
Cardiac 123I-Metaiodobenzylguanidine (MIBG) Scintigraphy in Parkinson’s Disease: A Comprehensive Review


Abstract
:1. Introduction
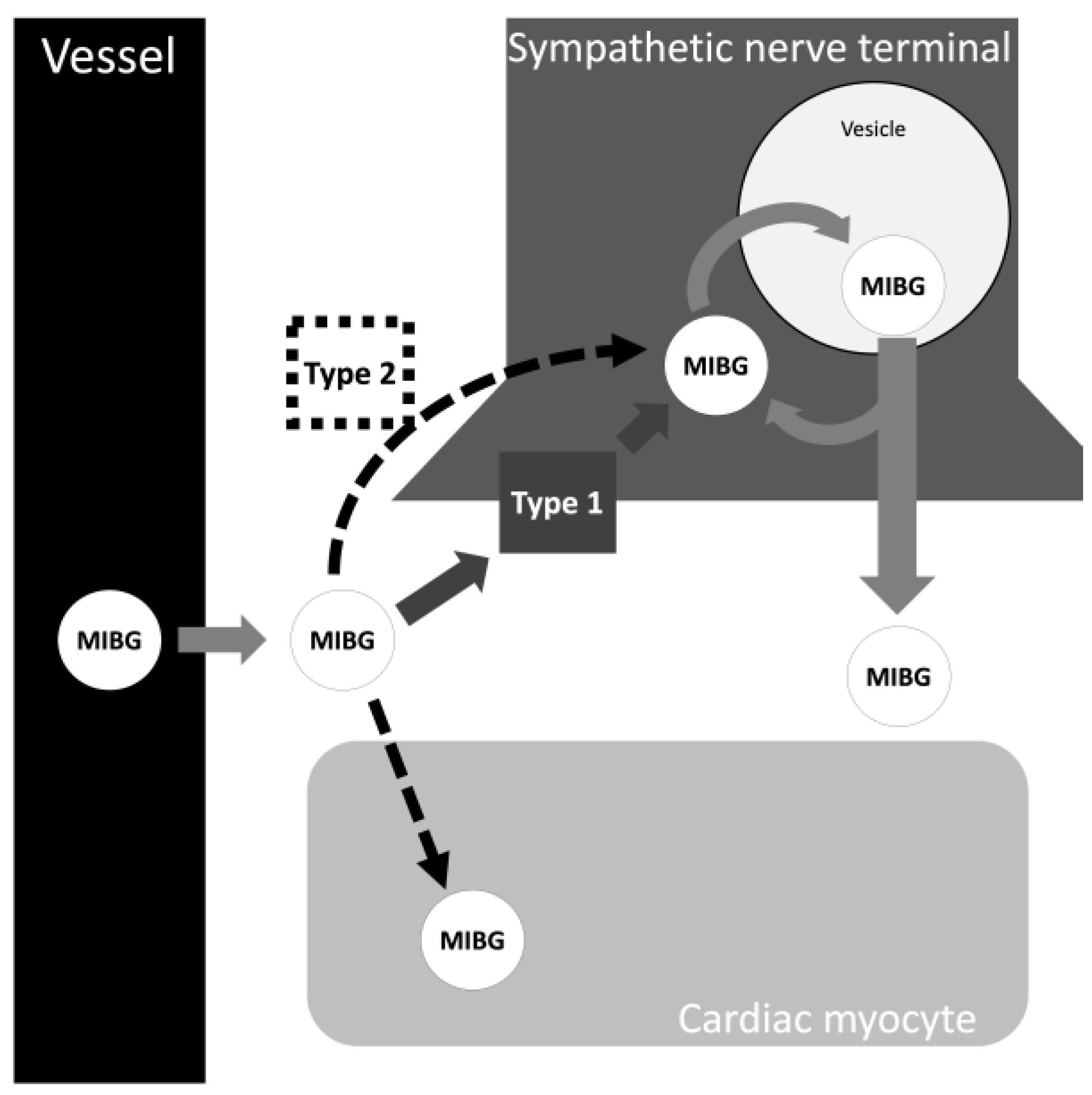
2. Cardiac MIBG Scintigraphy Technique
3. Parkinson’s Disease and Cardiac 123I-MIBG
3.1. Physiological and Anatomical Changes in the Cardiovascular System of Parkinson’s Disease
3.2. Cardiac MIBG Scintigraphy as a Supporting Criteria for PD
3.3. Cardiac MIBG Scintigraphy in Parkinson’s Disease
3.4. Autonomic Function in PD and Cardiac MIBG
3.5. Parkinson’s Disease Subtypes and Cardiac MIBG
3.6. Genetic Causes of Parkinson’s Disease
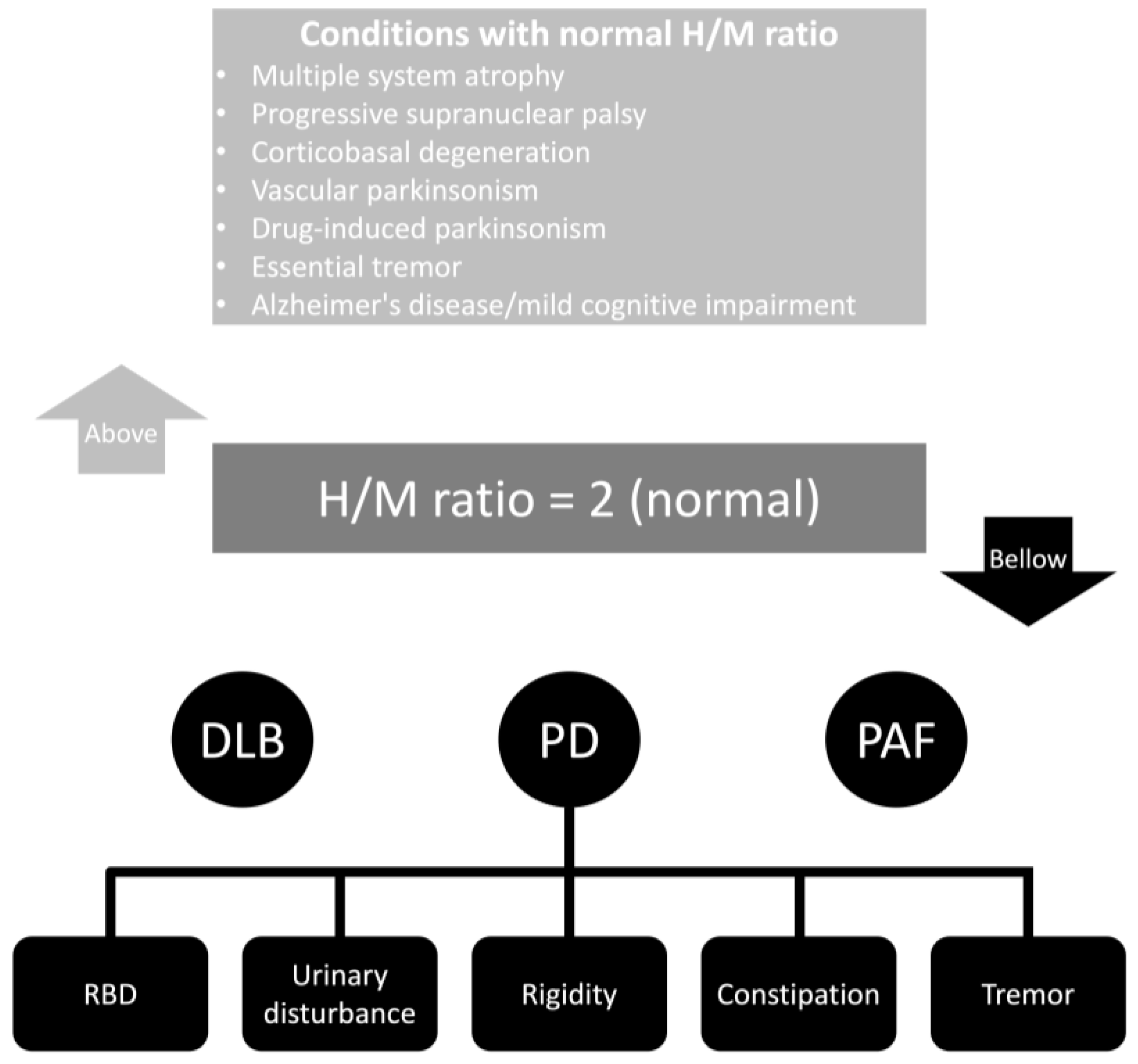
3.7. Normal Cardiac MIBG Uptake in Parkinson’s Disease
3.8. Sleep Behavior Disorder, Cognition, and Dysphagia
3.9. Cardiac MIBG Scintigraphy in Pre-Motor Parkinson’s Disease
4. Cardiac MIBG among Parkinsonian Syndromes
4.1. Dementia with Lewy Bodies
4.2. Multiple System Atrophy
4.3. Corticobasal Degeneration
4.4. Progressive Supranuclear Palsy
4.5. Essential Tremor
5. Dual Imaging Algorithm—Central and Peripheral Imaging
6. Automated Techniques in Cardiac MIBG Scintigraphy
7. Systematic Reviews
8. Expert Recommendations

{kind=link}
{kind=link}
{kind=link}
| Recommendation | Reference |
|---|---|
| 1. The medication list of the patient should be assessed. A clear observation should be performed for those drugs that influence the results of cardiac MIBG studies. A remarkable decrease in lung uptake in cardiac MIBG imaging may suggest the influence of drugs. | [24] |
| 2. Patients with structural cardiac conditions should be assessed case-by-case. Moreover, those individuals on use of inotropic agents should be assessed because false negative errors can occur. It is suggested to use polar model to have an anatominal localization of the defect and compare with previous cardiologic studies. | [194] |
| 3. Autonomic neuropathy should be investigated in individuals with risk factors for autonomic dysfunction before imaging is ordered. Noteworthy, some patients may have normal clinical findings, but their underlying conditions can lead to localized ganglioneuropathies. | [110] |
| 4. The heart-to-mediastinum ratio (H/M ratio) cut-off can significantly change the clinometric parameters of cardiac MIBG scintigraphy. A restrictive value can exclude many individuals with abnormal results. | [186] |
| 5. Cardiac MIBG scintigraphy should be used only as supporting criteria. No absolute conclusions should be obtained from this indirect test. | [6] |
| 6. The use of software to specifically assess the region of interest is recommended. Erroneous positions of the region of interest and abnormal anatomic positions can particularly lead to abnormal cardiac MIBG scintigraphy results. | [183] |
| 7. An electrocardiogram is recommended for some patients, especially the elderly. There is a significant association between aging and sick-sinus syndrome. It is worth mentioning that this syndrome at the early stages is usually asymptomatic. | [103] |
| 8. Cardiac MIBG imaging may be helpful in differentiating idiopathic PD from cases of secondary parkinsonism (drug-induced parkinsonism and vascular parkinsonism). Cardiac imaging should especially be applied when neuroimaging ([123I]-FP-CIT SPECT imaging) results can be misleading. | [200] |
| 9. Three-dimensional images, compared with planar, should be prioritized when available. They can provide better anatomical localization and a lower number of artifacts. | [194] |
| 10. Cardiac MIBG uptake abnormality with normal dopamine transporter imaging may suggest an early stage of PD. | [179] |
| 11. Follow-up sequential cardiac MIBG studies may improve the diagnostic accuracy of an abnormal result. It is recommended to pay special attention to the washout rate and delayed phase cardiac MIBG uptake, which are the first to change. | [197] |
| 12. The results of cardiac MIBG uptake can be used to assess the risk of developing syncope in individuals with PD. Also, it could be used as an objective finding of disease burden in patients with PD. | [123] |
| 13. In individuals with unknown cardiovascular structural disease, lung [123I]-MIBG scintigraphy can be used to assess the influence of the heart disease in the cardiac MIBG imaging. | [191] |
9. Future Studies
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marras, C.; Beck, J.C.; Bower, J.H.; Roberts, E.; Ritz, B.; Ross, G.W.; Abbott, R.D.; Savica, R.; Van Den Eeden, S.K.; Willis, A.W.; et al. Prevalence of Parkinson’s Disease across North America. NPJ Park. Dis. 2018, 4, 21. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Hamilton, J.L.; Kopil, C.; Beck, J.C.; Tanner, C.M.; Albin, R.L.; Ray Dorsey, E.; Dahodwala, N.; Cintina, I.; Hogan, P.; et al. Current and Projected Future Economic Burden of Parkinson’s Disease in the U.S. NPJ Park. Dis. 2020, 6, 15. [Google Scholar] [CrossRef] [PubMed]
- Rissardo, J.P.; Caprara, A.L.F.; Durante, Í. Risk Factors for Parkinson’s Disease Depression. Ann. Mov. Disord. 2022, 5, 134–136. [Google Scholar]
- Schröter, N.; van Eimeren, T.; Classen, J.; Levin, J.; Redecker, C.; Wolz, M.; Tönges, L. Significance of Clinical Symptoms and Red Flags in Early Differential Diagnosis of Parkinson’s Disease and Atypical Parkinsonian Syndromes. J. Neural. Transm. 2023, 130, 839–846. [Google Scholar] [CrossRef]
- Rissardo, J.P.; Caprara, A.L.F. Predictors of Drug-Induced Parkinsonism. APIK J. Int. Med. 2023, 11, 270–271. [Google Scholar] [CrossRef]
- Postuma, R.B.; Berg, D.; Stern, M.; Poewe, W.; Olanow, C.W.; Oertel, W.; Obeso, J.; Marek, K.; Litvan, I.; Lang, A.E.; et al. MDS Clinical Diagnostic Criteria for Parkinson’s Disease. Mov. Disord. 2015, 30, 1591–1601. [Google Scholar] [CrossRef]
- Wang, X.-Y.; Han, Y.-Y.; Li, G.; Zhang, B. Association between Autonomic Dysfunction and Olfactory Dysfunction in Parkinson’s Disease in Southern Chinese. BMC Neurol. 2019, 19, 17. [Google Scholar] [CrossRef]
- Nakajima, K.; Yoshita, M.; Matsuo, S.; Taki, J.; Kinuya, S. Iodine-123-MIBG Sympathetic Imaging in Lewy-Body Diseases and Related Movement Disorders. Q. J. Nucl. Med. Mol. Imaging 2008, 52, 378–387. [Google Scholar]
- Iellamo, F.; Perrone, M.A.; Cimini, A.; Caminiti, G.; Chiaravalloti, A.; Parisi, A.; Schillaci, O. Complementary Role of Combined Indirect and Direct Cardiac Sympathetic (Hyper)Activity Assessment in Patients with Heart Failure by Spectral Analysis of Heart Rate Variability and Nuclear Imaging: Possible Application in the Evaluation of Exercise Training Effects. J. Cardiovasc. Dev. Dis. 2022, 9, 181. [Google Scholar]
- De Feo, M.S.; Frantellizzi, V.; Locuratolo, N.; Di Rocco, A.; Farcomeni, A.; Pauletti, C.; Marongiu, A.; Lazri, J.; Nuvoli, S.; Fattapposta, F.; et al. Role of Functional Neuroimaging with 123I-MIBG and 123I-FP-CIT in De Novo Parkinson’s Disease: A Multicenter Study. Life 2023, 13, 1786. [Google Scholar] [CrossRef]
- Hakusui, S.; Yasuda, T.; Yanagi, T.; Tohyama, J.; Hasegawa, Y.; Koike, Y.; Hirayama, M.; Takahashi, A. A Radiological Analysis of Heart Sympathetic Functions with Meta-[123I]Iodobenzylguanidine in Neurological Patients with Autonomic Failure. J. Auton. Nerv. Syst. 1994, 49, 81–84. [Google Scholar] [CrossRef] [PubMed]
- Vallabhajosula, S.; Nikolopoulou, A. Radioiodinated Metaiodobenzylguanidine (MIBG): Radiochemistry, Biology, and Pharmacology. Semin. Nucl. Med. 2011, 41, 324–333. [Google Scholar] [CrossRef] [PubMed]
- Pandit-Taskar, N.; Modak, S. Norepinephrine Transporter as a Target for Imaging and Therapy. J. Nucl. Med. 2017, 58, 39–53. [Google Scholar] [CrossRef] [PubMed]
- Lashford, L.S.; Hancock, J.P.; Kemshead, J.T. Meta-Iodobenzylguanidine (MIBG) Uptake and Storage in the Human Neuroblastoma Cell Line SK-N-BE(2C). Int. J. Cancer 1991, 47, 105–109. [Google Scholar] [CrossRef]
- Mangner, T.J.; Tobes, M.C.; Wieland, D.W.; Sisson, J.C.; Shapiro, B. Metabolism of Iodine-131 Metaiodobenzylguanidine in Patients with Metastatic Pheochromocytoma. J. Nucl. Med. 1986, 27, 37–44. [Google Scholar]
- Sakata, K.; Shirotani, M.; Yoshida, H.; Kurata, C. Physiological Fluctuation of the Human Left Ventricle Sympathetic Nervous System Assessed by Iodine-123-MIBG. J. Nucl. Med. 1998, 39, 1667–1671. [Google Scholar]
- Agrawal, A.; Rangarajan, V.; Shah, S.; Puranik, A.; Purandare, N. MIBG (Metaiodobenzylguanidine) Theranostics in Pediatric and Adult Malignancies. Br. J. Radiol. 2018, 91, 20180103. [Google Scholar] [CrossRef]
- Shulkin, B.L.; Shapiro, B. Current Concepts on the Diagnostic Use of MIBG in Children. J. Nucl. Med. 1998, 39, 679–688. [Google Scholar]
- Van Vickle, S.S.; Thompson, R.C. 123I-MIBG Imaging: Patient Preparation and Technologist’s Role. J. Nucl. Med. Technol. 2015, 43, 82–86. [Google Scholar] [CrossRef]
- Solanki, K.K.; Bomanji, J.; Moyes, J.; Mather, S.J.; Trainer, P.J.; Britton, K.E. A Pharmacological Guide to Medicines Which Interfere with the Biodistribution of Radiolabelled Meta-Iodobenzylguanidine (MIBG). Nucl. Med. Commun. 1992, 13, 513–521. [Google Scholar] [CrossRef]
- Kishi, M.; Sakakibara, R.; Terada, H.; Ogawa, E.; Tateno, T. Does Levodopa Affect Metaiodobenzylguanidine Myocardial Accumulation in Parkinson’s Disease? Mov. Disord. 2011, 26, 563–564. [Google Scholar] [CrossRef] [PubMed]
- Sakakibara, R.; Tateno, F.; Kishi, M.; Tsuyusaki, Y.; Terada, H.; Inaoka, T. MIBG Myocardial Scintigraphy in Pre-Motor Parkinson’s Disease: A Review. Park. Relat. Disord. 2014, 20, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Lode, H.N.; Bruchelt, G.; Seitz, G.; Gebhardt, S.; Gekeler, V.; Niethammer, D.; Beck, J. Reverse Transcriptase-Polymerase Chain Reaction (RT-PCR) Analysis of Monoamine Transporters in Neuroblastoma Cell Lines: Correlations to Meta-Iodobenzylguanidine (MIBG) Uptake and Tyrosine Hydroxylase Gene Expression. Eur. J. Cancer 1995, 31A, 586–590. [Google Scholar] [CrossRef] [PubMed]
- Adaniya, S.; Takahashi, M.; Koyama, K.; Ogane, K.; Momose, T. Influence of Antidepressant Use on 123I-MIBG Heart and Lung Uptakes in the Diagnosis of Lewy Body Disease. Ann. Nucl. Med. 2022, 36, 488–494. [Google Scholar] [CrossRef] [PubMed]
- Asghar, O.; Arumugam, P.; Armstrong, I.; Ray, S.; Schmitt, M.; Malik, R.A. Iodine-123 Metaiodobenzylguanidine Scintigraphy for the Assessment of Cardiac Sympathetic Innervation and the Relationship with Cardiac Autonomic Function in Healthy Adults Using Standardized Methods. Nucl. Med. Commun. 2017, 38, 44–50. [Google Scholar] [CrossRef]
- Sze, W.C.C.; Grossman, A.B.; Goddard, I.; Amendra, D.; Shieh, S.C.C.; Plowman, P.N.; Drake, W.M.; Akker, S.A.; Druce, M.R. Sequelae and Survivorship in Patients Treated with 131I-MIBG Therapy. Br. J. Cancer 2013, 109, 565–572. [Google Scholar] [CrossRef]
- Xu, D.; Zhu, W.; Huo, L.; Zhu, S.; Li, F.; Wang, H. Validation of Iodine-131-Meta-Iodobenzylguanidine Cardiac Scintigraphy in Parkinsonism: A Preliminary Study. Park. Relat. Disord. 2018, 50, 69–73. [Google Scholar] [CrossRef]
- Nakajima, K.; Scholte, A.J.H.A.; Nakata, T.; Dimitriu-Leen, A.C.; Chikamori, T.; Vitola, J.V.; Yoshinaga, K. Cardiac Sympathetic Nervous System Imaging with 123I-Meta-Iodobenzylguanidine: Perspectives from Japan and Europe. J. Nucl. Cardiol. 2017, 24, 952–960. [Google Scholar] [CrossRef]
- Verschure, D.O.; Nakajima, K.; Verberne, H.J. Cardiac 123I-MIBG Imaging in Heart Failure. Pharmaceuticals 2022, 15, 656. [Google Scholar] [CrossRef]
- Salerno, M.; Beller, G.A. Noninvasive Assessment of Myocardial Perfusion. Circ. Cardiovasc. Imaging 2009, 2, 412–424. [Google Scholar] [CrossRef]
- Frantellizzi, V.; Ricci, M.; Farcomeni, A.; Pontico, M.; Pani, A.; Vincentis, G.D. Usefulness of 5 Minutes 123I-MIBG Scan in Parkinson’s Disease and Heart Failure. Curr. Radiopharm. 2020, 13, 120–129. [Google Scholar] [CrossRef] [PubMed]
- Chun, I.K. Optimal Protocol and Clinical Usefulness of 123I-MIBG Cardiac Scintigraphy for Differentiation of Parkinson’s Disease and Dementia with Lewy Body from Non-Parkinson’s Diseases. Nucl. Med. Mol. Imaging 2023, 57, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Spiegel, J. Diagnostic and Pathophysiological Impact of Myocardial MIBG Scintigraphy in Parkinson’s Disease. Park. Dis. 2010, 2010, 295346. [Google Scholar] [CrossRef] [PubMed]
- Peix, A.; Mesquita, C.T.; Paez, D.; Pereira, C.C.; Felix, R.; Gutierrez, C.; Jaimovich, R.; Ianni, B.M.; Soares, J.J.; Olaya, P.; et al. Nuclear Medicine in the Management of Patients with Heart Failure: Guidance from an Expert Panel of the International Atomic Energy Agency (IAEA). Nucl. Med. Commun. 2014, 35, 818–823. [Google Scholar] [CrossRef]
- Jeong, Y.J.; Jeong, J.E.; Cheon, S.M.; Yoon, B.A.; Kim, J.W.; Kang, D.Y. Relationship between the Washout Rate of I-123 MIBG Scans and Autonomic Function in Parkinson’s Disease. PLoS ONE 2020, 15, e0229860. [Google Scholar] [CrossRef]
- van Santen, H.M.; de Kraker, J.; van Eck, B.L.F.; de Vijlder, J.J.M.; Vulsma, T. Improved Radiation Protection of the Thyroid Gland with Thyroxine, Methimazole, and Potassium Iodide during Diagnostic and Therapeutic Use of Radiolabeled Metaiodobenzylguanidine in Children with Neuroblastoma. Cancer 2003, 98, 389–396. [Google Scholar] [CrossRef]
- Chung, E.J.; Kim, S.J. 123I-Metaiodobenzylguanidine Myocardial Scintigraphy in Lewy Body-Related Disorders: A Literature Review. J. Mov. Disord. 2015, 8, 55–66. [Google Scholar] [CrossRef]
- Haqparwar, J.; Pepe, A.; Fassbender, K.; Dillmann, U.; Ezziddin, S.; Schaefer, A.; Leppert, D.; Spiegel, J. Reduced MIBG Accumulation of the Parotid and Submandibular Glands in Idiopathic Parkinson’s Disease. Park. Relat. Disord. 2017, 34, 26–30. [Google Scholar] [CrossRef]
- Li, S.; Yue, L.; Chen, S.; Wu, Z.; Zhang, J.; Hong, R.; Xie, L.; Peng, K.; Wang, C.; Lin, A.; et al. High Clinical Diagnostic Accuracy of Combined Salivary Gland and Myocardial Metaiodobenzylguanidine Scintigraphy in the Diagnosis of Parkinson’s Disease. Front. Aging Neurosci. 2022, 14, 1066331. [Google Scholar] [CrossRef]
- Jang, W.; Kim, J.S.; Cho, J.W.; Ahn, J.Y.; Choi, Y.Y.; Kim, H.T. Thyroid MIBG Uptake in Parkinson’s Disease with Diabetes Mellitus. Clin. Auton. Res. 2013, 23, 221–224. [Google Scholar] [CrossRef]
- Clement, S.C.; Tytgat, G.A.; van Trotsenburg, A.S.; Kremer, L.C.; van Santen, H.M. Thyroid Function after Diagnostic 123I-Metaiodobenzylguanidine in Children with Neuroblastic Tumors. Ann. Nucl. Med. 2022, 36, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, G.A. The Innervation of the Heart. Br. Heart J. 1953, 15, 159–171. [Google Scholar] [CrossRef] [PubMed]
- Burke, R.E.; Dauer, W.T.; Vonsattel, J.P. A Critical Evaluation of the Braak Staging Scheme for Parkinson’s Disease. Ann. Neurol. 2008, 64, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Mantri, S.; Morley, J.F.; Siderowf, A.D. The Importance of Preclinical Diagnostics in Parkinson Disease. Park. Relat. Disord. 2019, 64, 20–28. [Google Scholar] [CrossRef]
- Mitsui, J.; Saito, Y.; Momose, T.; Shimizu, J.; Arai, N.; Shibahara, J.; Ugawa, Y.; Kanazawa, I.; Tsuji, S.; Murayama, S. Pathology of the Sympathetic Nervous System Corresponding to the Decreased Cardiac Uptake in 123I-Metaiodobenzylguanidine (MIBG) Scintigraphy in a Patient with Parkinson Disease. J. Neurol. Sci. 2006, 243, 101–104. [Google Scholar] [CrossRef]
- Watanabe, H.; Sobue, G. Filling in the Missing Puzzle Piece between Cardiac MIBG Scintigraphy Findings and Parkinson’s Disease Pathology. J. Neurol. Neurosurg. Psychiatry 2015, 86, 937. [Google Scholar] [CrossRef]
- Nakamura, T.; Hirayama, M.; Ito, H.; Takamori, M.; Hamada, K.; Takeuchi, S.; Watanabe, H.; Koike, Y.; Sobue, G. Dobutamine Stress Test Unmasks Cardiac Sympathetic Denervation in Parkinson’s Disease. J. Neurol. Sci. 2007, 263, 133–138. [Google Scholar] [CrossRef]
- Nakamura, T.; Hirayama, M.; Yamashita, F.; Uchida, K.; Hama, T.; Watanabe, H.; Sobue, G. Lowered Cardiac Sympathetic Nerve Performance in Response to Exercise in Parkinson’s Disease. Mov. Disord. 2010, 25, 1183–1189. [Google Scholar] [CrossRef]
- Takahashi, M.; Ikemura, M.; Oka, T.; Uchihara, T.; Wakabayashi, K.; Kakita, A.; Takahashi, H.; Yoshida, M.; Toru, S.; Kobayashi, T.; et al. Quantitative Correlation between Cardiac MIBG Uptake and Remaining Axons in the Cardiac Sympathetic Nerve in Lewy Body Disease. J. Neurol. Neurosurg. Psychiatry 2015, 86, 939–944. [Google Scholar] [CrossRef]
- Lamotte, G.; Goldstein, D.S. What New Can We Learn from Cardiac Sympathetic Neuroimaging in Synucleinopathies? Clin. Auton. Res. 2022, 32, 95–98. [Google Scholar] [CrossRef]
- Kikuchi, K.; Hiwatashi, A.; Togao, O.; Yamashita, K.; Somehara, R.; Kamei, R.; Baba, S.; Yamaguchi, H.; Kira, J.I.; Honda, H. Structural Changes in Parkinson’s Disease: Voxel-Based Morphometry and Diffusion Tensor Imaging Analyses Based on 123I-MIBG Uptake. Eur. Radiol. 2017, 27, 5073–5079. [Google Scholar] [CrossRef] [PubMed]
- Park, D.G.; Kang, J.; An, Y.-S.; Chang, J.; Yoon, J.H. Association of Plasma α-Synuclein with Cardiac 123I-MIBG Scintigraphy in Early Parkinson’s Disease. Neurosci. Lett. 2022, 770, 136399. [Google Scholar] [CrossRef]
- Yamada, M.; Komatsu, J.; Nakamura, K.; Sakai, K.; Samuraki-Yokohama, M.; Nakajima, K.; Yoshita, M. Diagnostic Criteria for Dementia with Lewy Bodies: Updates and Future Directions. J. Mov. Disord. 2020, 13, 1–10. [Google Scholar] [CrossRef]
- Politis, M.; Niccolini, F. Serotonin in Parkinson’s Disease. Behav. Brain Res. 2015, 277, 136–145. [Google Scholar] [CrossRef] [PubMed]
- Politis, M.; Loane, C. Serotonergic Dysfunction in Parkinson’s Disease and Its Relevance to Disability. Sci. World J. 2011, 11, 1726–1734. [Google Scholar] [CrossRef] [PubMed]
- Murakami, H.; Yamamoto, K.; Yasumoto, T.; Kimura, A.; Sakae, Y.; Nomoto, S.; Kubota, S.; Watanabe, D.; Watanabe, K.; Saito, Y.; et al. Cerebrospinal Fluid 5-HIAA Concentrations Correlate with Cardiac Uptake of 123I-MIBG during Myocardial Scintigraphy in Drug Naïve Parkinson’s Disease. J. Neural. Transm. 2018, 125, 1511–1514. [Google Scholar] [CrossRef]
- Hughes, A.J.; Daniel, S.E.; Kilford, L.; Lees, A.J. Accuracy of Clinical Diagnosis of Idiopathic Parkinson’s Disease: A Clinico-Pathological Study of 100 Cases. J. Neurol. Neurosurg. Psychiatry 1992, 55, 181–184. [Google Scholar] [CrossRef]
- Kawazoe, M.; Arima, H.; Maeda, T.; Tsuji, M.; Mishima, T.; Fujioka, S.; Tsugawa, J.; Tsuboi, Y. Sensitivity and Specificity of Cardiac 123I-MIBG Scintigraphy for Diagnosis of Early-Phase Parkinson’s Disease. J. Neurol. Sci. 2019, 407, 116409. [Google Scholar] [CrossRef]
- Wang, T.; Wu, K.Y.; Miner, R.C.; Renaud, J.M.; Beanlands, R.S.B.; deKemp, R.A. Reproducible Quantification of Cardiac Sympathetic Innervation Using Graphical Modeling of Carbon-11-Meta-Hydroxyephedrine Kinetics with Dynamic PET-CT Imaging. EJNMMI Res. 2018, 8, 63. [Google Scholar] [CrossRef]
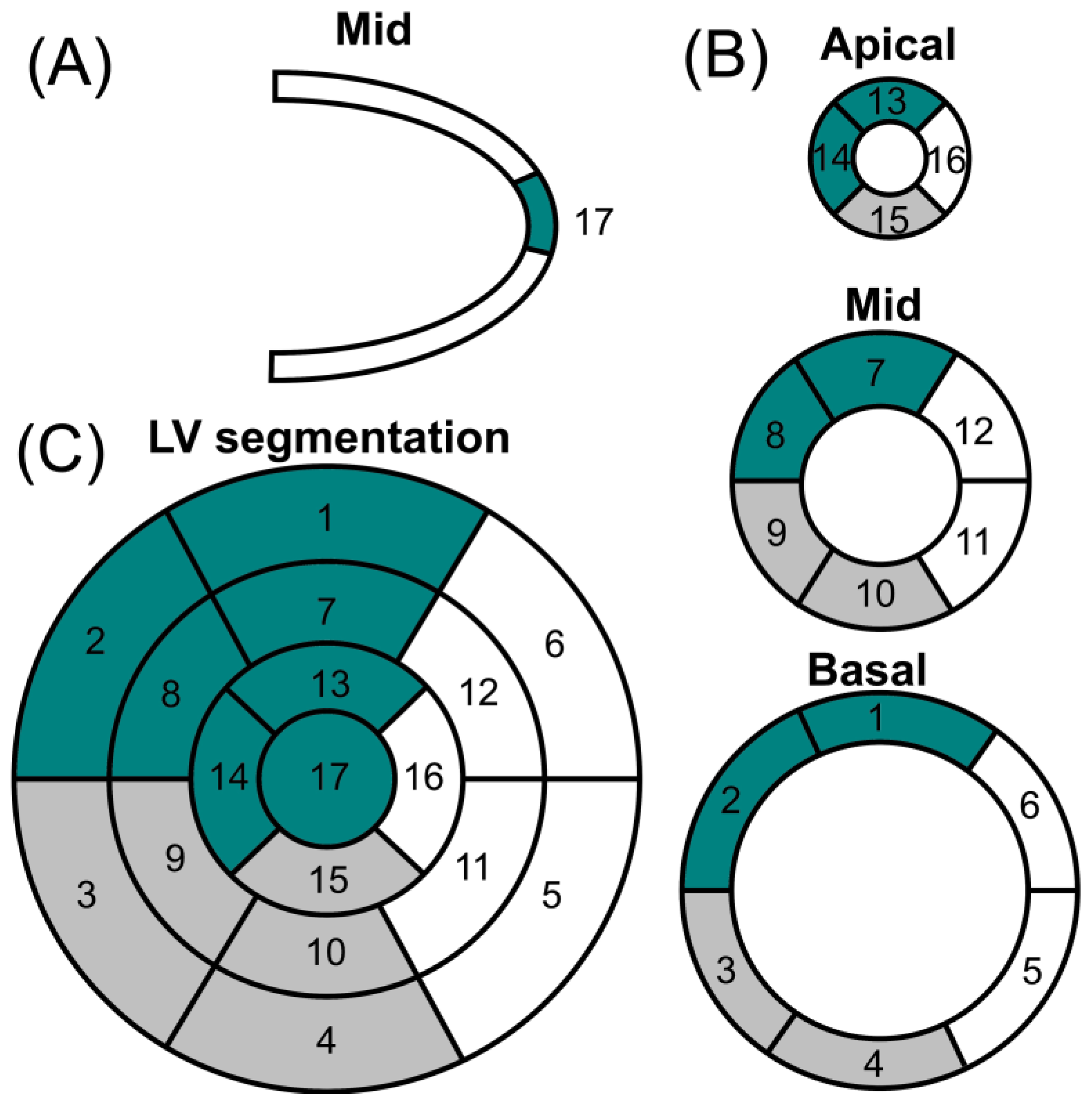
- Kwon, S.H.; Yoon, J.-K.; Yoon, J.H.; Lee, S.J.; Jo, K.S.; Lee, D.H.; An, Y.-S. The Utility of Segmental Analysis in Cardiac I-123 MIBG SPECT in Parkinson’s Disease. Nucl. Med. Mol. Imaging 2015, 49, 298–302. [Google Scholar] [CrossRef]
- Courbon, F.; Brefel-Courbon, C.; Thalamas, C.; Alibelli, M.-J.; Berry, I.; Montastruc, J.-L.; Rascol, O.; Senard, J.-M. Cardiac MIBG Scintigraphy Is a Sensitive Tool for Detecting Cardiac Sympathetic Denervation in Parkinson’s Disease. Mov. Disord. 2003, 18, 890–897. [Google Scholar] [CrossRef] [PubMed]
- Somsen, G.A.; Verberne, H.J.; Fleury, E.; Righetti, A. Normal Values and Within-Subject Variability of Cardiac I-123 MIBG Scintigraphy in Healthy Individuals: Implications for Clinical Studies. J. Nucl. Cardiol. 2004, 11, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Eckhardt, C.; Krismer, F.; Donnemiller, E.; Eschlböck, S.; Fanciulli, A.; Raccagni, C.; Bösch, S.; Mair, K.; Scherfler, C.; Djamshidian, A.; et al. Cardiac Sympathetic Innervation in Parkinson’s Disease versus Multiple System Atrophy. Clin. Auton. Res. 2022, 32, 103–114. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, D.S.; Holmes, C.S.; Dendi, R.; Bruce, S.R.; Li, S.T. Orthostatic Hypotension from Sympathetic Denervation in Parkinson’s Disease. Neurology 2002, 58, 1247–1255. [Google Scholar] [CrossRef]
- Wong, K.K.; Raffel, D.M.; Koeppe, R.A.; Frey, K.A.; Bohnen, N.I.; Gilman, S. Pattern of Cardiac Sympathetic Denervation in Idiopathic Parkinson Disease Studied with 11C Hydroxyephedrine PET. Radiology 2012, 265, 240–247. [Google Scholar] [CrossRef]
- Katagiri, A.; Asahina, M.; Araki, N.; Poudel, A.; Fujinuma, Y.; Yamanaka, Y.; Kuwabara, S. Myocardial 123I-MIBG Uptake and Cardiovascular Autonomic Function in Parkinson’s Disease. Park. Dis. 2015, 2015, 805351. [Google Scholar]
- Goetz, C.G.; Poewe, W.; Rascol, O.; Sampaio, C.; Stebbins, G.T.; Counsell, C.; Giladi, N.; Holloway, R.G.; Moore, C.G.; Wenning, G.K.; et al. Movement Disorder Society Task Force Report on the Hoehn and Yahr Staging Scale: Status and Recommendations. Mov. Disord. 2004, 19, 1020–1028. [Google Scholar] [CrossRef]
- Yoshita, M. Differentiation of Idiopathic Parkinson’s Disease from Striatonigral Degeneration and Progressive Supranuclear Palsy Using Iodine-123 Meta-Iodobenzylguanidine Myocardial Scintigraphy. J. Neurol. Sci. 1998, 155, 60–67. [Google Scholar] [CrossRef]
- Braune, S.; Reinhardt, M.; Bathmann, J.; Krause, T.; Lehmann, M.; Lücking, C.H. Impaired Cardiac Uptake of Meta-[123I]Iodobenzylguanidine in Parkinson’s Disease with Autonomic Failure. Acta Neurol. Scand. 1998, 97, 307–314. [Google Scholar] [CrossRef]
- Iwasa, K.; Nakajima, K.; Yoshikawa, H.; Tada, A.; Taki, J.; Takamori, M. Decreased Myocardial 123I-MIBG Uptake in Parkinson’s Disease. Acta Neurol. Scand. 1998, 97, 303–306. [Google Scholar] [CrossRef]
- Braune, S.; Reinhardt, M.; Schnitzer, R.; Riedel, A.; Lücking, C.H. Cardiac Uptake of [123I]MIBG Separates Parkinson’s Disease from Multiple System Atrophy. Neurology 1999, 53, 1020–1025. [Google Scholar] [CrossRef] [PubMed]
- Orimo, S.; Ozawa, E.; Nakade, S.; Sugimoto, T.; Mizusawa, H. 123I-Metaiodobenzylguanidine Myocardial Scintigraphy in Parkinson’s Disease. J. Neurol. Neurosurg. Psychiatry 1999, 67, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Druschky, A.; Hilz, M.J.; Platsch, G.; Radespiel-Tröger, M.; Druschky, K.; Kuwert, T.; Neundörfer, B. Differentiation of Parkinson’s Disease and Multiple System Atrophy in Early Disease Stages by Means of I-123-MIBG-SPECT. J. Neurol. Sci. 2000, 175, 3–12. [Google Scholar] [CrossRef]
- Taki, J.; Nakajima, K.; Hwang, E.H.; Matsunari, I.; Komai, K.; Yoshita, M.; Sakajiri, K.; Tonami, N. Peripheral Sympathetic Dysfunction in Patients with Parkinson’s Disease without Autonomic Failure Is Heart Selective and Disease Specific. Eur. J. Nucl. Med. 2000, 27, 566–573. [Google Scholar] [CrossRef] [PubMed]
- Reinhardt, M.J.; Jüngling, F.D.; Krause, T.M.; Braune, S. Scintigraphic Differentiation between Two Forms of Primary Dysautonomia Early after Onset of Autonomic Dysfunction: Value of Cardiac and Pulmonary Iodine-123 MIBG Uptake. Eur. J. Nucl. Med. 2000, 27, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Takatsu, H.; Nishida, H.; Matsuo, H.; Watanabe, S.; Nagashima, K.; Wada, H.; Noda, T.; Nishigaki, K.; Fujiwara, H. Cardiac Sympathetic Denervation from the Early Stage of Parkinson’s Disease: Clinical and Experimental Studies with Radiolabeled MIBG. J. Nucl. Med. 2000, 41, 71–77. [Google Scholar]
- Hamada, K.; Hirayama, M.; Watanabe, H.; Kobayashi, R.; Ito, H.; Ieda, T.; Koike, Y.; Sobue, G. Onset Age and Severity of Motor Impairment Are Associated with Reduction of Myocardial 123I-MIBG Uptake in Parkinson’s Disease. J. Neurol. Neurosurg. Psychiatry 2003, 74, 423–426. [Google Scholar] [CrossRef]
- Orimo, S.; Ozawa, E.; Nakade, S.; Hattori, H.; Tsuchiya, K.; Taki, K.; Takahashi, A. [123I] Meta-Iodobenzylguanidine Myocardial Scintigraphy Differentiates Corticobasal Degeneration from Parkinson’s Disease. Intern. Med. 2003, 42, 127–128. [Google Scholar] [CrossRef]
- Saiki, S.; Hirose, G.; Sakai, K.; Kataoka, S.; Hori, A.; Saiki, M.; Kaito, M.; Higashi, K.; Taki, S.; Kakeshita, K.; et al. Cardiac 123I-MIBG Scintigraphy Can Assess the Disease Severity and Phenotype of PD. J. Neurol. Sci. 2004, 220, 105–111. [Google Scholar] [CrossRef]
- Nagayama, H.; Hamamoto, M.; Ueda, M.; Nagashima, J.; Katayama, Y. Reliability of MIBG Myocardial Scintigraphy in the Diagnosis of Parkinson’s Disease. J. Neurol. Neurosurg. Psychiatry 2005, 76, 249–251. [Google Scholar] [CrossRef]
- Kashihara, K.; Ohno, M.; Kawada, S.; Okumura, Y. Reduced Cardiac Uptake and Enhanced Washout of 123I-MIBG in Pure Autonomic Failure Occurs Conjointly with Parkinson’s Disease and Dementia with Lewy Bodies. J. Nucl. Med. 2006, 47, 1099–1101. [Google Scholar]
- Kim, J.S.; Lee, P.H.; Lee, K.S.; Park, J.W.; Kim, Y.I.; Chung, Y.A.; Kim, S.H.; Kim, S.H.; Kim, J.; Choi, Y.Y.; et al. Cardiac [123I]Metaiodobenzylguanidine Scintigraphy for Vascular Parkinsonism. Mov. Disord. 2006, 21, 1990–1994. [Google Scholar] [CrossRef] [PubMed]
- Lee, P.H.; Kim, J.W.; Bang, O.Y.; Joo, I.S.; Yoon, S.-N.; Huh, K. Cardiac 123I-MIBG Scintigraphy in Patients with Essential Tremor. Mov. Disord. 2006, 21, 1235–1238. [Google Scholar] [CrossRef] [PubMed]
- Miyamoto, T.; Miyamoto, M.; Inoue, Y.; Usui, Y.; Suzuki, K.; Hirata, K. Reduced Cardiac 123I-MIBG Scintigraphy in Idiopathic REM Sleep Behavior Disorder. Neurology 2006, 67, 2236–2238. [Google Scholar] [CrossRef] [PubMed]
- Shin, D.H.; Lee, P.H.; Bang, O.Y.; Joo, I.S.; Huh, K. Clinical Implications of Cardiac-MIBG SPECT in the Differentiation of Parkinsonian Syndromes. J. Clin. Neurol. 2006, 2, 51–57. [Google Scholar] [CrossRef]
- Köllensperger, M.; Seppi, K.; Liener, C.; Boesch, S.; Heute, D.; Mair, K.J.; Mueller, J.; Sawires, M.; Scherfler, C.; Schocke, M.F.; et al. Diffusion Weighted Imaging Best Discriminates PD from MSA-P: A Comparison with Tilt Table Testing and Heart MIBG Scintigraphy. Mov. Disord. 2007, 22, 1771–1776. [Google Scholar] [CrossRef]
- Spiegel, J.; Hellwig, D.; Farmakis, G.; Jost, W.H.; Samnick, S.; Fassbender, K.; Kirsch, C.-M.; Dillmann, U. Myocardial Sympathetic Degeneration Correlates with Clinical Phenotype of Parkinson’s Disease. Mov. Disord. 2007, 22, 1004–1008. [Google Scholar] [CrossRef]
- Miyamoto, T.; Miyamoto, M.; Suzuki, K.; Nishibayashi, M.; Iwanami, M.; Hirata, K. 123I-MIBG Cardiac Scintigraphy Provides Clues to the Underlying Neurodegenerative Disorder in Idiopathic REM Sleep Behavior Disorder. Sleep 2008, 31, 717–723. [Google Scholar] [CrossRef]
- Chung, E.J.; Lee, W.Y.; Yoon, W.T.; Kim, B.J.; Lee, G.H. MIBG Scintigraphy for Differentiating Parkinson’s Disease with Autonomic Dysfunction from Parkinsonism-Predominant Multiple System Atrophy. Mov. Disord. 2009, 24, 1650–1655. [Google Scholar] [CrossRef]
- Novellino, F.; Arabia, G.; Bagnato, A.; Cascini, G.L.; Salsone, M.; Nicoletti, G.; Messina, D.; Morelli, M.; Paglionico, S.; Giofrè, L.; et al. Combined Use of DAT-SPECT and Cardiac MIBG Scintigraphy in Mixed Tremors. Mov. Disord. 2009, 24, 2242–2248. [Google Scholar] [CrossRef]
- Sawada, H.; Oeda, T.; Yamamoto, K.; Kitagawa, N.; Mizuta, E.; Hosokawa, R.; Ohba, M.; Nishio, R.; Yamakawa, K.; Takeuchi, H.; et al. Diagnostic Accuracy of Cardiac Metaiodobenzylguanidine Scintigraphy in Parkinson Disease. Eur. J. Neurol. 2009, 16, 174–182. [Google Scholar] [CrossRef] [PubMed]
- Fröhlich, I.; Pilloy, W.; Vaillant, M.; Diederich, N.J. Myocardial MIBG Scintigraphy: A Useful Clinical Tool?: A Retrospective Study in 50 Parkinsonian Patients. Neurol. Sci. 2010, 31, 403–406. [Google Scholar] [CrossRef] [PubMed]
- Ishibashi, K.; Saito, Y.; Murayama, S.; Kanemaru, K.; Oda, K.; Ishiwata, K.; Mizusawa, H.; Ishii, K. Validation of Cardiac 123I-MIBG Scintigraphy in Patients with Parkinson’s Disease Who Were Diagnosed with Dopamine PET. Eur. J. Nucl. Med. Mol. Imaging 2010, 37, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Izawa, M.O.; Miwa, H.; Kajimoto, Y.; Kondo, T. Combination of Transcranial Sonography, Olfactory Testing, and MIBG Myocardial Scintigraphy as a Diagnostic Indicator for Parkinson’s Disease. Eur. J. Neurol. 2012, 19, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Kikuchi, A.; Baba, T.; Hasegawa, T.; Sugeno, N.; Konno, M.; Takeda, A. Differentiating Parkinson’s Disease from Multiple System Atrophy by [123I] Meta-Iodobenzylguanidine Myocardial Scintigraphy and Olfactory Test. Park. Relat. Disord. 2011, 17, 698–700. [Google Scholar] [CrossRef]
- Kurata, T.; Kametaka, S.; Ohta, Y.; Morimoto, N.; Deguchi, S.; Deguchi, K.; Ikeda, Y.; Takao, Y.; Ohta, T.; Manabe, Y.; et al. PSP as Distinguished from CBD, MSA-P and PD by Clinical and Imaging Differences at an Early Stage. Intern. Med. 2011, 50, 2775–2781. [Google Scholar] [CrossRef]
- Muxí, A.; Paredes, P.; Navales, I.; Valldeoriola, F.; Gaig, C.; Lomeña, F.; de la Cerda, A.; Solà, O.; Domenech, B.; Tolosa, E.; et al. Diagnostic Cutoff Points for 123I-MIBG Myocardial Scintigraphy in a Caucasian Population with Parkinson’s Disease. Eur. J. Nucl. Med. Mol. Imaging 2011, 38, 1139–1146. [Google Scholar] [CrossRef]
- Südmeyer, M.; Antke, C.; Zizek, T.; Beu, M.; Nikolaus, S.; Wojtecki, L.; Schnitzler, A.; Müller, H.-W. Diagnostic Accuracy of Combined FP-CIT, IBZM, and MIBG Scintigraphy in the Differential Diagnosis of Degenerative Parkinsonism: A Multidimensional Statistical Approach. J. Nucl. Med. 2011, 52, 733–740. [Google Scholar] [CrossRef]
- Behnke, S.; Hellwig, D.; Bürmann, J.; Runkel, A.; Farmakis, G.; Kirsch, C.M.; Fassbender, K.; Becker, G.; Dillmann, U.; Spiegel, J. Evaluation of Transcranial Sonographic Findings and MIBG Cardiac Scintigraphy in the Diagnosis of Idiopathic Parkinson’s Disease. Park. Relat. Disord. 2013, 19, 995–999. [Google Scholar] [CrossRef]
- Chiaravalloti, A.; Stefani, A.; Di Biagio, D.; Pierantozzi, M.; Tavolozza, M.; Di Pietro, B.; Stanzione, P.; Schillaci, O. Cardiac Sympathetic Denervation Is Not Related to Nigrostriatal Degeneration in Parkinson’s Disease. Ann. Nucl. Med. 2013, 27, 444–451. [Google Scholar] [CrossRef]
- Umemura, A.; Oeda, T.; Hayashi, R.; Tomita, S.; Kohsaka, M.; Yamamoto, K.; Sawada, H. Diagnostic Accuracy of Apparent Diffusion Coefficient and 123I-Metaiodobenzylguanidine for Differentiation of Multiple System Atrophy and Parkinson’s Disease. PLoS ONE 2013, 8, e61066. [Google Scholar] [CrossRef]
- Leite, M.A.A.; Nascimento, O.J.M.; Pereira, J.S.; Amaral, C.; Mesquita, C.T.; Azevedo, J.C.; de Brito, A.S.X.; Pedras, F.V. Cardiac 123I-MIBG Uptake in de Novo Brazilian Patients with Parkinson’s Disease without Clinically Defined Dysautonomia. Arq. Neuropsiquiatr. 2014, 72, 430–434. [Google Scholar] [CrossRef]
- Mochizuki, H.; Ebihara, Y.; Ugawa, Y.; Ishii, N.; Taniguchi, A.; Nagamachi, S.; Shiomi, K.; Nakazato, M. PR Prolongation and Cardiac 123I-MIBG Uptake Reduction in Parkinson’s Disease. Eur. Neurol. 2015, 74, 107–111. [Google Scholar] [CrossRef]
- Rocchi, C.; Pierantozzi, M.; Galati, S.; Chiaravalloti, A.; Pisani, V.; Prosperetti, C.; Lauretti, B.; Stampanoni Bassi, M.; Olivola, E.; Schillaci, O.; et al. Autonomic Function Tests and MIBG in Parkinson’s Disease: Correlation to Disease Duration and Motor Symptoms. CNS Neurosci. Ther. 2015, 21, 727–732. [Google Scholar] [CrossRef] [PubMed]
- Fujita, H.; Suzuki, K.; Numao, A.; Watanabe, Y.; Uchiyama, T.; Miyamoto, T.; Miyamoto, M.; Hirata, K. Usefulness of Cardiac MIBG Scintigraphy, Olfactory Testing and Substantia Nigra Hyperechogenicity as Additional Diagnostic Markers for Distinguishing between Parkinson’s Disease and Atypical Parkinsonian Syndromes. PLoS ONE 2016, 11, e0165869. [Google Scholar] [CrossRef] [PubMed]
- Uyama, N.; Otsuka, H.; Shinya, T.; Otomi, Y.; Harada, M.; Sako, W.; Izumi, Y.; Kaji, R.; Watanabe, Y.; Takashi, S.; et al. The Utility of the Combination of a SPECT Study with [123I]-FP-CIT of Dopamine Transporters and [123I]-MIBG Myocardial Scintigraphy in Differentiating Parkinson Disease from Other Degenerative Parkinsonian Syndromes. Nucl. Med. Commun. 2017, 38, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.; Wang, L.; Li, Y.; Cheng, M.; Jiao, J.; Wang, Q.; Guo, H. 131I-MIBG Myocardial Scintigraphy for Differentiation of Parkinson’s Disease from Multiple System Atrophy or Essential Tremor in Chinese Population. J. Neurol. Sci. 2017, 373, 48–51. [Google Scholar] [CrossRef] [PubMed]
- Gabilondo, I.; Llorens, V.; Rodriguez, T.; Fernández, M.; Concha, T.P.; Acera, M.; Tijero, B.; Murueta-Goyena, A.; Del Pino, R.; Cortés, J.; et al. Myocardial MIBG Scintigraphy in Genetic Parkinson’s Disease as a Model for Lewy Body Disorders. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 376–384. [Google Scholar] [CrossRef]
- Brandl, S.J.; Braune, S. Sensitivity and Specificity of Cardiac Metaiodobenzylguanidine Scintigraphy in the Early Diagnosis of Parkinson’s Disease. Clin. Auton. Res. 2019, 29, 567–574. [Google Scholar] [CrossRef]
- Skowronek, C.; Zange, L.; Lipp, A. Cardiac 123I-MIBG Scintigraphy in Neurodegenerative Parkinson Syndromes: Performance and Pitfalls in Clinical Practice. Front. Neurol. 2019, 10, 152. [Google Scholar] [CrossRef]
- Sakuramoto, H.; Fujita, H.; Suzuki, K.; Matsubara, T.; Watanabe, Y.; Hamaguchi, M.; Hirata, K. Combination of Midbrain-to-Pontine Ratio and Cardiac MIBG Scintigraphy to Differentiate Parkinson’s Disease from Multiple System Atrophy and Progressive Supranuclear Palsy. Clin. Park. Relat. Disord. 2020, 2, 20–24. [Google Scholar] [CrossRef] [PubMed]
- Brumberg, J.; Kuzkina, A.; Lapa, C.; Mammadova, S.; Buck, A.; Volkmann, J.; Sommer, C.; Isaias, I.U.; Doppler, K. Dermal and Cardiac Autonomic Fiber Involvement in Parkinson’s Disease and Multiple System Atrophy. Neurobiol. Dis. 2021, 153, 105332. [Google Scholar] [CrossRef] [PubMed]
- Jang, W.; Lee, J.Y.; Kim, J.Y.; Lee, S.J.; Kim, T.Y.; Choi, Y.Y.; Kim, H.-T.; Kim, C.K. Intrasubject Relationship between Striatal 18F-FP-CIT Uptake and Cardiac 123I-MIBG Uptake Differs by Motor Subtype in Early Parkinson Disease. Medicine 2021, 100, e26995. [Google Scholar] [CrossRef] [PubMed]
- Iwabuchi, Y.; Kameyama, M.; Matsusaka, Y.; Narimatsu, H.; Hashimoto, M.; Seki, M.; Ito, D.; Tabuchi, H.; Yamada, Y.; Jinzaki, M. A Diagnostic Strategy for Parkinsonian Syndromes Using Quantitative Indices of DAT SPECT and MIBG Scintigraphy: An Investigation Using the Classification and Regression Tree Analysis. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1833–1841. [Google Scholar] [CrossRef] [PubMed]
- Miyagi, T.; Yamazato, M.; Nakamura, T.; Tokashiki, T.; Namihira, Y.; Kokuba, K.; Ishihara, S.; Sakima, H.; Ohya, Y. Power Spectral Analysis of Heart Rate Variability Is Useful as a Screening Tool for Detecting Sympathetic and Parasympathetic Nervous Dysfunctions in Parkinson’s Disease. BMC Neurol. 2022, 22, 339. [Google Scholar] [CrossRef] [PubMed]
- Low, P.A.; Tomalia, V.A.; Park, K.-J. Autonomic Function Tests: Some Clinical Applications. J. Clin. Neurol. 2013, 9, 1–8. [Google Scholar] [CrossRef]
- Nakahara, K.; Nakane, S.; Ando, Y. Correlation of heart rate variability analysis and MIBG myocardial scintigraphy in patients with Parkinson’s disease. Amyloid 2019, 26, 146–147. [Google Scholar] [CrossRef]
- Haensch, C.-A.; Lerch, H.; Jörg, J.; Isenmann, S. Cardiac Denervation Occurs Independent of Orthostatic Hypotension and Impaired Heart Rate Variability in Parkinson’s Disease. Park. Relat. Disord. 2009, 15, 134–137. [Google Scholar] [CrossRef]
- Berganzo, K.; Tijero, B.; Somme, J.H.; Llorens, V.; Sánchez-Manso, J.C.; Low, D.; Iodice, V.; Vichayanrat, E.; Mathias, C.J.; Lezcano, E.; et al. SCOPA-AUT Scale in Different Parkinsonisms and Its Correlation with (123) I-MIBG Cardiac Scintigraphy. Park. Relat. Disord. 2012, 18, 45–48. [Google Scholar] [CrossRef]
- Manabe, Y.; Fujii, D.; Kono, S.; Sakai, Y.; Tanaka, T.; Narai, H.; Omori, N.; Imai, Y.; Abe, K. Systemic Blood Pressure Profile Correlates with Cardiac 123I-MIBG Uptake in Patients with Parkinson’s Disease. J. Neurol. Sci. 2011, 307, 153–156. [Google Scholar] [CrossRef]
- Kim, J.-S.; Park, H.-E.; Oh, Y.-S.; Lee, S.-H.; Park, J.-W.; Son, B.-C.; Lee, K.-S. Orthostatic Hypotension and Cardiac Sympathetic Denervation in Parkinson Disease Patients with REM Sleep Behavioral Disorder. J. Neurol. Sci. 2016, 362, 59–63. [Google Scholar] [CrossRef]
- Pérez, T.; Tijero, B.; Gabilondo, I.; Luna, A.; Llorens, V.; Berganzo, K.; Acera, M.; Gonzalez, A.; Sanchez-Ferro, A.; Lezcano, E.; et al. Cardiocirculatory Manifestations in Parkinson’s Disease Patients without Orthostatic Hypotension. J. Hum. Hypertens. 2015, 29, 604–609. [Google Scholar] [CrossRef] [PubMed]
- Leńska-Mieciek, M.; Derecka-Charzyńska, I.; Fiszer, U.; Królicki, L.; Kułakowski, P. Syncope and Autonomic Cardiovascular Dysfunction in Parkinson Disease. Neurol. Neurochir. Pol. 2011, 45, 335–341. [Google Scholar] [CrossRef]
- Mochizuki, H.; Taniguchi, A.; Nakazato, Y.; Ishii, N.; Ebihara, Y.; Sugiyama, T.; Shiomi, K.; Nakazato, M. Increased Body Mass Index Associated with Autonomic Dysfunction in Parkinson’s Disease. Park. Relat. Disord. 2016, 24, 129–131. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, D.S.; Cheshire, W.P.J. Beat-to-Beat Blood Pressure and Heart Rate Responses to the Valsalva Maneuver. Clin. Auton. Res. 2017, 27, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Oka, H.; Toyoda, C.; Yogo, M.; Mochio, S. Reduced Cardiac 123I-MIBG Uptake Reflects Cardiac Sympathetic Dysfunction in de Novo Parkinson’s Disease. J. Neural. Transm. 2011, 118, 1323–1327. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, M.; Nakamura, T.; Hirayama, M.; Ueda, M.; Katsuno, M.; Sobue, G. Cardiac Parasympathetic Dysfunction in the Early Phase of Parkinson’s Disease. J. Neurol. 2017, 264, 333–340. [Google Scholar] [CrossRef]
- Chung, E.J.; Kim, E.G.; Kim, M.S.; Bae, S.K.; Seog, D.H.; Oh, S.J.; Oh, M.; Kim, S.J. Differences in Myocardial Sympathetic Degeneration and the Clinical Features of the Subtypes of Parkinson’s Disease. J. Clin. Neurosci. 2011, 18, 922–925. [Google Scholar] [CrossRef]
- Chiaravalloti, A.; Stefani, A.; Tavolozza, M.; Pierantozzi, M.; Di Biagio, D.; Olivola, E.; Di Pietro, B.; Stampanoni, M.; Danieli, R.; Simonetti, G.; et al. Different Patterns of Cardiac Sympathetic Denervation in Tremor-Type Compared to Akinetic-Rigid-Type Parkinson’s Disease: Molecular Imaging with 123I-MIBG. Mol. Med. Rep. 2012, 6, 1337–1342. [Google Scholar] [CrossRef]
- Marras, C.; Rochon, P.; Lang, A.E. Predicting Motor Decline and Disability in Parkinson Disease: A Systematic Review. Arch. Neurol. 2002, 59, 1724–1728. [Google Scholar] [CrossRef]
- Aasly, J.O. Long-Term Outcomes of Genetic Parkinson’s Disease. J. Mov. Disord. 2020, 13, 81–96. [Google Scholar] [CrossRef] [PubMed]
- Kalia, L.V.; Lang, A.E.; Hazrati, L.-N.; Fujioka, S.; Wszolek, Z.K.; Dickson, D.W.; Ross, O.A.; Van Deerlin, V.M.; Trojanowski, J.Q.; Hurtig, H.I.; et al. Clinical Correlations with Lewy Body Pathology in LRRK2-Related Parkinson Disease. JAMA Neurol. 2015, 72, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Quattrone, A.; Bagnato, A.; Annesi, G.; Novellino, F.; Morgante, L.; Savettieri, G.; Zappia, M.; Tarantino, P.; Candiano, I.C.C.; Annesi, F.; et al. Myocardial 123metaiodobenzylguanidine Uptake in Genetic Parkinson’s Disease. Mov. Disord. 2008, 23, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Orimo, S.; Amino, T.; Yokochi, M.; Kojo, T.; Uchihara, T.; Takahashi, A.; Wakabayashi, K.; Takahashi, H.; Hattori, N.; Mizuno, Y. Preserved Cardiac Sympathetic Nerve Accounts for Normal Cardiac Uptake of MIBG in PARK2. Mov. Disord. 2005, 20, 1350–1353. [Google Scholar] [CrossRef]
- Tijero, B.; Gabilondo, I.; Lezcano, E.; Teran-Villagrá, N.; Llorens, V.; Ruiz-Martinez, J.; Marti-Masso, J.F.; Carmona, M.; Luquin, M.R.; Berganzo, K.; et al. Autonomic Involvement in Parkinsonian Carriers of PARK2 Gene Mutations. Park. Relat. Disord. 2015, 21, 717–722. [Google Scholar] [CrossRef]
- Ruiz-Martínez, J.; Gorostidi, A.; Goyenechea, E.; Alzualde, A.; Poza, J.J.; Rodríguez, F.; Bergareche, A.; Moreno, F.; López de Munain, A.; Martí Massó, J.F. Olfactory Deficits and Cardiac 123I-MIBG in Parkinson’s Disease Related to the LRRK2 R1441G and G2019S Mutations. Mov. Disord. 2011, 26, 2026–2031. [Google Scholar] [CrossRef]
- Valldeoriola, F.; Gaig, C.; Muxí, A.; Navales, I.; Paredes, P.; Lomeña, F.; De la Cerda, A.; Buongiorno, M.; Ezquerra, M.; Santacruz, P.; et al. 123I-MIBG Cardiac Uptake and Smell Identification in Parkinsonian Patients with LRRK2 Mutations. J. Neurol. 2011, 258, 1126–1132. [Google Scholar] [CrossRef]
- Smith, L.; Schapira, A.H.V. GBA Variants and Parkinson Disease: Mechanisms and Treatments. Cells 2022, 11, 1261. [Google Scholar] [CrossRef]
- Kim, M.S.; Park, D.G.; An, Y.S.; Yoon, J.H. Dual-Phase 18F-FP-CIT Positron Emission Tomography and Cardiac 123I-MIBG Scintigraphy of Parkinson’s Disease Patients with GBA Mutations: Evidence of the Body-First Type? Eur. J. Neurol. 2023, 30, 344–352. [Google Scholar] [CrossRef]
- Tsujikawa, K.; Hasegawa, Y.; Yokoi, S.; Yasui, K.; Nanbu, I.; Yanagi, T.; Takahashi, A. Chronological Changes of 123I-MIBG Myocardial Scintigraphy and Clinical Features of Parkinson’s Disease. J. Neurol. Neurosurg. Psychiatry 2015, 86, 945–951. [Google Scholar] [CrossRef]
- Rissardo, J.P.; Caprara, A.L.F. Risk Factors for Parkinson’s Disease Dementia. Ann. Mov. Disord. 2023. [Google Scholar]
- Kim, J.S.; Park, H.E.; Park, I.S.; Oh, Y.S.; Ryu, D.W.; Song, I.U.; Jung, Y.A.; Yoo, I.R.; Choi, H.-S.; Lee, P.H.; et al. Normal “heart” in Parkinson’s Disease: Is This a Distinct Clinical Phenotype? Eur. J. Neurol. 2017, 24, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Yoo, S.W.; Kim, J.S.; Oh, Y.S.; Ryu, D.W.; Ha, S.; Yoo, J.Y.; Lee, K.S. Cardiac Sympathetic Burden Reflects Parkinson Disease Burden, Regardless of High or Low Orthostatic Blood Pressure Changes. NPJ Park. Dis. 2021, 7, 71. [Google Scholar] [CrossRef]
- Oh, Y.S.; Kim, J.S.; Yoo, S.W.; Hwang, E.J.; Lyoo, C.H.; Lee, K.S. Striatal Dopamine Activity and Myocardial 123I-Metaiodobenzylguanidine Uptake in Early Parkinson’s Disease. Park. Relat. Disord. 2019, 63, 156–161. [Google Scholar] [CrossRef]
- Park, D.G.; Kim, J.Y.; Kim, M.S.; Kim, M.H.; An, Y.-S.; Chang, J.; Yoon, J.H. Neurofilament Light Chain and Cardiac MIBG Uptake as Predictors for Phenoconversion in Isolated REM Sleep Behavior Disorder. J. Neurol. 2023, 270, 4393–4402. [Google Scholar] [CrossRef]
- Jellinger, K.A. Multiple System Atrophy—A Clinicopathological Update. Free Neuropathol. 2020, 1, 1–17. [Google Scholar]
- Gomperts, S.N. Lewy Body Dementias: Dementia with Lewy Bodies and Parkinson Disease Dementia. Continuum 2016, 22, 435–463. [Google Scholar] [CrossRef]
- Oka, H.; Umehara, T.; Nakahara, A.; Matsuno, H. Comparisons of Cardiovascular Dysautonomia and Cognitive Impairment between de Novo Parkinson’s Disease and de Novo Dementia with Lewy Bodies. BMC Neurol. 2020, 20, 350. [Google Scholar] [CrossRef] [PubMed]
- Youn, J.; Umemoto, G.; Oh, E.; Park, J.; Jang, W.; Oh, Y.-S.; Kim, H.-T.; Cho, J.W.; Fujioka, S.; Tsuboi, Y. Cardiac Sympathetic Denervation Could Be Associated with Dysphagia in Parkinson’s Disease. Front. Neurol. 2022, 13, 1010006. [Google Scholar] [CrossRef]
- Matsui, H.; Nishinaka, K.; Oda, M.; Komatsu, K.; Kubori, T.; Udaka, F. Does Cardiac Metaiodobenzylguanidine (MIBG) Uptake in Parkinson’s Disease Correlate with Major Autonomic Symptoms? Park. Relat. Disord. 2006, 12, 284–288. [Google Scholar] [CrossRef]
- Yoshida, M.; Fukumoto, Y.; Kuroda, Y.; Ohkoshi, N. Sympathetic Denervation of Myocardium Demonstrated by 123I-MIBG Scintigraphy in Pure Progressive Autonomic Failure. Eur. Neurol. 1997, 38, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Sakakibara, R.; Ogata, T.; Haruta, M.; Kishi, M.; Tsuyusaki, Y.; Tateno, A.; Tateno, F.; Mouri, T. Amnestic Mild Cognitive Impairment with Low Myocardial Metaiodobenzylguanidine Uptake. Am. J. Neurodegener. Dis. 2012, 1, 146–151. [Google Scholar] [PubMed]
- Choi, M.H.; Yoon, J.H.; Yong, S.W. Cardiac Sympathetic Denervation and Dementia in de Novo Parkinson’s Disease: A 7-Year Follow-up Study. J. Neurol. Sci. 2017, 381, 291–295. [Google Scholar] [CrossRef]
- Kobayashi, K.; Sumiya, H.; Nakano, H.; Akiyama, N.; Urata, K.; Koshino, Y. Detection of Lewy Body Disease in Patients with Late-Onset Depression, Anxiety and Psychotic Disorder with Myocardial Meta-Iodobenzylguanidine Scintigraphy. Int. J. Geriatr. Psychiatry 2010, 25, 55–65. [Google Scholar] [PubMed]
- Roberts, G.; Durcan, R.; Donaghy, P.C.; Lawley, S.; Ciafone, J.; Hamilton, C.A.; Colloby, S.J.; Firbank, M.J.; Allan, L.; Barnett, N.; et al. Accuracy of Cardiac Innervation Scintigraphy for Mild Cognitive Impairment with Lewy Bodies. Neurology 2021, 96, e2801–e2811. [Google Scholar] [CrossRef]
- Kitayama, M.; Wada-Isoe, K.; Irizawa, Y.; Nakashima, K. Association of Visual Hallucinations with Reduction of MIBG Cardiac Uptake in Parkinson’s Disease. J. Neurol. Sci. 2008, 264, 22–26. [Google Scholar] [CrossRef]
- Salsone, M.; Labate, A.; Quattrone, A. Cardiac Denervation Precedes Nigrostriatal Damage in Idiopathic Rapid Eye Movement Sleep Behavior Disorder. Mov. Disord. 2012, 27, 1068–1069. [Google Scholar] [CrossRef]
- Nomura, T.; Inoue, Y.; Högl, B.; Uemura, Y.; Kitayama, M.; Abe, T.; Miyoshi, H.; Nakashima, K. Relationship between 123I-MIBG Scintigrams and REM Sleep Behavior Disorder in Parkinson’s Disease. Park. Relat. Disord. 2010, 16, 683–685. [Google Scholar] [CrossRef]
- Miyamoto, T.; Miyamoto, M.; Iwanami, M.; Hirata, K. Follow-up Study of Cardiac 123I-MIBG Scintigraphy in Idiopathic REM Sleep Behavior Disorder. Eur. J. Neurol. 2011, 18, 1275–1278. [Google Scholar] [CrossRef]
- Janzen, A.; Vadasz, D.; Booij, J.; Luster, M.; Librizzi, D.; Henrich, M.T.; Timmermann, L.; Habibi, M.; Sittig, E.; Mayer, G.; et al. Progressive Olfactory Impairment and Cardiac Sympathetic Denervation in REM Sleep Behavior Disorder. J. Park. Dis. 2022, 12, 1921–1935. [Google Scholar] [CrossRef]
- Mizutani, Y.; Nakamura, T.; Okada, A.; Suzuki, J.; Watanabe, H.; Hirayama, M.; Sobue, G. Hyposmia and Cardiovascular Dysautonomia Correlatively Appear in Early-Stage Parkinson’s Disease. Park. Relat. Disord. 2014, 20, 520–524. [Google Scholar] [CrossRef] [PubMed]
- Murakami, N.; Sako, W.; Haji, S.; Furukawa, T.; Otomi, Y.; Otsuka, H.; Izumi, Y.; Harada, M.; Kaji, R. Potential Utility of 123I-MIBG Scintigraphy as a Predictor of Falls in Parkinson’s Disease. Front. Neurol. 2019, 10, 376. [Google Scholar] [CrossRef] [PubMed]
- Dorschner, J.; Farmakis, G.; Behnke, S.; Hellwig, D.; Schneider, S.; Fassbender, K.; Kirsch, C.-M.; Dillmann, U.; Spiegel, J. Myocardial MIBG Scintigraphy May Predict the Course of Motor Symptoms in Parkinson’s Disease. Park. Relat. Disord. 2011, 17, 372–375. [Google Scholar] [CrossRef] [PubMed]
- Olivola, E.; Brusa, L.; Rocchi, C.; Schillaci, O.; Liguori, C.; Cerroni, R.; Pierantozzi, M.; Chiaravalloti, A.; Stefani, A.; Stocchi, F. Does Fatigue in Parkinson’s Disease Correlate with Autonomic Nervous System Dysfunction? Neurol. Sci. 2018, 39, 2169–2174. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, T.; Hirayama, M.; Hara, T.; Hama, T.; Watanabe, H.; Sobue, G. Does Cardiovascular Autonomic Dysfunction Contribute to Fatigue in Parkinson’s Disease? Mov. Disord. 2011, 26, 1869–1874. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, M.; Kurita, A.; Hashimoto, M.; Fukumitsu, N.; Abo, M.; Ito, Y.; Urashima, M.; Inoue, K. Impaired Myocardial 123I-Metaiodobenzylguanidine Uptake in Lewy Body Disease: Comparison between Dementia with Lewy Bodies and Parkinson’s Disease. J. Neurol. Sci. 2006, 240, 15–19. [Google Scholar] [CrossRef]
- Oka, H.; Morita, M.; Onouchi, K.; Yoshioka, M.; Mochio, S.; Inoue, K. Cardiovascular Autonomic Dysfunction in Dementia with Lewy Bodies and Parkinson’s Disease. J. Neurol. Sci. 2007, 254, 72–77. [Google Scholar] [CrossRef]
- Komatsu, J.; Samuraki, M.; Nakajima, K.; Arai, H.; Arai, H.; Arai, T.; Asada, T.; Fujishiro, H.; Hanyu, H.; Iizuka, O.; et al. 123I-MIBG Myocardial Scintigraphy for the Diagnosis of DLB: A Multicentre 3-Year Follow-up Study. J. Neurol. Neurosurg. Psychiatry 2018, 89, 1167–1173. [Google Scholar] [CrossRef]
- Braune, S. The Role of Cardiac Metaiodobenzylguanidine Uptake in the Differential Diagnosis of Parkinsonian Syndromes. Clin. Auton. Res. 2001, 11, 351–355. [Google Scholar] [CrossRef]
- Armstrong, M.J.; Litvan, I.; Lang, A.E.; Bak, T.H.; Bhatia, K.P.; Borroni, B.; Boxer, A.L.; Dickson, D.W.; Grossman, M.; Hallett, M.; et al. Criteria for the Diagnosis of Corticobasal Degeneration. Neurology 2013, 80, 496–503. [Google Scholar] [CrossRef]
- Baschieri, F.; Vitiello, M.; Cortelli, P.; Calandra-Buonaura, G.; Morgante, F. Autonomic Dysfunction in Progressive Supranuclear Palsy. J. Neurol. 2023, 270, 109–129. [Google Scholar] [CrossRef] [PubMed]
- Sepúlveda Soto, M.C.; Fasano, A. Essential Tremor: New Advances. Clin. Park. Relat. Disord. 2020, 3, 100031. [Google Scholar] [CrossRef] [PubMed]
- Adler, C.H.; Beach, T.G.; Hentz, J.G.; Shill, H.A.; Caviness, J.N.; Driver-Dunckley, E.; Sabbagh, M.N.; Sue, L.I.; Jacobson, S.A.; Belden, C.M.; et al. Low Clinical Diagnostic Accuracy of Early vs Advanced Parkinson Disease: Clinicopathologic Study. Neurology 2014, 83, 406–412. [Google Scholar] [CrossRef]
- Langston, J.W.; Wiley, J.C.; Tagliati, M. Optimizing Parkinson’s Disease Diagnosis: The Role of a Dual Nuclear Imaging Algorithm. NPJ Park. Dis. 2018, 4, 5. [Google Scholar] [CrossRef]
- Yoshii, F.; Ryo, M.; Baba, Y.; Koide, T.; Hashimoto, J. Combined Use of Dopamine Transporter Imaging (DAT-SPECT) and 123I-Metaiodobenzylguanidine (MIBG) Myocardial Scintigraphy for Diagnosing Parkinson’s Disease. J. Neurol. Sci. 2017, 375, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Okada, Y.; Shiraishi, M.; Nakamura, H.; Maki, F.; Sasaki, N.; Hasegawa, Y.; Sasaki, O.; Nakashima, Y. Usefulness of the Combination of Iodine-123-Metaiodobenzylguanidine Scintigraphy and Iodine-123-Ioflupane Scintigraphy in New-Onset Parkinson’s Disease. Nucl. Med. Commun. 2018, 39, 983–988. [Google Scholar] [CrossRef]
- Sakamoto, F.; Shiraishi, S.; Yoshida, M.; Tomiguchi, S.; Hirai, T.; Namimoto, T.; Hashimoto, M.; Ikeda, M.; Uetani, H.; Yamashita, Y. Diagnosis of Dementia with Lewy Bodies: Diagnostic Performance of Combined 123I-IMP Brain Perfusion SPECT and 123I-MIBG Myocardial Scintigraphy. Ann. Nucl. Med. 2014, 28, 203–211. [Google Scholar] [CrossRef]
- Strano, S.; Fanciulli, A.; Rizzo, M.; Marinelli, P.; Palange, P.; Tiple, D.; De Vincentis, G.; Calcagnini, G.; Censi, F.; Meco, G.; et al. Cardiovascular Dysfunction in Untreated Parkinson’s Disease: A Multi-Modality Assessment. J. Neurol. Sci. 2016, 370, 251–255. [Google Scholar] [CrossRef]
- Nuvoli, S.; Spanu, A.; Piras, M.R.; Nieddu, A.; Mulas, A.; Rocchitta, G.; Galleri, G.; Serra, P.A.; Madeddu, G. 123I-Ioflupane Brain SPECT and 123I-MIBG Cardiac Planar Scintigraphy Combined Use in Uncertain Parkinsonian Disorders. Medicine 2017, 96, e6967. [Google Scholar] [CrossRef]
- Janzen, A.; Kogan, R.V.; Meles, S.K.; Sittig, E.; Renken, R.J.; Geibl, F.F.; Booij, J.; Stormezand, G.; Luster, M.; Mayer, G.; et al. Rapid Eye Movement Sleep Behavior Disorder: Abnormal Cardiac Image and Progressive Abnormal Metabolic Brain Pattern. Mov. Disord. 2022, 37, 624–629. [Google Scholar] [CrossRef]
- Taïeb, D.; Timmers, H.J.; Hindié, E.; Guillet, B.A.; Neumann, H.P.; Walz, M.K.; Opocher, G.; de Herder, W.W.; Boedeker, C.C.; de Krijger, R.R.; et al. EANM 2012 Guidelines for Radionuclide Imaging of Phaeochromocytoma and Paraganglioma. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 1977–1995. [Google Scholar] [CrossRef] [PubMed]
- Boccalini, C.; Carli, G.; Vanoli, E.G.; Cocco, A.; Albanese, A.; Garibotto, V.; Perani, D. Manual and Semi-Automated Approaches to MIBG Myocardial Scintigraphy in Patients with Parkinson’s Disease. Front. Med. 2022, 9, 1073720. [Google Scholar] [CrossRef] [PubMed]
- Veltman, C.E.; Boogers, M.J.; Meinardi, J.E.; Al Younis, I.; Dibbets-Schneider, P.; Van der Wall, E.E.; Bax, J.J.; Scholte, A.J.H.A. Reproducibility of Planar 123I-Meta-Iodobenzylguanidine (MIBG) Myocardial Scintigraphy in Patients with Heart Failure. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 1599–1608. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, K.; Okuda, K.; Yoshimura, M.; Matsuo, S.; Wakabayashi, H.; Imanishi, Y.; Kinuya, S. Multicenter Cross-Calibration of I-123 Metaiodobenzylguanidine Heart-to-Mediastinum Ratios to Overcome Camera-Collimator Variations. J. Nucl. Cardiol. 2014, 21, 970–978. [Google Scholar] [CrossRef] [PubMed]
- Ebina, J.; Mizumura, S.; Ishii, N.; Kobayashi, Y.; Shibukawa, M.; Morioka, H.; Nagasawa, J.; Yanagihashi, M.; Hirayama, T.; Kawabe, K.; et al. Reduced 123I-MIBG Uptake in the Parotid and Submandibular Glands in Patients with Parkinson’s Disease Identified Using a Quantitative Semi-Automatic Method. J. Neurol. 2023, 270, 4385–4392. [Google Scholar] [CrossRef]
- Nuvoli, S.; Spanu, A.; Fravolini, M.L.; Bianconi, F.; Cascianelli, S.; Madeddu, G.; Palumbo, B. [123I]Metaiodobenzylguanidine (MIBG) Cardiac Scintigraphy and Automated Classification Techniques in Parkinsonian Disorders. Mol. Imaging Biol. 2020, 22, 703–710. [Google Scholar] [CrossRef]
- Treglia, G.; Cason, E.; Stefanelli, A.; Cocciolillo, F.; Di Giuda, D.; Fagioli, G.; Giordano, A. MIBG Scintigraphy in Differential Diagnosis of Parkinsonism: A Meta-Analysis. Clin. Auton. Res. 2012, 22, 43–55. [Google Scholar] [CrossRef]
- Orimo, S.; Suzuki, M.; Inaba, A.; Mizusawa, H. 123I-MIBG Myocardial Scintigraphy for Differentiating Parkinson’s Disease from Other Neurodegenerative Parkinsonism: A Systematic Review and Meta-Analysis. Park. Relat. Disord. 2012, 18, 494–500. [Google Scholar] [CrossRef]
- Giannoccaro, M.P.; Donadio, V.; Incensi, A.; Pizza, F.; Cason, E.; Di Stasi, V.; Martinelli, P.; Scaglione, C.; Capellari, S.; Treglia, G.; et al. Skin Biopsy and I-123 MIBG Scintigraphy Findings in Idiopathic Parkinson’s Disease and Parkinsonism: A Comparative Study. Mov. Disord. 2015, 30, 986–989. [Google Scholar] [CrossRef]
- Giannoccaro, M.P.; Donadio, V.; Giannini, G.; Devigili, G.; Rizzo, G.; Incensi, A.; Cason, E.; Calandra-Buonaura, G.; Eleopra, R.; Cortelli, P.; et al. Comparison of 123I-MIBG Scintigraphy and Phosphorylated α-Synuclein Skin Deposits in Synucleinopathies. Park. Relat. Disord. 2020, 81, 48–53. [Google Scholar] [CrossRef]
- Nakae, I.; Hayashi, H.; Mitsunami, K.; Horie, M. Clinical Significance of Lung Iodine-123 Metaiodobenzylguanidine Uptake Assessment in Parkinson’s and Heart Diseases. Ann. Nucl. Med. 2013, 27, 737–747. [Google Scholar] [CrossRef] [PubMed]
- Asahi, T.; Kashiwazaki, D.; Yoneyama, T.; Noguchi, K.; Kuroda, S. Importance of 123I-Ioflupane SPECT and Myocardial MIBG Scintigraphy to Determine the Candidate of Deep Brain Stimulation for Parkinson’s Disease. Neurol. Med. Chir. 2016, 56, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Otano, J.; Gaig, C.; Muxi, A.; Lomeña, F.; Compta, Y.; Buongiorno, M.T.; Martí, M.J.; Tolosa, E.; Valldeoriola, F. 123I-MIBG Cardiac Uptake, Smell Identification and 123I-FP-CIT SPECT in the Differential Diagnosis between Vascular Parkinsonism and Parkinson’s Disease. Park. Relat. Disord. 2014, 20, 192–197. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.K.; Choi, E.K.; Song, I.U.; Kim, J.S.; Chung, Y.A. Comparison of I-123 MIBG Planar Imaging and SPECT for the Detection of Decreased Heart Uptake in Parkinson Disease. J. Neural. Transm. 2015, 122, 1421–1427. [Google Scholar] [CrossRef]
- Ikeda, T.; Ikenoshita, S.; Sakamoto, F.; Shiraishi, S.; Nakahara, K.; Masuda, T.; Yamashita, S. Is 123I-MIBG Scintigraphy Beneficial or Excessive for the Diagnosis of Parkinson’s Disease in the Early Phase? Neurodegener. Dis. 2019, 19, 88–95. [Google Scholar] [CrossRef]
- Asayama, S.; Wate, R.; Kaneko, S.; Asayama, T.; Oki, M.; Tsuge, A.; Nagashima, M.; Morita, J.; Nakamura, S.; Nakamura, M.; et al. Levodopa Challenge Test and 123I-Metaiodobenzylguanidine Scintigraphy for Diagnosing Parkinson’s Disease. Acta Neurol. Scand. 2013, 128, 160–165. [Google Scholar] [CrossRef]
- Ryu, D.W.; Kim, J.S.; Lee, J.E.; Oh, Y.S.; Yoo, S.W.; Yoo, I.R.; Lee, K.S. Initial Versus Follow-up Sequential Myocardial 123I-MIBG Scintigraphy to Discriminate Parkinson Disease From Atypical Parkinsonian Syndromes. Clin. Nucl. Med. 2019, 44, 282–288. [Google Scholar] [CrossRef]
- Mizutani, Y.; Ito, S.; Murate, K.; Hirota, S.; Fukui, T.; Hikichi, C.; Ishikawa, T.; Shima, S.; Ueda, A.; Kizawa, M.; et al. Retrospective Analysis of Parkinsonian Patients Exhibiting Normal 123I-MIBG Cardiac Uptake. J. Neurol. Sci. 2015, 359, 236–240. [Google Scholar] [CrossRef]
- Watanabe, M.; Takeda, T.; Nakamagoe, K.; Tamaoka, A. Sequential Imaging Analysis Using MIBG Scintigraphy Revealed Progressive Degeneration of Cardiac Sympathetic Nerve in Parkinson’s Disease. Eur. J. Neurol. 2011, 18, 1010–1013. [Google Scholar] [CrossRef]
- Lee, P.H.; Kim, J.S.; Shin, D.H.; Yoon, S.-N.; Huh, K. Cardiac 123I-MIBG Scintigraphy in Patients with Drug Induced Parkinsonism. J. Neurol. Neurosurg. Psychiatry 2006, 77, 372–374. [Google Scholar] [CrossRef]



| Mechanism | Medication | Time to Hold before the Procedure |
|---|---|---|
| Inhibition of sodium-dependent uptake | Fluphenazine, pipotiazine, zuclopenthixol | 1 month (depot) |
| Labetalol, levomepromazine (methotrimeprazine), pimozide | 72 h | |
| Amitriptyline, amoxapine, benperidol, butriptyline, flupenthixol, haloperidol, lofepramine, loxapine, maprotiline, mianserin, periciazine, trimipramine, thiethylperazine, trifluoperazine, trimipramine, viloxazine, zuclopenthixol | 48 h | |
| Chlorpromazine, clomipramine, cocaine, desipramine, doxepin, dothiepin, droperidol, ephedrine, imipramine, iprindole, oxypertine, nortriptyline, perphenazine, prochlorperazine, promazine, promethazine, protriptyline, thioridazine, trifluperidol | 24 h | |
| Inhibition of uptake by active transport into vesicle | Methoserpidine, reserpine | 72 h |
| Xamoterol | 48 h | |
| Competition for transport into vesicle | Bethanidine, bretylium, debrisoquine, guanethidine | 48 h |
| Depletion of content from storage vesicle | Labetalol, methoserpidine, reserpine | 72 h |
| Amfepramone (diethylpropion), bethanidine, bretylium, debrisoquine, dextroamphetamine, fenfluramine, guanethidine, mazindol, phentermine, phenylephedrine, phenylpropanolamine, pirbuterol, trazodone | 48 h | |
| Dopamine, dobutamine, fenoterol, isoetharine, isoprenaline (isoproterenol), metaraminol, methylephedrine, methoxamine, norepinephrine (noradrenaline), orciprenaline, pseudoephedrine, reproterol, rimiterol, albuterol (salbutamol), terbutaline | 24 h | |
| Calcium-mediated | Isradipine, lidoflazine, nicardipine, verapamil | 48 h |
| Diltiazem, nifedipine, nimodipine | 24 h |
| Reference | n | n PD | H&Y Stage a | H/M Ratio | Sensitivity c | Specificity c | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| PD b | Cutoff | Early Phase | Delayed Phase | Early Phase | Delayed Phase | ||||||
| Early Phase | Delayed Phase | Early Phase | Delayed Phase | ||||||||
| Yoshita et al. [68] | 54 | 25 | 2.1 | 1.36 ± 0.15 | 1.19 ± 0.15 | NA | 1.00 | 0.79 | |||
| Braune et al. [69] | 10 | 10 | NA | NA | 1.06 ± 0.06 | NA | NA | NA | |||
| Iwasa et al. [70] | 12 | 12 | 2.5 | 1.55 ± 0.17 | 1.37 ± 0.15 | NA | NA | NA | |||
| Braune et al. [71] | 20 | 15 | NA | NA | 1.08 ± 0.13 | NA | NA | NA | |||
| Orimo et al. [72] | 68 | 45 | 3.0 | 1.71 ± 0.36 | 1.53 ± 0.36 | NA | 0.80 | 0.87 | |||
| Druschky et al. [73] | 30 | 10 | 1.6 | NA | 1.25 ± 0.61 | NA | NA | NA | |||
| Taki et al. [74] | 70 | 41 | 1.9 | 1.61 ± 0.29 | 1.47 ± 0.34 | 1.89 | 2.02 | 0.83 | 0.90 | 0.83 | 0.76 |
| Reinhardt et al. [75] | 28 | 21 | 3.4 | 1.05 | NA | 1.00 | 1.00 | ||||
| Takatsu et al. [76] | 32 | 32 | 2.84 | 1.58 ± 0.37 | 1.33 ± 0.28 | NA | 0.93 | 1.00 | |||
| Courbon et al. [61] | 28 | 18 | 2.34 | NA | 1.50 ± 0.53 | NA | 1.30 | 0.80 | 1.00 | ||
| Hamada et al. [77] | 113 | 88 | 2.61 | 1.51 ± 0.32 | 1.39 ± 0.33 | NA | NA | NA | |||
| Orimo et al. [78] | 98 | 90 | 2.73 | 1.72 ± 0.33 | 1.54 ± 0.35 | NA | NA | NA | |||
| Saiki et al. [79] | 45 | 34 | 2.55 | 1.45 ± 0.20 | 1.33 ± 0.27 | 1.38 | 1.25 | 0.83 | 0.66 | 0.86 | 0.73 |
| Nagayama et al. [80] | 391 | 122 | 3.0 | NA | 1.38 ± 0.29 | NA | 1.84 | NA | 0.87 | NA | 0.37 |
| Kashihara et al. [81] | 204 | 130 | 3.1 | 1.63 ± 0.29 | 1.37 ± 0.27 | NA | 0.84 | 1.00 | |||
| Kim et al. [82] | 65 | 30 | NA | NA | 1.27 ± 0.13 | NA | 1.00 | 0.84 | |||
| Lee et al. [83] | 93 | 51 | 1.61 | NA | 1.28 ± 0.35 | NA | 0.98 | 1.00 | |||
| Miyamoto et al. [84] | 34 | 12 | 2.3 | NA | 1.43 ± 0.20 | NA | NA | NA | |||
| Shin et al. [85] | 119 | 40 | 2.25 | 1.34 ± 0.15 | 1.29 ± 0.15 | 1.38 | 1.36 | 0.65 | 0.80 | 0.95 | 1.00 |
| Köllensperger et al. [86] | 18 | 9 | 3.2 | 1.51 ± 0.24 | 1.32 ± 0.25 | 1.93 | 1.68 | 0.44 | 0.55 | 0.88 | 0.88 |
| Spiegel et al. [87] | 102 | 102 | 1.7 | NA | 1.45 ± 0.29 | NA | NA | 0.93 | NA | ||
| Miyamoto et al. [88] | 95 | 26 | NA | 2.08 ± 0.55 | 1.80 ± 0.68 | 1.82 | NA | 0.65 | NA | 0.77 | NA |
| Chung et al. [89] | 51 | 27 | 2.5 | 1.53 ± 0.27 | 1.35 ± 0.24 | 1.74 | 1.79 | 0.85 | 1.00 | 0.54 | 0.68 |
| Novellino et al. [90] | 70 | 20 | NA | NA | 1.10 ± 0.09 | NA | 1.0 | 1.0 | |||
| Sawada et al. [91] | 400 | 267 | 3.2 | 1.66 ± 0.33 | 1.44 ± 0.39 | 1.92 | 1.68 | 0.81 | 0.84 | 0.85 | 0.89 |
| Fröhlich et al. [92] | 50 | 39 | NA | NA | 1.48 ± 0.46 | NA | 1.60 | NA | 0.87 | NA | 0.46 |
| Ishibashi et al. [93] | 39 | 24 | 2.41 | 1.66 ± 0.45 | 1.46 ± 0.41 | 1.95 | 1.60 | 0.79 | 0.93 | 0.70 | 0.93 |
| Izawa et al. [94] | 80 | 44 | NA | 1.67 ± 0.37 | NA | 1.66 | NA | 0.60 | NA | NA | |
| Kikuchi et al. [95] | 84 | 42 | NA | NA | 1.55 ± 0.30 | NA | 1.75 | NA | 0.85 | NA | 0.76 |
| Kurata et al. [96] | 295 | 166 | 2.96 | 1.74 ± 0.41 | 1.53 ± 0.48 | NA | NA | NA | |||
| Muxí et al. [97] | 28 | 14 | 1.57 | 1.28 ± 0.11 | 1.12 ± 0.11 | 1.48 | 1.43 | 0.86 | 0.93 | 0.92 | 1.00 |
| Südmeyer et al. [98] | 48 | 31 | NA | NA | 1.34 ± 0.27 | NA | 1.34 | NA | 0.88 | NA | 0.65 |
| Behnke et al. [99] | 42 | 42 | 1.47 | NA | 1.47 ± 0.31 | NA | NA | NA | |||
| Chiaravalloti et al. [100] | 37 | 37 | 1.67 | 1.72 ± 0.33 | 1.6 ± 0.32 | NA | NA | NA | |||
| Umemura et al. [101] | 138 | 118 | NA | NA | 1.75 ± 0.63 | NA | 1.85 | NA | 0.67 | NA | 0.80 |
| Leite et al. [102] | 21 | 21 | 2 | 1.53 ± 0.27 | 1.46 ± 0.29 | 1.8 | 1.7 | NA | NA | ||
| Katagiri et al. [66] | 100 | 50 | 2.3 | 2.05 ± 0.68 | 1.84 ± 0.88 | NA | NA | NA | |||
| Mochizuki et al. [103] | 357 | 191 | 2.3 | 1.91 ± 0.51 | 1.62 ± 0.60 | NA | NA | NA | |||
| Rocchi et al. [104] | 27 | 27 | 2.4 | NA | 1.53 ± 0.39 | NA | NA | NA | 0.70 | ||
| Tsujikawa et al. [49] | 70 | 70 | 2.1 | 1.83 ± 0.40 | 1.69 ± 0.48 | 1.90 | 1.97 | 1.00 | 0.64 | 1.00 | 0.71 |
| Fujita et al. [105] | 139 | 101 | 2.7 | NA | 1.9 ± 0.1 | NA | 2.00 | NA | 0.70 | NA | 0.86 |
| Uyama et al. [106] | 34 | 15 | NA | NA | 2.19 ± 0.55 | NA | 2.74 | NA | 0.86 | NA | 0.79 |
| Yang et al. [107] | 64 | 25 | 2 | 1.65 ± 0.36 | 1.50 ± 0.43 | NA | NA | NA | |||
| Gabilondo et al. [108] | 194 | 85 | NA | 1.80 ± 0.51 | 1.60 ± 0.46 | 2.16 | NA | 0.87 | NA | 0.89 | NA |
| Brandl et al. [109] | 167 | 104 | 2.0 | NA | 1.26 ± 0.24 | NA | NA | 0.94 | NA | 0.65 | |
| Kawazoe et al. [58] | 600 | 272 | 2.39 | NA | NA | 2.00 | 2.00 | 0.74 | 0.82 | 0.75 | 0.84 |
| Skowronek et al. [110] | 36 | 11 | NA | NA | 1.5 ± 0.5 | NA | NA | NA | 0.73 | ||
| Jeong et al. [35] | 60 | 60 | 2.2 | 1.39 ± 0.15 | 1.31 ± 0.15 | NA | NA | NA | |||
| Sakuramoto et al. [111] | 96 | 70 | 2.6 | NA | 1.99 ± 0.89 | NA | 2.00 | NA | 0.67 | NA | 1.00 |
| Brumberg et al. [112] | 42 | 21 | NA | NA | 1.94 ± 0.63 | NA | 2.76 | NA | 0.90 | NA | 0.66 |
| Jang et al. [113] | 31 | 31 | NA | 2.10 ± 0.87 | 1.85 ± 1.22 | NA | NA | NA | |||
| Iwabuchi et al. [114] | 216 | 90 | NA | 1.99 ± 0.44 | 1.82 ± 0.54 | NA | 2.26 | NA | NA | ||
| Eckhardt et al. [63] | 31 | 19 | 2.42 | NA | 1.18 ± 0.19 | NA | NA | 0.89 | NA | 0.67 | |
| Miyagi et al. [115] | 28 | 17 | 2.0 | 1.92 ± 0.56 | 1.69 ± 0.71 | 2.2 | 2.2 | NA | NA | ||
| Symptom | Description | Differential Diagnosis | Reference |
|---|---|---|---|
| Constipation | Constipation and abnormal cardiac MIBG were associated with the initial manifestation of PD. One in every four individuals with this presentation will have a diagnosis of PD. | DLB | [22,150] |
| Postural hypotension | Pure autonomic failure may be a risk factor for the development of PD. There is a significant association between reduced cardiac MIBG in patients with pure autonomic failure and the development of PD. | MSA | [81,151] |
| Cognitive impairment | Most patients who present with cognitive impairment and abnormal cardiac MIBG will develop dementia with Lewy bodies; only a small percentage of individuals will develop PD. Reduced cardiac MIBG may be associated with a subsequent risk of dementia and may reflect the wider extension of alpha-synuclein pathology. | DLB | [152,153] |
| Depression/ anxiety | Depression is among the most common neuropsychiatric disorders in PD. Of 13 patients presenting with depression and anxiety and abnormal cardiac MIBG, 11 developed PD years later. | DLB | [154,155] |
| Visual hallucinations | Visual hallucinations are a possible risk factor for the development of PD. Four individuals presented with visual hallucinations and abnormal cardiac MIBG, but no discussion is given in the follow-up of these individuals. Also, visual hallucinations is an independent risk factor for abnormal cardiac MIBG uptake. | Corticobasal degeneration | [154,156] |
| Sleep disorders | Low MIBG uptake and rapid eye movement sleep behavior disorder was associated with PD severity. Also, REM sleep behavior disorder is an independent risk factor associated with abnormal MIBG uptake in individuals with PD. | DLBMSA | [157,158,159] |
| Olfactory | A relationship between abnormal MIBG uptake and hyposmia in the early prodromal stage of PD (before nigrostriatal degeneration) was observed. Degeneration in broad aspects of the cardiovascular sympathetic system occurs concurrently with olfactory system degeneration during the premotor phase of PD. | DLB | [160,161] |
| Gait | Abnormal MIBG uptake was already associated with a higher incidence of falls. This may be an indirect finding of autonomic dysfunction. Also, cardiac MIBG uptake correlated significantly with the annual progress of rigidity and axial symptoms. | MSA | [162,163] |
| Fatigue | The results in the literature are contradictory. Some authors found, and others did not, a correlation between cardiac MIBG uptake and PD-related fatigue. | MSA | [164,165] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pitton Rissardo, J.; Fornari Caprara, A.L. Cardiac 123I-Metaiodobenzylguanidine (MIBG) Scintigraphy in Parkinson’s Disease: A Comprehensive Review. Brain Sci. 2023, 13, 1471. https://doi.org/10.3390/brainsci13101471
Pitton Rissardo J, Fornari Caprara AL. Cardiac 123I-Metaiodobenzylguanidine (MIBG) Scintigraphy in Parkinson’s Disease: A Comprehensive Review. Brain Sciences. 2023; 13(10):1471. https://doi.org/10.3390/brainsci13101471
Chicago/Turabian StylePitton Rissardo, Jamir, and Ana Letícia Fornari Caprara. 2023. "Cardiac 123I-Metaiodobenzylguanidine (MIBG) Scintigraphy in Parkinson’s Disease: A Comprehensive Review" Brain Sciences 13, no. 10: 1471. https://doi.org/10.3390/brainsci13101471