
Cortical Sensorimotor Integration as a Neural Origin of Impaired Grip Force Direction Control following Stroke

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
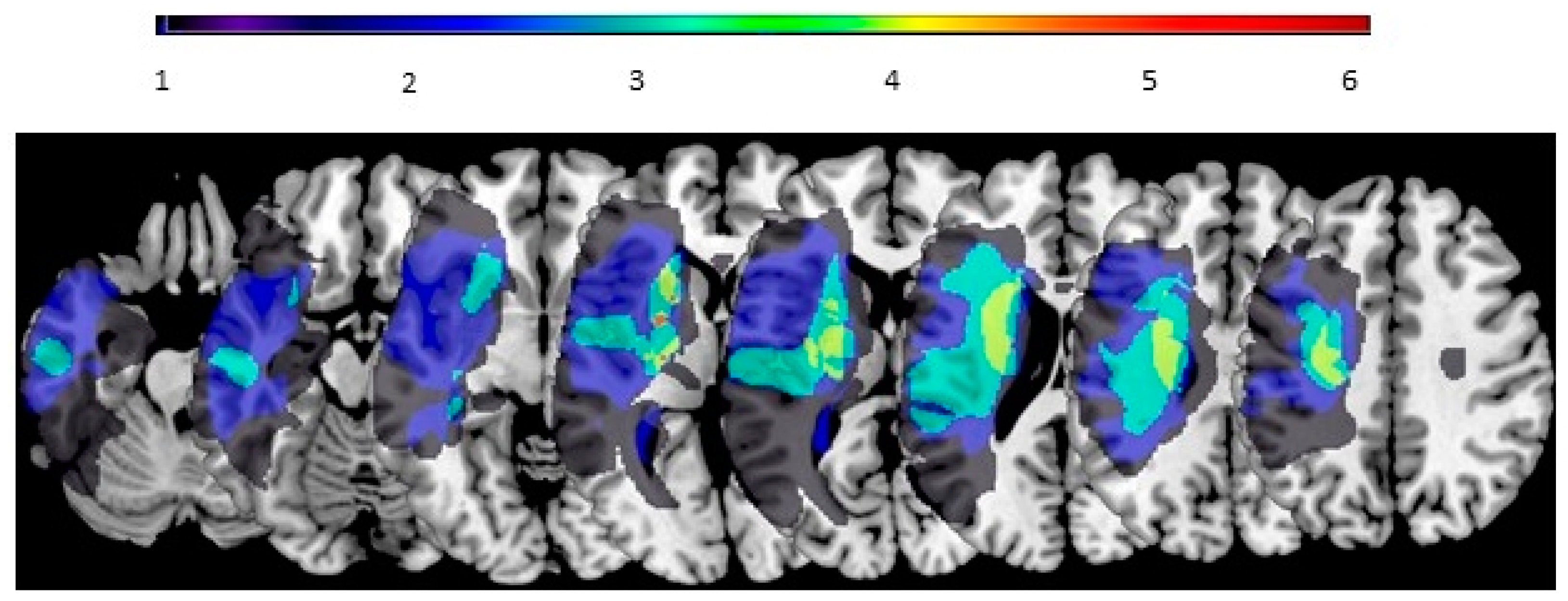
2.2. Brain MRI
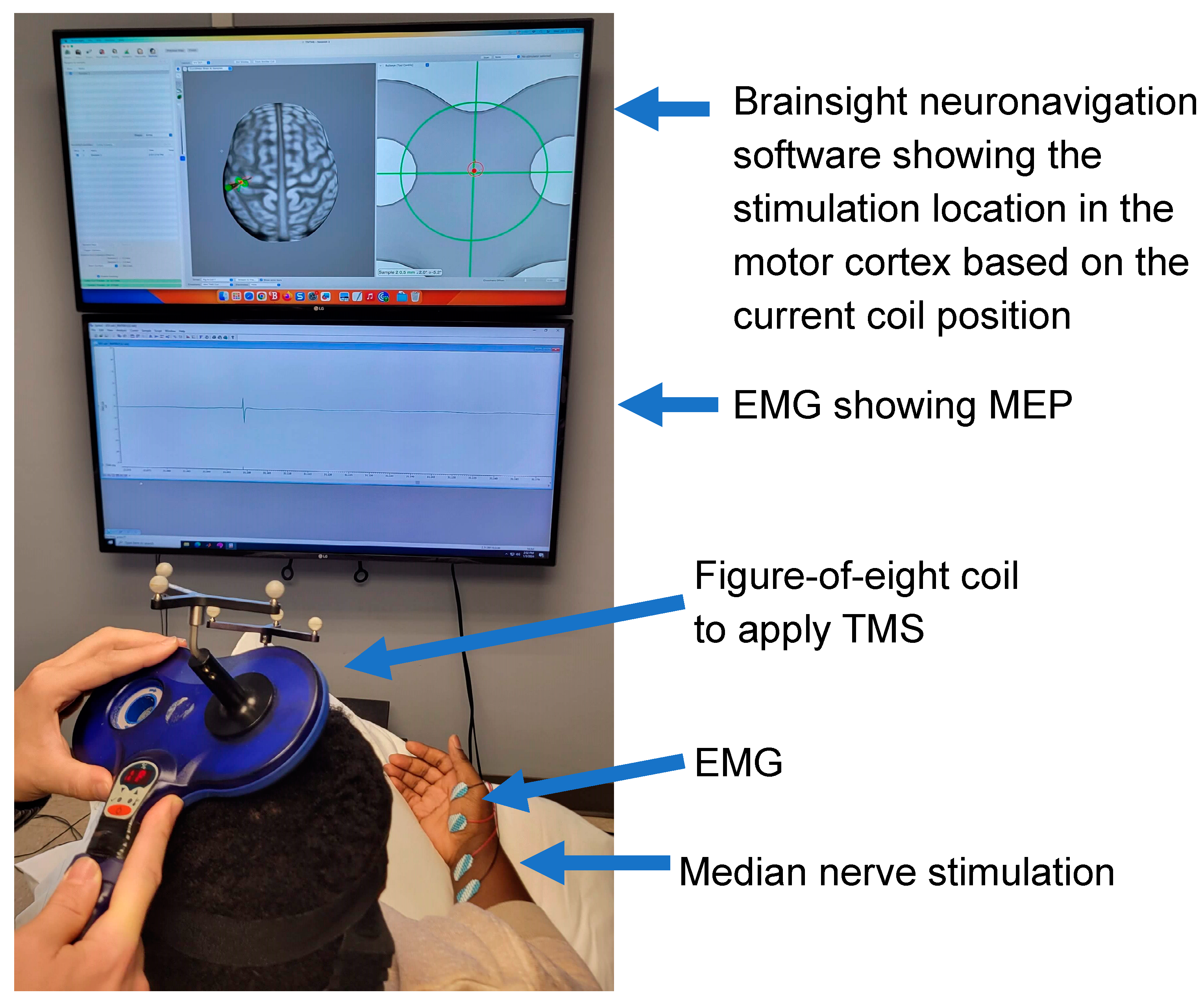
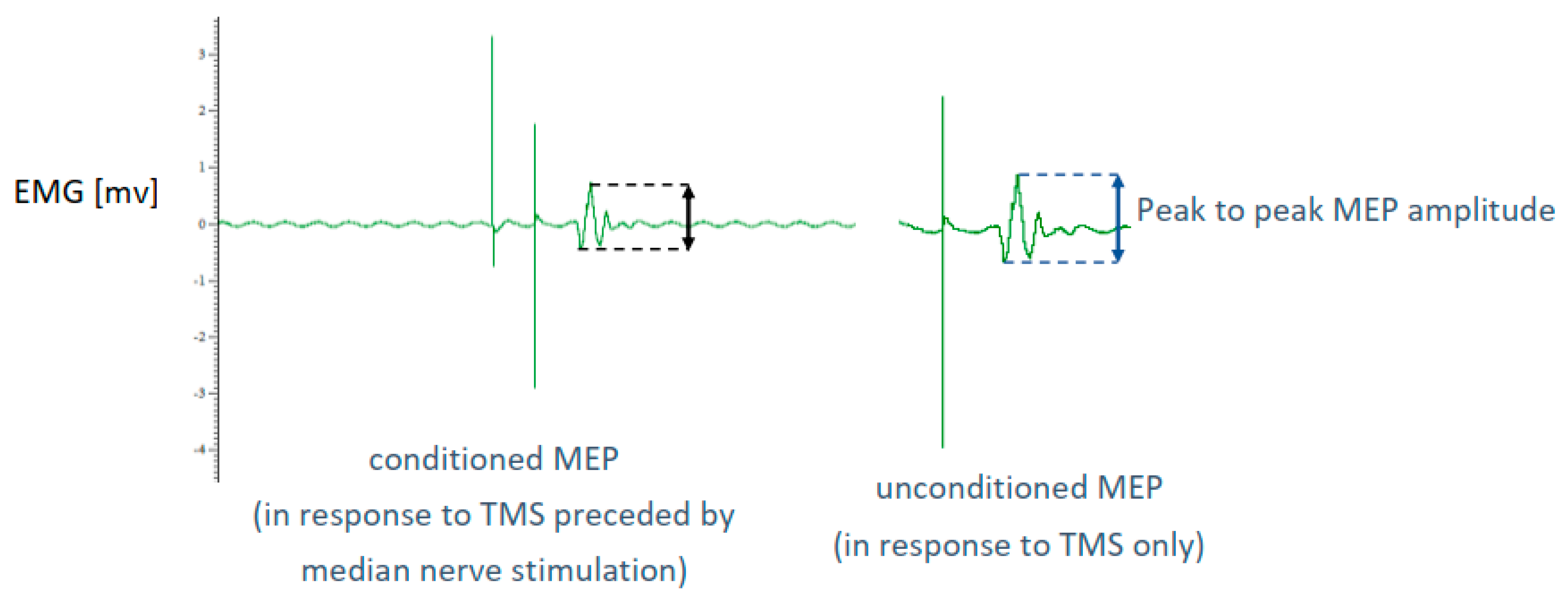
2.3. Short Latency Afferent Inhibition (SAI) Measures
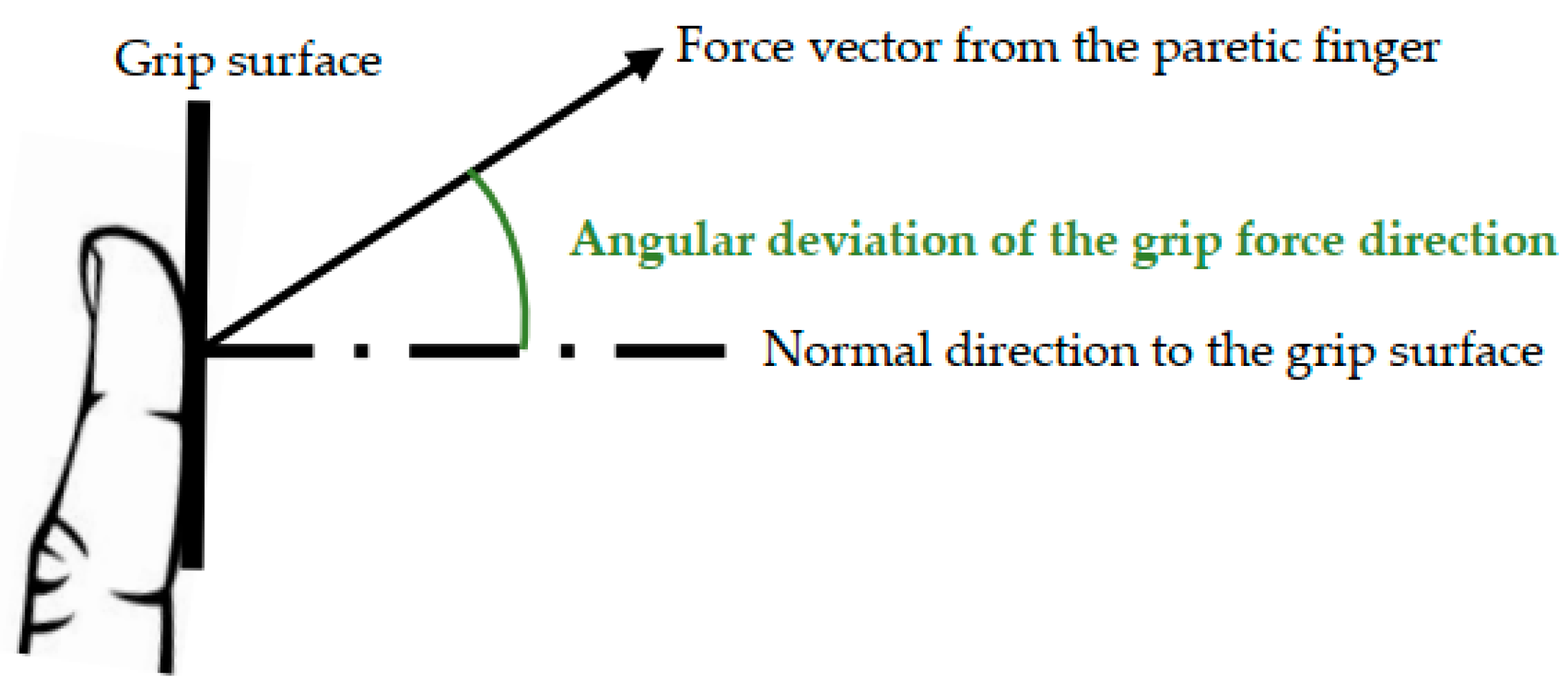
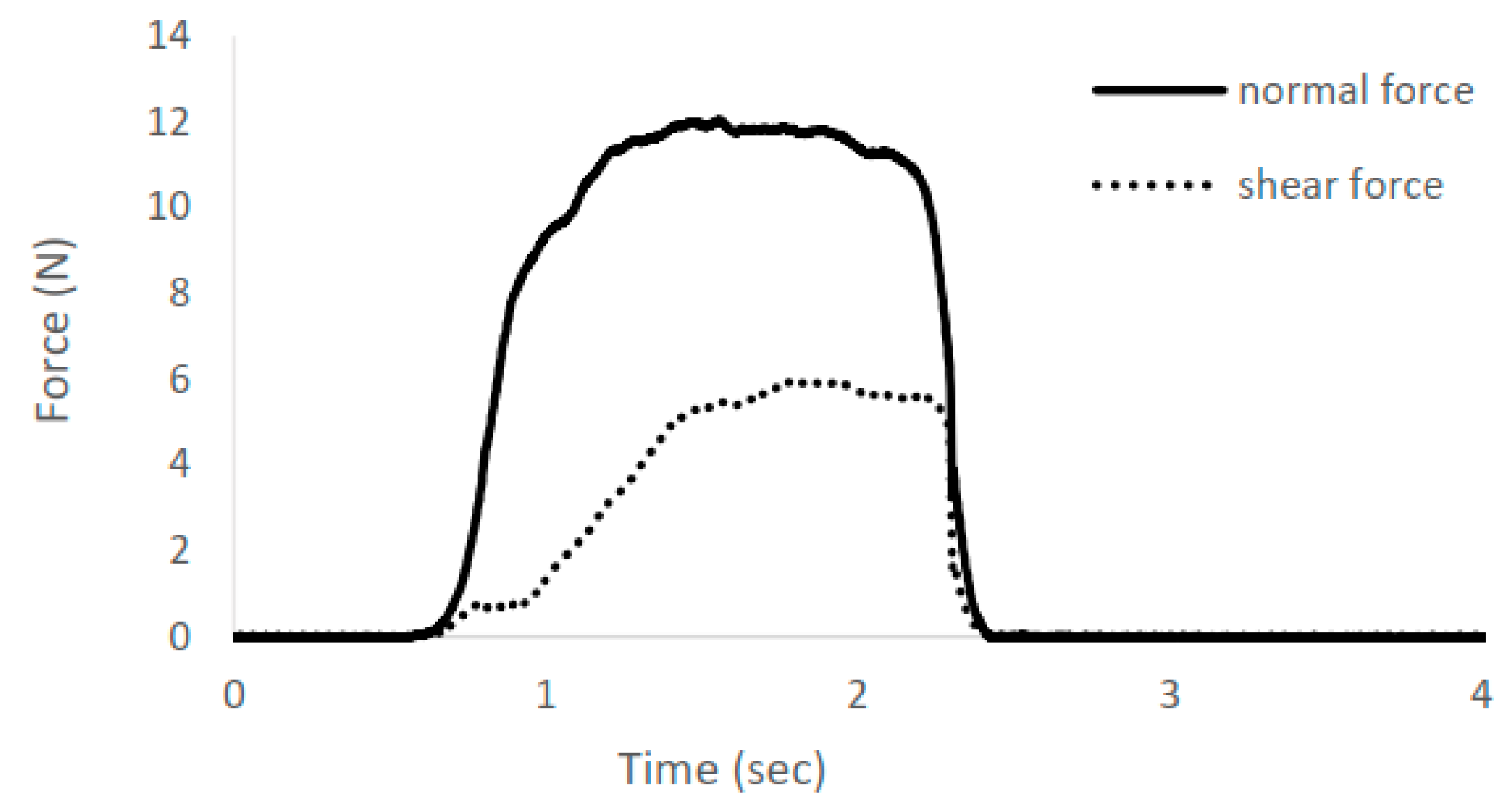
2.4. Grip Force Direction Control Measure
2.5. Statistical Analysis
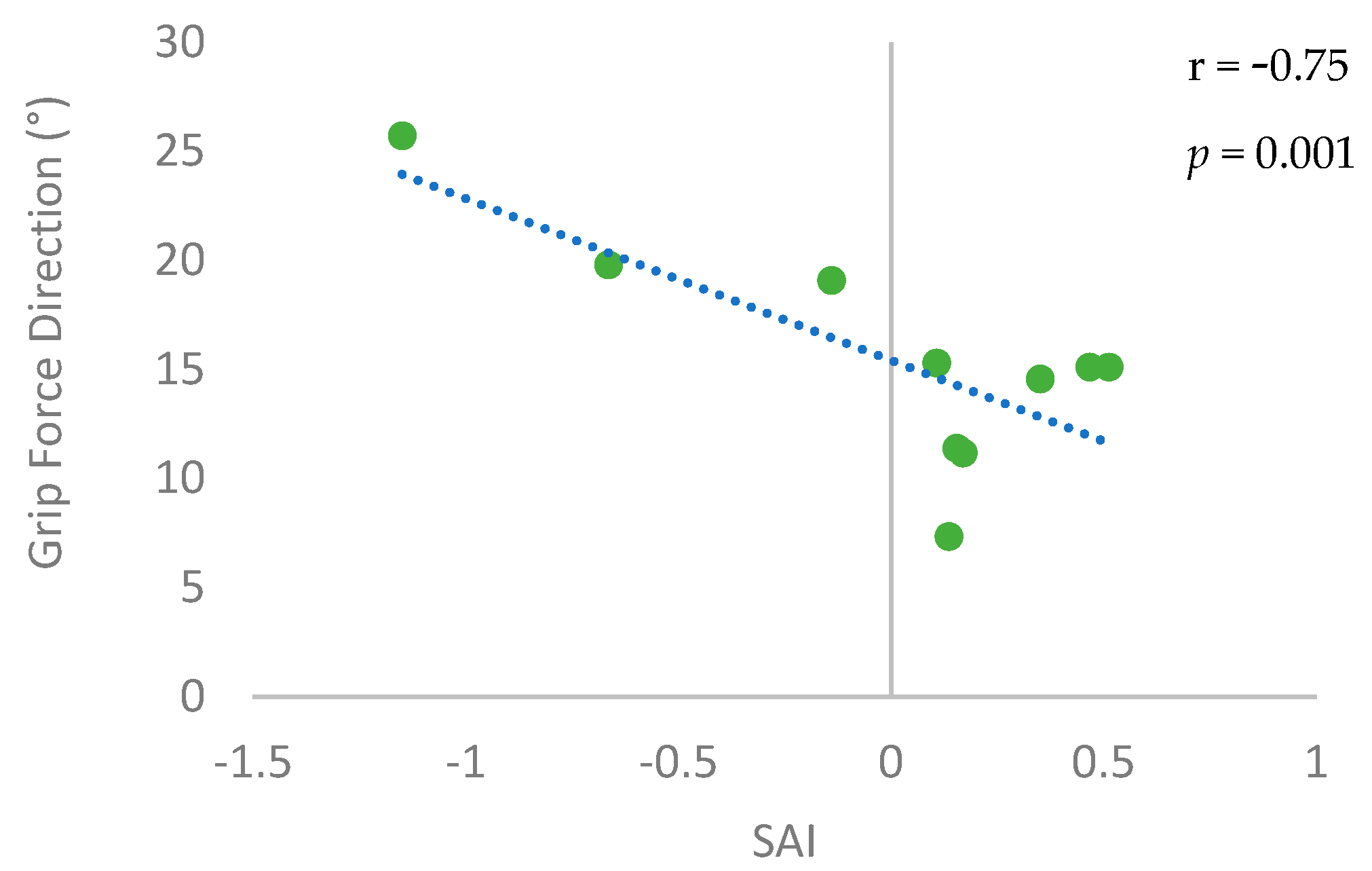
3. Results
4. Discussion
4.1. The Role of SAI for Functional Recovery Post Stroke
4.2. The Neural Origin of Impaired Grip Force Direction Control Post Stroke
4.3. Influence of Sensory Impairment on SAI and Grip Force Direction Control Post Stroke
4.4. Clinical Implications
4.5. Limitations and Future Direction
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Katan, M.; Luft, A. Global Burden of Stroke. Semin. Neurol. 2018, 38, 208–211. [Google Scholar] [CrossRef]
- Lawrence, E.S.; Coshall, C.; Dundas, R.; Stewart, J.; Rudd, A.G.; Howard, R.; Wolfe, C.D. Estimates of the prevalence of acute stroke impairments and disability in a multiethnic population. Stroke 2001, 32, 1279–1284. [Google Scholar] [CrossRef]
- Stewart, J.C.; Cramer, S.C. Patient-reported measures provide unique insights into motor function after stroke. Stroke 2013, 44, 1111–1116. [Google Scholar] [CrossRef] [PubMed]
- Soechting, J.F.; Flanders, M. Sensorimotor control of contact force. Curr. Opin. Neurobiol. 2008, 18, 565–572. [Google Scholar] [CrossRef]
- Fikes, T.G.; Klatzky, R.L.; Lederman, S.J. Effects of Object Texture on Precontact Movement Time in Human Prehension. J. Mot. Behav. 1994, 26, 325–332. [Google Scholar] [CrossRef]
- MacKenzie, C.L.; Iberall, T. The Grasping Hand, 1st ed.; Elsevier Science: Amsterdam, The Netherlands, 1994. [Google Scholar]
- Seo, N.J.; Enders, L.R.; Motawar, B.; Kosmopoulos, M.; Fathi-Firoozabad, M. The extent of altered digit force direction correlates with clinical upper extremity impairment in chronic stroke survivors. J. Biomech. 2015, 48, 383. [Google Scholar] [CrossRef] [PubMed]
- Enders, L.R.; Seo, N.J. Phalanx force magnitude and trajectory deviation increased during power grip with an increased coefficient of friction at the hand-object interface. J. Biomech. 2011, 44, 1447–1453. [Google Scholar] [CrossRef]
- Seo, N.J.; Armstrong, T.J.; Drinkaus, P. A comparison of two methods of measuring static coefficient of friction at low normal forces: A pilot study. Ergonomics 2009, 52, 121–135. [Google Scholar] [CrossRef] [PubMed]
- Hermsdorfer, J.; Hagl, E.; Nowak, D.A.; Marquardt, C. Grip force control during object manipulation in cerebral stroke. Clin. Neurophysiol. 2003, 114, 915–929. [Google Scholar] [CrossRef]
- Seo, N.J.; Rymer, W.Z.; Kamper, D.G. Altered digit force direction during pinch grip following stroke. Exp. Brain Res. 2010, 202, 891–901. [Google Scholar] [CrossRef]
- Enders, L.R.; Seo, N.J. Altered phalanx force direction during power grip following stroke. Exp. Brain Res. 2015, 233, 1677–1688. [Google Scholar] [CrossRef] [PubMed]
- Fugl-Meyer, A.R.; Jääskö, L.; Leyman, I.; Olsson, S.; Steglind, S. The post-stroke hemiplegic patient. 1. a method for evaluation of physical performance. Scand. J. Rehabil. Med. 1975, 7, 13–31. [Google Scholar] [CrossRef] [PubMed]
- Gladstone, D.J.; Danells, C.J.; Black, S.E. The fugl-meyer assessment of motor recovery after stroke: A critical review of its measurement properties. Neurorehabilit. Neural Repair 2002, 16, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Miller, P.; Huijbregts, M.; Gowland, C.; Barreca, S.; Torresin, W.; Moreland, J.; Dunkley, M.; Griffiths, J.; Van Hulenaar, S.; Vanspall, B. CHEDOKE-McMASTER Stroke Assessment: Development, Validation, and Administration Manual; McMaster University: Hamilton, ON, Canada, 2008. [Google Scholar]
- Gowland, C.; Stratford, P.; Ward, M.; Moreland, J.; Torresin, W.; Van Hullenaar, S.; Sanford, J.; Barreca, S.; Vanspall, B.; Plews, N. Measuring physical impairment and disability with the Chedoke-McMaster Stroke Assessment. Stroke 1993, 24, 58–63. [Google Scholar] [CrossRef]
- Seo, N.J.; Fischer, H.W.; Bogey, R.A.; Rymer, W.Z.; Kamper, D.G. Use of visual force feedback to improve digit force direction during pinch grip in persons with stroke: A pilot study. Arch. Phys. Med. Rehabil. 2011, 92, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Enders, L.R.; Seo, N.J. Effects of Sensory Deficit on Phalanx Force Deviation During Power Grip Post Stroke. J. Mot. Behav. 2017, 49, 55–66. [Google Scholar] [CrossRef]
- Nowak, D.A.; Hermsdorfer, J. Grip force behavior during object manipulation in neurological disorders: Toward an objective evaluation of manual performance deficits. Mov. Disord. 2005, 20, 11–25. [Google Scholar] [CrossRef]
- Parry, R.; Soria, S.M.; Pradat-Diehl, P.; Marchand-Pauvert, V.; Jarrassé, N.; Roby-Brami, A. Effects of Hand Configuration on the Grasping, Holding, and Placement of an Instrumented Object in Patients With Hemiparesis. Front. Neurol. 2019, 10, 240. [Google Scholar] [CrossRef]
- Westling, G.; Johansson, R.S. Factors influencing the force control during precision grip. Exp. Brain Res. 1984, 53, 277–284. [Google Scholar] [CrossRef]
- Bolognini, N.; Russo, C.; Edwards, D.J. The sensory side of post-stroke motor rehabilitation. Restor. Neurol. Neurosci. 2016, 34, 571–586. [Google Scholar] [CrossRef]
- Kasuga, S.; Telgen, S.; Uchiba, J.; Nozaki, D.; Diedrichsen, J. Learning feedback and feedforward control in a mirror-reversed visual environment. J. Neurophysiol. 2015, 114, 2187–2193. [Google Scholar] [CrossRef]
- Ackerley, S.J.; Stinear, C.M.; Barber, P.A.; Byblow, W.D. Priming sensorimotor cortex to enhance task-specific training after subcortical stroke. Clin. Neurophysiol. 2014, 125, 1451–1458. [Google Scholar] [CrossRef]
- Tokimura, H.; Di Lazzaro, V.; Tokimura, Y.; Oliviero, A.; Profice, P.; Insola, A.; Mazzone, P.; Tonali, P.; Rothwell, J.C. Short latency inhibition of human hand motor cortex by somatosensory input from the hand. J. Physiol. 2000, 523, 503. [Google Scholar] [CrossRef]
- Tokimura, H.; Ridding, M.C.; Tokimura, Y.; Amassian, V.E.; Rothwell, J.C. Short latency facilitation between pairs of threshold magnetic stimuli applied to human motor cortex. Electroencephalogr. Clin. Neurophysiol. 1996, 101, 263–272. [Google Scholar] [CrossRef]
- Koizume, Y.; Hirano, M.; Kubota, S.; Tanaka, S.; Funase, K. Relationship between the changes in M1 excitability after motor learning and arousal state as assessed by short-latency afferent inhibition. Behav. Brain Res. 2017, 330, 56–62. [Google Scholar] [CrossRef]
- Sawaki, L.; Boroojerdi, B.; Kaelin-Lang, A.; Burstein, A.H.; Butefisch, C.M.; Kopylev, L.; Davis, B.; Cohen, L.G. Cholinergic influences on use-dependent plasticity. J. Neurophysiol. 2002, 87, 166–171. [Google Scholar] [CrossRef]
- Meintzschel, F.; Ziemann, U. Modification of practice-dependent plasticity in human motor cortex by neuromodulators. Cereb. Cortex 2006, 16, 1106–1115. [Google Scholar] [CrossRef]
- Ackerley, S.J.; Stinear, C.M.; Barber, P.A.; Byblow, W.D. Combining theta burst stimulation with training after subcortical stroke. Stroke 2010, 41, 1568–1572. [Google Scholar] [CrossRef]
- Di Lazzaro, V.; Profice, P.; Pilato, F.; Capone, F.; Ranieri, F.; Florio, L.; Colosimo, C.; Pravatà, E.; Pasqualetti, P.; Dileone, M. The level of cortical afferent inhibition in acute stroke correlates with long-term functional recovery in humans. Stroke 2012, 43, 250–252. [Google Scholar] [CrossRef]
- Brown, K.E.; Neva, J.L.; Feldman, S.J.; Staines, W.R.; Boyd, L.A. Sensorimotor integration in chronic stroke: Baseline differences and response to sensory training. Restor. Neurol. Neurosci. 2018, 36, 245–259. [Google Scholar] [CrossRef]
- Woodbury, M.L.; Velozo, C.A.; Richards, L.G.; Duncan, P.W.; Studenski, S.; Lai, S.M. Dimensionality and construct validity of the Fugl-Meyer Assessment of the upper extremity. Arch. Phys. Med. Rehabil. 2007, 88, 715–723. [Google Scholar] [CrossRef] [PubMed]
- Desrosiers, J.; Bravo, G.; Hébert, R.; Dutil, E.; Mercier, L. Validation of the Box and Block Test as a measure of dexterity of elderly people: Reliability, validity, and norms studies. Arch. Phys. Med. Rehabil. 1994, 75, 751–755. [Google Scholar] [CrossRef] [PubMed]
- Mathiowetz, V.; Volland, G.; Kashman, N.; Weber, K. Adult norms for the Box and Block Test of manual dexterity. Am. J. Occup. Ther. 1985, 39, 386–391. [Google Scholar] [CrossRef] [PubMed]
- Bell-Krotoski, J.; Tomancik, E. The repeatability of testing with Semmes-Weinstein monofilaments. J. Hand Surg. Am. 1987, 12, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Brant-Zawadzki, M.; Gillan, G.D.; Nitz, W.R. MP RAGE: A three-dimensional, T1-weighted, gradient-echo sequence--initial experience in the brain. Radiology 1992, 182, 769–775. [Google Scholar] [CrossRef] [PubMed]
- Rorden, C.; Brett, M. Stereotaxic display of brain lesions. Behav. Neurol. 2000, 12, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Liew, S.L.; Schweighofer, N.; Cole, J.H.; Zavaliangos-Petropulu, A.; Lo, B.P.; Han, L.K.; Hahn, T.; Schmaal, L.; Donnelly, M.; Jeong, J.N.; et al. Association of Brain Age, Lesion Volume, and Functional Outcome in Patients With Stroke. Neurology 2023, 100, e2103–e2113. [Google Scholar] [CrossRef] [PubMed]
- Liew, S.L.; Zavaliangos-Petropulu, A.; Jahanshad, N.; Lang, C.E.; Haywards, K.S.; Lohse, K.R.; Juliano, J.M.; Assogna, F.; Baugh, L.A.; Bhattacharya, A.K. The ENIGMA Stroke Recovery Working Group: Big data neuroimaging to study brain-behavior relationships after stroke. Hum. Brain Mapp. 2022, 43, 129–148. [Google Scholar] [CrossRef]
- Vucic, S.; Chen, K.H.S.; Kiernan, M.C.; Hallett, M.; Benninger, D.H.; Di Lazarro, V.; Rossini, P.M.; Benussi, A.; Berardelli, A.; Currà, A.; et al. Clinical diagnostic utility of transcranial magnetic stimulation in neurological disorders. Updated report of an IFCN committee. Clin. Neurophysiol. 2023, 150, 131–175. [Google Scholar] [CrossRef]
- Rossini, P.M.; Burke, D.; Chen, R.; Cohen, L.G.; Daskalakis, Z.; Di Iorio, R.; Di Lazzaro, V.; Ferreri, F.; Fitzgerald, P.B.; George, M.S.; et al. Non-invasive electrical and magnetic stimulation of the brain, spinal cord, roots and peripheral nerves: Basic principles and procedures for routine clinical and research application. An updated report from an IFCN Committee. Clin. Neurophysiol. 2015, 126, 1071–1107. [Google Scholar] [CrossRef]
- Mishory, A.; Molnar, C.; Koola, J.; Li, X.; Kozel, A.; Myrick, H.; Stroud, Z.; Nahas, Z.; George, M.S. The maximum-likelihood strategy for determining transcranial magnetic stimulation motor threshold, using parameter estimation by sequential testing is faster than conventional methods with similar precision. J. ECT 2004, 20, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Butefisch, C.M.; Netz, J.; Wessling, M.; Seitz, R.J.; Hömberg, V. Remote changes in cortical excitability after stroke. Brain 2003, 126, 470–481. [Google Scholar] [CrossRef]
- Toepp, S.L.; Turco, C.V.; Reshi, R.S.; Nelson, A.J. The distribution and reliability of TMS-evoked short- and long-latency afferent interactions. PLoS ONE 2021, 16, e0260663. [Google Scholar] [CrossRef] [PubMed]
- Ehrenstein, W.H.; Ehrenstein, A. Psychophysical methods. In Modern Techniques in Neuroscience Research; Windhorst, U., Johansson, H., Eds.; Springer: Berlin/Heidelberg, Germany, 1999; pp. 1211–1241. [Google Scholar]
- Fischer, M.; Orth, M. Short-latency sensory afferent inhibition: Conditioning stimulus intensity, recording site, and effects of 1 Hz repetitive TMS. Brain Stimul. 2011, 4, 202–209. [Google Scholar] [CrossRef]
- Du, X.; Summerfelt, A.; Chiappelli, J.; Holocomb, H.H.; Hong, L.E. Individualized brain inhibition and excitation profile in response to paired-pulse TMS. J. Mot. Behav. 2014, 46, 39–48. [Google Scholar] [CrossRef]
- Asmussen, M.J.; Jacobs, M.F.; Lee, K.G.H.; Zapallow, C.M.; Nelson, A.J. Short-Latency Afferent Inhibition Modulation during Finger Movement. PLoS ONE 2013, 8, e60496. [Google Scholar] [CrossRef]
- Turco, C.V.; El-Sayes, J.; Savoie, M.J.; Fassett, H.J.; Locke, M.B.; Nelson, A.J. Short- and long-latency afferent inhibition; uses, mechanisms and influencing factors. Brain Stimul. 2018, 11, 59–74. [Google Scholar] [CrossRef]
- Paulus, W.; Classen, J.; Cohen, L.G.; Large, C.H.; Di Lazzaro, V.; Nitsche, M.; Pascual-Leone, A.; Rosenow, F.; Rothwell, J.C.; Ziemann, U. State of the art: Pharmacologic effects on cortical excitability measures tested by transcranial magnetic stimulation. Brain Stimul. 2008, 1, 151–163. [Google Scholar] [CrossRef]
- Dobkin, B.H. Do electrically stimulated sensory inputs and movements lead to long-term plasticity and rehabilitation gains? Curr. Opin. Neurol. 2003, 16, 685–691. [Google Scholar] [CrossRef]
- Mirdamadi, J.L.; Block, H.J. Somatosensory changes associated with motor skill learning. J. Neurophysiol. 2020, 123, 1052–1062. [Google Scholar] [CrossRef]
- Honaga, K.; Fujiwara, T.; Tsuji, T.; Hase, K.; Uchiba, J.; Liu, M. State of intracortical inhibitory interneuron activity in patients with chronic stroke. Clin. Neurophysiol. 2013, 124, 364–370. [Google Scholar] [CrossRef] [PubMed]
- Turco, C.V.; Locke, M.B.; El—Sayes, J.; Tommerdahl, M.; Nelson, A.J. Exploring behavioral correlates of afferent inhibition. Brain Sci. 2018, 8, 64. [Google Scholar] [CrossRef] [PubMed]
- Baker, A.; Schranz, C.; Seo, N.J. Associating Functional Neural Connectivity and Specific Aspects of Sensorimotor Control in Chronic Stroke. Sensors 2023, 23, 5398. [Google Scholar] [CrossRef] [PubMed]
- Schranz, C.; Srivastava, S.; Seamon, B.A.; Marebwa, B.; Bonilha, L.; Ramakrishnan, V.; Wilmskoetter, J.; Neptune, R.R.; Kautz, S.A.; Seo, N.J. Different aspects of hand grip performance associated with structural connectivity of distinct sensorimotor networks in chronic stroke. Physiol. Rep. 2023, 11, e15659. [Google Scholar] [CrossRef] [PubMed]
- Oliviero, A.; Molina Leon, A.; Holler, I.; Florensa Vila, J.; Siebner, H.R.; Della Marca, G.; Di Lazzaro, V.; Tejeira Alvarez, J. Reduced sensorimotor inhibition in the ipsilesional motor cortex in a patient with chronic stroke of the paramedian thalamus. Clin. Neurophysiol. 2005, 116, 2592–2598. [Google Scholar] [CrossRef]
- Alaydin, H.C.; Ataoglu, E.E.; Caglayan, H.Z.B.; Togoz, N.; Cengiz, B. Short-latency afferent inhibition remains intact without cortical somatosensory input: Evidence from a patient with isolated thalamic infarct. Brain Stimul. Basic Transl. Clin. Res. Neuromodul. 2021, 14, 804–806. [Google Scholar] [CrossRef]
- Vidoni, E.D.; Boyd, L.A. Preserved motor learning after stroke is related to the degree of proprioceptive deficit. Behav. Brain Funct. 2009, 5, 36. [Google Scholar] [CrossRef]
- Blaschke, J.; Vatinno, A.A.; Scronce, G.; Ramakrishnan, V.; Seo, N.J. Effect of Sensory Impairment on Hand Functional Improvement with Therapy and Sensory Stimulation. Neurol. Neurorehabilit. 2022, 4, 1–4. [Google Scholar] [PubMed]
- Tyson, S.F.; Hanley, M.; Chillala, J.; Selley, A.B.; Tallis, R.C. Sensory loss in hospital-admitted people with stroke: Characteristics, associated factors, and relationship with function. Neurorehabilit. Neural Repair 2008, 22, 166–172. [Google Scholar] [CrossRef]
- Meyer, S.; Karttunen, A.H.; Thijs, V.; Feys, H.; Verheyden, G. How do somatosensory deficits in the arm and hand relate to upper limb impairment, activity, and participation problems after stroke? A systematic review. Phys. Ther. 2014, 94, 1220–1231. [Google Scholar] [CrossRef] [PubMed]
- Hammerbeck, U.; Tyson, S.F.; Samraj, P.; Hollands, K.; Krakauer, J.W.; Rothwell, J. The Strength of the Corticospinal Tract Not the Reticulospinal Tract Determines Upper-Limb Impairment Level and Capacity for Skill-Acquisition in the Sub-Acute Post-Stroke Period. Neurorehabilit. Neural Repair 2021, 35, 812–822. [Google Scholar] [CrossRef]
- Hammerbeck, U.; Hoad, D.; Greenwood, R.; Rothwell, J. The unsolved role of heightened connectivity from the unaffected hemisphere to paretic arm muscles in chronic stroke. Clin. Neurophysiol. 2019, 130, 781–788. [Google Scholar] [CrossRef] [PubMed]
- Buetefisch, C.M.; Revill, K.P.; Haut, M.W.; Kowalski, G.M.; Wischnewski, M.; Pifer, M.; Belagaje, S.R.; Nahab, F.; Cobia, D.J.; Hu, X.; et al. Abnormally reduced primary motor cortex output is related to impaired hand function in chronic stroke. J. Neurophysiol. 2018, 120, 1680–1694. [Google Scholar] [CrossRef]
- Maier, M.; Ballester, B.R.; Verschure, P.F.M.J. Principles of Neurorehabilitation after Stroke Based on Motor Learning and Brain Plasticity Mechanisms. Front. Syst. Neurosci. 2019, 13, 74. [Google Scholar] [CrossRef] [PubMed]
- Fisicaro, F.; Lanza, G.; Grasso, A.A.; Pennsisi, G.; Bella, R.; Paulus, W.; Pennisi, M. Repetitive transcranial magnetic stimulation in stroke rehabilitation: Review of the current evidence and pitfalls. Ther. Adv. Neurol. Disord. 2019, 12, 1756286419878317. [Google Scholar] [CrossRef] [PubMed]
- Edwards, L.L.; King, E.M.; Buetefisch, C.M.; Borich, M.R. Putting the “sensory” into sensorimotor control: The role of sensorimotor integration in goal-directed hand movements after stroke. Front. Integr. Neurosci. 2019, 13, 16. [Google Scholar] [CrossRef]
- Seo, N.J.; Kamper, D.G.; Ramakrishnan, V.; Harvey, J.B.; Finetto, C.; Schranz, C.; Scronce, G.; Coupland, K.; Howard, K.; Blaschke, J.; et al. Effect of novel training to normalize altered finger force direction post-stroke: Study protocol for a double-blind randomized controlled trial. Trials 2022, 23, 301. [Google Scholar] [CrossRef] [PubMed]
- Palmer, J.A.; Wolf, S.L.; Borich, M.R. Paired associative stimulation modulates corticomotor excitability in chronic stroke: A preliminary investigation. Restor. Neurol. Neurosci. 2018, 36, 183–194. [Google Scholar] [CrossRef] [PubMed]
- Turco, C.V.; Pesevski, A.; McNicholas, P.D.; Beaulieu, L.D.; Nelson, A.J. Reliability of transcranial magnetic stimulation measures of afferent inhibition. Brain Res. 2019, 1723, 146394. [Google Scholar] [CrossRef]
- Brown, K.E.; Lohse, K.R.; Mayer, I.M.S.; Stigaro, G.; Desikan, M.; Capsula, E.P.; Meunier, S.; Popa, T.; Lahmy, J.-C.; Odish, O.; et al. The reliability of commonly used electrophysiology measures. Brain Stimul. 2017, 10, 1102–1111. [Google Scholar] [CrossRef]
- Wang, L.; Wang, S.; Zhang, S.; Dou, Z.; Guo, T. Effectiveness and electrophysiological mechanisms of focal vibration on upper limb motor dysfunction in patients with subacute stroke: A randomized controlled trial. Brain Res. 2023, 1809, 148353. [Google Scholar] [CrossRef] [PubMed]
- Kutch, J.J.; Valero-Cuevas, F.J. Muscle redundancy does not imply robustness to muscle dysfunction. J. Biomech. 2011, 44, 1264–1270. [Google Scholar] [CrossRef] [PubMed]
- Cruz, E.G.; Waldinger, H.C.; Kamper, D.G. Kinetic and kinematic workspaces of the index finger following stroke. Brain 2005, 128, 1112–1121. [Google Scholar] [CrossRef] [PubMed]
- Kamper, D.; Barry, A.; Bansal, N.; Stoykov, M.E.; Triandafilou, K.; Vindakovic, L.; Seo, N.J.; Roth, E. Use of cyproheptadine hydrochloride (HCl) to reduce neuromuscular hypertonicity in stroke survivors: A Randomized Trial: Reducing Hypertonicity in Stroke. J. Stroke Cerebrovasc. Dis. 2022, 31, 106724. [Google Scholar] [CrossRef]
- Ruddy, K.L.; Jaspers, E.; Keller, M.; Wenderoth, N. Interhemispheric sensorimotor integration; an upper limb phenomenon? Neuroscience 2016, 333, 104–113. [Google Scholar] [CrossRef]
- Smith, M.C.; Ackerley, S.J.; Barber, P.A.; Byblow, W.D.; Stinear, C.M. PREP2 Algorithm Predictions Are Correct at 2 Years Poststroke for Most Patients. Neurorehabilit. Neural Repair 2019, 33, 635–642. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Descriptive Statistics |
|---|---|
| Age in years (mean ± SD) | 61.1 ± 10.9 |
| Gender (male/female) | 5/5 |
| Race (White/African American) | 5/5 |
| Type of stroke (ischemic/hemorrhagic) | 8/2 |
| Affected side (right/left) | 7/3 |
| Time since stroke in months (mean ± SD) | 59.9 ± 38.4 |
| Fugl-Meyer Assessment of Motor Recovery after Stroke—Upper Extremity score (mean ± SD out of 66) | 47.8 ± 11.6 |
| Box and Block Test score (# of blocks that could be moved with the paretic hand in one minute, mean ± SD) | 30.0 ± 16.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schranz, C.; Seo, N.J. Cortical Sensorimotor Integration as a Neural Origin of Impaired Grip Force Direction Control following Stroke. Brain Sci. 2024, 14, 253. https://doi.org/10.3390/brainsci14030253
Schranz C, Seo NJ. Cortical Sensorimotor Integration as a Neural Origin of Impaired Grip Force Direction Control following Stroke. Brain Sciences. 2024; 14(3):253. https://doi.org/10.3390/brainsci14030253
Chicago/Turabian StyleSchranz, Christian, and Na Jin Seo. 2024. "Cortical Sensorimotor Integration as a Neural Origin of Impaired Grip Force Direction Control following Stroke" Brain Sciences 14, no. 3: 253. https://doi.org/10.3390/brainsci14030253