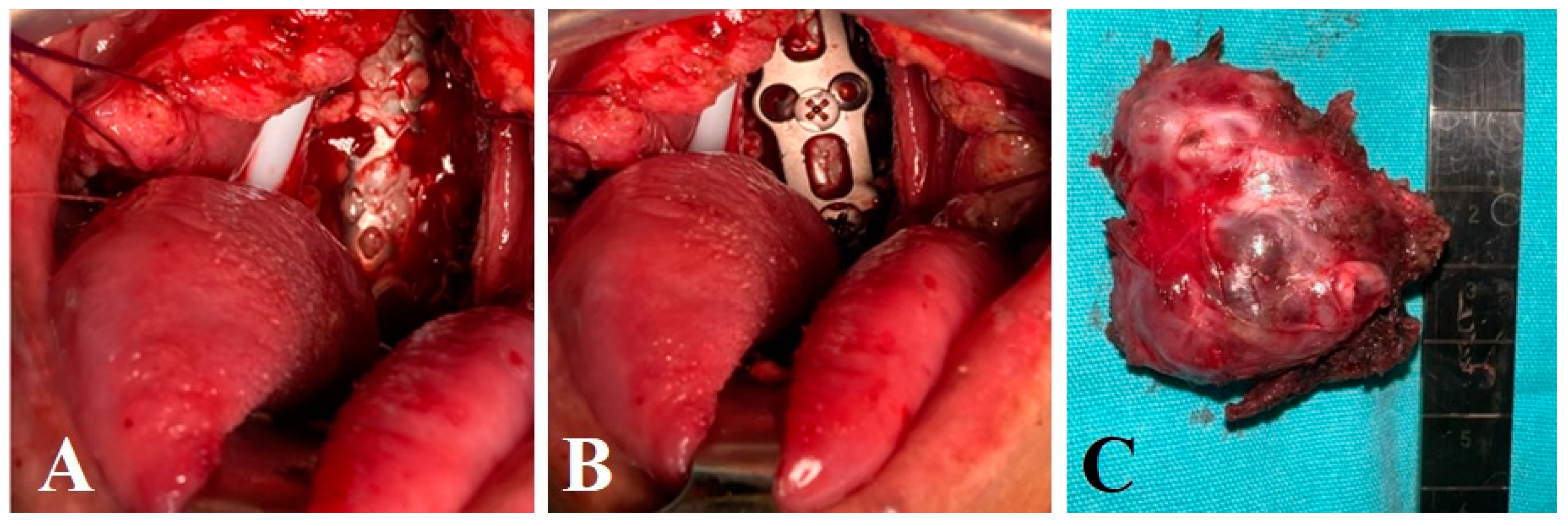
Surgical Technique
3. Results
3.1. Clinical Cases
3.1.1. Clinical Case 1
3.1.2. Clinical Case 2
3.1.3. Clinical Case 3
3.2. Outcome and Surgical Complications
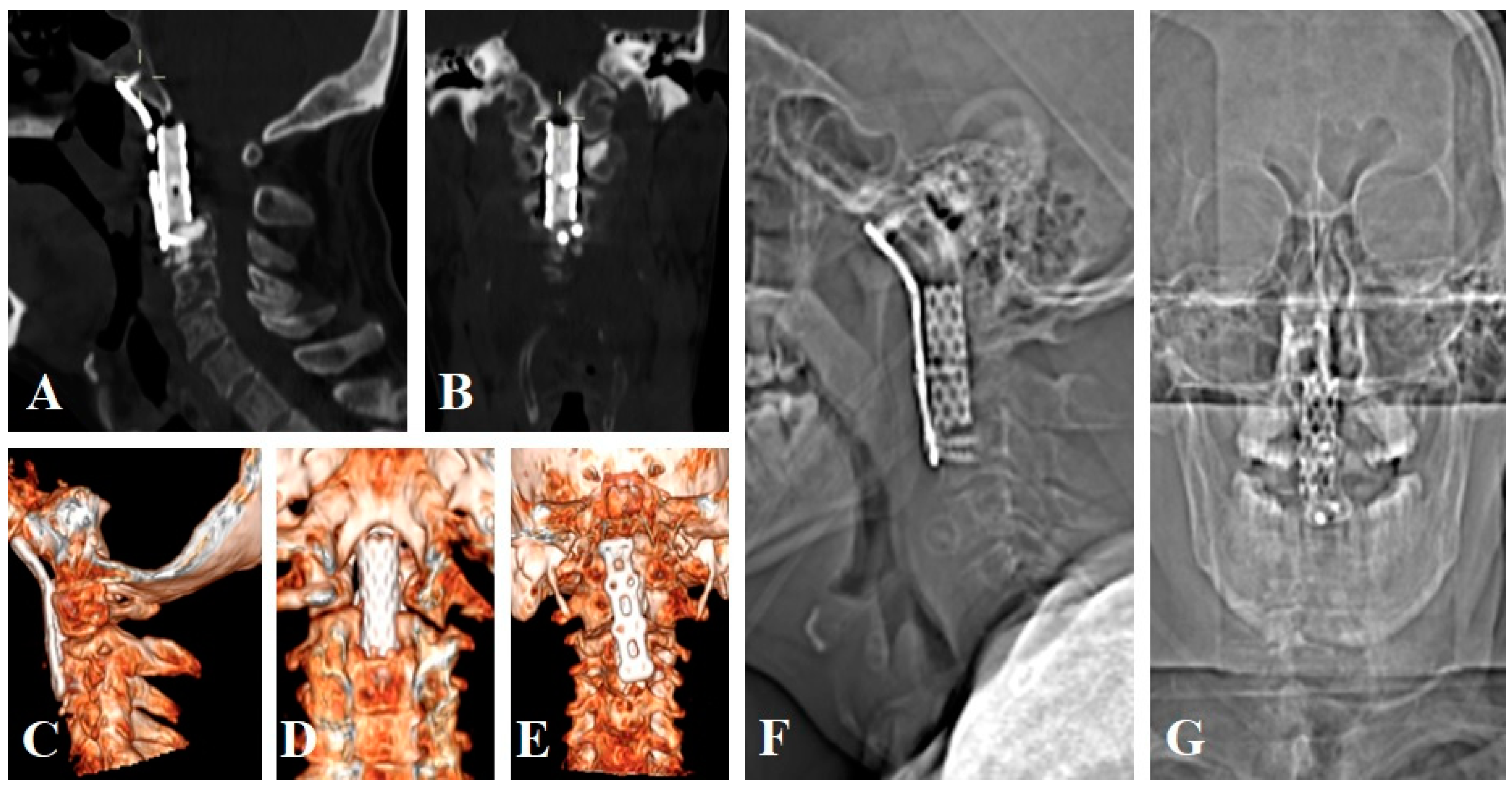
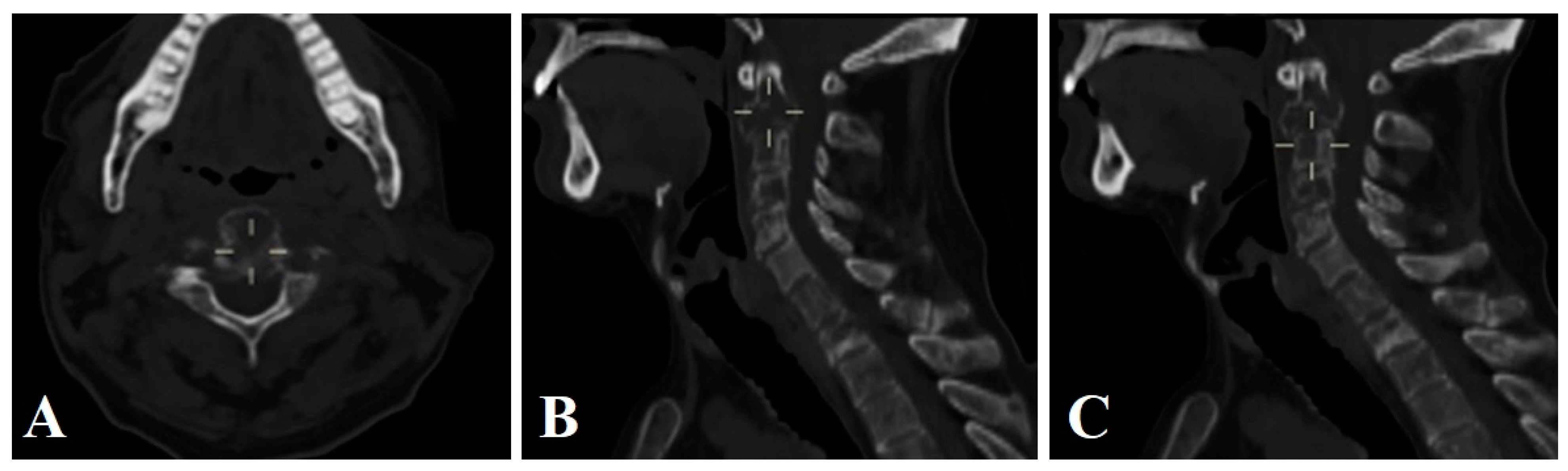
3.3. Surgical Technique and Radiological Follow-Up
4. Discussion
4.1. Incorporating Advanced Surgical Technologies
4.2. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- González-Díaz, R.; Egea-Gámez, R.M.; Ortega-García, F.J.; González-Menocal, A.; Galán-Olleros, M. Management of vertebral metastases in the cervico-occipital junction. Rev. Esp. Cir. Ortop. Traumatol. 2023, 67, S505–S510. [Google Scholar]
- Bakker, S.H.; Jacobs, W.C.H.; Pondaag, W.; Gelderblom, H.; Nout, R.A.; Dijkstra, P.D.S.; Peul, W.C.; Vleggeert-Lankamp, C.L.A. Chordoma: A systematic review of the epidemiology and clinical prognostic factors predicting progression-free and overall survival. Eur. Spine J. 2018, 27, 3043–3058. [Google Scholar] [CrossRef]
- Biega, P.; Guzik, G.; Pitera, T. Surgical treatment outcomes in metastatic tumours located at the craniocervical junction. Ortop. Traumatol. Rehabil. 2018, 20, 5–13. [Google Scholar] [CrossRef] [PubMed]
- O’sullivan, M.D.; Lyons, F.; Morris, S.; Synnott, K.; Munigangaiah, S.; Devitt, A. Metastasis Affecting Craniocervical Junction: Current Concepts and an Update on Surgical Management. Glob. Spine J. 2018, 8, 866–871. [Google Scholar] [CrossRef] [PubMed]
- Ottenhausen, M.; Greco, E.; Bertolini, G.; Gerosa, A.; Ippolito, S.; Middlebrooks, E.H.; Serrao, G.; Bruzzone, M.G.; Costa, F.; Ferroli, P.; et al. Craniovertebral Junction Instability after Oncological Resection: A Narrative Review. Diagnostics 2023, 13, 1502. [Google Scholar] [CrossRef] [PubMed]
- Cano Gómez, J.C.; Mantic Lugo, M.; Vela Panés, T.; García Guerrero, G.L. Epidemiology and clinic of vertebral metastasis. Rev. Esp. Cir. Ortop. Traumatol. 2023, 1, 1. [Google Scholar]
- Joaquim, A.F.; Osorio, J.A.; Riew, K.D. Transoral and endoscopic endonasal odontoidectomies—Surgical techniques, indications, and complications. Neurospine 2019, 16, 462–469. [Google Scholar] [CrossRef]
- Reyes Soto, G.; Cacho-Díaza, B.; Bravo-Reynab, C.; Guerra-Mora, J.R.; Ovalles, C.; Catillo-Rangel, C.; Ramirez, M.J.E.; Montemurro, N. Prognostic Factors Associated with Overall Survival in Breast Cancer Patients with Metastatic Spinal Disease. Cureus 2023, 15, e48909. [Google Scholar] [CrossRef] [PubMed]
- Soto, G.R.; Torres, C.S.O.; Terrazas, J.P.; Partida, K.H.; Rosario, A.R.; Campero, A.; Baldoncini, M.; Ramirez, M.d.J.E.; Montemurro, N. Multiple Myeloma Treatment Challenges: A Case Report of Vertebral Artery Pseudoaneurysm Complicating Occipitocervical Arthrodesis and a Review of the Literature. Cureus 2023, 15, e49716. [Google Scholar]
- Hsu, W.; Wolinsky, J.P.; Gokaslan, Z.L.; Sciubba, D.M. Transoral Approaches to the Cervical Spine. Neurosurgery 2010, 66, A119–A125. [Google Scholar] [CrossRef]
- Pennington, Z.; Westbroek, E.M.; Lo, S.; Sciubba, D.M. Surgical Approaches to Tumors of the Occipito-Cervical, Subaxial Cervical, and Cervicothoracic Spine: An Algorithm for Standard versus Extended Anterior Cervical Access. World Neurosurg. 2021, 156, e41–e56. [Google Scholar] [CrossRef]
- Yaniv, D.; Soudry, E.; Strenov, Y.; Cohen, M.A.; Mizrachi, A. Skull base chordomas review of current treatment paradigms. World J. Otorhinolaryngol. Head. Neck Surg. 2020, 6, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Peng, Z.; Wang, Y.; Fan, R.; Zhang, H.; Jiang, W. The prognostic significance of different degrees of resection of skull base chordoma. Clin. Transl. Oncol. 2022, 24, 2441–2452. [Google Scholar] [CrossRef] [PubMed]
- Korwutthikulrangsri, E.; Ongard, S.; Pisutbenya, J.; Ruangchainikom, M.; Sutipornpalangkul, W. Midterm outcome after en bloc resection of C2 chordoma with transoral mandibular split and mesh cage reconstruction: A case report. J. Med. Case Rep. 2023, 17, 1. [Google Scholar] [CrossRef] [PubMed]
- Quirk, B.; Connor, S. Skull base imaging, anatomy, pathology and protocols. Pract. Neurol. 2020, 20, 39–49. [Google Scholar] [CrossRef] [PubMed]
- Chapman, P.R.; Bag, A.K.; Tubbs, R.S.; Gohlke, P. Practical anatomy of the central skull base region. Semin. Ultrasound CT MR 2013, 34, 381–392. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.; Paul, R.; Liao, X.; Doulgeris, J.; Menzer, E.L.; Dhar, U.K.; Tsai, C.-T.; Vrionis, F.D. A New Method to Evaluate Pressure Distribution Using a 3D-Printed C2-C3 Cervical Spine Model with an Embedded Sensor Array. Sensors 2023, 23, 9547. [Google Scholar] [CrossRef]
- Ramirez, M.E.; Pena, I.R.; Castillo, R.E.B.; Sufianov, A.; Goncharov, E.; Sanchez, J.A.S.; Colome-Hidalgo, M.; Nurmukhametov, R.; Céspedes, J.R.C.; Montemurro, N. Development of a 3D printed brain model with vasculature for neurosurgical procedure visualisation and training. Biomedicines 2023, 11, 330. [Google Scholar]
- Uhl, J.F.; Sufianov, A.; Ruiz, C.; Iakimov, Y.; Mogorron, H.J.; Encarnacion Ramirez, M.; Prat, G.; Lorea, B.; Baldoncini, M.; Goncharov, E.; et al. The use of 3D printed models for surgical simulation of cranioplasty in craniosynostosis as training and education. Brain Sci. 2023, 13, 894. [Google Scholar] [CrossRef]
- Karamian, B.A.; Schroeder, G.D.; Lambrechts, M.J.; Canseco, J.A.; Oner, C.; Vialle, E.; Rajasekaran, S.; Dvorak, M.R.; Benneker, L.M.; Kandziora, F.; et al. An international validation of the AO spine subaxial injury classification system. Eur. Spine J. 2023, 32, 46–54. [Google Scholar] [CrossRef]
- Montemurro, N.; Cocciaro, A.; Liberti, G.; Cosottini, M.; Perrini, P. The internal trabecular bone structure of the odontoid process of the axis. A retrospective single-center comparative study in patients following cervical trauma. J. Neurol. Surg. A Cent. Eur. Neurosurg. 2022, 25, 1. [Google Scholar] [CrossRef] [PubMed]
- Baker, J.F.; Shafqat, A.; Devitt, A.; McCabe, J.P. Stabilization of metastatic lesions affecting the second cervical vertebra. J. Craniovertebral Junction Spine 2015, 6, 56–59. [Google Scholar] [CrossRef] [PubMed]
- Sen, C.; Shrivastava, R.; Anwar, S.; Triana, A. Lateral transcondylar approach for tumors at the anterior aspect of the craniovertebral junction. Neurosurgery 2010, 66, 104–112. [Google Scholar] [CrossRef]
- Rossmann, T.; Veldeman, M.; Nurminen, V.; Lehecka, M. How I do it: Lateral approach for craniocervical junction tumors. Acta Neurochir. 2023, 165, 1315–1322. [Google Scholar] [CrossRef]
- Mertens, K.; Vanhoenacker, F.M. Imaging of the Craniocervical Junction: A Pictorial Review. Semin. Musculoskelet. Radiol. 2023, 27, 499–511. [Google Scholar] [CrossRef] [PubMed]
- Goel, A.; Karapurkar, A.P. Transoral plate and screw fixation of the craniovertebral region—A preliminary report. Br. J. Neurosurg. 1994, 8, 743–745. [Google Scholar] [CrossRef]
- Goel, A. Progressive basilar invagination after transoral odontoidectomy: Treatment by atlantoaxial facet distraction and craniovertebral realignment. Spine 2005, 30, E551–E555. [Google Scholar] [CrossRef]
- Ahsan, F.; Inglis, T.; Allison, R.; Inglis, G.S. Cervical chordoma managed with multidisciplinary surgical approach. ANZ J. Surg. 2011, 81, 331–335. [Google Scholar] [CrossRef]
- Wewel, J.T.; Nunna, R.S.; Tan, L.A.; Kasliwal, M.K.; O’Toole, J.E. Novel reconstruction of the anterior craniocervical junction using an expandable cage with integrated fixation after total C2 spondylectomy for chordoma. J. Clin. Neurosci. 2016, 30, 157–160. [Google Scholar] [CrossRef]
- Sundaresan, N.; Galicich, J.H.; Lane, J.M.; Greenberg, H.S. Treatment of odontoid fractures in cancer patients. J. Neurosurg. 1981, 54, 187–192. [Google Scholar] [CrossRef]
- Yang, J.; Jia, Q.; Peng, D.; Wan, W.; Zhong, N.; Lou, Y.; Cai, X.; Wu, Z.; Zhao, C.; Yang, X.; et al. Surgical treatment of upper cervical spine metastases: A retrospective study of 39 cases. World J. Surg. Oncol. 2017, 15, 21. [Google Scholar] [CrossRef] [PubMed]
- Das, S.; Montemurro, N.; Ashfaq, M.; Ghosh, D.; Sarker, A.C.; Khan, A.H.; Dey, S.; Chaurasia, B. Resolution of Papilledema Following Ventriculoperitoneal Shunt or Endoscopic Third Ventriculostomy for Obstructive Hydrocephalus: A Pilot Study. Medicina 2022, 58, 281. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Toyama, Y.; Suzuki, N.; Fujimura, Y. Metastases to the upper cervical spine. J. Spinal Disord. 1996, 9, 195–201. [Google Scholar] [CrossRef]
- Lizana, J.; Reinoso, C.M.D.; Aliaga, N.; Marani, W.; Montemurro, N. Bilateral central retinal artery occlusion: An exceptional complication after frontal parasagittal meningioma resection. Surg. Neurol. Int. 2021, 12, 397. [Google Scholar] [CrossRef]
- Passeri, T.; Champagne, P.O.; Giammattei, L.; Abbritti, R.; Cartailler, J.; Calugaru, V.; Feuvret, L.; Guichard, J.P.; Polivka, M.; Adle-Biassette, H.; et al. Management strategies in clival and craniovertebral junction chordomas: A 29-year experience. J. Neurosurg. 2022, 138, 1640–1652. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Li, M.; Xu, W.; Wang, X.; Feng, M.; Wang, R.; Liu, X. Surgical Outcomes of Clival Chordoma Through Endoscopic Endonasal Approach: A Single-Center Experience. Front. Endocrinol. 2022, 13, 800923. [Google Scholar] [CrossRef] [PubMed]
- Aquino, A.A.; Ramirez, M.d.J.E.; Bozkurt, I.; González, J.A.A.; Goncharov, E.; Caballero, A.D.; Nurmukhametov, R.; Montemurro, N.; Chaurasia, B. Treatment of Intracranial Tumors with Stereotactic Radiosurgery: Short-Term Results from Cuba. Cureus 2022, 14, e29955. [Google Scholar]
- Tamaki, N.; Nagashima, T.; Ehara, K.; Motooka, Y.; Barua, K.K. Surgical approaches and strategies for skull base chordomas. Neurosurg. Focus 2001, 10, E9. [Google Scholar] [CrossRef]
- Dassoulas, K.; Schlesinger, D.; Yen, C.P.; Sheehan, J. The role of Gamma Knife surgery in the treatment of skull base chordomas. J. Neurooncol. 2009, 94, 243–248. [Google Scholar] [CrossRef]
- Martin, J.J.; Niranjan, A.; Kondziolka, D.; Flickinger, J.C.; Lozanne, K.A.; Lunsford, L.D. Radiosurgery for chordomas and chondrosarcomas of the skull base. J. Neurosurg. 2007, 107, 758–764. [Google Scholar] [CrossRef]
- Muthukumar, N.; Kondziolka, D.; Lunsford, L.D.; Flickinger, J.C. Stereotactic radiosurgery for chordoma and chondrosarcoma: Further experiences. Int. J. Radiat. Oncol. Biol. Phys. 1998, 41, 387–392. [Google Scholar] [CrossRef]
- Napieralska, A.; Blamek, S. Intracranial chordoma: Radiosurgery, hypofractionated stereotactic radiotherapy and treatment outcomes. Rep. Pract. Oncol. Radiother. 2021, 26, 764–772. [Google Scholar] [CrossRef]
- Koga, T.; Shin, M.; Saito, N. Treatment with high marginal dose is mandatory to achieve long-term control of skull base chordomas and chondrosarcomas by means of stereotactic radiosurgery. J. Neurooncol. 2010, 98, 233–238. [Google Scholar] [CrossRef]
- Liu, J.K.; Rosenberg, W.S.; Schmidt, M.H. Titanium cage-assisted polymethylmethacrylate reconstruction for cervical spinal metastasis: Technical note. Neurosurgery 2005, 56, E207. [Google Scholar] [CrossRef]
- Islam, M.A.; Afreen, M.S.; Montemurro, N.; Chaurasia, B. Surgical Approach for Spinal Tumors: Our Experience in Combined Military Hospital Dhaka. Surgeries 2021, 2, 303–307. [Google Scholar] [CrossRef]
- Zhang, Y.; Ai, F.; Fu, S.; Li, K.; Xia, H.; Wu, Z.; Ma, X. An application of posterior cervical and transoral approaches to treating primary malignant osseous tumors in craniovertebral junction. Chin. J. Reparative Reconstr. Surg. 2020, 34, 1149–1157. [Google Scholar]
- Peron, S.; Rusconi, A.; Minotti, M.; Stefini, R. High definition 4K-three-dimensional exoscope for removal of a C1-C2 meningioma: Technical case report. Neurocirugía 2022, 34, 48–52. [Google Scholar] [CrossRef]
- Eco, L.C.; Brayton, A.; Whitehead, W.E.; Jea, A. Reconstruction of the anterior craniocervical junction using an expandable cage after resection of a C1 chordoma in a 5-year-old child: Case report. J. Neurosurg. Pediatr. 2019, 24, 62–65. [Google Scholar] [CrossRef] [PubMed]
- Fehlings, M.G.; David, K.S.; Vialle, L.; Vialle, E.; Setzer, M.; Vrionis, F.D. Decision Making in the Surgical Treatment of Cervical Spine Metastases. Spine 2009, 34, S108–S117. [Google Scholar] [CrossRef]
- Ramirez, M.D.J.E.; Peralta, I.; Ramirez, I.; Dauly, V.; Mainer, G.; Nurmukhametov, R.; Efe, I.E. Development of a novel low-cost exoscope to expand access to microneurosurgical care in low-and middle-income countries. World Neurosurg. 2022, 163, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Montemurro, N.; Scerrati, A.; Ricciardi, L.; Trevisi, G. The Exoscope in Neurosurgery: An Overview of the Current Literature of Intraoperative Use in Brain and Spine Surgery. J. Clin. Med. 2021, 11, 223. [Google Scholar] [CrossRef] [PubMed]
- Encarnacion Ramirez, M.; Peralta Baez, I.; Nurmukhametov, R.; Goncharov, E.; Efe, I.E.; Sufianov, A.; Ramirez Pena, I. Comparative survey study of the use of a low cost exoscope vs. microscope for anterior cervical discectomy and fusion (ACDF). Front. Med. Technol. 2022, 4, 1055189. [Google Scholar] [CrossRef]
- Montemurro, N.; Condino, S.; Carbone, M.; Cattari, N.; D’amato, R.; Cutolo, F.; Ferrari, V. Brain Tumor and Augmented Reality: New Technologies for the Future. Int. J. Environ. Res. Public Health 2022, 19, 6347. [Google Scholar] [CrossRef] [PubMed]
- Montemurro, N. Telemedicine: Could it represent a new problem for spine surgeons to solve? Glob. Spine J. 2022, 12, 1306–1307. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Age/ Sex | Comorbidities | Tumor Localization | Histology | SINS (pts) | Preop. Karnofsky | Postop. Karnofsky | Resection | DEH | Surgical Approach |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 59/M | Epilepsy | C2–C4 | Adenocarcinoma (prostate) | 12 | 60% | 80% | Total | 4 | Ant. |
| 2 | 68/M | N/A | C2 | Chordoma | 14 | 50% | 75% | Total | 4 | Post. */ Ant. |
| 3 | 68/F | Art. hypertension | C2 | Chordoma | 15 | 55% | 85% | Total | 15 | Post./ Ant. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reyes-Soto, G.; Corona De la Torre, A.; Honda Partida, K.G.; Nurmukhametov, R.; Encarnacion Ramirez, M.D.J.; Montemurro, N. Clivus-Cervical Stabilization through Transoral Approach in Patients with Craniocervical Tumor: Three Cases and Surgical Technical Note. Brain Sci. 2024, 14, 254. https://doi.org/10.3390/brainsci14030254
Reyes-Soto G, Corona De la Torre A, Honda Partida KG, Nurmukhametov R, Encarnacion Ramirez MDJ, Montemurro N. Clivus-Cervical Stabilization through Transoral Approach in Patients with Craniocervical Tumor: Three Cases and Surgical Technical Note. Brain Sciences. 2024; 14(3):254. https://doi.org/10.3390/brainsci14030254
Chicago/Turabian StyleReyes-Soto, Gervith, Alfonso Corona De la Torre, Kaori Guadalupe Honda Partida, Renat Nurmukhametov, Manuel De Jesus Encarnacion Ramirez, and Nicola Montemurro. 2024. "Clivus-Cervical Stabilization through Transoral Approach in Patients with Craniocervical Tumor: Three Cases and Surgical Technical Note" Brain Sciences 14, no. 3: 254. https://doi.org/10.3390/brainsci14030254