
Clinical Study of Intraoperative Microelectrode Recordings during Awake and Asleep Subthalamic Nucleus Deep Brain Stimulation for Parkinson’s Disease: A Retrospective Cohort Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
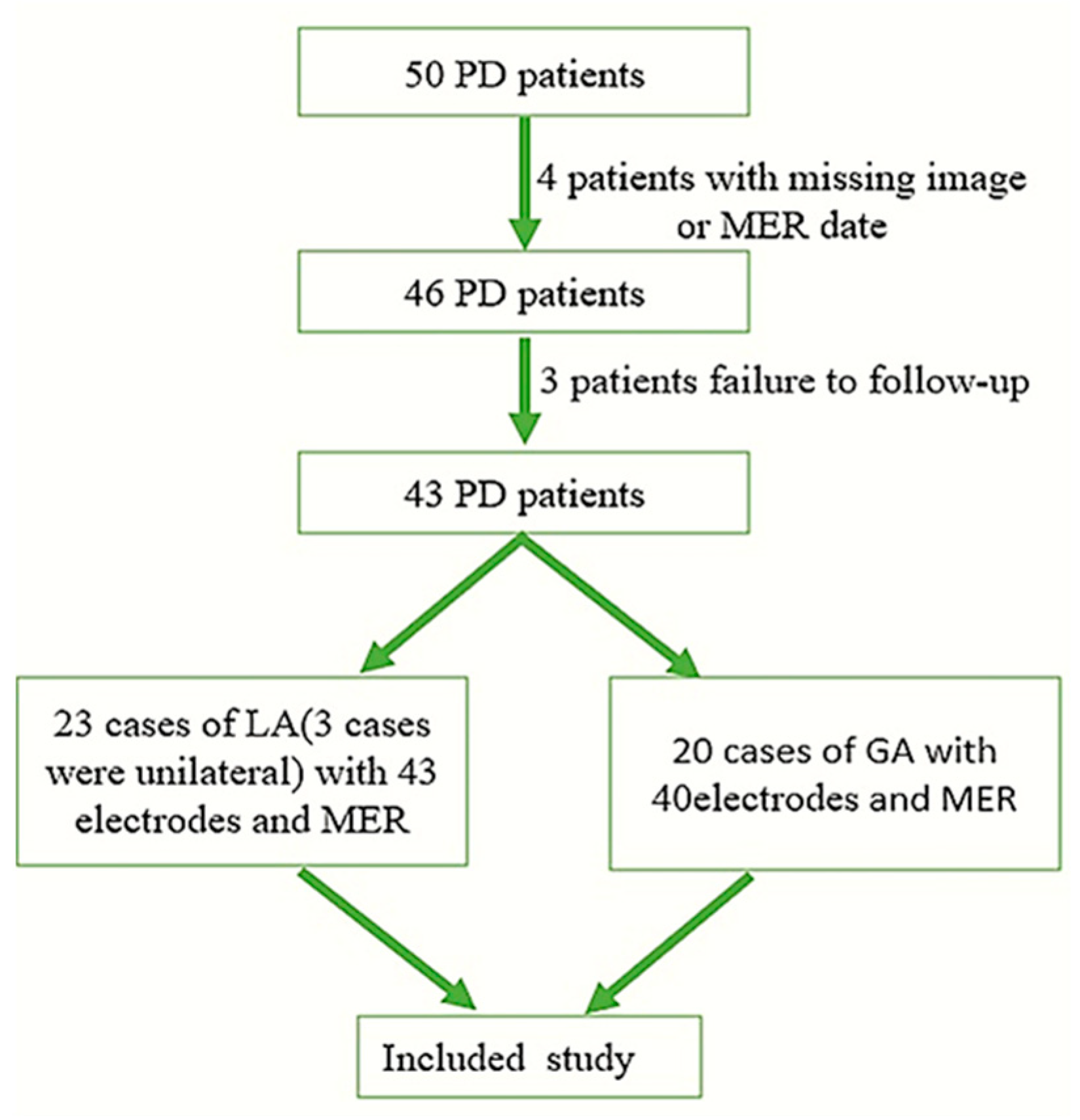
2.1. Participants
2.2. Target Planning
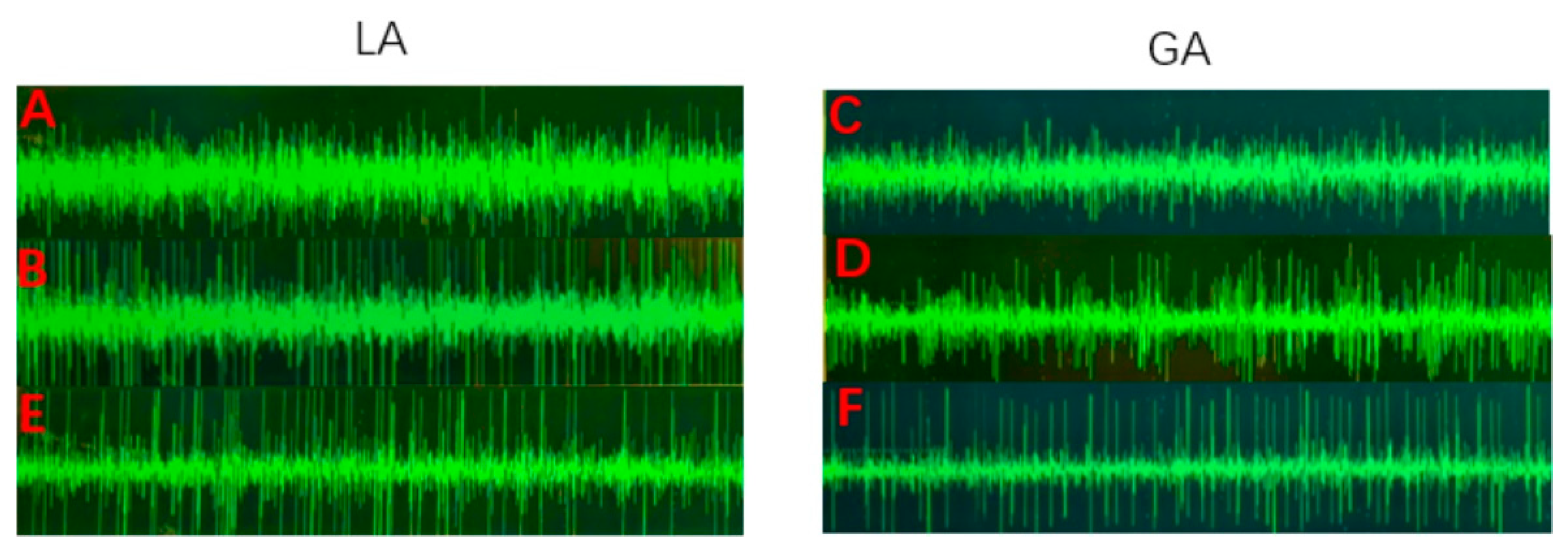
2.3. Electrophysiology Protocol
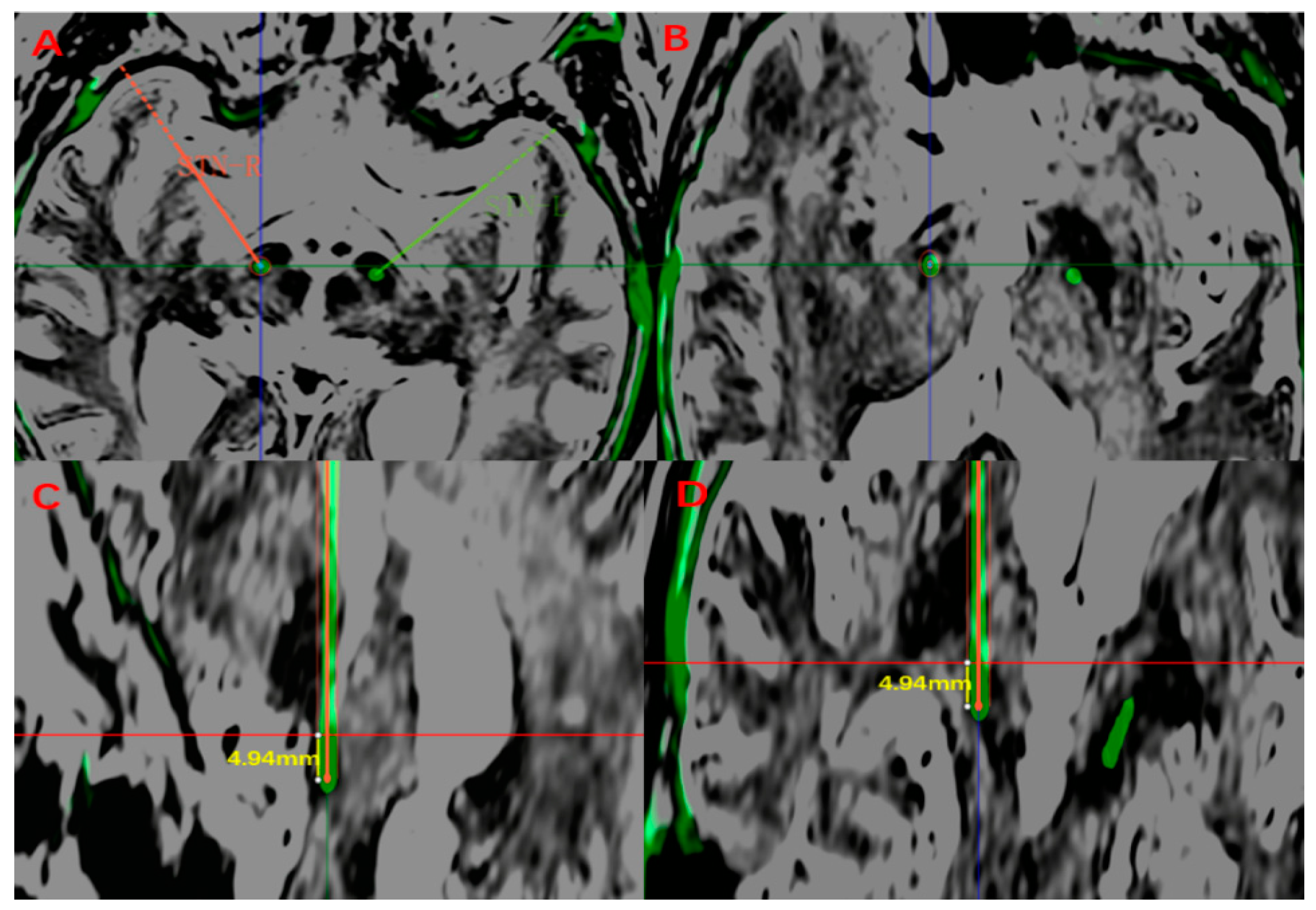
2.4. Measurements
2.5. Clinical Outcome Assessment
2.6. Statistical Analysis
3. Result
3.1. Patients
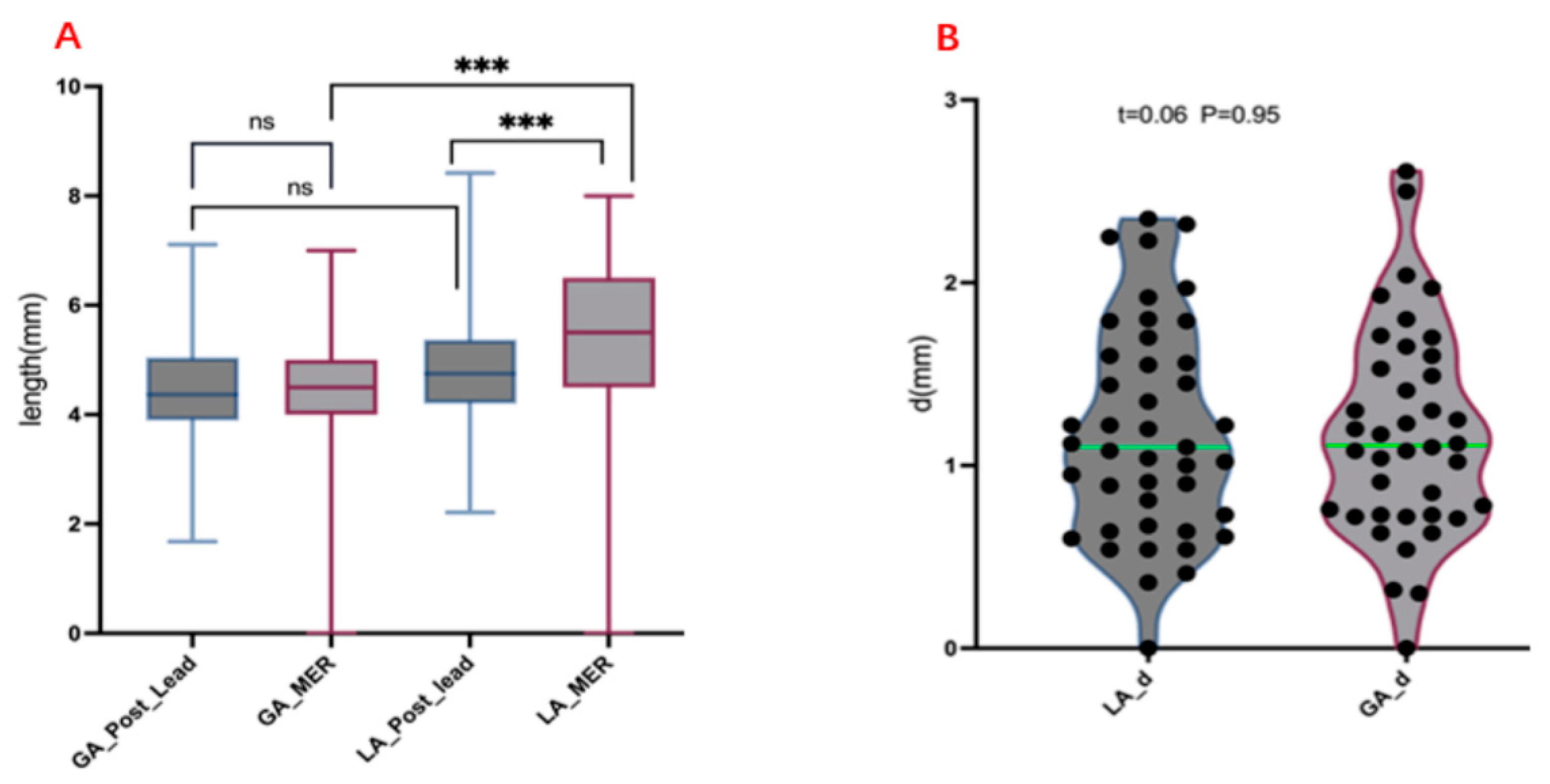
3.2. Measurement of Electrode Length and MER Length
3.3. Comparison of Prognosis and LEED between the Two Groups
4. Discussion
Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dorsey, E.R.; Bloem, B.R. The Parkinson Pandemic-A Call to Action. JAMA Neurol. 2018, 75, 9–10. [Google Scholar] [CrossRef] [PubMed]
- Merola, A.; Singh, J.; Reeves, K.; Changizi, B.; Goetz, S.; Rossi, L.; Pallavaram, S.; Carcieri, S.; Harel, N.; Shaikhouni, A.; et al. New Frontiers for Deep Brain Stimulation: Directionality, Sensing Technologies, Remote Programming, Robotic Stereotactic Assistance, Asleep Procedures, and Connectomics. Front. Neurol. 2021, 12, 694747. [Google Scholar] [CrossRef]
- Chen, T.; Mirzadeh, Z.; Ponce, F.A. “Asleep” Deep Brain Stimulation Surgery: A Critical Review of the Literature. World Neurosurg. 2017, 105, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Brodsky, M.A.; Anderson, S.; Murchison, C.; Seier, M.; Wilhelm, J.; Vederman, A.; Burchiel, K.J. Clinical outcomes of asleep vs awake deep brain stimulation for Parkinson disease. Neurology 2017, 89, 1944–1950. [Google Scholar] [CrossRef]
- Soares, M.I.; Soares-Dos-Reis, R.; Rosas, M.J.; Monteiro, P.; Massano, J. Intraoperative microelectrode recording in Parkinson’s disease subthalamic deep brain stimulation: Analysis of clinical utility. J. Clin. Neurosci. 2019, 69, 104–108. [Google Scholar] [CrossRef]
- Kocabicak, E.; Aygun, D.; Ozaydin, I.; Jahanshahi, A.; Tan, S.; Onar, M.; Boke, O.; Kurt, M.; Guz, H.; Terzi, M.; et al. Does probe’s eye subthalamic nucleus length on T2W MRI correspond with microelectrode recording in patients with deep brain stimulation for advanced Parkinson’s disease? Turk. Neurosurg. 2013, 23, 658–665. [Google Scholar]
- Verhagen Metman, L.; Slavin, K.V.; Rosenow, J.M.; Vitek, J.L.; van den Munckhof, P. More Than Just the Level of Consciousness: Comparing Asleep and Awake Deep Brain Stimulation. Mov. Disord. 2021, 36, 2763–2766. [Google Scholar] [CrossRef]
- Andrade-Souza, Y.M.; Schwalb, J.M.; Hamani, C.; Eltahawy, H.; Hoque, T.; Saint-Cyr, J.; Lozano, A.M. Comparison of three methods of targeting the subthalamic nucleus for chronic stimulation in Parkinson’s disease. Neurosurgery 2008, 62, 875–883. [Google Scholar] [CrossRef]
- Jiang, N.; Ling, Y.-T.; Yang, C.; Liu, Y.; Xian, W.-B.; Zhang, L.-N.; Guo, Q.-Q.; Jin, X.-Y.; Wu, B.; Zhang, C.-M.; et al. Optimized Propofol Anesthesia Increases Power of Subthalamic Neuronal Activity in Patients with Parkinson’s Disease Undergoing Deep Brain Stimulation. Neurol. Ther. 2021, 10, 785–802. [Google Scholar] [CrossRef]
- Rodriguez-Oroz, M.C.; Rodriguez, M.; Guridi, J.; Mewes, K.; Chockkman, V.; Vitek, J.; DeLong, M.R.; Obeso, J.A. The subthalamic nucleus in Parkinson’s disease: Somatotopic organization and physiological characteristics. Brain 2001, 124, 1777–1790. [Google Scholar] [CrossRef]
- Maltête, D.; Jodoin, N.; Karachi, C.; Houeto, J.L.; Navarro, S.; Cornu, P.; Agid, Y.; Welter, M.L. Subthalamic stimulation and neuronal activity in the substantia nigra in Parkinson’s disease. J. Neurophysiol. 2007, 97, 4017–4022. [Google Scholar] [CrossRef]
- Nowacki, A.; Debove, I.; Fiechter, M.; Rossi, F.; Oertel, M.F.; Wiest, R.; Schüpbach, M.; Pollo, C. Targeting Accuracy of the Subthalamic Nucleus in Deep Brain Stimulation Surgery: Comparison Between 3 T T2-Weighted Magnetic Resonance Imaging and Microelectrode Recording Results. Oper. Neurosurg. 2018, 15, 66–71. [Google Scholar] [CrossRef]
- Peto, V.; Jenkinson, C.; Fitzpatrick, R.; Greenhall, R. The development and validation of a short measure of functioning and wellbeing for individuals with Parkinson’s disease. Qual. Life Res. 1995, 4, 241–248. [Google Scholar] [CrossRef]
- Tomlinson, C.L.; Stowe, R.; Patel, S.; Rick, C.; Gray, R.; Clarke, C.E. Systematic review of levodopa dose equivalency reporting in Parkinson’s disease. Mov. Disord. 2010, 25, 2649–2653. [Google Scholar] [CrossRef]
- Ivan, M.E.; Yarlagadda, J.; Saxena, A.P.; Martin, A.J.; Starr, P.A.; Sootsman, W.K.; Larson, P.S. Brain shift during bur hole-based procedures using interventional MRI. J. Neurosurg. 2014, 121, 149–160. [Google Scholar] [CrossRef]
- Maciunas, R.J.; Galloway, R.L., Jr.; Latimer, J.W. The application accuracy of stereotactic frames. Neurosurgery 1994, 35, 682–694. [Google Scholar] [CrossRef]
- Burke, J.F.; Tanzillo, D.; Starr, P.A.; Lim, D.A.; Larson, P.S. CT and MRI Image Fusion Error: An Analysis of Co-Registration Error Using Commercially Available Deep Brain Stimulation Surgical Planning Software. Stereotact. Funct. Neurosurg. 2021, 99, 196–202. [Google Scholar] [CrossRef]
- Zheng, Z.; Zhu, Z.; Ying, Y.; Jiang, H.; Wu, H.; Tian, J.; Luo, W.; Zhu, J. The Accuracy of Imaging Guided Targeting with Microelectrode Recoding in Subthalamic Nucleus for Parkinson’s Disease: A Single-Center Experience. J. Park. Dis. 2022, 12, 897–903. [Google Scholar] [CrossRef]
- Holewijn, R.A.; Verbaan, D.; van den Munckhof, P.M.; Bot, M.; Geurtsen, G.J.; Dijk, J.M.; Odekerken, V.J.; Beudel, M.; de Bie, R.M.A.; Schuurman, P.R. General Anesthesia vs Local Anesthesia in Microelectrode Recording-Guided Deep-Brain Stimulation for Parkinson Disease: The GALAXY Randomized Clinical Trial. JAMA Neurol. 2021, 78, 1212–1219. [Google Scholar] [CrossRef]
- Engelhardt, J.; Caire, F.; Damon-Perrière, N.; Guehl, D.; Branchard, O.; Auzou, N.; Tison, F.; Meissner, W.G.; Krim, E.; Bannier, S.; et al. A Phase 2 Randomized Trial of Asleep versus Awake Subthalamic Nucleus Deep Brain Stimulation for Parkinson’s Disease. Stereotact. Funct. Neurosurg. 2021, 99, 230–240. [Google Scholar] [CrossRef]
- Ho, A.L.; Ali, R.; Connolly, I.D.; Henderson, J.M.; Dhall, R.; Stein, S.C.; Halpern, C.H. Awake versus asleep deep brain stimulation for Parkinson’s disease: A critical comparison and meta-analysis. J. Neurol. Neurosurg. Psychiatry 2018, 89, 687–691. [Google Scholar] [CrossRef]
- Chen, T.; Mirzadeh, Z.; Chapple, K.M.; Lambert, M.; Shill, H.A.; Moguel-Cobos, G.; Tröster, A.I.; Dhall, R.; Ponce, F.A. Clinical outcomes following awake and asleep deep brain stimulation for Parkinson disease. J. Neurosurg. 2018, 130, 109–120. [Google Scholar] [CrossRef] [Green Version]
- Shenai, M.B.; Patel, D.M.; Romeo, A.; Whisenhunt, J.D.; Walker, H.C.; Guthrie, S.; Guthrie, B.L. The Relationship of Electrophysiologic Subthalamic Nucleus Length as a Predictor of Outcomes in Deep Brain Stimulation for Parkinson Disease. Stereotact. Funct. Neurosurg. 2017, 95, 341–347. [Google Scholar] [CrossRef]
- Frequin, H.L.; Bot, M.; Dilai, J.; Scholten, M.N.; Postma, M.; Bour, L.J.; Contarino, M.F.; de Bie, R.M.A.; Schuurman, P.R.; van den Munckhof, P. Relative Contribution of Magnetic Resonance Imaging, Microelectrode Recordings, and Awake Test Stimulation in Final Lead Placement during Deep Brain Stimulation Surgery of the Subthalamic Nucleus in Parkinson’s Disease. Stereotact. Funct. Neurosurg. 2020, 98, 118–128. [Google Scholar] [CrossRef]
- Wodarg, F.; Herzog, J.; Reese, R.; Falk, D.; Pinsker, M.O.; Steigerwald, F.; Jansen, O.; Deuschl, G.; Mehdorn, H.M.; Volkmann, J. Stimulation site within the MRI-defined STN predicts postoperative motor outcome. Mov. Disord. 2012, 27, 874–879. [Google Scholar] [CrossRef]
- Kulisevsky, J.; Berthier, M.L.; Gironell, A.; Pascual-Sedano, B.; Molet, J.; Parés, P. Mania following deep brain stimulation for Parkinson’s disease. Neurology 2002, 59, 1421–1424. [Google Scholar] [CrossRef] [Green Version]
- Bejjani, B.P.; Damier, P.; Arnulf, I.; Thivard, L.; Bonnet, A.M.; Dormont, D.; Cornu, P.; Pidoux, B.; Samson, Y.; Agid, Y. Transient acute depression induced by high-frequency deep-brain stimulation. N. Engl. J. Med. 1999, 340, 1476–1480. [Google Scholar] [CrossRef]
- Weiss, D.; Walach, M.; Meisner, C.; Fritz, M.; Scholten, M.; Breit, S.; Plewnia, C.; Bender, B.; Gharabaghi, A.; Wächter, T.; et al. Nigral stimulation for resistant axial motor impairment in Parkinson’s disease? A randomized controlled trial. Brain 2013, 136, 2098–2108. [Google Scholar] [CrossRef] [Green Version]
- Valldeoriola, F.; Muñoz, E.; Rumià, J.; Roldán, P.; Cámara, A.; Compta, Y.; Martí, M.J.; Tolosa, E. Simultaneous low-frequency deep brain stimulation of the substantia nigra pars reticulata and high-frequency stimulation of the subthalamic nucleus to treat levodopa unresponsive freezing of gait in Parkinson’s disease: A pilot study. Park. Relat. Disord. 2019, 60, 153–157. [Google Scholar] [CrossRef] [Green Version]
- Bos, M.J.; Buhre, W.; Temel, Y.; Joosten, E.A.J.; Absalom, A.R.; Janssen, M.L.F. Effect of Anesthesia on Microelectrode Recordings During Deep Brain Stimulation Surgery: A Narrative Review. J. Neurosurg. Anesthesiol. 2021, 33, 300–307. [Google Scholar] [CrossRef]
- Kwon, W.-K.; Kim, J.H.; Lee, J.-H.; Lim, B.-G.; Lee, I.-O.; Koh, S.B.; Kwon, T.H. Microelectrode recording (MER) findings during sleep-awake anesthesia using dexmedetomidine in deep brain stimulation surgery for Parkinson’s disease. Clin. Neurol. Neurosurg. 2016, 143, 27–33. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| GA (n = 20) | LA (n = 23) | p Value | |
|---|---|---|---|
| Sex ratio (M/F) | 12/8 | 14/9 | 0.95 |
| Age in years (mean ± SD) | 68.05 ± 8.62 | 64.48 ± 5.95 | 0.07 |
| Years since PD diagnosis | 7.60 ± 2.06 | 7.22 ± 3.53 | 0.22 |
| Baseline UPDRS III (mean ± SD) | 50.31 ± 19.64 | 47.70 ± 15.18 | 0.63 |
| Baseline LEDD (mean ± SD) | 711.16 ± 375.34 | 790.88 ± 346.31 | 0.47 |
| Duration of use of medication (mean ± SD) | 5.71 ± 3.07 | 6.05 ± 3.27 | 0.72 |
| PDQ39(mean ± SD) | 32.86 ± 17.77 | 29.62 ± 20.82 | 0.59 |
| HAMA (mean ± SD) | 12.95 ± 8.08 | 11.52 ± 8.53 | 0.43 |
| HAMD (mean ± SD) | 14.05 ± 8.16 | 11.91 ± 8.37 | 0.31 |
| MoCA (mean ± SD) | 23.95 ± 3.40 | 24.52 ± 2.98 | 0.78 |
| MMSE (mean ± SD) | 26.10 ± 2.45 | 26.09 ± 2.78 | 0.87 |
| Post-Lead Length (mm) | MER Length (mm) | d (mm) | Post-Lead Length vs. MER Length | |
|---|---|---|---|---|
| LA (n = 43) | 4.69 ± 1.14 | 5.48 ± 1.39 | 1.19 ± 0.58 | T = −4.27 p = 0.001 |
| GA (n = 40) | 4.47 ± 1.13 | 4.38 ± 1.43 | 1.18 ± 0.57 | T = 0.50 p = 0.61 |
| p | 0.38 | 0.001 | 0.95 |
| GA | LA | p Value | |
|---|---|---|---|
| Post-LEED (mean ± SD) | 507.64 ± 207.01 | 539.61 ± 129.81 | 0.56 |
| Post-UPDRS III (mean ± SD) | 24.40 ± 10.69 | 25.00 ± 9.96 | 0.85 |
| Post-HAMA (mean ± SD) | 10.55 ± 4.99 | 9.61 ± 6.15 | 0.36 |
| Post-HAMD (mean ± SD) | 11.05 ± 4.57 | 10.78 ± 6.94 | 0.43 |
| Post-MoCA (mean ± SD) | 23.75 ± 3.70 | 24.74 ± 2.53 | 0.49 |
| Post-MMSE (mean ± SD) | 25.80 ± 2.33 | 25.70 ± 2.84 | 0.99 |
| Post-PDQ39 (mean ± SD) | 30.59 ± 16.23 | 23.46 ± 15.78 | 0.15 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, G.-R.; Cheng, Y.-F.; Feng, K.-K.; Wang, M.; Wang, Y.-G.; Wu, Y.-Z.; Yin, S.-Y. Clinical Study of Intraoperative Microelectrode Recordings during Awake and Asleep Subthalamic Nucleus Deep Brain Stimulation for Parkinson’s Disease: A Retrospective Cohort Study. Brain Sci. 2022, 12, 1469. https://doi.org/10.3390/brainsci12111469
Zhao G-R, Cheng Y-F, Feng K-K, Wang M, Wang Y-G, Wu Y-Z, Yin S-Y. Clinical Study of Intraoperative Microelectrode Recordings during Awake and Asleep Subthalamic Nucleus Deep Brain Stimulation for Parkinson’s Disease: A Retrospective Cohort Study. Brain Sciences. 2022; 12(11):1469. https://doi.org/10.3390/brainsci12111469
Chicago/Turabian StyleZhao, Guang-Rui, Yi-Feng Cheng, Ke-Ke Feng, Min Wang, Yan-Gang Wang, Yu-Zhang Wu, and Shao-Ya Yin. 2022. "Clinical Study of Intraoperative Microelectrode Recordings during Awake and Asleep Subthalamic Nucleus Deep Brain Stimulation for Parkinson’s Disease: A Retrospective Cohort Study" Brain Sciences 12, no. 11: 1469. https://doi.org/10.3390/brainsci12111469