
Determinants of the Quality of Life in Patients with Drug-Resistant Temporal Lobe Epilepsy: A Comparison of the Results before and after Surgery
 , ,
, ,
Abstract
:1. Introduction
2. Methods
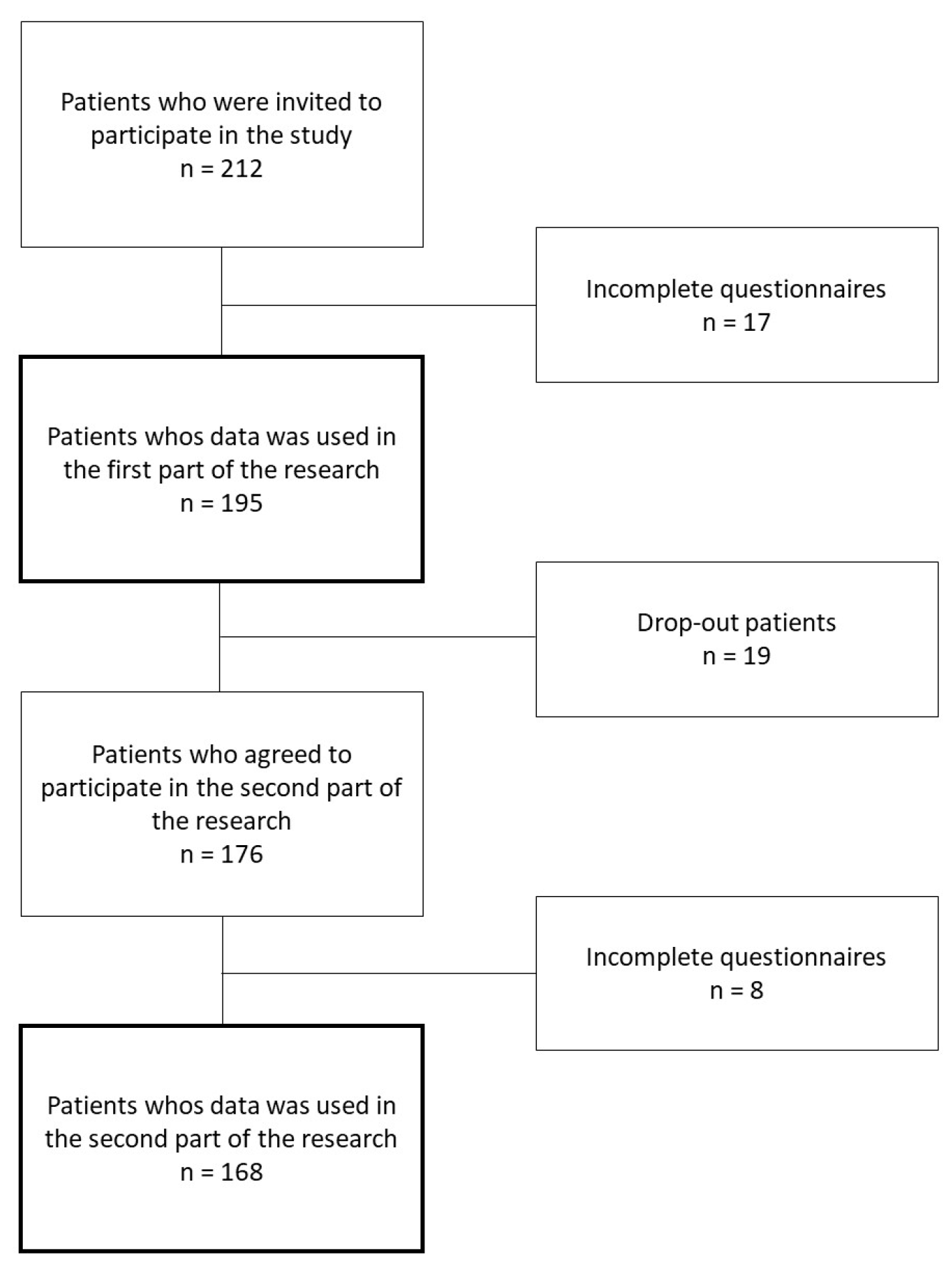
2.1. Participants
2.2. Procedure
2.3. Assessment Tools
- (a)
- Quality of Life in Epilepsy Inventory-Patient-Weighted (QoLIE-31-P) [29] is a widely utilized questionnaire designed to assess the quality of life in adults with epilepsy. It comprises seven distinct scales that each address different aspects of an individual’s life: Emotional Well-Being, Social Functioning, Energy/Fatigue, Cognitive Functioning, Seizure Worry, Medication Effects, and Overall QoL. The cumulative scores from these seven scales provide an estimation of the overall QoL. Furthermore, the questionnaire includes two additional scales: the distress scale and an unscored overall health-level scale, both of which allow for a comprehensive evaluation of an individual’s well-being. Each subtest of the QoLIE-31-P allows respondents to accrue between 0 to 100 points, with higher scores indicating a better QoL. It is noteworthy that the authors of this study employed a validated Polish version of the QoLIE-31-P questionnaire.
- (b)
- The Hospital Anxiety and Depression Scale (HADS) [30] is a self-reporting questionnaire designed to assess and measure symptoms of anxiety and depression in individuals who are receiving medical treatment but do not have a formal diagnosis of a psychiatric disorder. The HADS is widely used in healthcare settings to screen for and evaluate the emotional well-being of patients, particularly those with physical health conditions. It consists of 14 questions, with 7 questions dedicated to assessing symptoms of anxiety and 7 questions for assessing symptoms of depression. These questions are designed to be simple and straightforward, making them easily understandable for a wide range of individuals. For each section (anxiety and depression), a score of 0–7 is considered “normal” or indicative of no or minimal symptoms, scores between 8 and 10 suggest the presence of mild symptoms, scores between 11 and 14 are indicative of moderate symptoms, and scores above 14 may indicate severe symptoms.
2.4. Statistical Analyses
3. Results
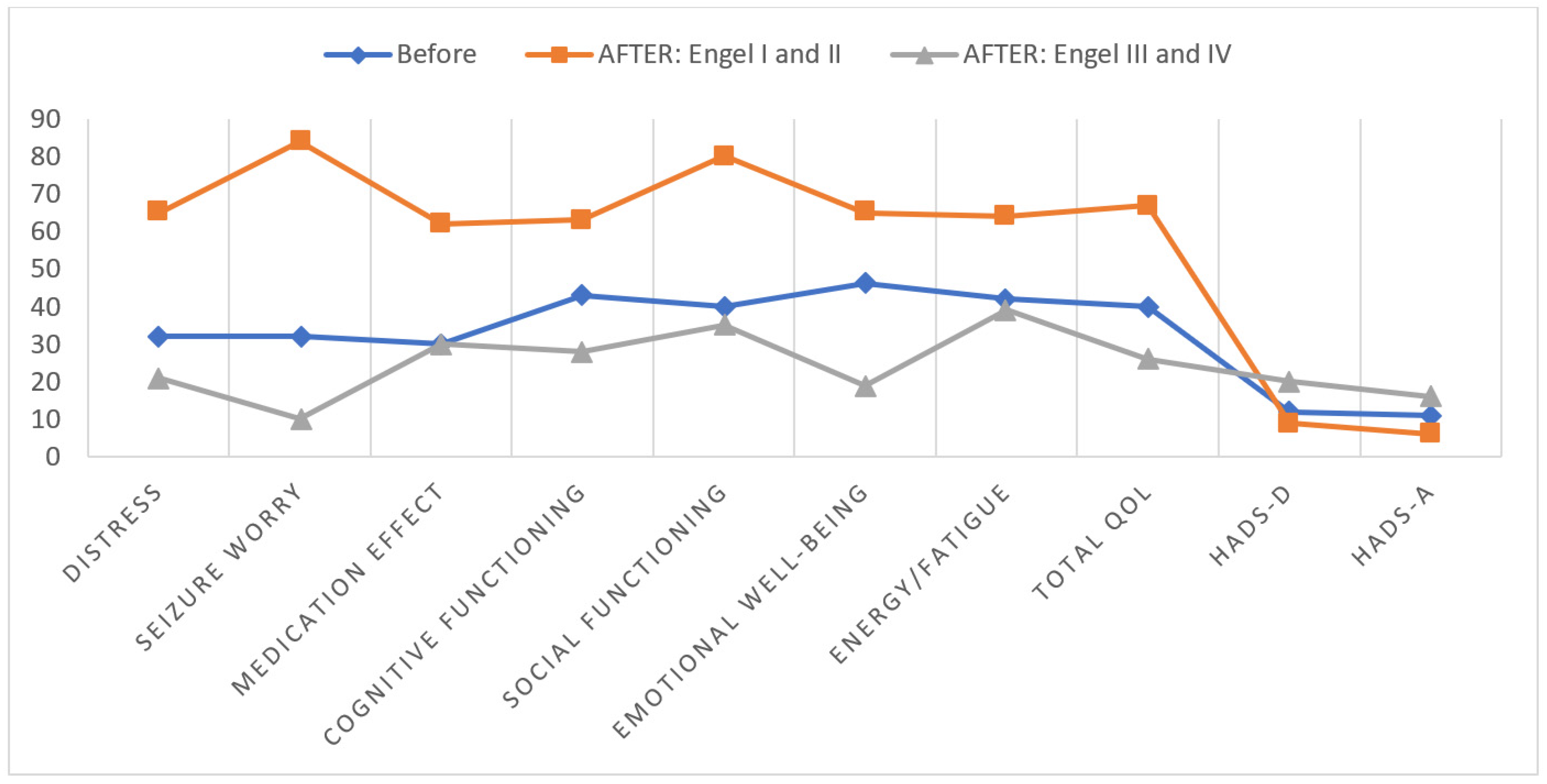
3.1. Differences in QoL and Emotional State in Patients with Good and Unfavorable Treatment Outcomes
3.2. Correlation between QoL and Other Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Beghi, E. The Epidemiology of Epilepsy. Neuroepidemiology 2019, 54, 185–191. [Google Scholar] [CrossRef]
- Chen, Y.; Huang, S.; Wu, W.; Liu, C.; Yang, X.; Zhao, H.; Wu, L.; Tan, L.; Long, L.; Xiao, B. Associated and predictive factors of quality of life in patients with temporal lobe epilepsy. Epilepsy Behav. 2018, 86, 85–90. [Google Scholar] [CrossRef]
- Fiest, K.M.; Birbeck, G.L.; Jacoby, A.; Jette, N. Stigma in epilepsy. Curr. Neurol. Neurosci. Rep. 2014, 14, 444. [Google Scholar] [CrossRef] [PubMed]
- Fiest, K.M.; Sauro, K.M.; Wiebe, S.; Patten, S.B.; Kwon, C.S.; Dykeman, J.; Pringsheim, T.; Lorenzetti, D.L.; Jetté, N. Prevalence and incidence of epilepsy: A systematic review and meta-analysis of international studies. Neurology 2017, 88, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Fisher, R.S.; Boas, W.v.E.; Blume, W.; Elger, C.; Genton, P.; Lee, P.; Engel, J.J. Epileptic Seizures and Epilepsy: Definitions Proposed by the International League Against Epilepsy (ILAE) and the International Bureau for Epilepsy (IBE). Epilepsia 2005, 46, 470–472. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Linera, J. Temporal Lobe Epilepsy (TLE) and Neuroimaging. In Clinical Neuroradiology; Barkhof, F., Jäger, H., Thurnher, M., Rovira, À., Eds.; Springer: Cham, Switzerland, 2019; pp. 891–914. [Google Scholar]
- Gaitatzis, A.; Trimble, M.E.; Sander, J.W. The psychiatric comorbidity of epilepsy. Acta Neurol. Scand. 2004, 110, 207–220. [Google Scholar] [CrossRef]
- Allone, C.; Buono, V.L.; Corallo, F.; Pisani, L.R.; Pollicino, P.; Bramanti, P.; Marino, S. Neuroimaging and cognitive functions in temporal lobe epilepsy: A review of the literature. J. Neurol. Sci. 2017, 381, 7–15. [Google Scholar] [CrossRef]
- Bala, A.; Okruszek, Ł.; Piejka, A.; Głębicka, A.; Szewczyk, E.; Bosak, K.; Szantroch, M.; Hyniewska, S.; Rysz, A.; Marchel, A. Social Perception in Mesial Temporal Lobe Epilepsy: Interpreting Social Information From Moving Shapes and Biological Motion. J. Neuropsychiatry Clin. Neurosci. 2018, 30, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Bell, B.; Lin, J.J.; Seidenberg, M.; Hermann, B. The neurobiology of cognitive disorders in temporal lobe epilepsy. Nat. Rev. Neurol. 2011, 7, 154–164. [Google Scholar] [CrossRef]
- Olejnik, A.; Bala, A.; Dziedzic, T.; Rysz, A.; Marchel, A.; Kunert, P. Executive dysfunction profile in mesial temporal lobe epilepsy. Acta Neuropsychol. 2024, 22, 1–13. [Google Scholar] [CrossRef]
- Wang, W.; Shih, Y.; Yu, H.; Yen, D.; Lin, Y.; Kwan, S.; Chen, C.; Hua, M. Theory of mind and social functioning in patients with temporal lobe epilepsy. Epilepsia 2015, 56, 1117–1123. [Google Scholar] [CrossRef] [PubMed]
- Tanriverdi, T.; Olivier, N.P.; Olivier, A. Quality of life after extratemporal epilepsy surgery: A prospective clinical study. Clin. Neurol. Neurosurg. 2008, 110, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Mohan, M.; Keller, S.; Nicolson, A.; Biswas, S.; Smith, D.; Osman Farah, J.; Eldridge, P.; Wieshmann, U. The long-term outcomes of epilepsy surgery. PLoS ONE 2018, 13, 5. [Google Scholar] [CrossRef]
- Loring, D.W.; Meador, K.J.; Lee, G.P. Determinants of quality of life in epilepsy. Epilepsy Behav. 2004, 5, 976–980. [Google Scholar] [CrossRef] [PubMed]
- Suurmeijer, T.P.; Reuvekamp, M.F.; Aldenkamp, B.P. Social functioning, psychological functioning, and quality of life in epilepsy. Epilepsia 2001, 42, 1160–1168. [Google Scholar] [CrossRef]
- Harden, C.L.; Maroof, D.A.; Nikolov, B.; Fowler, K.; Sperling, M.; Liporace, J.; Pennell, P.; Labar, D.; Herzog, A. The effect of seizure severity on quality of life in epilepsy. Epilepsy Behav. 2007, 11, 208–211. [Google Scholar] [CrossRef]
- Johnson, E.K.; Jones, J.E.; Seidenberg, M.; Hermann, B.P. The relative impact of anxiety, depression, and clinical seizure features on health-related quality of life in epilepsy. Epilepsia 2004, 45, 544–550. [Google Scholar] [CrossRef]
- Salgado, P.C.B.; Cendes, F. The effects of epileptic seizures upon quality of life. J. Epilepsy Clin. Neurophysiol. 2009, 15, 110–113. [Google Scholar] [CrossRef]
- Choi-Kwon, S.; Chung, C.; Kim, H.; Lee, S.; Yoon, S.; Kho, H.; Oh, J.; Lee, S. Factors affecting the quality of life in patients with epilepsy in Seoul, South Korea. Acta Neurol. Scand. 2003, 108, 428–434. [Google Scholar] [CrossRef]
- Alanis-Guevara, I.; Peña, E.; Corona, T.; López-Ayala, T.; López-Meza, E.; López-Gómez, M. Sleep disturbances, socioeconomic status, and seizure control as main predictors of quality of life in epilepsy. Epilepsy Behav. 2005, 7, 481–485. [Google Scholar] [CrossRef]
- Baker, G.A.; Jacoby, A.; Buck, D.; Stalgis, C.; Monnet, D. Quality of life of people with epilepsy: A European study. Epilepsia 1997, 38, 353–362. [Google Scholar] [CrossRef]
- Szaflarski, M.; Meckler, J.M.; Privitera, M.D.; Szaflarski, J.P. Quality of life in medication-resistant epilepsy: The effects of patient’s age, age at seizure onset, and disease duration. Epilepsy Behav. 2006, 8, 547–551. [Google Scholar] [CrossRef] [PubMed]
- Schachter, S.C. Improving quality of life beyond seizure control. Epileptic. Disord. 2005, 7 (Suppl. S1), S34–S38. [Google Scholar] [PubMed]
- Benevides, M.L.; Costa Nunes, J.; Guarnieri, R.; Pauli, C.; Wolf, P.; Lunardi, M.; Kondageski, C.; Neves Linhares, M.; Lin, K.; Walz, R. Quality of life long after temporal lobe epilepsy surgery. Acta Neurol. Scand. 2021, 143, 629–636. [Google Scholar] [CrossRef] [PubMed]
- Pauli, C.; Schwarzbold, M.L.; Diaz, A.P.; Rodrigues de Oliveira Thais, M.E.; Kondageski, C.; Linhares, M.N.; Guarnieri, R.; de Lemos Zingano, B.; Ben, J.; Nunes, J.C.; et al. Predictors of meaningful improvement in quality of life after temporal lobe epilepsy surgery: A prospective study. Epilepsia 2017, 58, 755–763. [Google Scholar] [CrossRef] [PubMed]
- Arifin, M.T.; Ashari, A.; Brilliantika, S.P.; Bunyamin, J.; Hardian, H.; Brotoarianto, H.K.; Fitrikasari, A.; Muttaqin, Z. Seizure free status as a good predictor for quality of life of temporal lobe epilepsy patients after amygdalohippocampectomy. Bali. Med. J. 2020, 9, 855–858. [Google Scholar] [CrossRef]
- Elsharkawy, A.E.; May, T.; Thorbecke, R.; Koch-Stoecker, S.; Villagran, A.; Urak, L.; Pfäfflin, M.; Pannek, H.; Pietilä, T.A.; Ebner, A. Long-term outcome and determinants of quality of life after temporal lobe epilepsy surgery in adults. Epilepsy Res. 2009, 86, 191–199. [Google Scholar] [CrossRef]
- Cramer, J.A.; Perrine, K.; Devinsky, O.; Bryant-Comstock, L.; Meador, K.; Hermann, B. Development and cross-cultural translations of a 31-item quality of life in epilepsy inventory. Epilepsia 1998, 39, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Engel, J., Jr.; Van Ness, P.C.; Rasmussen, T.B.; Ojemann, L.M. Outcome with respect to epileptic seizures. In Surgical Treatment of the Epilepsies; Engel, J., Jr., Ed.; Raven Press: New York, NY, USA, 1993; pp. 609–621. [Google Scholar]
- Cao, Z.; Guo, M.; Cao, X.; Liu, T.; Hu, S.; Xiao, Y.; Zhang, M.; Liu, H. Progress in TLE treatment from 2003 to 2023: Scientific measurement and visual analysis based on CiteSpace. Front. Neurol. 2023, 14, 1223457. [Google Scholar] [CrossRef]
- Vinti, V.; Dell’Isola, G.B.; Tascini, G.; Mencaroni, E.; Cara, G.D.; Striano, P.; Verrotti, A. Temporal Lobe Epilepsy and Psychiatric Comorbidity. Front. Neurol. 2021, 12, 775781. [Google Scholar] [CrossRef]
- Celiker Uslu, S.; Yuksel, B.; Tekin, B.; Sariahmetoglu, H.; Atakli, D. Cognitive impairment and drug responsiveness in mesial temporal lobe epilepsy. Epilepsy Behav. 2019, 90, 162–167. [Google Scholar] [CrossRef]
- Giovagnoli, A.R.; Parente, A.; Ciuffini, R.; Tallarita, G.M.; Turner, K.; Maialetti, A.; Marrelli, A.M.; Pucci, B. Diversified social cognition in temporal lobe epilepsy. Acta Neurol. Scand. 2021, 143, 396–406. [Google Scholar] [CrossRef] [PubMed]
- Filho, G.M.; Rosa, V.P.; Lin, K.; Caboclo, L.O.; Sakamoto, A.C.; Yacubian, E.M. Psychiatric comorbidity in epilepsy: A study comparing patients with mesial temporal sclerosis and juvenile myoclonic epilepsy. Epilepsy Behav. 2008, 13, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Kanner, A.M. Mood disorder and epilepsy: A neurobiologic perspective of their relationship. Dialogues Clin. Neurosci. 2008, 10, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Au, A.; Li, P.; Chan, J.; Lui, C.; Ng, P.; Kwok, A.; Leung, P. Predicting the quality of life in Hong Kong Chinese adults with epilepsy. Epilepsy Behav. 2002, 3, 350–357. [Google Scholar] [CrossRef] [PubMed]
- Devinsky, O.; Barr, W.B.; Vickrey, B.G.; Berg, A.T.; Bazil, C.W.; Pacia, S.V.; Langfitt, J.T.; Walczak, T.S.; Sperling, M.R.; Shinnar, S.; et al. Changes in depression and anxiety after resective surgery for epilepsy. Neurology 2005, 65, 1744–1749. [Google Scholar] [CrossRef] [PubMed]
- Derry, P.A.; Rose, K.J.; McLachlan, R.S. Moderators of the effect of preoperative emotional adjustment on postoperative depression after surgery for temporal lobe epilepsy. Epilepsia 2000, 41, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Wrench, J.M.; Rayner, G.; Wilson, S.J. Profiling the evolution of depression after epilepsy surgery. Epilepsia 2011, 52, 900–908. [Google Scholar] [CrossRef] [PubMed]
- Siebenbrodt, K.; Willems, L.M.; von Podewils, F.; Mross, P.M.; Strüber, M.; Langenbruch, L.; Bierhansl, L.; Gorny, I.; Schulz, J.; Gaida, B.; et al. Determinants of quality of life in adults with epilepsy: A multicenter, cross-sectional study from Germany. Neurol. Res. Pract. 2023, 5, 41. [Google Scholar] [CrossRef]
- Luoni, C.; Bisulli, F.; Canevini, M.P.; De Sarro, G.; Fattore, C.; Galimberti, C.A.; Gatti, G.; La Neve, A.; Muscas, G.; Specchio, L.M.; et al. Determinants of health-related quality of life in pharmacoresistant epilepsy: Results from a large multicenter study of consecutively enrolled patients using validated quantitative assessments. Epilepsia 2011, 52, 2181–2191. [Google Scholar] [CrossRef]
- Meldolesi, G.N.; Di Gennaro, G.; Quarato, P.P.; Esposito, V.; Grammaldo, L.G.; Morosini, P.; Cascavilla, I.; Picardi, A. Changes in depression, anxiety, anger, and personality after resective surgery for drug-resistant temporal lobe epilepsy: A 2-year follow-up study. Epilepsy Res. 2007, 77, 22–30. [Google Scholar] [CrossRef]
- Edefonti, V.; Bravi, F.; Turner, K.; Beghi, E.; Canevini, M.P.; Ferraroni, M.; Piazzini, A. Health-related quality of life in adults with epilepsy: The effect of age, age at onset and duration of epilepsy in a multicentre Italian study. BMC Neurol. 2011, 11, 33. [Google Scholar] [CrossRef] [PubMed]
- Spencer, S.S.; Berg, A.T.; Vickrey, B.G.; Sperling, M.R.; Bazil, C.W.; Haut, S.; Langfitt, J.T.; Walczak, T.S.; Devinsky, O. Health-related quality of life over time since resective epilepsy surgery. Ann. Neurol. 2007, 62, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Punia, V.; Sheikh, S.R.; Thompson, N.R.; Bingaman, W.; Jehi, L. Quality of life before and after epilepsy surgery: Age is just a number. Epilepsy Behav. 2020, 113, 107574. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Before Surgery M (SD) | After Surgery M (SD) | Statistics | p Value | Cohen’s d | ||
|---|---|---|---|---|---|---|
| QOLIE-31-P | Distress | 34.3 (8.8) | 44.3 (7.4) | t = 1.23 | p = 0.007 | 0.61 |
| Seizures Worry | 35.7 (7.5) | 47.1 (6.9) | t = 2.01 | p = 0.002 | 0.72 | |
| Medication Effects | 33.2 (6.9) | 48.4 (5.3) | t = 3.98 | p = 0.004 | 0.65 | |
| Cognitive Functioning | 45.1 (7.1) | 47.8 (8.3) | t = 2.27 | p = 0.039 | 0.34 | |
| Social Functioning | 44.5 (5.2) | 54.6 (4.6) | t = 2.63 | p = 0.009 | 0.31 | |
| Emotional Well-Being | 48.4 (9.5) | 53.9 (6.9) | t = 3.12 | p = 0.021 | 0.25 | |
| Energy/Fatigue | 45.2 (3.6) | 53.2 (3.9) | t = 2.45 | p = 0.046 | 0.35 | |
| Total | 43.1 (7.9) | 49.4 (5.5) | t = 1.99 | p = 0.008 | 0.48 | |
| HADS | Depression | 15.1 (9.6) | 9.7 (7.3) | t = 3.12 | p = 0.045 | 0.46 |
| Anxiety | 13.6 (8.1) | 8.9 (6.9) | t = 2.57 | p = 0.039 | 0.51 |
| Post-Operative Group: Engel I and II n = 136 | Post-Operative Group: Engel III and IV n = 32 | p Value | |
|---|---|---|---|
| Age, M (SD) | 32.7 (13.6) | 34.3 (12.1) | p > 0.05 * |
| Sex, M/F | 57/79 | 13/19 | p > 0.05 ** |
| Years of formal education, M (SD) | 13.3 (3.1) | 13.2 (4.3) | p > 0.05 * |
| Epilepsy Focus, R/L | 70/66 | 17/15 | p > 0.05 ** |
| Age at epilepsy onset, M (SD) | 13.4 (9.1) | 12.1 (8.8) | p = 0.053 * |
| Seizures per month, M (SD) | 0.31 (0.1) | 6.41 (5.7) | p < 0.001 * |
| Extend of ATL resection, cm from temporal pole, M (SD) | 3.92 (1.4) | 4.01 (1.2) | p > 0.05 * |
| Histopathology: HS/HS-FCD | 89/47 | 12/20 | p < 0.01 ** |
| Treatment status: mono-/polytherapy | 5/131 | 1/28 | p > 0.05 ** |
| HADS-A | HADS-D | Seizures/Month | Epilepsy Onset | |
|---|---|---|---|---|
| QoL: Distress | r = −0.44; p < 0.05 | r = −0.48; p < 0.05 | r = −0.63; p < 0.001 | |
| QoL: Seizures Worry | r = −0.53; p < 0.01 | r = −0.46; p < 0.05 | r = −0.52; p < 0.01 | r = −0.43; p < 0.01 |
| QoL: Medication Effects | r = −0.38; p < 0.05 | |||
| QoL: Cognitive Functioning | r = −0.51; p < 0.05 | r = −0.41; p < 0.05 | r = 0.35; p < 0.05 | |
| QoL: Social Functioning | r = −0.66; p < 0.05 | r = −0.42; p < 0.05 | r = −0.42; p < 0.05 | r = −0.62; p < 0.01 |
| QoL: Emotional Well-Being | r = −0.39; p < 0.05 | r = −0.46; p < 0.01 | r = −0.71; p < 0.01 | |
| QoL: Energy/Fatigue | r = −0.72; p < 0.01 | r = −0.33; p < 0.05 | ||
| Total QoL | r = −0.31; p < 0.05 | r = −0.52; p < 0.05 | r = −0.44; p < 0.05 | r = −0.55; p < 0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bala, A.; Olejnik, A.; Kułak, M.; Rysz, A.; Dziedzic, T.; Nowak, A.; Marchel, A.; Kunert, P. Determinants of the Quality of Life in Patients with Drug-Resistant Temporal Lobe Epilepsy: A Comparison of the Results before and after Surgery. Brain Sci. 2024, 14, 241. https://doi.org/10.3390/brainsci14030241
Bala A, Olejnik A, Kułak M, Rysz A, Dziedzic T, Nowak A, Marchel A, Kunert P. Determinants of the Quality of Life in Patients with Drug-Resistant Temporal Lobe Epilepsy: A Comparison of the Results before and after Surgery. Brain Sciences. 2024; 14(3):241. https://doi.org/10.3390/brainsci14030241
Chicago/Turabian StyleBala, Aleksandra, Agnieszka Olejnik, Michał Kułak, Andrzej Rysz, Tomasz Dziedzic, Arkadiusz Nowak, Andrzej Marchel, and Przemysław Kunert. 2024. "Determinants of the Quality of Life in Patients with Drug-Resistant Temporal Lobe Epilepsy: A Comparison of the Results before and after Surgery" Brain Sciences 14, no. 3: 241. https://doi.org/10.3390/brainsci14030241