
Transcranial Direct Current Stimulation over the Temporoparietal Junction Modulates Posture Control in Unfamiliar Environments
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
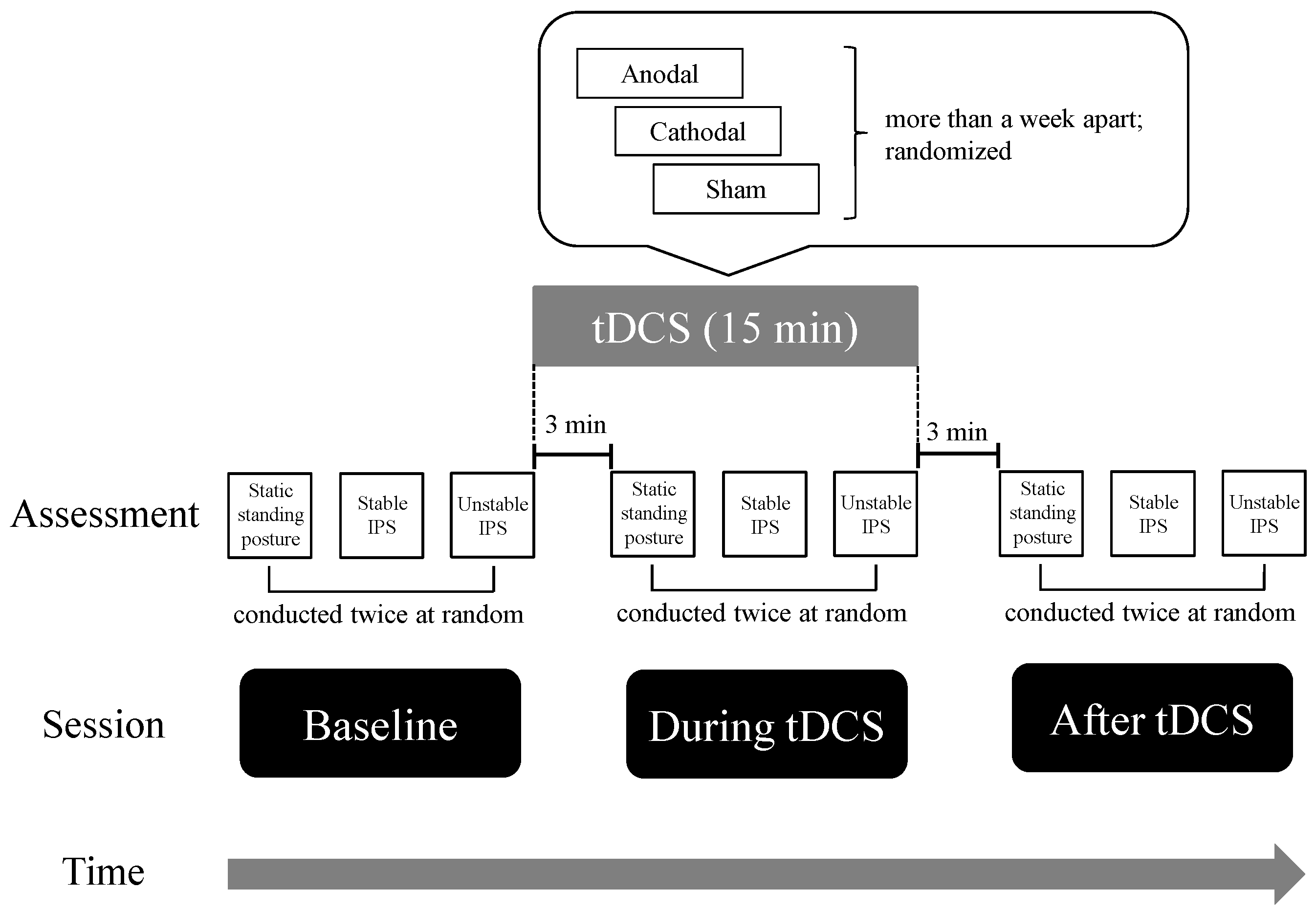
2.2. Experimental Flow
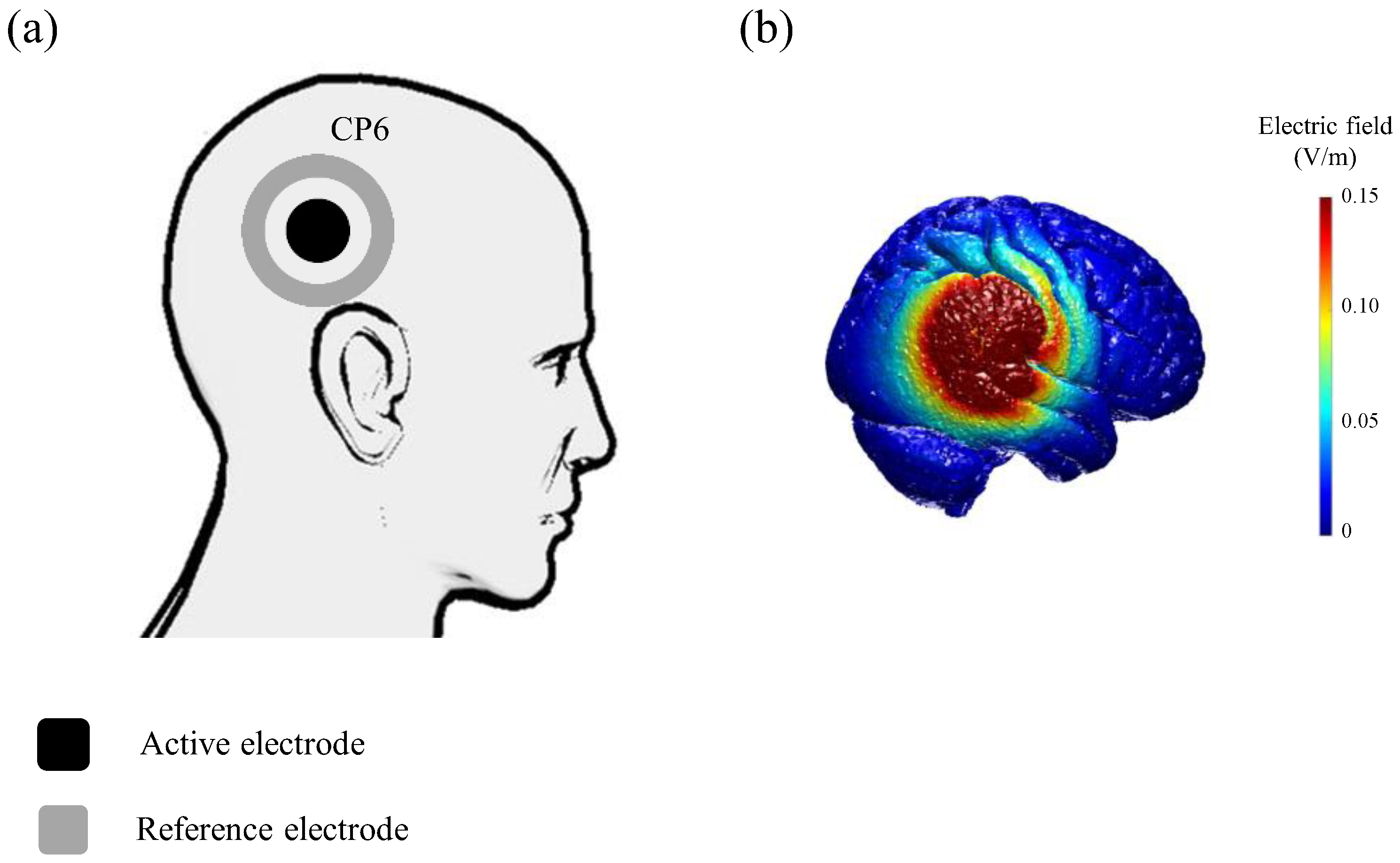
2.3. Application of tDCS
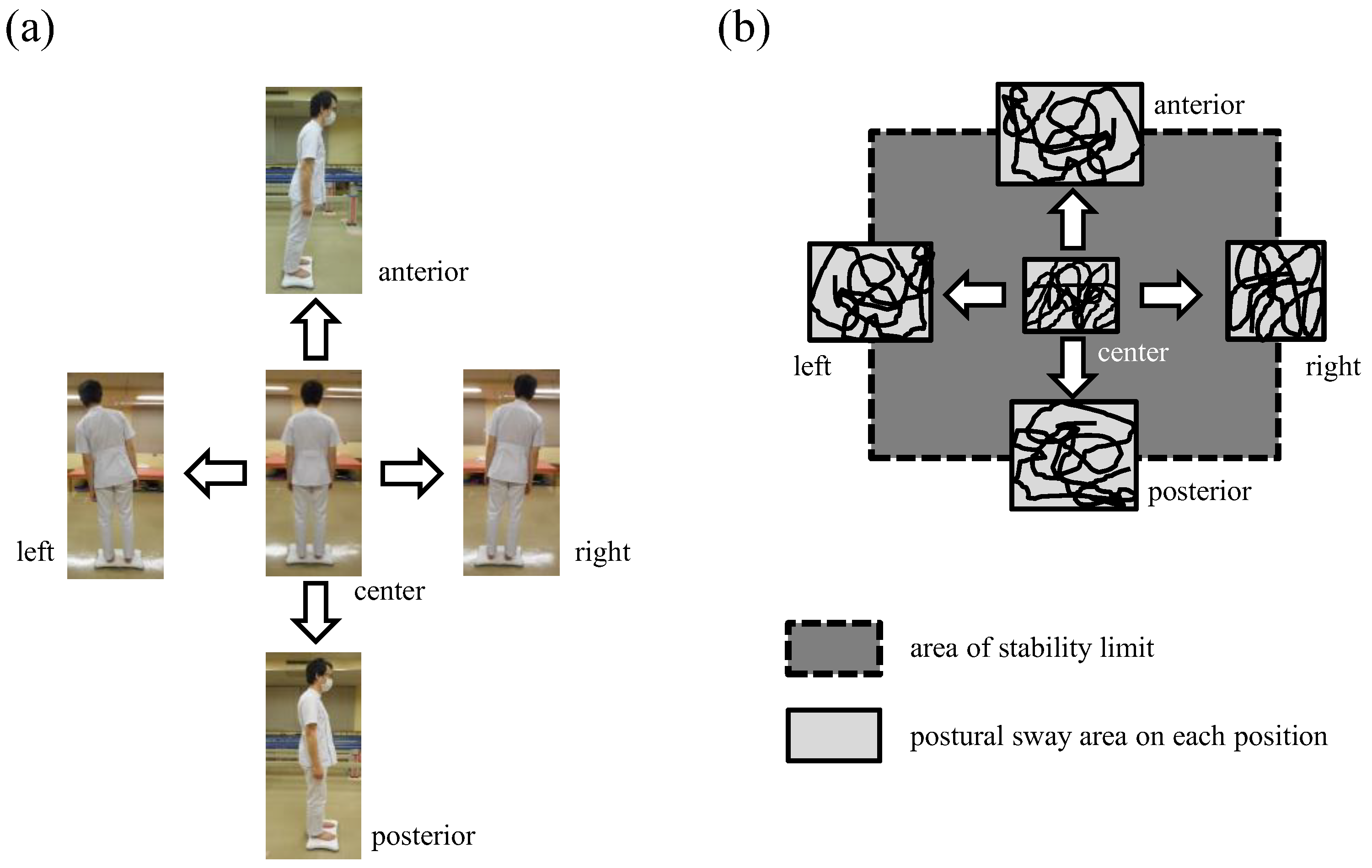
2.4. Measurement of Postural Control Performance
2.5. Statistical Analysis
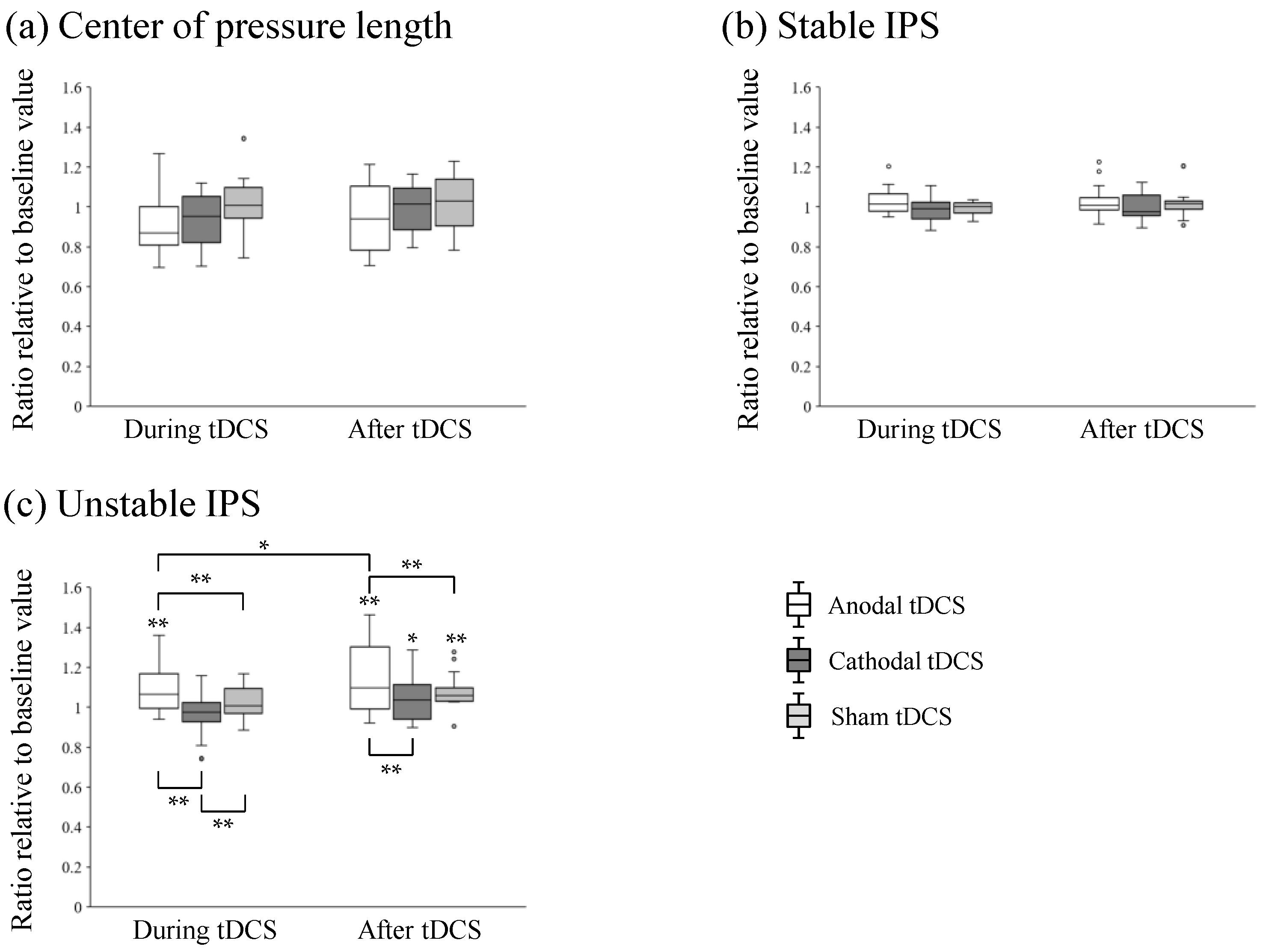
3. Results
4. Discussion
4.1. Neural Mechanisms through Which tDCS over the TPJ Modulated Postural Control
4.2. Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wallmann, H.W. The Basics of Balance and Falls. Home Health Care Manag. Pract. 2009, 21, 436–439. [Google Scholar] [CrossRef]
- Chiba, R.; Takakusaki, K.; Ota, J.; Yozu, A.; Haga, N. Human upright posture control models based on multisensory inputs; in fast and slow dynamics. Neurosci. Res. 2016, 104, 96–104. [Google Scholar] [CrossRef]
- Horak, F.B. Postural orientation and equilibrium: What do we need to know about neural control of balance to prevent falls? Age Ageing 2006, 35 (Suppl. S2), ii7–ii11. [Google Scholar] [CrossRef] [PubMed]
- Takakusaki, K. Neurophysiology of gait: From the spinal cord to the frontal lobe. Mov. Disord. 2013, 28, 1483–1491. [Google Scholar] [CrossRef] [PubMed]
- Osoba, M.Y.; Rao, A.K.; Agrawal, S.K.; Lalwani, A.K. Balance and gait in the elderly: A contemporary review. Laryngoscope Investig. Otolaryngol. 2019, 4, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Judge, J.O.; King, M.B.; Whipple, R.; Clive, J.; Wolfson, L.I. Dynamic balance in older persons: Effects of reduced visual and proprioceptive input. J. Gerontol. A Biol. Sci. Med. Sci. 1995, 50, M263–M270. [Google Scholar] [CrossRef] [PubMed]
- Kheradmand, A.; Winnick, A. Perception of Upright: Multisensory Convergence and the Role of Temporo-Parietal Cortex. Front. Neurol. 2017, 8, 552. [Google Scholar] [CrossRef]
- Karim, H.; Schmidt, B.; Dart, D.; Beluk, N.; Huppert, T. Functional near-infrared spectroscopy (fNIRS) of brain function during active balancing using a video game system. Gait Posture 2012, 35, 367–372. [Google Scholar] [CrossRef]
- Karim, H.; Fuhrman, S.I.; Sparto, P.; Furman, J.; Huppert, T. Functional brain imaging of multi-sensory vestibular processing during computerized dynamic posturography using near-infrared spectroscopy. Neuroimage 2013, 74, 318–325. [Google Scholar] [CrossRef]
- Perennou, D.A.; Leblond, C.; Amblard, B.; Micallef, J.P.; Rouget, E.; Pelissier, J. The polymodal sensory cortex is crucial for controlling lateral postural stability: Evidence from stroke patients. Brain Res. Bull. 2000, 53, 359–365. [Google Scholar] [CrossRef]
- Filmer, H.L.; Dux, P.E.; Mattingley, J.B. Applications of transcranial direct current stimulation for understanding brain function. Trends Neurosci. 2014, 37, 742–753. [Google Scholar] [CrossRef] [PubMed]
- Nitsche, M.A.; Paulus, W. Excitability changes induced in the human motor cortex by weak transcranial direct current stimulation. J. Physiol. 2000, 527 Pt 3, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Hogeveen, J.; Obhi, S.S.; Banissy, M.J.; Santiesteban, I.; Press, C.; Catmur, C.; Bird, G. Task-dependent and distinct roles of the temporoparietal junction and inferior frontal cortex in the control of imitation. Soc. Cogn. Affect. Neurosci. 2015, 10, 1003–1009. [Google Scholar] [CrossRef]
- Donaldson, P.H.; Rinehart, N.J.; Enticott, P.G. Noninvasive stimulation of the temporoparietal junction: A systematic review. Neurosci. Biobehav. Rev. 2015, 55, 547–572. [Google Scholar] [CrossRef]
- Downar, J.; Crawley, A.P.; Mikulis, D.J.; Davis, K.D. A multimodal cortical network for the detection of changes in the sensory environment. Nat. Neurosci. 2000, 3, 277–283. [Google Scholar] [CrossRef]
- Kyriakareli, A.; Cousins, S.; Pettorossi, V.E.; Bronstein, A.M. Effect of transcranial direct current stimulation on vestibular-ocular and vestibulo-perceptual thresholds. Neuroreport 2013, 24, 808–812. [Google Scholar] [CrossRef]
- Dalong, G.; Jiyuan, L.; Yubin, Z.; Yufei, Q.; Jinghua, Y.; Cong, W.; Hongbo, J. Cathodal Transcranial Direct Current Stimulation over the Right Temporoparietal Junction Suppresses Its Functional Connectivity and Reduces Contralateral Spatial and Temporal Perception. Front. Neurosci. 2021, 15, 629331. [Google Scholar] [CrossRef] [PubMed]
- Gandiga, P.C.; Hummel, F.C.; Cohen, L.G. Transcranial DC stimulation (tDCS): A tool for double-blind sham-controlled clinical studies in brain stimulation. Clin. Neurophysiol. 2006, 117, 845–850. [Google Scholar] [CrossRef]
- Huang, Y.; Datta, A.; Bikson, M.; Parra, L.C. Realistic Volumetric-Approach to Simulate Transcranial Electric Stimulation—ROAST—A fully automated open-source pipeline. J. Neural Eng. 2019, 16, 056006. [Google Scholar] [CrossRef]
- Grabner, G.; Janke, A.L.; Budge, M.M.; Smith, D.; Pruessner, J.; Collins, D.L. Symmetric atlasing and model based segmentation: An application to the hippocampus in older adults. Med. Image Comput. Comput. Assist. Interv. 2006, 9, 58–66. [Google Scholar] [CrossRef]
- Takeuchi, N.; Mori, T.; Suzukamo, Y.; Izumi, S.I. Modulation of Excitability in the Temporoparietal Junction Relieves Virtual Reality Sickness. Cyberpsychol. Behav. Soc. Netw. 2018, 21, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Yatoh, S.; Suzuki, H.; Tanabe, Y.; Shimizu, Y.; Hada, Y.; Shimano, H. Age-dependent changes in dynamic standing-balance ability evaluated quantitatively using a stabilometer. J. Phys. Ther. Sci. 2018, 30, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Takakura, H.; Nishijo, H.; Ishikawa, A.; Shojaku, H. Cerebral Hemodynamic Responses During Dynamic Posturography: Analysis with a Multichannel Near-Infrared Spectroscopy System. Front. Hum. Neurosci. 2015, 9, 620. [Google Scholar] [CrossRef] [PubMed]
- Kaski, D.; Quadir, S.; Nigmatullina, Y.; Malhotra, P.A.; Bronstein, A.M.; Seemungal, B.M. Temporoparietal encoding of space and time during vestibular-guided orientation. Brain 2016, 139, 392–403. [Google Scholar] [CrossRef]
- Santos, T.E.G.; Favoretto, D.B.; Toostani, I.G.; Nascimento, D.C.; Rimoli, B.P.; Bergonzoni, E.; Lemos, T.W.; Truong, D.Q.; Delbem, A.C.B.; Makkiabadi, B.; et al. Manipulation of Human Verticality Using High-Definition Transcranial Direct Current Stimulation. Front. Neurol. 2018, 9, 825. [Google Scholar] [CrossRef]
- Eikema, D.J.; Hatzitaki, V.; Tzovaras, D.; Papaxanthis, C. Application of intermittent galvanic vestibular stimulation reveals age-related constraints in the multisensory reweighting of posture. Neurosci. Lett. 2014, 561, 112–117. [Google Scholar] [CrossRef]
- Day, B.L.; Guerraz, M.; Cole, J. Sensory interactions for human balance control revealed by galvanic vestibular stimulation. Adv. Exp. Med. Biol. 2002, 508, 129–137. [Google Scholar] [CrossRef]
- Kaulmann, D.; Hermsdörfer, J.; Johannsen, L. Disruption of right posterior parietal cortex by continuous Theta Burst Stimulation alters the control of body balance in quiet stance. Eur. J. Neurosci. 2017, 45, 671–678. [Google Scholar] [CrossRef] [PubMed]
- Saturnino, G.B.; Madsen, K.H.; Siebner, H.R.; Thielscher, A. How to target inter-regional phase synchronization with dual-site Transcranial Alternating Current Stimulation. Neuroimage 2017, 163, 68–80. [Google Scholar] [CrossRef]
- Balasubramaniam, R.; Riley, M.A.; Turvey, M.T. Specificity of postural sway to the demands of a precision task. Gait Posture 2000, 11, 12–24. [Google Scholar] [CrossRef]
- Kheradmand, A.; Lasker, A.; Zee, D.S. Transcranial magnetic stimulation (TMS) of the supramarginal gyrus: A window to perception of upright. Cereb. Cortex 2015, 25, 765–771. [Google Scholar] [CrossRef] [PubMed]
- Corbetta, M.; Shulman, G.L. Spatial neglect and attention networks. Annu. Rev. Neurosci. 2011, 34, 569–599. [Google Scholar] [CrossRef] [PubMed]
- Guo, Z.; Bao, D.; Manor, B.; Zhou, J. The Effects of Transcranial Direct Current Stimulation (tDCS) on Balance Control in Older Adults: A Systematic Review and Meta-Analysis. Front. Aging Neurosci. 2020, 12, 275. [Google Scholar] [CrossRef]
- Baharlouei, H.; Saba, M.A.; Shaterzadeh Yazdi, M.J.; Jaberzadeh, S. The effect of transcranial direct current stimulation on balance in healthy young and older adults: A systematic review of the literature. Neurophysiol. Clin. 2020, 50, 119–131. [Google Scholar] [CrossRef] [PubMed]
- Nitsche, M.A.; Paulus, W. Sustained excitability elevations induced by transcranial DC motor cortex stimulation in humans. Neurology 2001, 57, 1899–1901. [Google Scholar] [CrossRef]
- Rostami, M.; Mosallanezhad, Z.; Ansari, S.; Ehsani, F.; Kidgell, D.; Nourbakhsh, M.R.; Bakhshi, E.; Jaberzadeh, S. Multi-session anodal transcranial direct current stimulation enhances lower extremity functional performance in healthy older adults. Exp. Brain Res. 2020, 238, 1925–1936. [Google Scholar] [CrossRef]
- Manor, B.; Zhou, J.; Harrison, R.; Lo, O.Y.; Travison, T.G.; Hausdorff, J.M.; Pascual-Leone, A.; Lipsitz, L. Transcranial Direct Current Stimulation May Improve Cognitive-Motor Function in Functionally Limited Older Adults. Neurorehabilit. Neural Repair 2018, 32, 788–798. [Google Scholar] [CrossRef]
- Ehsani, F.; Samaei, A.; Zoghi, M.; Hedayati, R.; Jaberzadeh, S. The effects of cerebellar transcranial direct current stimulation on static and dynamic postural stability in older individuals: A randomized double-blind sham-controlled study. Eur. J. Neurosci. 2017, 46, 2875–2884. [Google Scholar] [CrossRef]
- Yosephi, M.H.; Ehsani, F.; Zoghi, M.; Jaberzadeh, S. Multi-session anodal tDCS enhances the effects of postural training on balance and postural stability in older adults with high fall risk: Primary motor cortex versus cerebellar stimulation. Brain Stimul. 2018, 11, 1239–1250. [Google Scholar] [CrossRef]
- Kaminski, E.; Hoff, M.; Rjosk, V.; Steele, C.J.; Gundlach, C.; Sehm, B.; Villringer, A.; Ragert, P. Anodal Transcranial Direct Current Stimulation Does Not Facilitate Dynamic Balance Task Learning in Healthy Old Adults. Front. Hum. Neurosci. 2017, 11, 16. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Center of Pressure Length of Static Standings (cm) | Stable IPS | Unstable IPS | |
|---|---|---|---|
| 1st visit | 235.7 ± 48.8 | 2.110 ± 0.180 | 0.916 ± 0.292 |
| 2nd visit | 242.7 ± 59.5 | 2.080 ± 0.179 | 0.937 ± 0.244 |
| 3rd visit | 231.0 ± 49.2 | 2.025 ± 0.198 * | 0.946 ± 0.235 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kamada, H.; Takeuchi, N. Transcranial Direct Current Stimulation over the Temporoparietal Junction Modulates Posture Control in Unfamiliar Environments. Brain Sci. 2023, 13, 1514. https://doi.org/10.3390/brainsci13111514
Kamada H, Takeuchi N. Transcranial Direct Current Stimulation over the Temporoparietal Junction Modulates Posture Control in Unfamiliar Environments. Brain Sciences. 2023; 13(11):1514. https://doi.org/10.3390/brainsci13111514
Chicago/Turabian StyleKamada, Hiroshi, and Naoyuki Takeuchi. 2023. "Transcranial Direct Current Stimulation over the Temporoparietal Junction Modulates Posture Control in Unfamiliar Environments" Brain Sciences 13, no. 11: 1514. https://doi.org/10.3390/brainsci13111514