
Risk of Motor Vehicle Collisions and Culpability among Older Drivers Using Cannabis: A Meta-Analysis
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
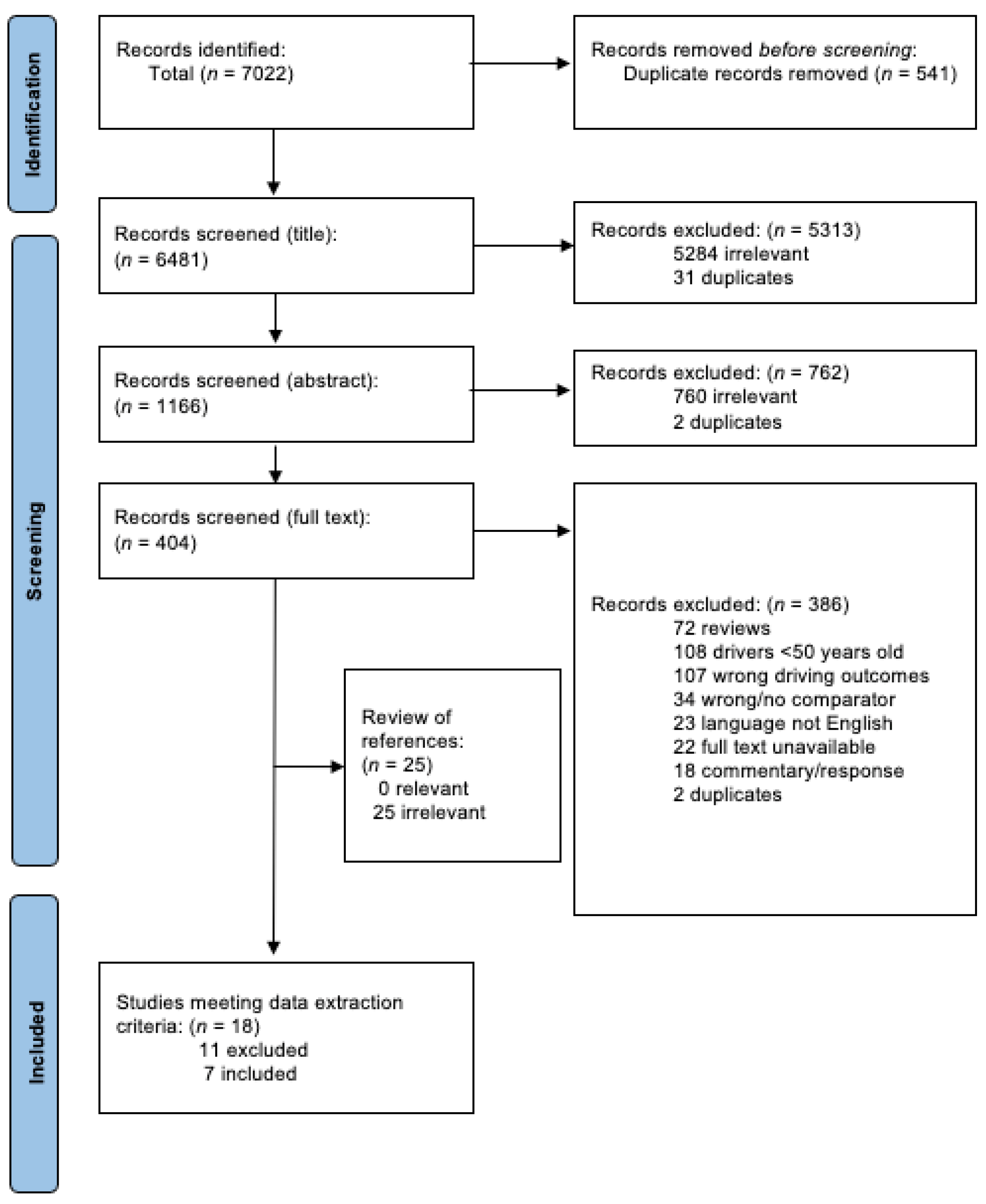
2.1. Search Strategy
2.2. Data Synthesis and Quality Assessment
2.3. Statistical Analysis
3. Results
3.1. Overview of Included Studies
3.2. Studies of THC Exposure and MVC Risk
3.3. Studies of THC Exposure and Driver Culpability
3.4. Other Features of Studies
- i.
- Confounding Variables
- ii.
- Measures of THC Exposure
- iii.
- Timeframe of THC Exposure
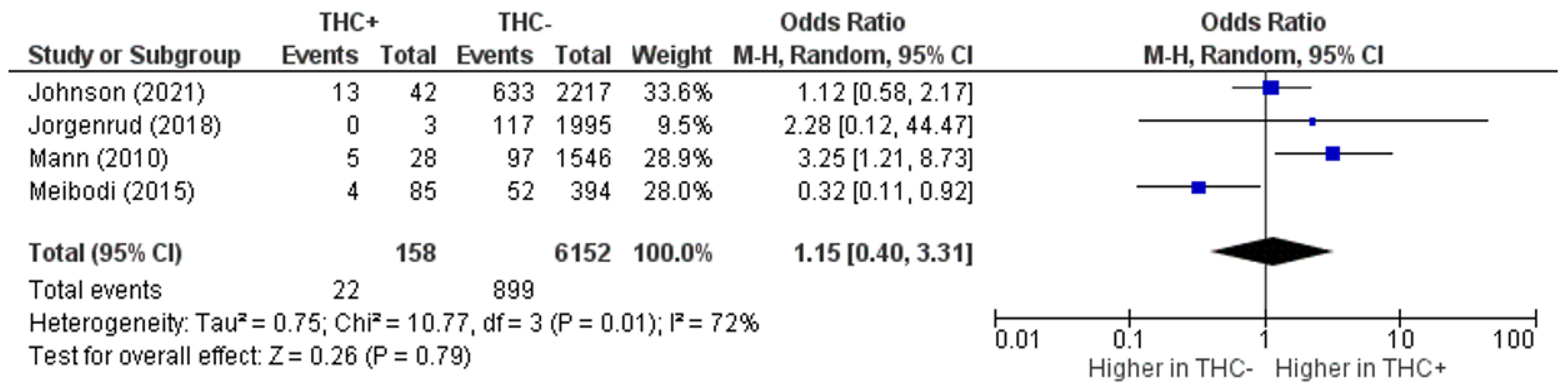
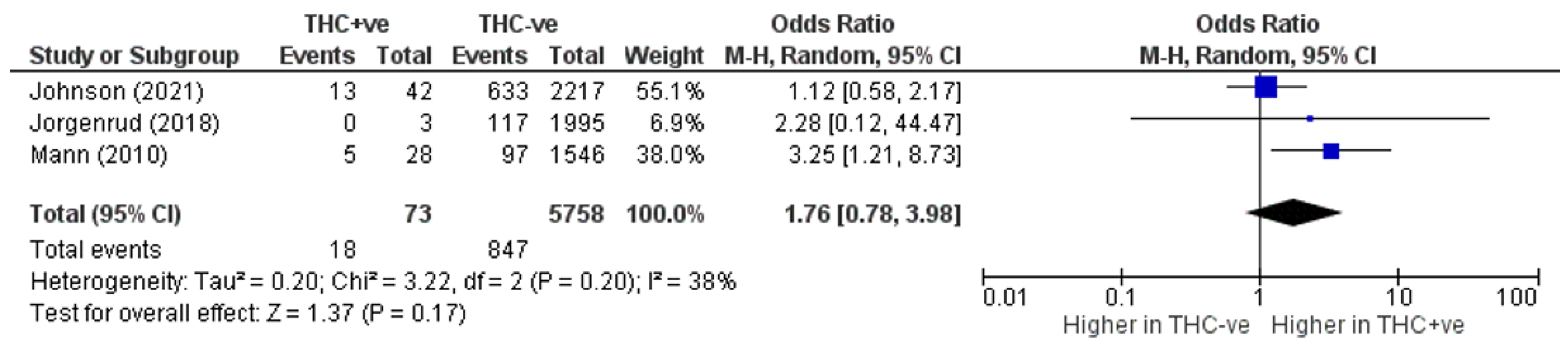
3.5. Meta-Analysis of Risk of MVC with THC
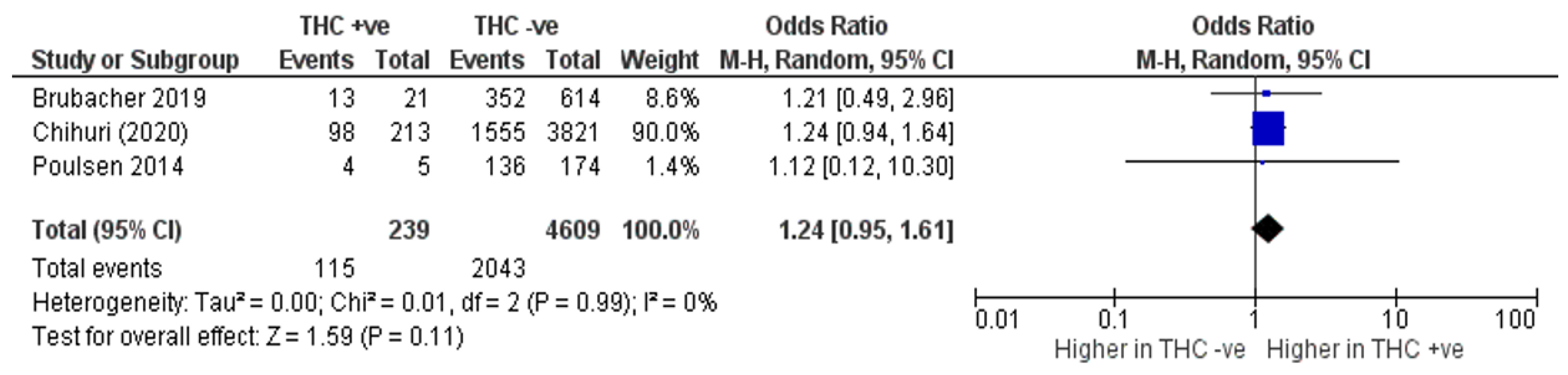
3.6. Meta-Analysis of MVC Culpability with THC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| Search Strategies |
| Database: EBM Reviews-Cochrane Central Register of Controlled Trials <January 2021> |
| Search Strategy: |
| -------------------------------------------------------------------------------- |
| 1 exp Cannabis/(303) |
| 2 cannabis.mp. (2655) |
| 3 exp Cannabinoids/(826) |
| 4 cannabinoid*.mp. (1133) |
| 5 marijuana.mp. (1926) |
| 6 exp Dronabinol/(737) |
| 7 tetrahydrocannabinol*.mp. (1014) |
| 8 nabilone.mp. (156) |
| 9 exp Cannabidiol/(131) |
| 10 cannabidiol*.mp. (700) |
| 11 sativex.mp. (153) |
| 12 or/1–11 (4763) |
| 13 exp Automobile Driving/(821) |
| 14 driv*.mp. (19485) |
| 15 motorist*.mp. (15) |
| 16 Safety/(3149) |
| 17 Automobile Driver Examination/(23) |
| 18 Licensure/(36) |
| 19 ((driv* or motor* or safe*) adj3 (assess* or reassess* or screen* or licen* or relicen* or re-licen* or |
| test or re-test* or permit*)).mp. (55056) |
| 20 Accidents, Traffic/(420) |
| 21 crash*.mp. (688) |
| 22 collision*.mp. (396) |
| 23 accident*.mp. (21938) |
| 24 or/13– 23 (95411) |
| 25 12 and 24 (474) |
| Database: Embase Classic+Embase <1947 to 2021 Week 05> |
| Search Strategy: |
| -------------------------------------------------------------------------------- |
| 1 exp cannabis/(38661) |
| 2 exp cannabis addiction/(10178) |
| 3 exp cannabis derivative/(332) |
| 4 cannabis.mp. (55670) |
| 5 exp cannabinoid/(73223) |
| 6 cannabinoid*.mp. (35085) |
| 7 marijuana.mp. (19346) |
| 8 exp tetrahydrocannabinol/(7048) |
| 9 tetrahydrocannabinol*.mp. (14376) |
| 10 exp nabilone/(1394) |
| 11 nabilone.mp. (1451) |
| 12 exp cannabidiol/(5459) |
| 13 cannabidiol.mp. (6330) |
| 14 exp nabiximols/(763) |
| 15 sativex.mp. (727) |
| 16 or/1–15 (94981) |
| 17 exp car driving/(27133) |
| 18 driv*.mp. (620343) |
| 19 motorist*.mp. (729) |
| 20 safety/(263615) |
| 21 licensing/(24183) |
| 22 driver licence/(2921) |
| 23 ((driv* or motor* or safe*) adj3 (assess* or reassess* or screen* or licen* or relicen* or re-licen* or |
| test or re-test* or permit*)).tw. (93362) |
| 24 exp traffic accident/(66650) |
| 25 exp driver/(16113) |
| 26 exp driving ability/(7496) |
| 27 crash*.mp. (17733) |
| 28 collision*.mp. (35924) |
| 29 accident*.mp. (476435) |
| 30 or/17– 29 (1429215) |
| 31 16 and 30 (5535) |
| Database: Ovid MEDLINE(R) and Epub Ahead of Print, In-Process & Other Non-Indexed Citations, Daily |
| and Versions(R) <1946 to February 10, 2021> |
| Search Strategy: |
| -------------------------------------------------------------------------------- |
| 1 exp Cannabis/(9548) |
| 2 cannabis.mp. (24434) |
| 3 exp Cannabinoids/(14641) |
| 4 cannabinoid*.mp. (24303) |
| 5 marijuana.mp. (21437) |
| 6 exp Dronabinol/(7197) |
| 7 tetrahydrocannabinol*.mp. (7803) |
| 8 nabilone.mp. (354) |
| 9 exp Cannabidiol/(1823) |
| 10 cannabidiol*.mp. (3715) |
| 11 sativex.mp. (201) |
| 12 or/1–11 (55974) |
| 13 exp Automobile Driving/(20791) |
| 14 driv*.mp. (491344) |
| 15 motorist*.mp. (568) |
| 16 Safety/(40479) |
| 17 Automobile Driver Examination/(1424) |
| 18 Licensure/(7134) |
| 19 ((driv* or motor* or safe*) adj3 (assess* or reassess* or screen* or licen* or relicen* or re-licen* or |
| test or re-test* or permit*)).mp. (58034) |
| 20 Accidents, Traffic/(44092) |
| 21 crash*.mp. (14958) |
| 22 collision*.mp. (39736) |
| 23 accident*.mp. (200303) |
| 24 or/13– 23 (798657) |
| 25 12 and 24 (2680) |
| Database: APA PsycInfo <1806 to February Week 2 2021> |
| Search Strategy: |
| -------------------------------------------------------------------------------- |
| 1 exp Cannabis/(8919) |
| 2 exp “Cannabis Use Disorder”/(492) |
| 3 cannabis.mp. (12901) |
| 4 exp Cannabinoids/(5766) |
| 5 cannabinoid*.mp. (6588) |
| 6 exp Marijuana/(3303) |
| 7 exp Marijuana Usage/(3021) |
| 8 marijuana.mp. (12183) |
| 9 dronabinol*.mp. (1682) |
| 10 exp Tetrahydrocannabinol/(1560) |
| 11 tetrahydrocannabinol*.mp. (2594) |
| 12 nabilone.mp. (90) |
| 13 cannabidiol*.mp. (801) |
| 14 sativex.mp. (71) |
| 15 or/1–14 (26992) |
| 16 exp Driving Behavior/(14895) |
| 17 driv*.mp. (122720) |
| 18 motorist*.mp. (498) |
| 19 Safety/(14143) |
| 20 exp Drivers/(6416) |
| 21 ((driv* or motor* or safe*) adj3 (assess* or reassess* or screen* or licen* or relicen* or re-licen* or |
| test or re-test* or permit*)).mp. (15322) |
| 22 exp Motor Traffic Accidents/(5889) |
| 23 crash*.mp. (5702) |
| 24 collision*.mp. (3585) |
| 25 accident*.mp. (55110) |
| 26 or/16 – 25 (193190) |
| 27 15 and 26 (1347) |
References
- Burkhardt, J.E.; Mcgavock, A.T. Tomorrow’s Older Drivers: Who? How Many? What Impacts? Transp. Res. Rec. J. Transp. Res. Board 1999, 1693, 62–70. [Google Scholar] [CrossRef]
- Anstey, K.J.; Wood, J.M.; Lord, S.R.; Walker, J.G. Cognitive, sensory and physical factors enabling driving safety in older adults. Clin. Psychol. Rev. 2005, 25, 45–65. [Google Scholar] [CrossRef] [PubMed]
- Office of Highway Policy Information Highway Statistics 2020. Available online: https://www.fhwa.dot.gov/policyinformation/statistics/2020/ (accessed on 1 December 2022).
- Klein, R.; Klein, B.E.K. The Prevalence of Age-Related Eye Diseases and Visual Impairment in Aging: Current Estimates. Investig. Opthalmology Vis. Sci. 2013, 54, ORSF5–ORSF13. [Google Scholar] [CrossRef] [Green Version]
- Dahlhamer, J.; Lucas, J.; Zelaya, C.; Nahin, R.; Mackey, S.; DeBar, L.; Kerns, R.; Von Korff, M.; Porter, L.; Helmick, C. Prevalence of Chronic Pain and High-Impact Chronic Pain Among Adults—United States, 2016. MMWR. Morb. Mortal. Wkly. Rep. 2018, 67, 1001–1006. [Google Scholar] [CrossRef] [PubMed]
- Yazdanyar, A.; Newman, A.B. The Burden of Cardiovascular Disease in the Elderly: Morbidity, Mortality, and Costs. Clin. Geriatr. Med. 2009, 25, 563–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marshall, S.C.; Man-Son-Hing, M. Multiple Chronic Medical Conditions and Associated Driving Risk: A Systematic Review. Traffic Inj. Prev. 2011, 12, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Cox, A.E.; Cicchino, J.B. Continued trends in older driver crash involvement rates in the United States: Data through 2017–2018. J. Saf. Res. 2021, 77, 288–295. [Google Scholar] [CrossRef] [PubMed]
- Langford, J.; Koppel, S. The case for and against mandatory age-based assessment of older drivers. Transp. Res. Part F Traffic Psychol. Behav. 2006, 9, 353–362. [Google Scholar] [CrossRef]
- Karthaus, M.; Falkenstein, M. Functional Changes and Driving Performance in Older Drivers: Assessment and Interventions. Geriatrics 2016, 1, 12. [Google Scholar] [CrossRef] [Green Version]
- Choi, N.G.; DiNitto, D.M.; Marti, C.N. Risk Factors for Self-reported Driving Under the Influence of Alcohol and/or Illicit Drugs Among Older Adults. Gerontologist 2014, 56, 282–291. [Google Scholar] [CrossRef] [Green Version]
- Li, M.-C.; Brady, J.E.; DiMaggio, C.J.; Lusardi, A.R.; Tzong, K.Y.; Li, G. Marijuana Use and Motor Vehicle Crashes. Epidemiologic Rev. 2011, 34, 65–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, J.-L.; Gadegbeku, B.; Wu, D.; Viallon, V.; Laumon, B. Cannabis, alcohol and fatal road accidents. PLoS ONE 2017, 12, e0187320. [Google Scholar] [CrossRef]
- Broyd, S.J.; van Hell, H.H.; Beale, C.; Yücel, M.; Solowij, N. Acute and Chronic Effects of Cannabinoids on Human Cognition—A Systematic Review. Biol. Psychiatry 2015, 79, 557–567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bahji, A.; Stephenson, C. International Perspectives on the Implications of Cannabis Legalization: A Systematic Review & Thematic Analysis. Int. J. Environ. Res. Public Health 2019, 16, 3095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pearlson, G.D.; Stevens, M.C.; D’Souza, D.C. Cannabis and Driving. Front. Psychiatry 2021, 12, 689444. [Google Scholar] [CrossRef]
- Pollini, R.A.; Romano, E.; Johnson, M.B.; Lacey, J.H. The impact of marijuana decriminalization on California drivers. Drug Alcohol Depend. 2015, 150, 135–140. [Google Scholar] [CrossRef]
- Dubois, S.; Mullen, N.; Weaver, B.; Bédard, M. The combined effects of alcohol and cannabis on driving: Impact on crash risk. Forensic Sci. Int. 2015, 248, 94–100. [Google Scholar] [CrossRef]
- Brubacher, J.R.; Chan, H.; Erdelyi, S.; Staples, J.A.; Asbridge, M.; Mann, R.E. Cannabis Legalization and Detection of Tetrahydrocannabinol in Injured Drivers. N. Engl. J. Med. 2022, 386, 148–156. [Google Scholar] [CrossRef]
- Asbridge, M.; A Hayden, J.; Cartwright, J.L. Acute cannabis consumption and motor vehicle collision risk: Systematic review of observational studies and meta-analysis. BMJ 2012, 344, e536. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.H.; Mooney, S.J. The epidemiologic principles underlying traffic safety study designs. Leuk. Res. 2016, 45, 1668–1675. [Google Scholar] [CrossRef] [Green Version]
- Longo, M.C.; Hunter, C.E.; Lokan, R.J.; White, J.M.; White, M.A. The prevalence of alcohol, cannabinoids, benzodiazepines and stimulants amongst injured drivers and their role in driver culpability: Part i: The prevalence of drug use in drive the drug-positive group. Accid. Anal. Prev. 2000, 32, 613–622. [Google Scholar] [CrossRef] [PubMed]
- Drummer, O.H.; Gerostamoulos, J.; Batziris, H.; Chu, M.; Caplehorn, J.; Robertson, M.D.; Swann, P. The involvement of drugs in drivers of motor vehicles killed in Australian road traffic crashes. Accid. Anal. Prev. 2003, 36, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Laumon, B.; Gadegbeku, B.; Martin, J.L.; Biecheler, M.B.; Group, S.A.M. Cannabis intoxication and fatal road crashes in France: Population based case-control study. BMJ 2005, 331, 1371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brubacher, J.; Chan, H.; Asbridge, M. Culpability analysis is still a valuable technique. Int. J. Epidemiol. 2014, 43, 270–272. [Google Scholar] [CrossRef] [Green Version]
- Drummer, O.H.; Gerostamoulos, D.; Di Rago, M.; Woodford, N.W.; Morris, C.; Frederiksen, T.; Jachno, K.; Wolfe, R. Odds of culpability associated with use of impairing drugs in injured drivers in Victoria, Australia. Accid. Anal. Prev. 2020, 135, 105389. [Google Scholar] [CrossRef]
- Rosen, D.; Hunsaker, A.; Albert, S.M.; Cornelius, J.R.; Reynolds, C.F. Characteristics and consequences of heroin use among older adults in the United States: A review of the literature, treatment implications, and recommendations for further research. Addict. Behav. 2011, 36, 279–285. [Google Scholar] [CrossRef] [Green Version]
- Velayudhan, L.; McGoohan, K.; Bhattacharyya, S. Safety and tolerability of natural and synthetic cannabinoids in adults aged over 50 years: A systematic review and meta-analysis. PLoS Med. 2021, 18, e1003524. [Google Scholar] [CrossRef]
- Meibodi, M.K.; Esfandyari, S.; Siyabi, V.; Roosta, S. Illicit Drug Abuse in Drivers of Motor Vehicle Collisions. Galen Med. J. 2015, 4, 39–46. [Google Scholar] [CrossRef]
- National Heart Lung and Blood Institute, Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 1 December 2022).
- Johnson, M.B.; Mechtler, L.; Ali, B.; Swedler, D.; Kelley-Baker, T. Cannabis and crash risk among older drivers. Accid. Anal. Prev. 2021, 152, 105987. [Google Scholar] [CrossRef]
- Jørgenrud, B.; Bogstrand, S.T.; Furuhaugen, H.; Jamt, R.E.G.; Vindenes, V.; Gjerde, H. Association between speeding and use of alcohol and medicinal and illegal drugs and involvement in road traffic crashes among motor vehicle drivers. Traffic Inj. Prev. 2018, 19, 779–785. [Google Scholar] [CrossRef]
- Mann, R.E.; Stoduto, G.; Butters, J.; Ialomiteanu, A.; Boase, P.; Asbridge, M.; Chipman, M.; Wickens, C.M. Age group differences in collision risk. J. Saf. Res. 2010, 41, 445–449. [Google Scholar] [CrossRef] [PubMed]
- Brubacher, J.R.; Chan, H.; Erdelyi, S.; Macdonald, S.; Asbridge, M.; Mann, R.E.; Eppler, J.; Lund, A.; MacPherson, A.; Martz, W.; et al. Cannabis use as a risk factor for causing motor vehicle crashes: A prospective study. Addiction 2019, 114, 1616–1626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poulsen, H.; Moar, R.; Pirie, R. The culpability of drivers killed in New Zealand road crashes and their use of alcohol and other drugs. Accid. Anal. Prev. 2014, 67, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Chihuri, S.; Li, G. Direct and indirect effects of marijuana use on the risk of fatal 2-vehicle crash initiation. Inj. Epidemiol. 2020, 7, 49. [Google Scholar] [CrossRef]
- Regev, S.; Rolison, J.J.; Moutari, S. Crash risk by driver age, gender, and time of day using a new exposure methodology. J. Saf. Res. 2018, 66, 131–140. [Google Scholar] [CrossRef]
- Turner, C.; McClure, R. Age and gender differences in risk-taking behaviour as an explanation for high incidence of motor vehicle crashes as a driver in young males. Inj. Control Saf. Promot. 2003, 10, 123–130. [Google Scholar] [CrossRef]
- Taylor, B.; Rehm, J. The Relationship Between Alcohol Consumption and Fatal Motor Vehicle Injury: High Risk at Low Alcohol Levels. Alcohol. Clin. Exp. Res. 2012, 36, 1827–1834. [Google Scholar] [CrossRef] [Green Version]
- Rudisill, T.M.; Zhu, M.; Kelley, G.A.; Pilkerton, C.; Rudisill, B.R. Medication use and the risk of motor vehicle collisions among licensed drivers: A systematic review. Accid. Anal. Prev. 2016, 96, 255–270. [Google Scholar] [CrossRef] [Green Version]
- A Soderstrom, C.; Dischinger, P.C.; A Kufera, J.; Ho, S.M.; Shepard, A. Crash culpability relative to age and sex for injured drivers using alcohol, marijuana or cocaine. Annu. Proc. Assoc. Adv. Automot. Med. 2005, 49, 327–341. [Google Scholar]
- Sharma, P.; Murthy, P.; Bharath, M.S. Chemistry, Metabolism, and Toxicology of Cannabis: Clinical Implications. Iran. J. Psychiatry 2012, 7, 149–156. [Google Scholar]
- Grotenhermen, F. Cannabinoids. Curr. Drug Target-CNS Neurol. Disord. 2005, 4, 507–530. [Google Scholar] [CrossRef]
- Grotenhermen, F. Pharmacokinetics and Pharmacodynamics of Cannabinoids. Clin. Pharmacokinet. 2003, 42, 327–360. [Google Scholar] [CrossRef]
- Rogeberg, O.; Elvik, R. The effects of cannabis intoxication on motor vehicle collision revisited and revised. Addiction 2016, 111, 1348–1359. [Google Scholar] [CrossRef] [Green Version]
- Hostiuc, S.; Moldoveanu, A.; Negoi, I.; Drima, E. Corrigendum: The Association of Unfavorable Traffic Events and Cannabis Usage: A Meta-Analysis. Front. Pharmacol. 2018, 9, 564. [Google Scholar] [CrossRef]
- White, M.A.; Burns, N.R. The risk of being culpable for or involved in a road crash after using cannabis: A systematic review and meta-analyses. Drug Sci. Policy Law 2021, 7, 20503245211055381. [Google Scholar] [CrossRef]
- Bergamaschi, M.M.; Karschner, E.L.; Goodwin, R.S.; Scheidweiler, K.B.; Hirvonen, J.; Queiroz, R.H.; A Huestis, M. Impact of Prolonged Cannabinoid Excretion in Chronic Daily Cannabis Smokers’ Blood on Per Se Drugged Driving Laws. Clin. Chem. 2013, 59, 519–526. [Google Scholar] [CrossRef] [Green Version]
- Augsburger, M.; Donzé, N.; Ménétrey, A.; Brossard, C.; Sporkert, F.; Giroud, C.; Mangin, P. Concentration of drugs in blood of suspected impaired drivers. Forensic Sci. Int. 2005, 153, 11–15. [Google Scholar] [CrossRef]
- Jones, A.W.; Holmgren, A.; Kugelberg, F.C. Driving under the influence of cannabis: A 10-year study of age and gender differences in the concentrations of tetrahydrocannabinol in blood. Addiction 2008, 103, 452–461. [Google Scholar] [CrossRef]
- Karschner, E.L.; Schwilke, E.W.; Lowe, R.H.; Darwin, W.D.; Herning, R.I.; Cadet, J.L.; Huestis, M.A. Implications of Plasma 9-Tetrahydrocannabinol, 11-Hydroxy-THC, and 11-nor-9-Carboxy-THC Concentrations in Chronic Cannabis Smokers. J. Anal. Toxicol. 2009, 33, 469–477. [Google Scholar] [CrossRef]
- Downey, L.A.; King, R.; Papafotiou, K.; Swann, P.; Ogden, E.; Boorman, M.; Stough, C. The effects of cannabis and alcohol on simulated driving: Influences of dose and experience. Accid. Anal. Prev. 2013, 50, 879–886. [Google Scholar] [CrossRef]
- Mura, P.; Kintz, P.; Ludes, B.; Gaulier, J.-M.; Marquet, P.; Martin-Dupont, S.; Vincent, F.; Kaddour, A.; Goullé, J.; Nouveau, J.; et al. Comparison of the prevalence of alcohol, cannabis and other drugs between 900 injured drivers and 900 control subjects: Results of a French collaborative study. Forensic Sci. Int. 2003, 133, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Verdejo-García, A.J.; López-Torrecillas, F.; de Arcos, F.A.; Pérez-García, M. Differential effects of MDMA, cocaine, and cannabis use severity on distinctive components of the executive functions in polysubstance users: A multiple regression analysis. Addict. Behav. 2005, 30, 89–101. [Google Scholar] [CrossRef] [PubMed]
- Baumbusch, J.; Yip, I.S. Older adults experiences of using recreational cannabis for medicinal purposes following legalization. Int. J. Drug Policy 2022, 108, 103812. [Google Scholar] [CrossRef] [PubMed]
- Gali, K.; Winter, S.J.; Ahuja, N.J.; Frank, E.; Prochaska, J.J. Changes in cannabis use, exposure, and health perceptions following legalization of adult recreational cannabis use in California: A prospective observational study. Subst. Abus. Treat. Prev. Policy 2021, 16, 16. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Question Number | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author (Year) | 1 | 2 | 3 * | 4 | 5 | 6 | 7 | 8 | 9 | 10 * | 11 | 12 | 13 * | 14 | Quality Rating |
| Culpability Studies | |||||||||||||||
| Brubacher | Yes | Yes | NA | Yes | Yes | No | No | Yes | Yes | NA | Yes | Yes | NA | Yes | “Good” |
| Chihuri | Yes | Yes | NA | Yes | No | No | No | No | Yes | NA | Yes | Yes | NA | Yes | “Fair” |
| Poulsen | No | Yes | NA | Yes | No | No | No | Yes | Yes | NA | Yes | Yes | NA | Yes | “Good” |
| MVC Risk Studies | |||||||||||||||
| Johnson | Yes | Yes | NA | Yes | No | No | No | No | Yes | NA | Yes | No | NA | Yes | “Good” |
| Jørgenrud | Yes | Yes | NA | Yes | No | No | No | No | Yes | NA | No | No | NA | Yes | “Poor” |
| Mann | Yes | Yes | NA | Yes | No | No | No | No | No | NA | No | No | NA | Yes | “Poor” |
| Kalantari Meibodi | Yes | Yes | NA | Yes | No | No | No | No | No | NA | Yes | No | NA | No | “Poor” |
| Author (Year), Quality Rating | Country (Dates) | Group Characteristics | THC Exposure Ascertainment | MVC Ascertainment | Key Findings in Older Adults |
|---|---|---|---|---|---|
| Johnson et al. (2021) “Good” [31] | United States (20-month period) | EXPT: Drivers (all ages) involved in MVC in Virginia Beach over a 20-month period COMP: Drivers (all ages) not involved in MVC that were sampled one week after crash cases in same location, road conditions and time of day | Blood and oral fluid; ELISA, LC-MS or GC-MS | On-scene data collection and police response | Crash rate of THC-positive drivers was significantly higher than that of sober drivers at ages 64 and 76 (F (1, 6757) = 3.8, p = 0.049; F (1, 6757) = 4.8, p = 0.028) |
| Kalantari Meibodi et al. (2015) “Poor” [29] | Iran (January–September 2012) | EXPT: Drivers (all ages) admitted to the emergency department following MVC COMP: Drivers (all ages) admitted to the emergency department for non-traumatic reasons | Self-report and urine (only drivers who claimed to have negative history of drug use); analytical technique not specified | Referral from emergency medical system following MVC | THC exposure was associated with lower odds of being involved in an MVC (OR, 95% CI 0.32 (0.11, 0.92)) in adults aged 55 and over |
| * Jørgenrud et al. (2018) “Poor” [32] | Norway (2016–2017) | EXPT: Drivers (all ages) with a positive history of MVC and speeding tickets in the last 12 months COMP: Drivers (all ages) with a negative history of MVC and speeding tickets in the last 12 months | Oral fluid; UPLC-MS/MS | Self-reported road traffic crashes | THC exposure was not significantly associated with odds of MVC involvement (OR, 95% CI 2.28 (0.12, 44.47)) in adults aged 50 and older |
| Mann et al. (2010) “Poor” [33] | Canada (2002–2005) | EXPT: Drivers (all ages) involved in MVCs that caused any kind of damage or injury in the past 12 months COMP: Drivers (all ages) not involved in MVCs in the past 12 months | Self-reported cannabis use | CAMH monitor self-report | Self-reported THC exposure in the last 12 months was not significantly associated with MVC risk among adults aged 55 and older (OR, 95% CI 1.18 (0.32, 4.36)) |
| Author (Year), Quality Rating | Country (Dates) | Group Characteristics | THC Exposure Ascertainment | Culpability Ascertainment | Key Findings in Older Adults |
|---|---|---|---|---|---|
| * Brubacher et al. (2019) “Good” [34] | Canada (2010–2016) | EXPT: Drivers (all ages) who were moderately injured in MVCs and deemed culpable for their crash COMP: Drivers (all ages) who were moderately injured in MVCs and deemed not culpable for their crash | Blood; broad-spectrum toxicological testing | Police crash reports | THC exposure did not have a significant effect on driver culpability (OR, 95% CI 1.21 (0.49, 2.96)) in adults aged 50 and over. |
| * Poulsen et al. (2014) “Good” [35] | New Zealand (2004–2009) | EXPT: Drivers (all ages) killed in MVCs who were deemed culpable for their crash COMP: Drivers (all ages) killed in MVCs who were deemed not culpable for their crash | Blood; immunoassay and LC-MS/MS | Police crash reports analyzed with Roberston and Drummer (1994) validated methodology | THC exposure was not significantly associated with culpability (OR, 95% CI 1.12 (0.12, 10.30)) in adults aged 50 and over. |
| * Chihuri & Li (2020) “Fair” [36] | United States (2011–2016) | EXPT: Drivers (all ages) killed in 2-vehicle MVCs who made ≥ 1 unsafe driver actions or errors COMP: Drivers (all ages) killed in 2-vehicle MVCs who made no unsafe driver actions or errors | Blood and urine; radioimmunoassay, LC-MS or GC-MS | Police reports and supporting documents | THC exposure did not significantly affect the risk of being deemed culpable for an MVC (OR, 95% CI 1.24 (0.94, 1.64)) in adults aged 50 and over. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chinna-Meyyappan, A.; Wang, H.J.; Bawa, K.K.; Ellazar, E.; Norris-Roozmon, E.; Naglie, G.; Herrmann, N.; Charlton, J.L.; Koppel, S.; Castel, S.; et al. Risk of Motor Vehicle Collisions and Culpability among Older Drivers Using Cannabis: A Meta-Analysis. Brain Sci. 2023, 13, 421. https://doi.org/10.3390/brainsci13030421
Chinna-Meyyappan A, Wang HJ, Bawa KK, Ellazar E, Norris-Roozmon E, Naglie G, Herrmann N, Charlton JL, Koppel S, Castel S, et al. Risk of Motor Vehicle Collisions and Culpability among Older Drivers Using Cannabis: A Meta-Analysis. Brain Sciences. 2023; 13(3):421. https://doi.org/10.3390/brainsci13030421
Chicago/Turabian StyleChinna-Meyyappan, Arun, Hui Jue Wang, Kritleen K. Bawa, Edward Ellazar, Emilie Norris-Roozmon, Gary Naglie, Nathan Herrmann, Judith L. Charlton, Sjaan Koppel, Saulo Castel, and et al. 2023. "Risk of Motor Vehicle Collisions and Culpability among Older Drivers Using Cannabis: A Meta-Analysis" Brain Sciences 13, no. 3: 421. https://doi.org/10.3390/brainsci13030421