
A Validation Study for SHE Score for Acute Subdural Hematoma in the Elderly

 ,
,  ,
,  , , , ,
, , , ,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. SHE Score, Treatment Algorithm, and Primary Endpoint
2.2. Nonconvulsive Status Epilepticus—Secondary Endpoint
2.3. Surgery vs. Conservative Treatment
2.4. Statistics
3. Results
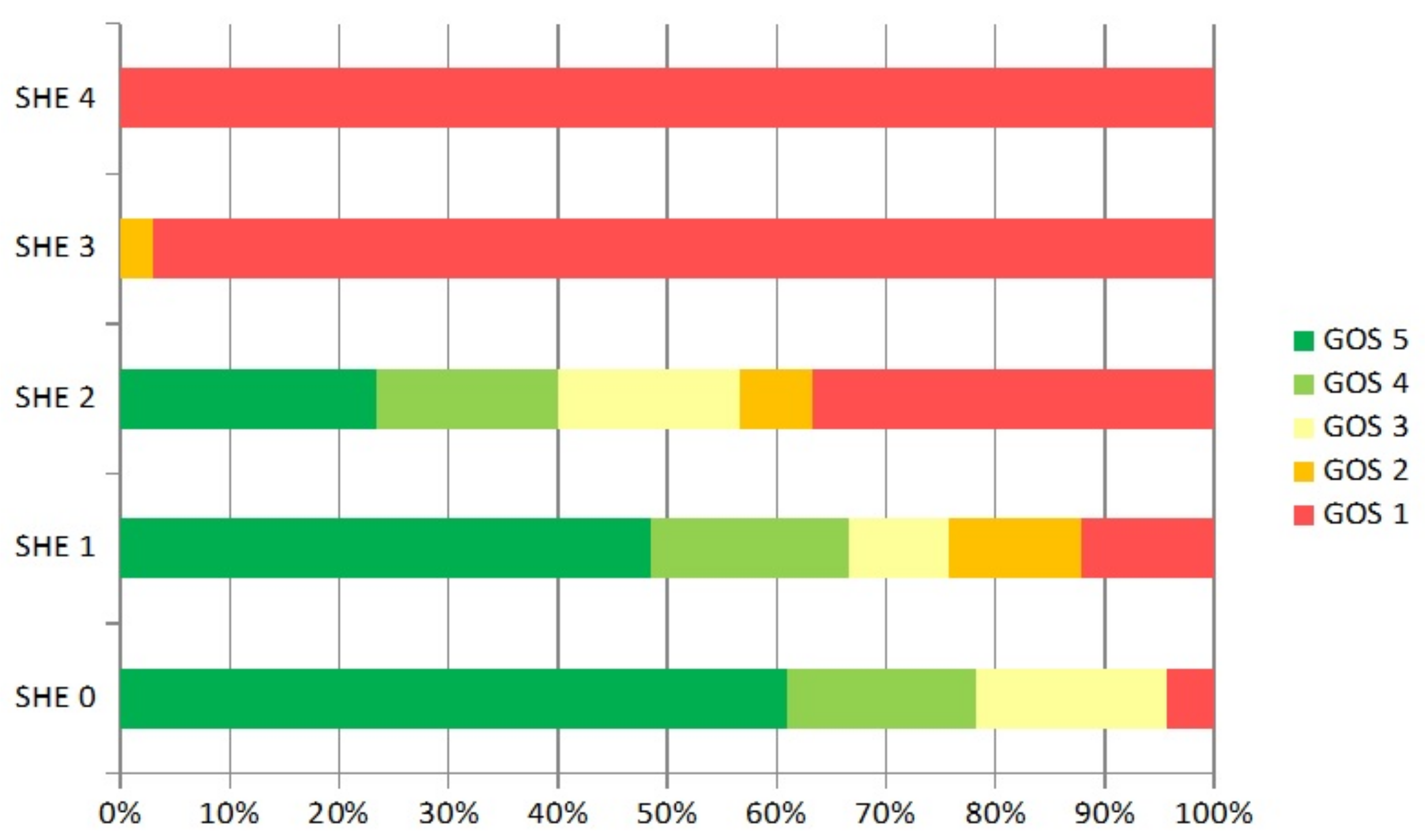
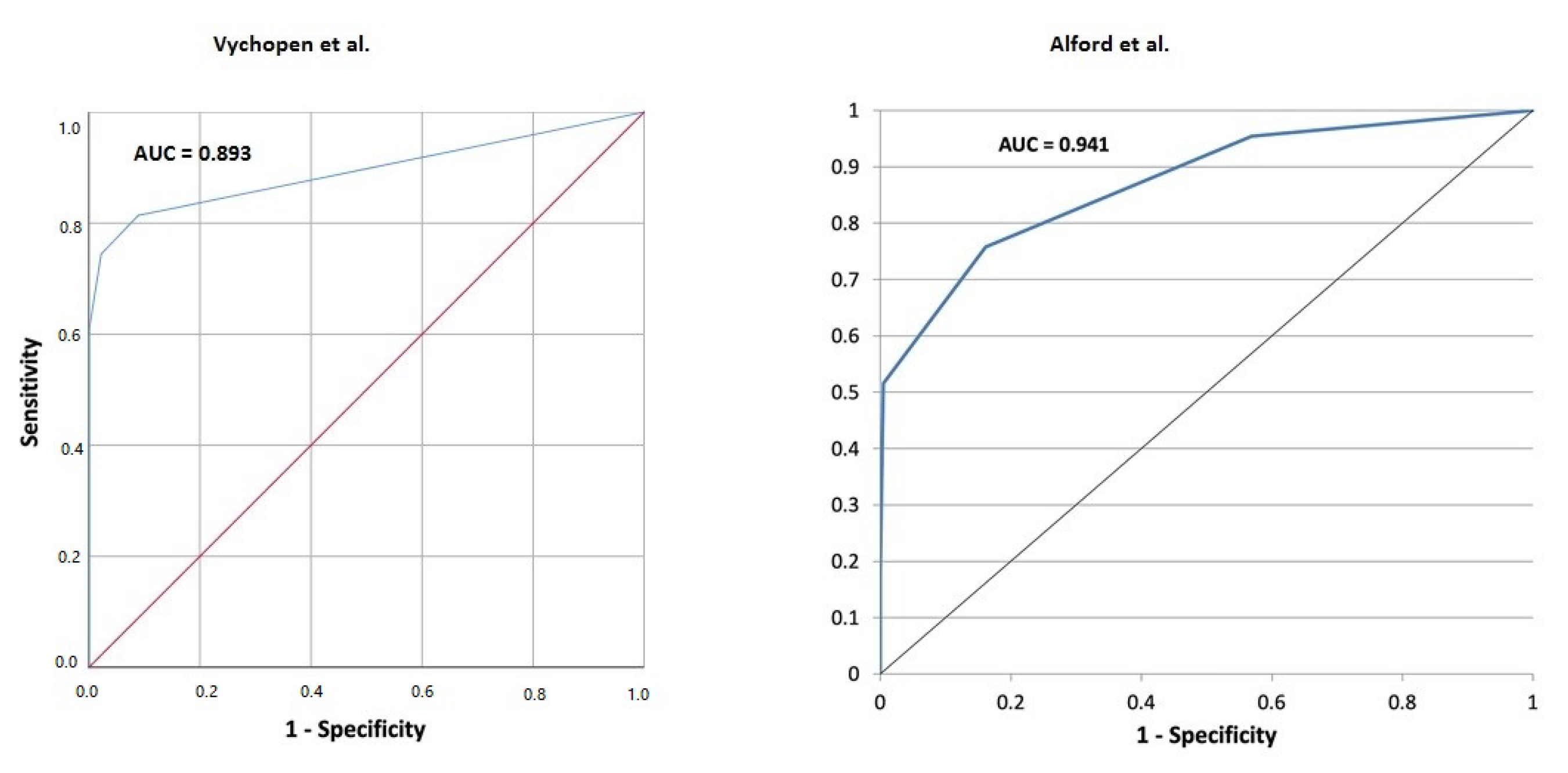
3.1. Validation of SHE Score in the Elderly with Acute Subdural Hematoma
3.2. Nonconvulsive Status Epilepticus as Strongest Independent Additional Outcome Measure
3.3. Surgery vs. Conservative Treatment
4. Discussion
4.1. SHE Score—Primary Endpoint
4.2. ncSE—Secondary Endpoint
5. Limitations
6. Conclusions
6.1. SHE Score—Reliable Mortality Predictor
6.2. ncSE—Secondary Endpoint
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| aSDH | acute subdural hematoma |
| ncSE | nonconvulsive status epilepticus |
| SHE | subdural hematoma in elderly score |
| GOS | Glasgow outcome score |
| CI | confidence interval |
| OR | odds ratio |
| AUC | area under curve |
| ROC | reciever operating characteristic |
| EEG | electroencephalography |
| cEEG | continuous electroencephalography |
References
- Gaist, D.; Rodríguez, L.A.G.; Hellfritzsch, M.; Poulsen, F.R.; Halle, B.; Hallas, J.; Pottegård, A. Association of Antithrombotic Drug Use With Subdural Hematoma Risk. JAMA 2017, 317, 836–846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trevisi, G.; Sturiale, C.L.; Scerrati, A.; Rustemi, O.; Ricciardi, L.; Raneri, F.; Tomatis, A.; Piazza, A.; Auricchio, A.M.; Stifano, V.; et al. Acute subdural hematoma in the elderly: Outcome analysis in a retrospective multicentric series of 213 patients. Neurosurg. Focus 2020, 49, E21. [Google Scholar] [CrossRef] [PubMed]
- Younsi, A.; Fischer, J.; Habel, C.; Riemann, L.; Scherer, M.; Unterberg, A.; Zweckberger, K. Mortality and functional outcome after surgical evacuation of traumatic acute subdural hematomas in octa- and nonagenarians. Eur. J. Trauma Emerg. Surg. 2021, 47, 1499–1510. [Google Scholar] [CrossRef]
- Alford, E.N.; Rotman, L.E.; Erwood, M.S.; Oster, R.A.; Davis, M.C.; Pittman, H.B.C.; Zeiger, H.E.; Fisher, W.S. Development of the Subdural Hematoma in the Elderly (SHE) score to predict mortality. J. Neurosurg. 2019, 12, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Atalay, T.; Ak, H.; Gülsen, I.; Karacabey, S. Risk factors associated with mortality and survival of acute subdural hematoma: A retrospective study. J. Res. Med. Sci. 2019, 25, 24–27. [Google Scholar]
- Weimer, J.M.; Gordon, E.; Frontera, J.A. Predictors of Functional Outcome After Subdural Hematoma: A Prospective Study. Neurocrit. Care 2017, 26, 70–79. [Google Scholar] [CrossRef] [PubMed]
- Bullock, M.R.; Chesnut, R.; Ghajar, J.; Gordon, D.; Hartl, R.; Newell, D.W.; Servadei, F.; Walters, B.C.; Wilberger, J.E. Surgical Management of Traumatic Brain Injury Author Group. Surgical management of acute subdural hematomas. Neurosurgery 2006, 58, S16–S24. [Google Scholar]
- Sharma, R.; Rocha, E.; Pasi, M.; Lee, H.; Patel, A.; Singhal, A.B. Subdural Hematoma: Predictors of Outcome and a Score to Guide Surgical Decision-Making. J. Stroke Cerebrovasc. Dis. 2020, 29, 105180. [Google Scholar] [CrossRef]
- AbdelFatah, M.A.R. Prognosis of acute subdural hematoma greater than 10 mm in thickness in head injury patients with an extension or no motor response to pain after resuscitation. Egypt. Neurosurg. 2019, 34, 9. [Google Scholar] [CrossRef] [Green Version]
- Koc, R.K.; Akdemir, H.; Öktem, I.S.; Meral, M.; Menkü, A. Acute subdural hematoma: Outcome and outcome prediction. Neurosurg. Rev. 1997, 20, 239–244. [Google Scholar] [CrossRef]
- Kotwica, Z.; Brzeziński, J. Acute subdural haematoma in adults: An analysis of outcome in comatose patients. Acta Neurochir. 1993, 121, 95–99. [Google Scholar] [CrossRef]
- Servadei, M.T.; Nasi, G.; Giuliani, A.; Maria Cremonini, P.; Cenni, D.; Zappi, G.S.; Taylor, F. CT prognostic factors in acute subdural haematomas: The value of the ‘worst’ CT scan. Br. J. Neurosurg. 2000, 14, 110–116. [Google Scholar] [CrossRef]
- Van den Brink, W.A. The prognostic importance of the volume of traumatic epidural and subdural haematomas revisited. Acta Neurochir. 1999, 141, 509–514. [Google Scholar] [CrossRef]
- Brown, S.C.; King, Z.A.; Kuohn, L.; Kamel, H.; Gilmore, E.J.; Frontera, J.A.; Murthy, S.; Kim, J.A.; Omay, S.B.; Falcone, G.J.; et al. Association of race and ethnicity to incident epilepsy, or epileptogenesis, after subdural hematoma. Neurology 2020, 95, e2890–e2899. [Google Scholar] [CrossRef]
- Brown, S.C.; King, Z.A.; Kuohn, L.; Kamel, H.; Gilmore, E.J.; Frontera, J.A.; Murthy, S.; Kim, J.A.; Omay, S.B.; Falcone, G.J.; et al. Seizure and status epilepticus in chronic subdural hematoma. Acta Neurol. Scand. 2019, 140, 194–203. [Google Scholar]
- Peterella, L. Use of the Subdural Hematoma in the Elderly (SHE) Score to Predict 30-Day Mortality After Chronic Subdural Hematoma Evacuation. World Neurosurg. 2022, 157, e294–e300. [Google Scholar] [CrossRef]
- Masters, S.J.; McClean, P.M.; Arcarese, J.S.; Brown, R.F.; Campbell, J.A.; Freed, H.A.; Hess, G.H.; Hoff, J.T.; Kobrine, A.; Koziol, D.F.; et al. Skull x-ray examinations after head trauma. Recommendations by a multidisciplinary panel and validation study. N. Engl. J. Med. 1987, 316, 84–91. [Google Scholar] [CrossRef]
- Marshall, S.; Bayley, M.; McCullagh, S.; Velikonja, D.; Berrigan, L.; Ouchterlony, D.; Weegar, K.; Expert Consensus Group. Updated clinical practice guidelines for concussion/mild traumatic brain injury and persistent symptoms. Brain Inj. 2015, 29, 688–700. [Google Scholar] [CrossRef]
- Sucu, H.K.; Gokmen, M.; Gelal, F. The value of XYZ/2 technique compared with computer-assisted volumetric analysis to estimate the volume of chronic subdural hematoma. Stroke 2005, 36, 998–1000. [Google Scholar] [CrossRef] [Green Version]
- Pack, A.M. Epilepsy Overview and Revised Classification of Seizures and Epilepsies. Continuum 2019, 25, 306–321. [Google Scholar] [CrossRef]
- Rai, S.; Drislane, F.W. Treatment of Refractory and Super-refractory Status Epilepticus. Neurotherapeutics 2018, 15, 697–712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferguson, M.; Bianchi, M.T.; Sutter, R.; Rosenthal, E.S.; Cash, S.S.; Kaplan, P.W.; Westover, M.B. Calculating the risk benefit equation for aggressive treatment of non-convulsive status epilepticus. Neurology 2013, 18, 216–227. [Google Scholar] [CrossRef] [PubMed]
- Frohlich, J.; Johnson, M.A.; McArthur, D.L.; Lutkenhoff, E.S.; Dell’Italia, J.; Real, C.; Shrestha, V.; Spivak, N.M.; Tejeda, J.E.R.; Vespa, P.M.; et al. Sedation-Induced Burst Suppression Predicts Positive Outcome Following Traumatic Brain Injury. Front. Neurol. 2021, 12, 750667. [Google Scholar] [CrossRef] [PubMed]
- Hanley, J.A.; McNeil, B.J. The meaning and use of the area under a Receiver Operating Characteristic (ROC) curve. Radiology 1982, 143, 29–36. [Google Scholar]
- Englander, J. Analyzing risk factors for late posttraumatic seizures: A prospective, multicenter investigation. Arch. Phys. Med. Rehabil. 2003, 84, 365–373. [Google Scholar] [CrossRef]
- Yeh, C.C.; Chen, T.L.; Hu, C.J.; Chiu, W.T.; Liao, C.C. Risk of epilepsy after traumatic brain injury: A retrospective population-based cohort study. J. Neurol. Neurosurg. Psych. 2013, 84, 441–445. [Google Scholar] [CrossRef]
- Morris, N.A.; Merkler, A.E.; Parker, W.E.; Claassen, J.; Connolly, E.S.; Sheth, K.N.; Kamel, H. Adverse Outcomes After Initial Non-surgical Management of Subdural Hematoma: A Population-Based Study. Neurocrit. Care 2016, 24, 226–232. [Google Scholar] [CrossRef]
- Mathew, P.; Oluoch-Olunya, D.L.; Condon, B.R.; Bullock, R. Acute subdural haematoma in the conscious patient: Outcome with initial non-operative management. Acta Neurochir. 2006, 121, 100–108. [Google Scholar] [CrossRef]
- Hemphill, J.C.; Bonovich, D.C.; Besmertis, L.; Manley, G.T.; Johnston, S.C. The ICH score: A simple, reliable grading scale for intracerebral hemorrhage. Stroke 2001, 32, 891–897. [Google Scholar] [CrossRef] [Green Version]
- De Marchis, G.M.; Pugin, D.; Meyers, E.; Velasquez, A.; Suwatcharangkoon, S.; Park, S.; Falo, M.C.; Agarwal, S.; Mayer, S.; Schmidt, J.M.; et al. Seizure burden in subarachnoid hemorrhage associated with functional and cognitive outcome. Neurology 2016, 86, 253–260. [Google Scholar] [CrossRef] [Green Version]
- Claassen, J.; Jette, N.; Chum, F.; Green, R.; Schmidt, M.; Choi, H.; Jirsch, J.; Frontera, J.A.; Connolly, E.S.; Emerson, R.G.; et al. Electrographic seizures and periodic discharges after intracerebral hemorrhage. Neurology 2007, 69, 1356–1365. [Google Scholar] [CrossRef]
- Rossetti, A.O.; Hirsch, L.J.; Drislane, F.W. Nonconvulsive seizures and nonconvulsive status epilepticus in the neuro ICU should or should not be treated aggressively: A debate. Clin. Neurophysiol. Pract. 2019, 4, 170–177. [Google Scholar] [CrossRef]
- Topjian, A.A.; Gutierrez-Colina, A.M.; Sanchez, S.M.; Berg, R.A.; Friess, S.H.; Dlugos, D.J.; Abend, N.S. Electrographic status epilepticus is associated with mortality and worse short-term outcome in critically ill children. Crit. Care Med. 2013, 41, 215–223. [Google Scholar] [CrossRef] [Green Version]
- Wagenman, K.L.; Blake, T.P.; Sanchez, S.M.; Schultheis, M.T.; Radcliffe, J.; Berg, R.A.; Dlugos, D.J.; Topjian, A.A.; Abend, N.S. Electrographic status epilepticus and long-term outcome in critically ill children. Neurology 2014, 82, 396–404. [Google Scholar] [CrossRef] [Green Version]
- Seifi, A.; Asadi-Pooya, A.A.; Carr, K.; Maltenfort, M.; Emami, M.; Bell, R.; Moussouttas, M.; Yazbeck, M.; Rincon, F. The epidemiology, risk factors, and impact on hospital mortality of status epilepticus after subdural hematoma in the United States. Springerplus 2014, 3, 332. [Google Scholar] [CrossRef] [Green Version]
- Schädel-Hirn-Trauma im Erwachsenenalter Deutsche Gesellschaft für Neurochirurgie e.V. (DGNC) 2015. Available online: https://www.awmf.org/leitlinien/detail/ll/008-001.html (accessed on 5 June 2022).
- Won, S.Y.; Dubinski, D.; Brawanski, N.; Strzelczyk, A.; Seifert, V.; Freiman, T.M.; Konczalla, J. Significant increase in acute subdural hematoma in octo- and nonagenarians: Surgical treatment, functional outcome, and predictors in this patient cohort. Neurosurg. Focus 2017, 43, E10. [Google Scholar] [CrossRef] [Green Version]
- Won, S.Y.; Dubinski, D.; Eibach, M.; Gessler, F.; Herrmann, E.; Keil, F.; Seifert, V.; Konczalla, J.; Behmanesh, B. External validation and modification of the Oslo grading system for prediction of postoperative recurrence of chronic subdural hematoma. Neurosurg. Rev. Scand. 2021, 44, 961–970. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Points Obtained |
|---|---|
| Age 80 years | 1 |
| GCS 15–12 | 0 |
| GCS 12–5 | 1 |
| GCS 4–3 | 2 |
| Hematoma volume 100 mL | 1 |
| Patient Characteristics | |||
|---|---|---|---|
| Number of patients | 131 | ||
| Sex (male:female) | 68:63 | ||
| Mean age (years ± SD) | 78.4 ± 7.4 | ||
| Mean hematoma size (mL) | 45 | ||
| History of anticoagulants/antiplatelet medication, n (%) | 103 (79) | ||
| Focal seizure, n (%) | 10 (7) | ||
| Generalized seizure, n (%) | 18 (14) | ||
| 30-day mortality, n (%) | 60 (46) | ||
| Surgical evacuation, n (%) | 99 (76) | ||
| Surgical evacuation vs. conservative treatment | |||
| SHE Score | Surgical evacuation | Conservative treatment | pvalues |
| Mean age (years ± SD) | 78.2 ± 7.2 | 79 ± 7.4 | 0.5882 |
| Sex (male:female) | 55:44 | 13:19 | 0.1588 |
| GCS by admission ± SD | 10.2 ± 4.6 | 9.5 ± 5.2 | 0.4700 |
| Focal seizure (%) | 8 (8) | 2 (6) | 0.0065 |
| Generalized seizure (%) | 18 (18) | 0 (0) | 0.7345 |
| 30-day mortality (%) | 45 (45) | 15 (47) | 0.99 |
| SHE 0 | 14 | 9 | |
| 30-days mortality | 0 (0%) | 1 (11.1%) | 0.3577 |
| SHE 1 | 24 | 9 | |
| 30-days mortality | 4 (16.6%) | 0 (0%) | |
| SHE 2 | 29 | 1 | |
| 30-days mortality | 10 (34.5%) | 1 (100%) | |
| SHE 3 | 26 | 8 | |
| 30-days mortality | 25 (96.1%) | 8 (100%) | 0.99 |
| SHE 4 | 6 | 5 | |
| 30-days mortality | 6 (100%) | 5 (100%) | 0.99 |
| Comparison Vychopen vs. Alford 30-Day Mortality | |||
|---|---|---|---|
| SHE Score | Vychopen 30-Day Mortality | Alford 30-Day Mortality | p Value |
| SHE 0 | 1/23 (4.3%) | 3/94 (3.2%) | 0.7135 |
| SHE 1 | 4/33 (12.1%) | 13/99 (13.1%) | 0.8807 |
| SHE 2 | 11/30 (36.6%) | 16/49 (32.7%) | 0.9039 |
| SHE 3 | 33/34 (97%) | 22/23 (95.6%) | 0.7771 |
| SHE 4 | 11/11 (100%) | 12/12 (100%) | 0.99 |
| Distribution of nonconvulsive Status epilepticus in correlation with SHE score. | |||
| SHE score | Nonconvulsive status epilepticus | % | |
| SHE 0 | 0/23 | 0 | |
| SHE 1 | 1/33 | 3 | |
| SHE 2 | 6/30 | 20 | |
| SHE 3 | 9/34 | 26.5 | |
| SHE 4 | 2/11 | 18.2 | |
| Variable | OR | CI 95% | p Value |
|---|---|---|---|
| Anticoagulation | 0.71 | 0.24–2.12 | 0.55 |
| SHE Score | 1.055 | 0.74–1.50 | 0.76 |
| Hematoma evacuation | 6.52 | 1.44–29.55 | 0.015 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vychopen, M.; Hamed, M.; Bahna, M.; Racz, A.; Ilic, I.; Salemdawod, A.; Schneider, M.; Lehmann, F.; Eichhorn, L.; Bode, C.; et al. A Validation Study for SHE Score for Acute Subdural Hematoma in the Elderly. Brain Sci. 2022, 12, 981. https://doi.org/10.3390/brainsci12080981
Vychopen M, Hamed M, Bahna M, Racz A, Ilic I, Salemdawod A, Schneider M, Lehmann F, Eichhorn L, Bode C, et al. A Validation Study for SHE Score for Acute Subdural Hematoma in the Elderly. Brain Sciences. 2022; 12(8):981. https://doi.org/10.3390/brainsci12080981
Chicago/Turabian StyleVychopen, Martin, Motaz Hamed, Majd Bahna, Attila Racz, Inja Ilic, Abdallah Salemdawod, Matthias Schneider, Felix Lehmann, Lars Eichhorn, Christian Bode, and et al. 2022. "A Validation Study for SHE Score for Acute Subdural Hematoma in the Elderly" Brain Sciences 12, no. 8: 981. https://doi.org/10.3390/brainsci12080981