
The Long-Term Efficacy, Prognostic Factors, Safety, and Hospitalization Costs Following Denervation and Myotomy of the Affected Muscles and Deep Brain Stimulation in 94 Patients with Spasmodic Torticollis

Abstract
:1. Introduction
2. Methods
2.1. Patients
2.2. DAM Techniques
2.3. DBS Surgical Procedure
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Camfield, L.; Ben-Shlomo, Y.; Warner, T.T. Epidemiological Study of Dystonia in Europe Collaborative Group: Impact of cervical dystonia on quality of life. Mov. Disord. 2002, 17, 838–841. [Google Scholar] [CrossRef] [PubMed]
- Brans, J.; Lindeboom, R.; Snoek, J.W.; Zwarts, M.J.; Van Weerden, T.W.; Brunt, E.; Van Hilten, J.J.; Van Der Kamp, W.; Prins, M.H.; Speelman, J.D. Botulinum toxin versus trihexyphenidyl in cervical dystonia: A prospective, randomized, double-blind controlled trial. Neurology 1996, 46, 1066–1072. [Google Scholar] [CrossRef] [PubMed]
- Benecke, R.; Moore, P.; Dressler, D.; Naumann, M. Cervical and axial dystonia. In Handbook of Botulinum Toxin Treatment; Moore, P., Naumann, M., Eds.; Wiley-Blackwell: Oxford, UK, 2003. [Google Scholar]
- Wang, J.; Li, J.; Han, L.; Guo, S.; Wang, L.; Xiong, Z.; Ma, J.; Liang, J.; Wang, L. Selective peripheral denervation for the treatment of spasmodic torticollis: Long-term follow-up results from 648 patients. Acta Neurochir. 2015, 157, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Ma, A.; Liang, J.; Ji, S.; Pei, S. Selective Denervation and Resection of Cervical Muscles in the Treatment of Spasmodic Torticollis: Long-Term Follow-Up Results in 207 Cases. Ster. Funct. Neurosurg. 2000, 75, 96–102. [Google Scholar] [CrossRef]
- Bertrand, C.; Molina-Negro, P.; Bouvier, G.; Gorczyca, W. Observations and Analysis of Results in 131 Cases of Spasmodic Torticollis after Selective Denervation. Ster. Funct. Neurosurg. 1987, 50, 319–323. [Google Scholar] [CrossRef]
- Bertrand, C.M. Selective peripheral denervation for spasmodic torticollis: Surgical technique, results, and observations in 260 cases. Surg. Neurol. 1993, 40, 96–103. [Google Scholar] [CrossRef]
- Chen, X.K.; Ji, S.X.; Zhu, G.H.; Ma, A.B. Operative treatment of bilateral retrocollis. Acta Neurochir. 1991, 113, 180–183. [Google Scholar] [CrossRef]
- Sun, K.; Lu, Y.; Hu, G.; Luo, C.; Hou, L.; Chen, J.; Wu, X.; Mei, Q. Microvascular decompression of the accessory nerve for treatment of spasmodic torticollis: Early results in 12 cases. Acta Neurochir. 2009, 151, 1251–1257. [Google Scholar] [CrossRef]
- Tsui, J.; Stoessl, A.J.; Eisen, A.; Calne, S.; Calne, D. Double-Blind Study of Botulinum Toxin in Spasmodic Torticollis. Lancet 1986, 328, 245–247. [Google Scholar] [CrossRef]
- Consky, E.S.; Lang, A.E. Clinical assessments of patients with cervical dystonia. In Therapy with Botulinum Toxin; Jankovic, J., Hallett, M., Eds.; Marcel Dekker: New York, NY, USA, 1994; pp. 211–237. [Google Scholar]
- Arce, C.; Russo, J. Selective peripheral denervation: A surgical alternative in the treatment for spasmodic torticollis: Review of 55 patients. Mov. Disord. 1992, 7, S128–S129. [Google Scholar]
- Davis, D.H.; Ahlskog, J.E.; Litchy, W.J.; Root, L.M. Selective Peripheral Denervation for Torticollis: Preliminary Results. Mayo Clin. Proc. 1991, 66, 365–371. [Google Scholar] [CrossRef]
- Bertrand, C.; Negro, P.M.; Martinez, S. Technical Aspects of Selective Peripheral Denervation for Spasmodic Torticollis. Ster. Funct. Neurosurg. 1982, 45, 326–330. [Google Scholar] [CrossRef] [PubMed]
- Meyer, C. Outcome of Selective Peripheral Denervation for Cervical Dystonia. Ster. Funct. Neurosurg. 2001, 77, 44–47. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Richter, H.-P. Selective peripheral denervation for spasmodic torticollis: 13-year experience with 155 patients. J. Neurosurg. Spine 2002, 97, 207–212. [Google Scholar] [CrossRef] [Green Version]
- Kupsch, A.; Benecke, R.; Müller, J.; Trottenberg, T.; Schneider, G.-H.; Poewe, W.; Eisner, W.; Wolters, A.; Müller, J.-U.; Deuschl, G.; et al. Pallidal Deep-Brain Stimulation in Primary Generalized or Segmental Dystonia. N. Engl. J. Med. 2006, 355, 1978–1990. [Google Scholar] [CrossRef] [Green Version]
- Vidailhet, M.; Vercueil, L.; Houeto, J.-L.; Krystkowiak, P.; Benabid, A.-L.; Cornu, P.; Lagrange, C.; du Montcel, S.T.; Dormont, D.; Grand, S.; et al. Bilateral Deep-Brain Stimulation of the Globus Pallidus in Primary Generalized Dystonia. N. Engl. J. Med. 2005, 352, 459–467. [Google Scholar] [CrossRef] [Green Version]
- Kiss, Z.H.; Doig-Beyaert, K.; Eliasziw, M.; Tsui, J.; Haffenden, A.; Suchowersky, O. Functional and Stereotactic Section of the Canadian Neurosurgical Society; Canadian Movement Disorders Group—The Canadian multicentre study of deep brain stimulation for cervical dystonia. Brain 2007, 130, 2879–2886. [Google Scholar] [CrossRef]
- Volkmann, J.; Mueller, J.; Deuschl, G.; A Kühn, A.; Krauss, J.K.; Poewe, W.; Timmermann, L.; Falk, D.; Kupsch, A.; Kivi, A.; et al. Pallidal neurostimulation in patients with medication-refractory cervical dystonia: A randomised, sham-controlled trial. Lancet Neurol. 2014, 13, 875–884. [Google Scholar] [CrossRef]
- Bittar, R.G.; Yianni, J.; Wang, S.; Liu, X.; Nandi, D.; Joint, C.; Scott, R.; Bain, P.G.; Gregory, R.; Stein, J.; et al. Deep brain stimulation for generalised dystonia and spasmodic torticollis. J. Clin. Neurosci. 2005, 12, 12–16. [Google Scholar] [CrossRef]
- Jeong, S.-G.; Lee, M.-K.; Kang, J.-Y.; Jun, S.-M.; Lee, W.-H.; Ghang, C.-G. Pallidal Deep Brain Stimulation in Primary Cervical Dystonia with Phasic Type: Clinical Outcome and Postoperative Course. J. Korean Neurosurg. Soc. 2009, 46, 346–350. [Google Scholar] [CrossRef]
- Hung, S.W.; Hamani, C.; Lozano, A.; Poon, Y.-Y.W.; Piboolnurak, P.; Miyasaki, J.M.; Lang, A.; Dostrovsky, J.O.; Hutchison, W.D.; Moro, E. Long-term outcome of bilateral pallidal deep brain stimulation for primary cervical dystonia. Neurology 2007, 68, 457–459. [Google Scholar] [CrossRef] [PubMed]
- Cacciola, F.; Farah, J.O.; Eldridge, P.R.; Byrne, P.; Varma, T.K. Bilateral Deep Brain Stimulation for Cervical Dystonia: Long-term Outcome in a Series of 10 Patients. Neurosurgery 2010, 67, 957–963. [Google Scholar] [CrossRef] [PubMed]
- Witt, J.L.; Moro, E.; Ash, R.S.; Hamani, C.; Starr, P.A.; Lozano, A.M.; Hodaie, M.; Poon, Y.-Y.; Markun, L.C.; Ostrem, J.L. Predictive factors of outcome in primary cervical dystonia following pallidal deep brain stimulation. Mov. Disord. 2013, 28, 1451–1455. [Google Scholar] [CrossRef] [PubMed]
- Tsuboi, T.; Wong, J.K.; Almeida, L.; Hess, C.W.; Shukla, A.W.; Foote, K.D.; Okun, M.S.; Ramirez-Zamora, A. A pooled meta-analysis of GPi and STN deep brain stimulation outcomes for cervical dystonia. J. Neurol. 2020, 267, 1278–1290. [Google Scholar] [CrossRef]
- Hua, X.; Zhang, B.; Zheng, Z.; Fan, H.; Luo, L.; Chen, X.; Duan, J.; Zhou, D.; Li, M.; Hong, T.; et al. Predictive factors of outcome in cervical dystonia following deep brainstimulation: An individual patient data meta-analysis. J Neurol. 2020, 267, 1780–1792. [Google Scholar] [CrossRef]
- Huh, R.; Han, I.B.; Chung, M.; Chung, S. Comparison of Treatment Results between Selective Peripheral Denervation and Deep Brain Stimulation in Patients with Cervical Dystonia. Ster. Funct. Neurosurg. 2010, 88, 234–238. [Google Scholar] [CrossRef]
- Contarino, M.F.; Munckhof, P.V.D.; Tijssen, M.A.J.; De Bie, R.M.A.; Bosch, D.A.; Schuurman, P.R.; Speelman, J.D. Selective peripheral denervation: Comparison with pallidal stimulation and literature review. J. Neurol. 2013, 261, 300–308. [Google Scholar] [CrossRef]
- Lad, S.P.; Kalanithi, P.S.; Patil, C.G.; Itthimathin, P.; Batya, S.; Bronte-Stewart, H.; Boakye, M.; Henderson, J.M. Socioeconomic Trends in Deep Brain Stimulation (DBS) Surgery. Neuromodulation Technol. Neural Interface 2010, 13, 182–186. [Google Scholar] [CrossRef]
- Eskandar, E.N.; Flaherty, A.; Cosgrove, G.R.; Shinobu, L.A.; Barker, F.G. Surgery for Parkinson disease in the United States, 1996 to 2000: Practice patterns, short-term outcomes, and hospital charges in a nationwide sample. J. Neurosurg. 2003, 99, 863–871. [Google Scholar] [CrossRef]
- Sharma, M.; Ambekar, S.; Guthikonda, B.; Wilden, J.; Nanda, A. Regional trends and the impact of various patient and hospital factors on outcomes and costs of hospitalization between academic and nonacademic centers after deep brain stimulation surgery for Parkinson’s disease: A United States Nationwide Inpatient Sample analysis from 2006 to 2010. Neurosurg. Focus 2013, 35, E2. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| DAM (n = 41) | DBS (n = 53) | t/χ2 | p-Value | |
|---|---|---|---|---|
| Sex | χ2 = 0.941 | p = 0.404 | ||
| M | 25 (61.0%) | 27 (50.9%) | ||
| F | 16 (39.0%) | 26 (49.1%) | ||
| Age (Y) | 49.44 ± 11.54 | 44.79 ± 12.88 | t = 1.814 | p = 0.073 |
| DOS (M) | 41.66 ± 46.64 | 47.11 ± 49.06 | z = −0.332 | p = 0.740 |
| FU (M) | 105.46 ± 18.02 | 40.49 ± 19.82 | z = −8.072 | p < 0.001 * |
| ME (USD) | 5934.03 ± 2086.95 | 40,636.54 ± 1046.88 | z = −8.284 | p < 0.001 * |
| Surgical Procedure | Case | |
|---|---|---|
| DAM | Triad procedure [4,5] | 19 |
| Extradural section of the roots of C1 and C2, combined with section of the posterior primary divisions (ramisectomy) of C3, C4 and C5 + denervation of contralateral SCM with a transection of the muscle | 14 | |
| Ipsilateral microvascular decompression of the accessory nerve [9] + subdural selective C3-5 sensory nerve root rhizotomy | 4 | |
| Denervation of contralateral SCM with a transection of the muscle | 2 | |
| Bilateral myotomies of the splenius capitis/cervicis and semispinalis capitis/cervicis | 2 | |
| DBS | GPI-DBS | 49 |
| STN-DBS | 3 | |
| VIM-DBS | 1 | |
| Total | 94 | |
| Group | p-Value | Pre-O and Post-O | |
|---|---|---|---|
| TWSTRS Score | Tsui Score | ||
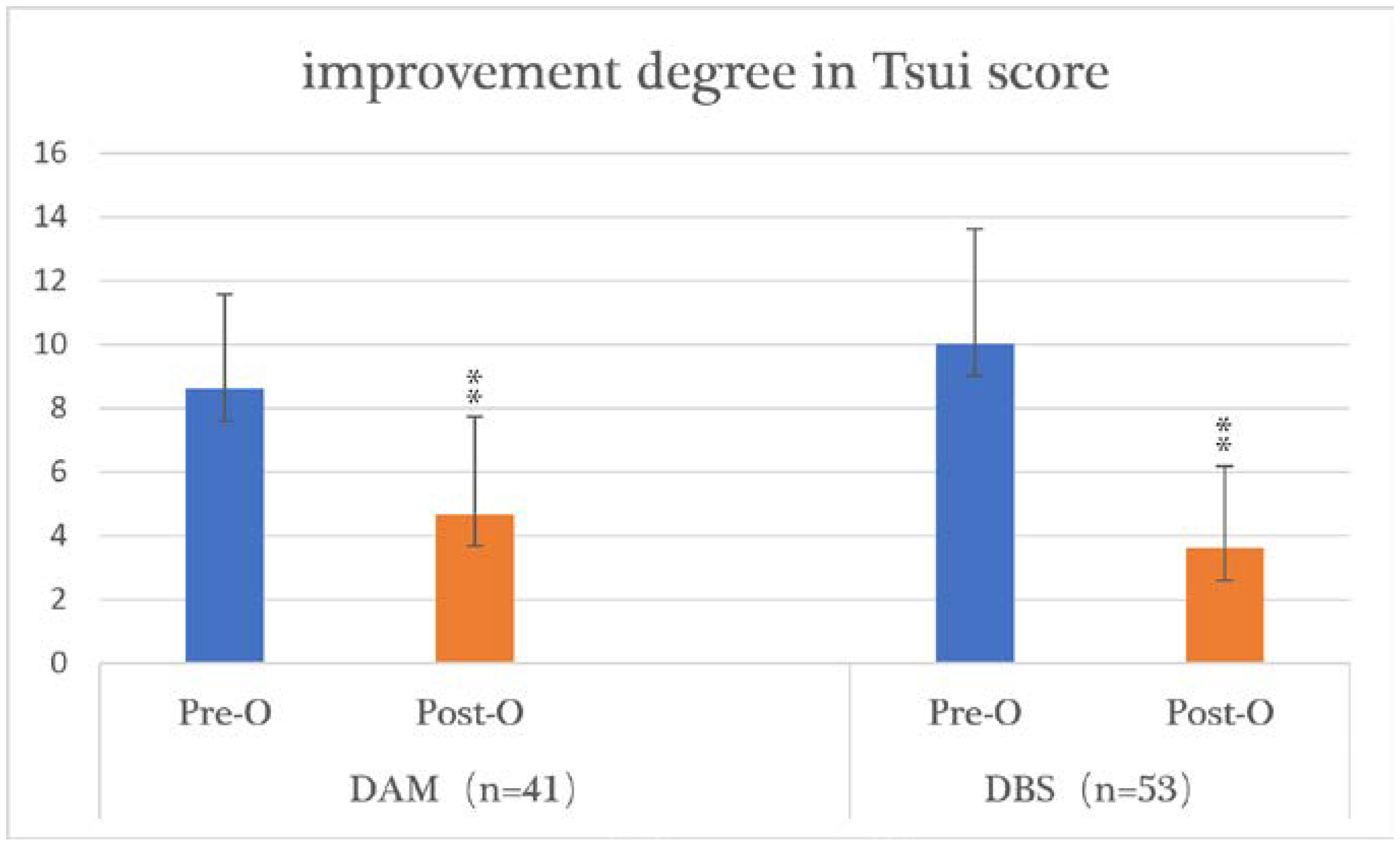
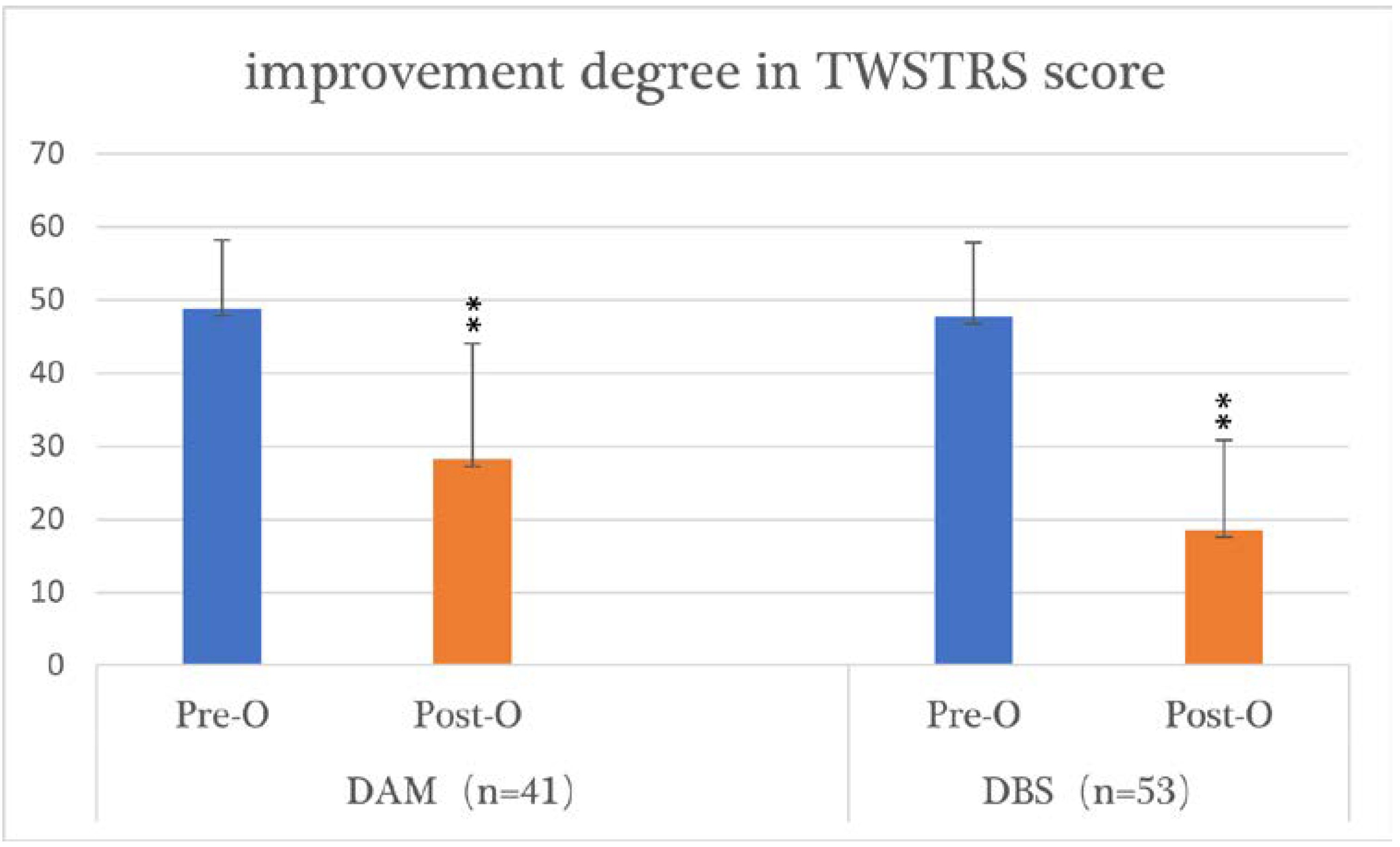
| DAM (n = 41) | t (z) | 8.762 | −5.103 |
| p | 0.000 * | 0.000 * | |
| Improvement (%) | 42.20 | 45.64 | |
| DBS (n = 53) | t (z) | −6.308 | −6.210 |
| p | 0.000 * | 0.000 * | |
| Improvement (%) | 61.08 | 63.87 | |
| DAM and DBS (n = 94) | t (z) | −3.161 | −1.796 |
| p | 0.002 * | 0.072 | |
| Factors | p-Value | Pre-O TWSTRS Score | Post-O TWSTRS Score | Pre-O Tsui Score | Post-O Tsui Score | |
|---|---|---|---|---|---|---|
| Sex | M (25), F (16) | t (z) | −1.572 | 0.323 | −1.029 (z) | −0.111 |
| p | 0.124 | 0.749 | 0.304 | 0.912 | ||
| Age at surgery (years) | ≤40 and >40 | t (z) | −0.542 | −0.898 (z) | −0.242 | −0.162 |
| p | 0.591 | 0.369 | 0.810 | 0.872 | ||
| ≤50 and >50 | t (z) | 0.304 | −0.817 | −0.675 (z) | −0.613 | |
| p | 0.763 | 0.419 | 0.500 | 0.542 | ||
| Disease duration (months) | ≤24 and >24 | t (z) | −3.800 | 1.479 | −0.745 (z) | −0.728 |
| p | 0.000 * | 0.145 | 0.456 | 0.467 | ||
| ≤60 and >60 | t (z) | −0.352 | −0.996 | −1.738 | −1.219 | |
| p | 0.727 | 0.325 | 0.090 | 0.230 | ||
| Follow-up period (months) | ≤100 and >100 | t (z) | −0.412 | 1.226 | 1.096 | −1.278 (z) |
| p | 0.683 | 0.228 | 0.280 | 0.201 |
| Factors | p-Value | Pre-O TWSTRS Score | Post-O TWSTRS Score | Pre-O Tsui Score | Post-O Tsui Score | |
|---|---|---|---|---|---|---|
| Sex | M (27), F (26) | t (z) | −2.119 | −0.810 | 0.564 | −0.405 |
| p | 0.034 * | 0.418 | 0.575 | 0.687 | ||
| Age at surgery (years) | ≤40 and >40 | t (z) | −1.225 | −1.856 | −1.384 | −0.272 |
| p | 0.221 | 0.063 | 0.172 | 0.786 | ||
| ≤50 and >50 | t (z) | −0.357 | −1.353 | −2.930 | −0.874 | |
| p | 0.721 | 0.176 | 0.003 * | 0.382 | ||
| Disease duration (months) | ≤12 and >12 | t (z) | 0.733 | −1.581 | 0.986 | −1.298 |
| p | 0.467 | 0.114 | 0.329 | 0.194 | ||
| ≤24 and >24 | t (z) | −0.614 | −0.240 | 1.338 | −0.020 | |
| p | 0.539 | 0.810 | 0.187 | 0.984 | ||
| ≤60 and >60 | t (z) | −1.478 | −1.106 | −1.726 | −0.116 | |
| p | 0.139 | 0.269 | 0.084 | 0.908 | ||
| Follow-up period (months) | ≤24 and >24 | t (z) | −1.620 | −0.079 | −1.530 | −1.428 |
| p | 0.105 | 0.937 | 0.126 | 0.153 | ||
| ≤36 and >36 | t (z) | −0.241 | −1.114 | −1.784 | −1.740 | |
| p | 0.810 | 0.265 | 0.074 | 0.082 | ||
| ≤48 and >48 | t (z) | −1.034 | −2.068 | −2.892 | −3.287 | |
| p | 0.301 | 0.039 * | 0.004 | 0.001 * | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cui, Z.; Chen, T.; Wang, J.; Jiang, C.; Gao, Q.; Mao, Z.; Pan, L.; Ling, Z.; Zhang, J.; Li, X. The Long-Term Efficacy, Prognostic Factors, Safety, and Hospitalization Costs Following Denervation and Myotomy of the Affected Muscles and Deep Brain Stimulation in 94 Patients with Spasmodic Torticollis. Brain Sci. 2022, 12, 881. https://doi.org/10.3390/brainsci12070881
Cui Z, Chen T, Wang J, Jiang C, Gao Q, Mao Z, Pan L, Ling Z, Zhang J, Li X. The Long-Term Efficacy, Prognostic Factors, Safety, and Hospitalization Costs Following Denervation and Myotomy of the Affected Muscles and Deep Brain Stimulation in 94 Patients with Spasmodic Torticollis. Brain Sciences. 2022; 12(7):881. https://doi.org/10.3390/brainsci12070881
Chicago/Turabian StyleCui, Zhiqiang, Tong Chen, Jian Wang, Chao Jiang, Qingyao Gao, Zhiqi Mao, Longsheng Pan, Zhipei Ling, Jianning Zhang, and Xuemei Li. 2022. "The Long-Term Efficacy, Prognostic Factors, Safety, and Hospitalization Costs Following Denervation and Myotomy of the Affected Muscles and Deep Brain Stimulation in 94 Patients with Spasmodic Torticollis" Brain Sciences 12, no. 7: 881. https://doi.org/10.3390/brainsci12070881