
Correlation between Electrode Location and Anxiety Depression of Subthalamic Nucleus Deep Brain Stimulation in Parkinson’s Disease

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Clinical Evaluation
2.3. Surgical Procedures
2.4. Postoperative Programming
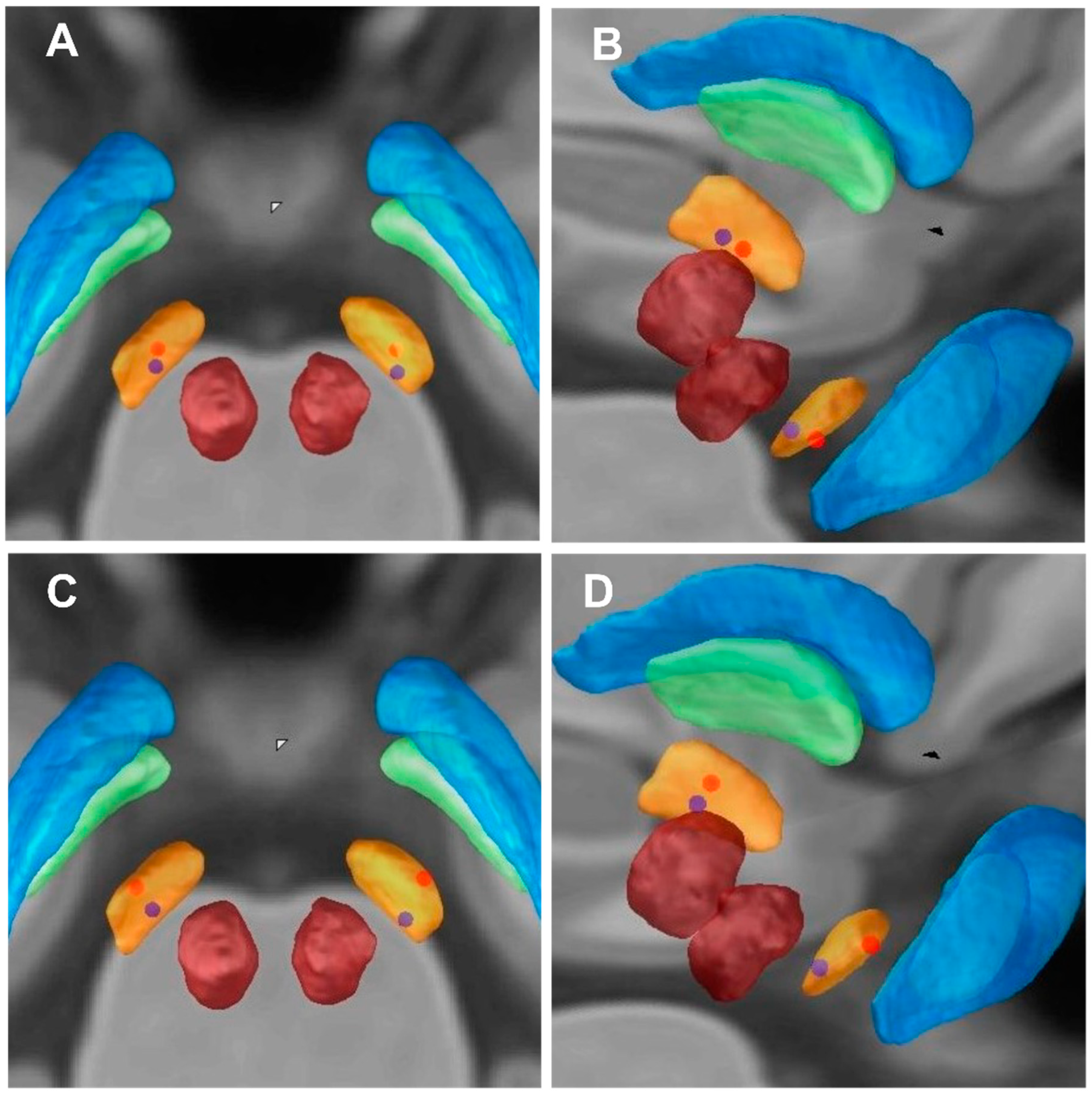
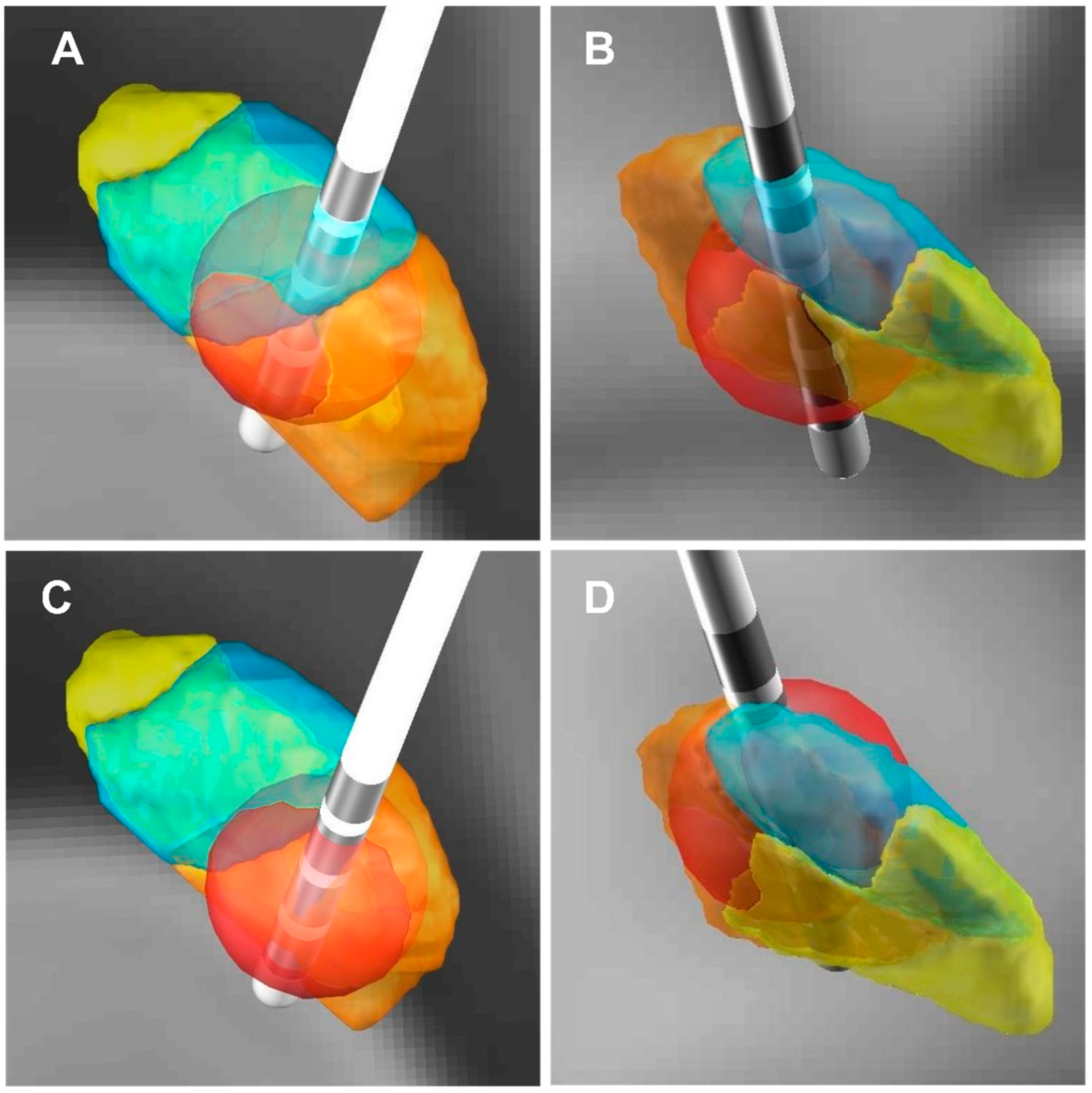
2.5. The Coordinates of the Contacts and VTA
2.6. Statistical Analyses
3. Results
3.1. Patient General Outcomes
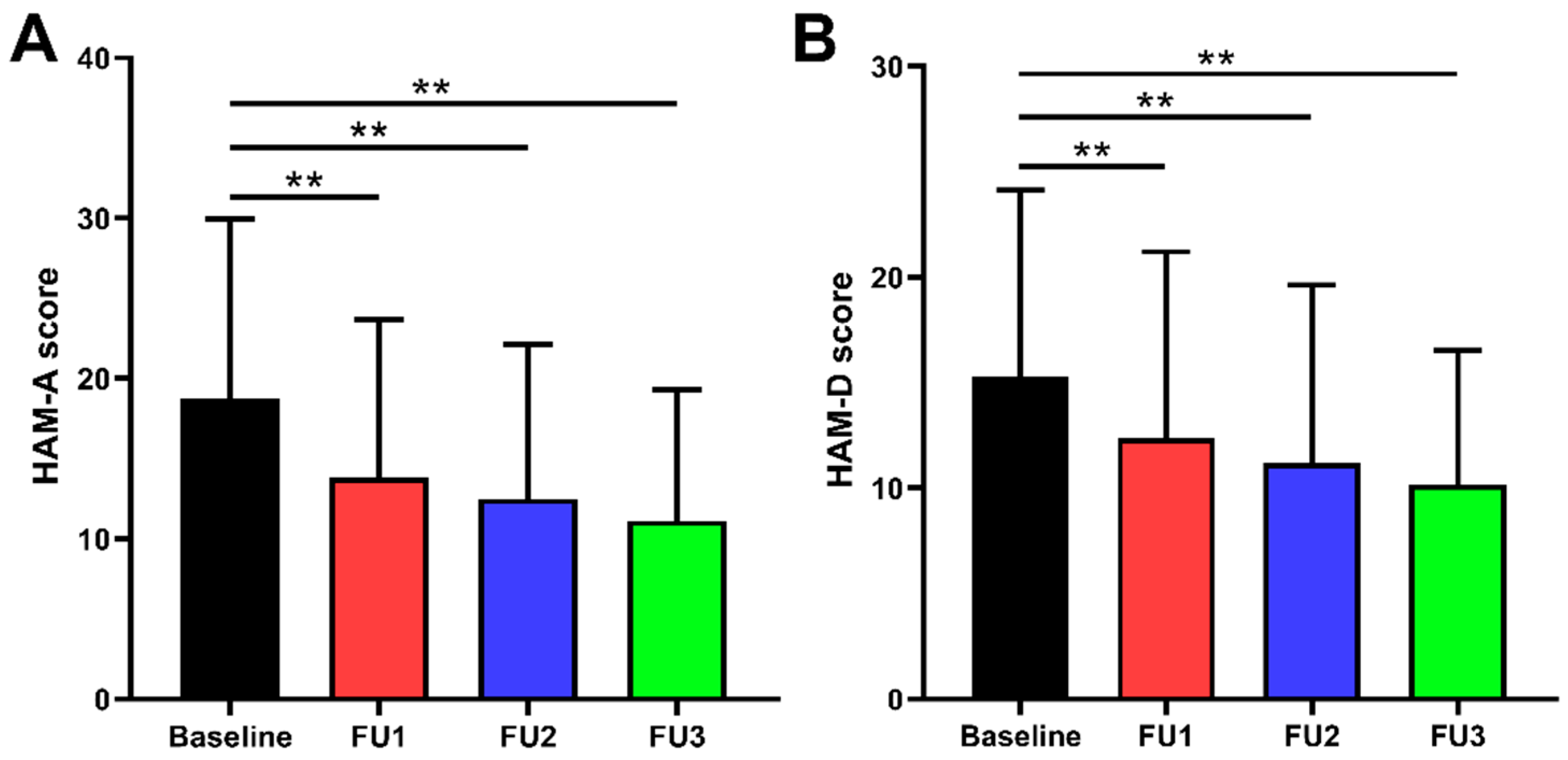
3.2. Clinical Outcomes
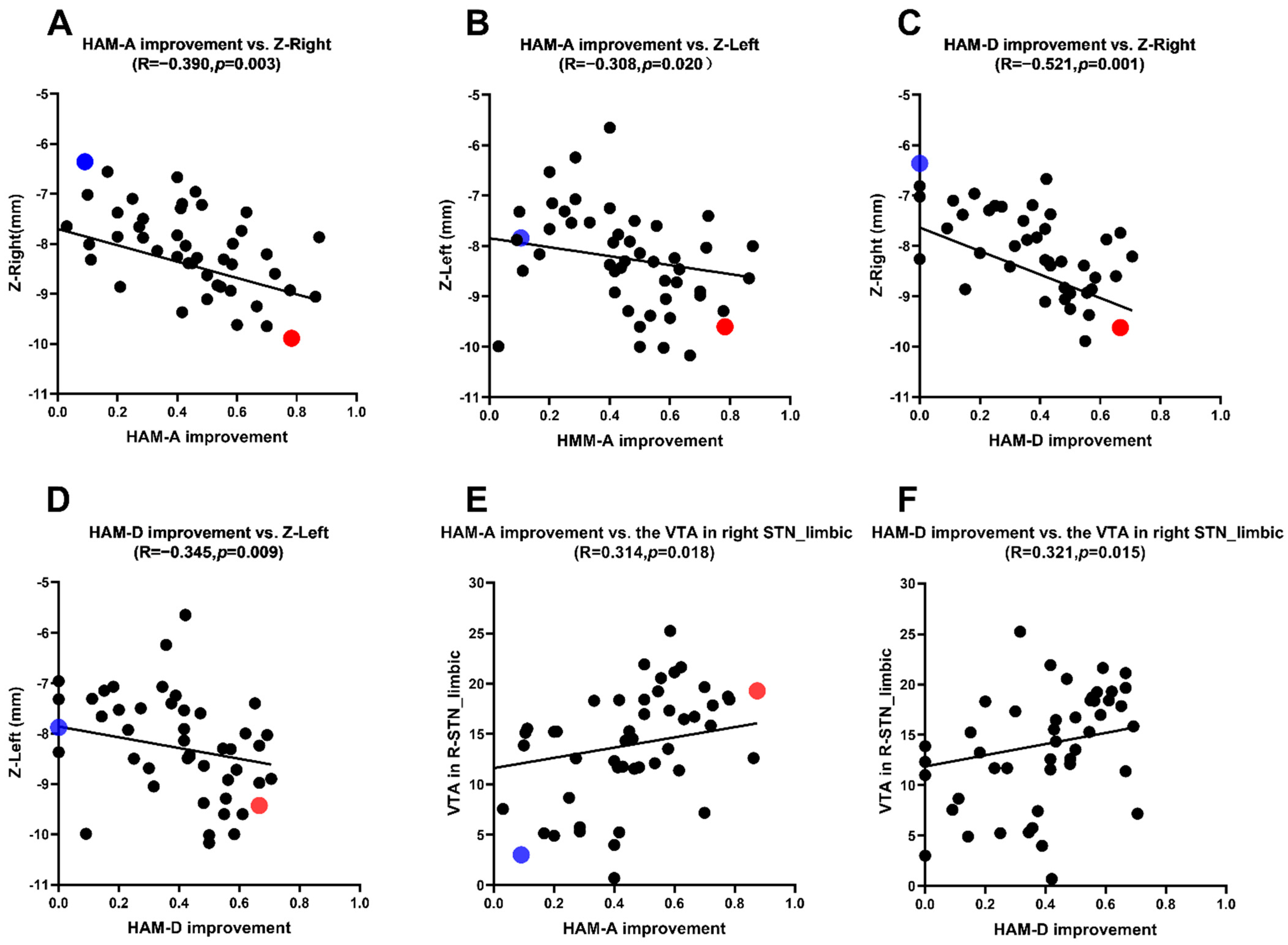
3.3. Correlation Analysis between the HAM-A, HAM-D Scores Improvement Rate and the Location of Active Contacts
3.4. Correlation Analysis between the HAM-A, HAM-D Scores Improvement Rate and the VTAs
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lu, J.; Feng, Z.; Shi, X.; Jiang, L.; Hao, Y. Correlation between programmed stimulation parameters and their efficacy after deep brain electrode implantation for Parkinson’s disease. J. Neurorestoratol. 2020, 8, 53–59. [Google Scholar] [CrossRef] [Green Version]
- Wichmann, T.; DeLong, M.R. Deep brain stimulation for movement disorders of basal Ganglia origin: Restoring function or functionality? Neurotherapeutics 2016, 13, 264–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Birchall, E.L.; Walker, H.C.; Cutter, G.; Guthrie, S.; Joop, A.; Memon, R.A.; Watts, R.L.; Standaert, D.G.; Amara, A.W. The effect of unilateral subthalamic nucleus deep brain stimulation on depression in Parkinson’s disease. Brain Stimul. 2017, 10, 651–656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, F.; Wang, F.; Li, W.; Wang, N.; Han, C.; Fan, S.; Li, P.; Xu, L.; Zhang, J.; Meng, F. Relationship between electrode position of deep brain stimulation and motor symptoms of Parkinson’s disease. BMC Neurol. 2021, 17, 122. [Google Scholar] [CrossRef] [PubMed]
- Berg, D.; Lang, A.E.; Postuma, R.B.; Maetzler, W.; Deuschl, G.; Gasser, T.; Siderowf, A.; Schapira, A.H.; Oertel, W.; Obeso, J.A.; et al. Changing the research criteria for the diagnosis of Parkinson’s disease: Obstacles and opportunities. Lancet Neurol. 2013, 12, 514–524. [Google Scholar] [CrossRef]
- Zach, H.; Walter, U.; Liepelt-Scarfone, I.; Maetzler, W. Diagnostics of clinical and prodromal idiopathic Parkinson’s disease: New criteria. Nervenarzt 2017, 88, 356–364. [Google Scholar] [CrossRef] [PubMed]
- Horn, A.; Reich, M.; Vorwerk, J.; Li, N.; Wenzel, G.; Fang, Q.; Schmitz-Hübsch, T.; Nickl, R.; Kupsch, A.; Volkmann, J.; et al. Connectivity Predicts deep brain stimulation outcome in Parkinson disease. Ann. Neurol. 2017, 82, 67–78. [Google Scholar] [CrossRef]
- Chen, Y.; Hao, H.; Chen, H.; Li, L. The study on a telemedicine interaction mode for Deep Brain Stimulation postoperative follow-up. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2015, 2015, 186–189. [Google Scholar] [CrossRef]
- Husch, A.; Petersen, M.V.; Gemmar, P.; Goncalves, J.; Hertel, F. PaCER—A fully automated method for electrode trajectory and contact reconstruction in deep brain stimulation. Neuroimage Clin. 2018, 17, 80–89. [Google Scholar] [CrossRef]
- Ewert, S.; Plettig, P.; Li, N.; Chakravarty, M.M.; Collins, D.L.; Herrington, T.M.; Kühn, A.A.; Horn, A. Toward defining deep brain stimulation targets in MNI space: A subcortical atlas based on multimodal MRI, histology and structural connectivity. Neuroimage 2018, 170, 271–282. [Google Scholar] [CrossRef]
- Pauli, W.M.; Nili, A.N.; Tyszka, J.M. A high-resolution probabilistic in vivo atlas of human subcortical brain nuclei. Sci. Data 2018, 17, 180063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dulski, J.; Schinwelski, M.; Konkel, A.; Grabowski, K.; Libionka, W.; Wąż, P.; Sitek, E.J.; Sławek, J. The impact of subthalamic deep brain stimulation on sleep and other non-motor symptoms in Parkinson’s disease. Parkinsonism Relat. Disord. 2019, 64, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Jaafari, N.; Giré, P.; Houeto, J.L. Deep brain stimulation, Parkinson’s disease and neuropsychiatric complications. Presse Med. 2009, 38, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- Castelli, L.; Perozzo, P.; Zibetti, M.; Crivelli, B.; Morabito, U.; Lanotte, M.; Cossa, F.; Bergamasco, B.; Lopiano, L. Chronic deep brain stimulation of the subthalamic nucleus for Parkinson’s disease: Effects on cognition, mood, anxiety and personality traits. Eur. Neurol. 2006, 55, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Bronstein, J.M.; Tagliati, M.; Alterman, R.L.; Lozano, A.M.; Volkmann, J.; Stefani, A.; Horak, F.B.; Okun, M.S.; Foote, K.D.; Krack, P.; et al. Deep brain stimulation for Parkinson disease: An expert consensus and review of key issues. Arch. Neurol. 2011, 68, 165. [Google Scholar] [CrossRef]
- Follett, K.A.; Weaver, F.M.; Stern, M.; Hur, K.; Harris, C.L.; Luo, P.; Marks, W.J., Jr.; Rothlind, J.; Sagher, O.; Moy, C.; et al. Pallidal versus subthalamic deep-brain stimulation for Parkinson’s disease. N. Engl. J. Med. 2010, 362, 2077–2091. [Google Scholar] [CrossRef] [Green Version]
- McDonald, L.M.; Page, D.; Wilkinson, L.; Jahanshahi, M. Deep brain stimulation of the subthalamic nucleus improves sense of well-being in Parkinson’s disease. Mov. Disord. 2012, 27, 372–378. [Google Scholar] [CrossRef]
- Blomstedt, P.; Hariz, M.I.; Lees, A.; Silberstein, P.; Limousin, P.; Yelnik, J.; Agid, Y. Acute severe depression induced by intraoperative stimulation of the substantia nigra: A case report. Parkinsonism Relat. Disord. 2008, 14, 253–256. [Google Scholar] [CrossRef]
- Etiévant, A.; Lucas, G.; Dkhissi-Benyahya, O.; Haddjeri, N. The Role of Astroglia in the Antidepressant Action of Deep Brain Stimulation. Front. Cell. Neurosci. 2016, 12, 509. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Chang, C.; Geng, N.; Li, N.; Wang, J.; Ma, J.; Xue, W.; Zhao, W.; Wu, H.; Wang, P.; et al. Long-term effects of bilateral deep brain stimulation of the subthalamic nucleus on depression in patients with Parkinson’s disease. Parkinsonism Relat. Disord. 2009, 15, 587–591. [Google Scholar] [CrossRef]
- Frank, M.J.; Samanta, J.; Moustafa, A.A.; Sherman, S.J. Hold your horses: Impulsivity, deep brain stimulation and medication in Parkinsonism. Science 2007, 318, 1309–1312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krack, P.; Hariz, M.I.; Baunez, C.; Guridi, J.; Obeso, J.A. Deep brain stimulation: From neurology to psychiatry? Trends Neuro. Sci. 2010, 33, 474–484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- York, M.K.; Wilde, E.A.; Simpson, R.A. Relationship between neuropsychological outcome and DBS surgical trajectory and electrode location. J. Neuro. Sci. 2009, 287, 159–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunenberg, E.J.; Moeskops, P.; Backes, W.H.; Pollo, C.; Cammoun, L.; Vilanova, A.; Janssen, M.L.; Visser-Vandewalle, V.E.; ter Haar Romeny, B.M.; Thiran, J.P.; et al. Structural and resting state functional connectivity of the subthalamic nucleus: Identification of motor STN parts and the hyperdirect pathway. PLoS ONE 2012, 7, e39061. [Google Scholar] [CrossRef] [PubMed]
- Dafsari, H.S.; Petry-Schmelzer, J.N.; Ray-Chaudhuri, K.; Ashkan, K.; Weis, L.; Dembek, T.A.; Samuel, M.; Rizos, A.; Silverdale, M.; Barbe, M.T.; et al. Non-motor outcomes of subthalamic stimulation in Parkinson’s disease depend on location of active contacts. Brain Stimil. 2018, 11, 904–912. [Google Scholar] [CrossRef] [Green Version]
- Gourisankar, A.; Eisenstein, S.A.; Trapp, N.T.; Koller, J.M.; Campbell, M.C.; Ushe, M.; Perlmutter, J.S.; Hershey, T.; Black, K.J. Mapping movement, mood, motivation and mentation in the subthalamic nucleus. R. Soc. Open Sci. 2018, 18, 171177. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Preoperative | Postoperative | Total p | χ2 | p1 | p2 | p3 | |||
|---|---|---|---|---|---|---|---|---|---|
| 1 Month | 3 Months | 6 Months | |||||||
| HAM-A (0–56) | 16 (14) | 11 (11) | 9 (10) | 11 (11) | <0.001 | 60.464 | <0.001 | <0.001 | <0.001 |
| HAM-D (0–68) | 14 (13) | 9 (9) | 9 (8) | 9 (9) | <0.001 | 45.592 | <0.001 | <0.001 | <0.001 |
| HAM-A Improvement Rate | HAM-D Improvement Rate | |||
|---|---|---|---|---|
| r | p | r | p | |
| right | ||||
| X | 0.017 | 0.899 | −0.063 | 0.642 |
| Y | 0.003 | 0.985 | 0.032 | 0.811 |
| Z | −0.390 | 0.003 | −0.521 | 0.001 |
| left | ||||
| X | 0.237 | 0.076 | 0.210 | 0.117 |
| Y | 0.027 | 0.842 | −0.078 | 0.566 |
| Z | −0.308 | 0.020 | −0.345 | 0.009 |
| HAM-A Improvement | HAM-D Improvement | |||
|---|---|---|---|---|
| r | p | r | p | |
| right STN | ||||
| motor subregion | −0.027 | 0.839 | −0.085 | 0.531 |
| associative subregion | −0.176 | 0.190 | −0.189 | 0.159 |
| limbic subregion | 0.314 | 0.018 | 0.321 | 0.015 |
| left STN | ||||
| motor subregion | −0.078 | 0.566 | 0.163 | 0.226 |
| associative subregion | 0.086 | 0.524 | 0.042 | 0.755 |
| limbic subregion | 0.174 | 0.196 | 0.154 | 0.254 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, F.; Wang, F.; Xing, Y.-J.; Yang, M.-M.; Wang, J.-W.; Li, C.-H.; Han, C.-L.; Fan, S.-Y.; Gao, D.-M.; Yang, C.; et al. Correlation between Electrode Location and Anxiety Depression of Subthalamic Nucleus Deep Brain Stimulation in Parkinson’s Disease. Brain Sci. 2022, 12, 755. https://doi.org/10.3390/brainsci12060755
Zhang F, Wang F, Xing Y-J, Yang M-M, Wang J-W, Li C-H, Han C-L, Fan S-Y, Gao D-M, Yang C, et al. Correlation between Electrode Location and Anxiety Depression of Subthalamic Nucleus Deep Brain Stimulation in Parkinson’s Disease. Brain Sciences. 2022; 12(6):755. https://doi.org/10.3390/brainsci12060755
Chicago/Turabian StyleZhang, Feng, Feng Wang, Yu-Jing Xing, Man-Man Yang, Ji-Wei Wang, Cong-Hui Li, Chun-Lei Han, Shi-Ying Fan, Dong-Mei Gao, Chen Yang, and et al. 2022. "Correlation between Electrode Location and Anxiety Depression of Subthalamic Nucleus Deep Brain Stimulation in Parkinson’s Disease" Brain Sciences 12, no. 6: 755. https://doi.org/10.3390/brainsci12060755