Behavioral Symptomatology in the Premenstruum


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Sample
2.3. Study Measures
2.4. Data Analysis
3. Results
3.1. Study Participants
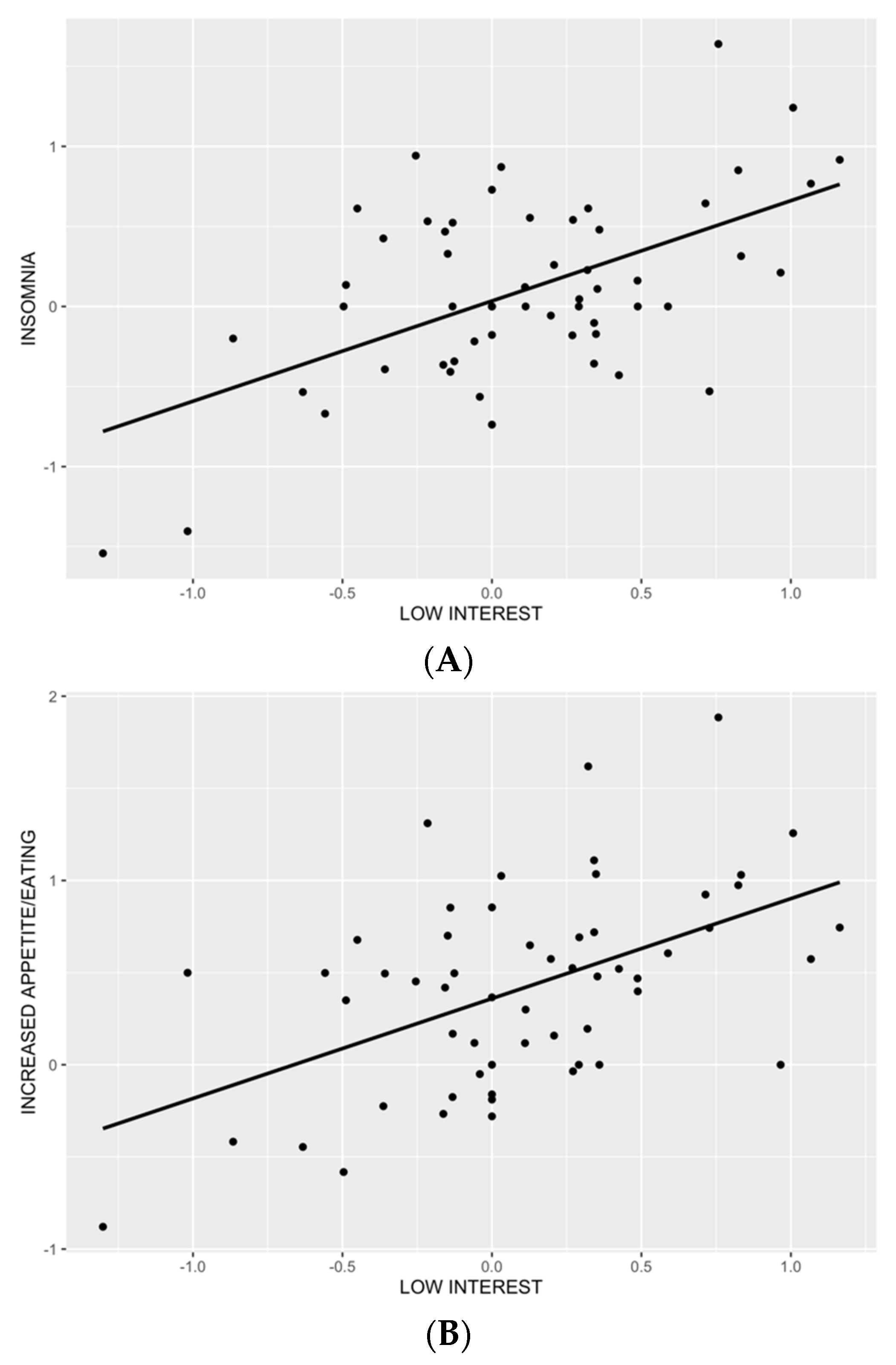
3.2. Relationships between Behavioral, Affective and Psychological Premenstrual Symptoms
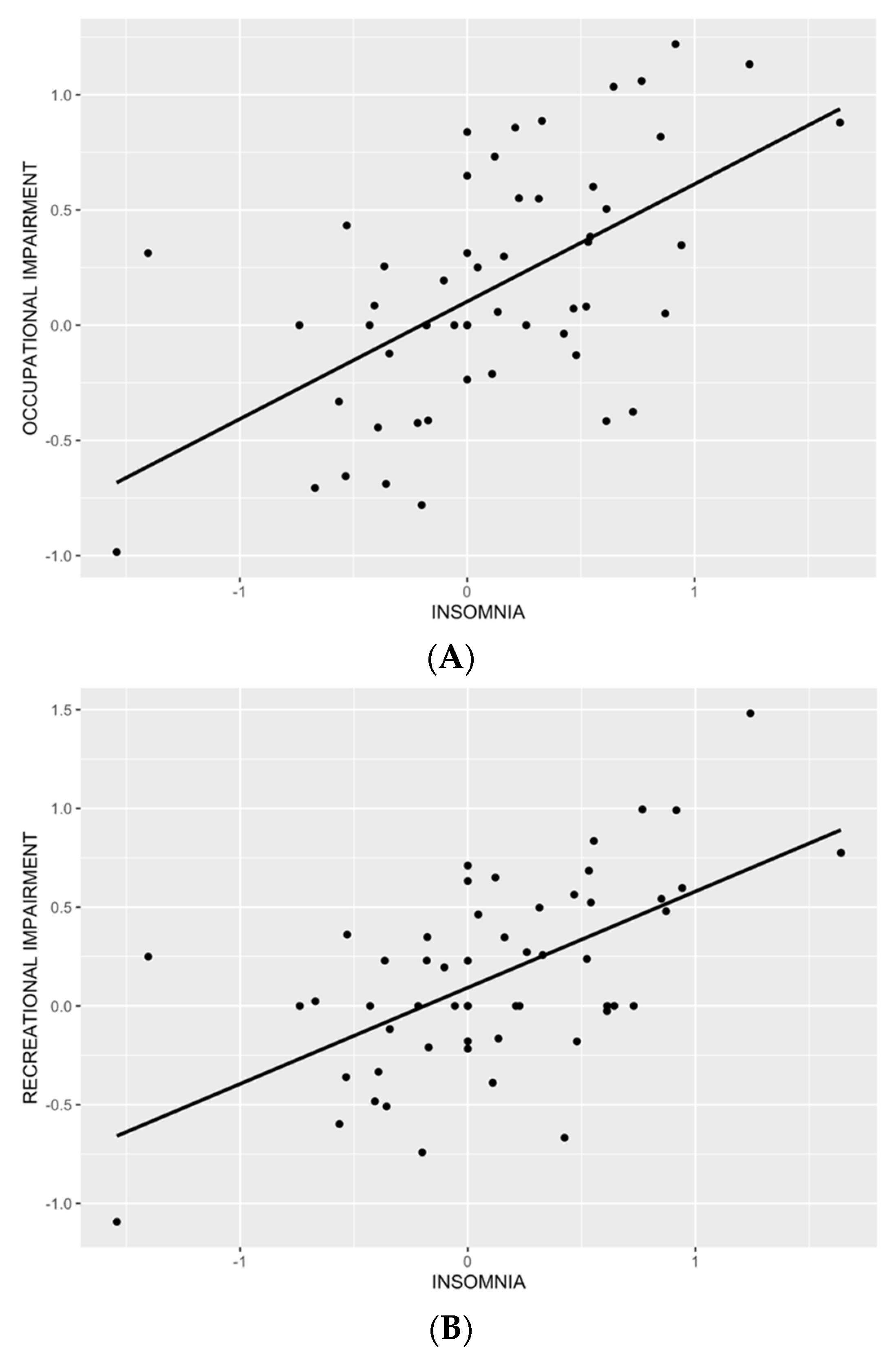
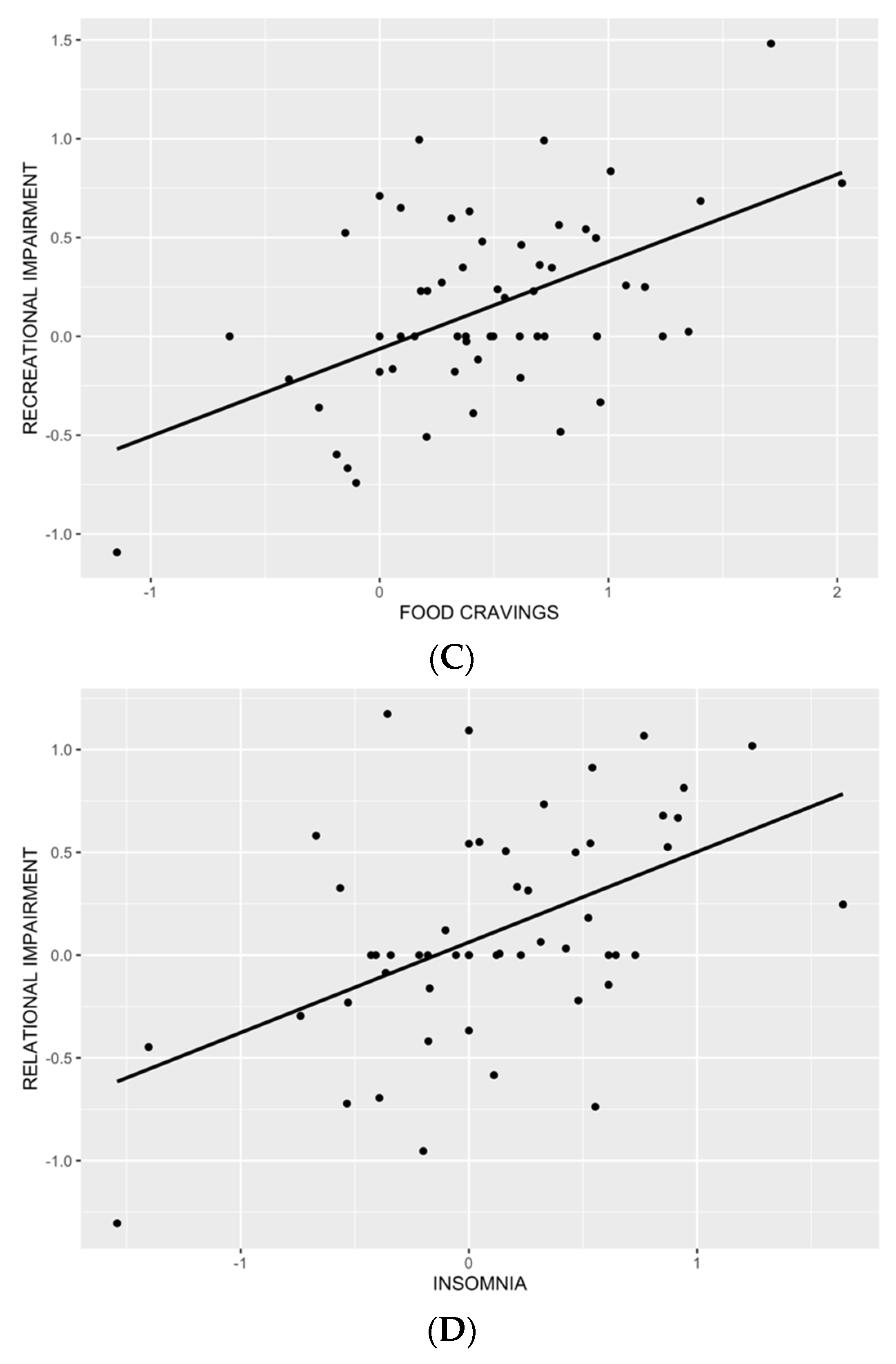
3.3. Relationships between Premenstrual Functionality and Behavioral Symptoms
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ginsburg, K.; Dinsay, R. Premenstrual syndrome. In Practical Strategies in Obstetrics and Gynecology; Ransom, S.B., Ed.; WB Saunders Company: Philadelphia, PA, USA, 2000. [Google Scholar]
- Hill, A.J. Symposium on ‘molecular mechanisms and psychology of food intake’—The psychology of food craving. Proc. Nutr. Soc. 2007, 66, 277–285. [Google Scholar] [CrossRef] [PubMed]
- Weingarten, H.P.; Elston, D. The phenomenology of food cravings. Appetite 1990, 15, 231–246. [Google Scholar] [CrossRef]
- Delahanty, L.M.; Meigs, J.B.; Hayden, D.; Williamson, D.A.; Nathan, D.M.; Group, D.R. Psychological and behavioral correlates of baseline BMI in the diabetes prevention program (DPP). Diabetes Care 2002, 25, 1992–1998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cepeda-Benito, A.; Fernandez, M.C.; Moreno, S. Relationship of gender and eating disorder symptoms to reported cravings for food: Construct validation of state and trait craving questionnaires in Spanish. Appetite 2003, 40, 47–54. [Google Scholar] [CrossRef]
- McVay, M.A.; Copeland, A.L.; Geiselman, P.J. Eating disorder pathology and menstrual cycle fluctuations in eating variables in oral contraceptive users and non-users. Eat. Behav. 2011, 12, 49–55. [Google Scholar] [CrossRef]
- Rozin, P.; Levine, E.; Stoess, C. Chocolate craving and liking. Appetite 1991, 17, 199–212. [Google Scholar] [CrossRef]
- Hartlage, S.A.; Freels, S.; Gotman, N.; Yonkers, K. Criteria for Premenstrual Dysphoric Disorder Secondary Analyses of Relevant Data Sets. Arch. Gen. Psychiatry 2012, 69, 300–305. [Google Scholar] [CrossRef] [Green Version]
- Hill, A.J.; Heatonbrown, L. The experience of food craving—A prospective investigation in healthy women. J. Psychosom. Res. 1994, 38, 801–814. [Google Scholar] [CrossRef]
- Zellner, D.A.; Garriga-Trillo, A.; Centeno, S.; Wadsworth, E. Chocolate craving and the menstrual cycle. Appetite 2004, 42, 119–121. [Google Scholar] [CrossRef]
- Alonso-Alonso, M.; Ziemke, F.; Magkos, F.; Barrios, F.A.; Brinkoetter, M.; Boyd, I.; Rifkin-Graboi, A.; Yannakoulia, M.; Rojas, R.; Pascual-Leone, A.; et al. Brain responses to food images during the early and late follicular phase of the menstrual cycle in healthy young women: Relation to fasting and feeding. Am. J. Clin. Nutr. 2011, 94, 377–384. [Google Scholar] [CrossRef]
- Arnoni-Bauer, Y.; Bick, A.; Raz, N.; Imbar, T.; Amos, S.; Agmon, O.; Marko, L.; Levin, N.; Weiss, R. Is It Me or My Hormones? Neuroendocrine Activation Profiles to Visual Food Stimuli Across the Menstrual Cycle. J. Clin. Endocrinol. Metab. 2017, 102, 3406–3414. [Google Scholar] [CrossRef] [PubMed]
- Frank, T.C.; Kim, G.L.; Krzemien, A.; Van Vugt, D.A. Effect of menstrual cycle phase on corticolimbic brain activation by visual food cues. Brain Res. 2010, 1363, 81–92. [Google Scholar] [CrossRef] [PubMed]
- Van Vugt, D.A. Brain imaging studies of appetite in the context of obesity and the menstrual cycle. Hum. Reprod. Update 2010, 16, 276–292. [Google Scholar] [CrossRef] [PubMed]
- Strine, T.W.; Chapman, D.P.; Ahluwalia, I.B. Menstrual-related problems and psychological distress among women in the United States. J. Women’s Health 2005, 14, 316–323. [Google Scholar] [CrossRef]
- Mauri, M.; Reid, R.; MacLean, A. Sleep in the premenstrual phase: A self-report study of PMS patients and normal controls. Acta Psychiatr. Scand. 1988, 78, 82–86. [Google Scholar] [CrossRef]
- Rivera-Tovar, A.D.; Frank, E. Late luteal phase dysphoric disorder in young women. Am. J. Psychiatry 1990, 147, 1634–1636. [Google Scholar] [CrossRef]
- Cappuccio, F.P.; Miller, M.A. Sleep and Cardio-Metabolic Disease. Curr. Cardiol. Rep. 2017, 19, 110. [Google Scholar] [CrossRef] [Green Version]
- Engel, S.G.; Wonderlich, S.A.; Crosby, R.D.; Mitchell, J.E.; Crow, S.; Peterson, C.B.; Le Grange, D.; Simonich, H.K.; Cao, L.; Lavender, J.M.; et al. The role of affect in the maintenance of anorexia nervosa: Evidence from a naturalistic assessment of momentary behaviors and emotion. J. Abnorm. Psychol. 2013, 122, 709–719. [Google Scholar] [CrossRef] [Green Version]
- Berg, K.C.; Crosby, R.D.; Cao, L.; Peterson, C.B.; Engel, S.G.; Mitchell, J.E.; Wonderlich, S.A. Facets of negative affect prior to and following binge-only, purge-only, and binge/purge events in women with bulimia nervosa. J. Abnorm. Psychol. 2013, 122, 111–118. [Google Scholar] [CrossRef] [Green Version]
- Fischer, S.; Wonderlich, J.; Breithaupt, L.; Byrne, C.; Engel, S. Negative urgency and expectancies increase vulnerability to binge eating in bulimia nervosa. Eat. Disord. 2018, 26, 39–51. [Google Scholar] [CrossRef]
- Smyth, J.M.; Wonderlich, S.A.; Heron, K.E.; Sliwinski, M.J.; Crosby, R.D.; Mitchell, J.E.; Engel, S.G. Daily and momentary mood and stress are associated with binge eating and vomiting in bulimia nervosa patients in the natural environment. J. Consult. Clin. Psychol. 2007, 75, 629–638. [Google Scholar] [CrossRef] [Green Version]
- Schaefer, L.M.; Smith, K.E.; Anderson, L.M.; Cao, L.; Crosby, R.D.; Engel, S.G.; Crow, S.J.; Peterson, C.B.; Wonderlich, S.A. The role of affect in the maintenance of binge-eating disorder: Evidence from an ecological momentary assessment study. J. Abnorm. Psychol. 2020, 129, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Valenza, C.; Valenza, G.; Muñoz-Casaubon, T.; Botella-López, M.; Puentedura, E.J.; Arroyo-Morales, M.; Fernández-de-las-Peñas, C. Epidemiology of sleep-related complaints associated with obstructive sleep apnea, insomnia and non-restorative sleep in an at-risk population in Granada, Spain Marie. Sleep Biol. Rhythm. 2012, 10, 222–230. [Google Scholar] [CrossRef]
- Alhola, P.; Polo-Kantola, P. Sleep deprivation: Impact on cognitive performance. Neuropsychiatr. Dis. Treat. 2007, 3, 553–567. [Google Scholar] [PubMed]
- Endicott, J.; Nee, J.; Harrison, W. Daily Record of Severity of Problems (DRSP): Reliability and validity. Arch. Women’s Ment. Health 2006, 9, 41–49. [Google Scholar] [CrossRef]
- Hamidovic, A.; Dang, N.; Khalil, D.; Sun, J. Association between Neuroticism and Premenstrual Affective/Psychological Symptomatology. Psychiatry Int. 2022, 3, 52–64. [Google Scholar] [CrossRef]
- Sohda, S.; Suzuki, K.; Igari, I. Relationship Between the Menstrual Cycle and Timing of Ovulation Revealed by New Protocols: Analysis of Data from a Self-Tracking Health App. J. Med. Internet Res. 2017, 19, e391. [Google Scholar] [CrossRef] [Green Version]
- Wei, S.-M.; Baller, E.B.; Martinez, P.E.; Goff, A.C.; Li, H.J.; Kohn, P.D.; Kippenhan, J.S.; Soldin, S.J.; Rubinow, D.R.; Goldman, D.; et al. Subgenual cingulate resting regional cerebral blood flow in premenstrual dysphoric disorder: Differential regulation by ovarian steroids and preliminary evidence for an association with expression of ESC/E(Z) complex genes. Transl. Psychiatry 2021, 11, 206. [Google Scholar] [CrossRef]
- Li, H.J.; Goff, A.; Rudzinskas, S.A.; Jung, Y.; Dubey, N.; Hoffman, J.; Hipolito, D.; Mazzu, M.; Rubinow, D.R.; Schmidt, P.J.; et al. Altered estradiol-dependent cellular Ca2+ homeostasis and endoplasmic reticulum stress response in Premenstrual Dysphoric Disorder. Mol. Psychiatry 2021, 26, 6963–6974. [Google Scholar] [CrossRef]
- Lu, D.; Aleknaviciute, J.; Bjarnason, R.; Tamimi, R.M.; Valdimarsdóttir, U.A.; Bertone-Johnson, E.R. Pubertal development and risk of premenstrual disorders in young adulthood. Hum. Reprod. 2020, 36, 455–464. [Google Scholar] [CrossRef]
- Freeman, E.W.; Rickels, K.; Schweizer, E.; Ting, T. Relationships between age and symptom severity among women seeking medical treatment for premenstrual symptoms. Psychol. Med. 1995, 25, 309–315. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.R-project.org/ (accessed on 15 April 2022).
- Levy, R.; Dubois, B. Apathy and the functional anatomy of the prefrontal cortex-basal ganglia circuits. Cereb. Cortex 2006, 16, 916. [Google Scholar] [CrossRef] [Green Version]
- Robert, P.; Lanctôt, K.L.; Agüera-Ortiz, L.; Aalten, P.; Bremond, F.; Defrancesco, M.; Hanon, C.; David, R.; Dubois, B.; Dujardin, K.; et al. Is it time to revise the diagnostic criteria for apathy in brain disorders? Te 2018 international consensus group. Eur. Psychiatr. 2018, 54, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Cosin, C.; Sibon, I.; Poli, M.; Allard, M.; Debruxelles, S.; Renou, P.; Rouanet, F.; Mayo, W. Circadian sleep/wake rhythm abnormalities as a risk factor of a poststroke apathy. Int. J. Stroke 2015, 10, 710–715. [Google Scholar] [CrossRef] [PubMed]
- Mulin, E.; Zeitzer, J.M.; Friedman, L.; Le Duff, F.; Yesavage, J.; Robert, P.H.; David, R. Relationship between apathy and sleep disturbance in mild and moderate Alzheimer’s disease: An actigraphic study. J. Alzheimers Dis. 2011, 25, 85–91. [Google Scholar] [CrossRef] [Green Version]
- Bargiotas, P.; Ntafouli, M.; Lachenmayer, M.L.; Krack, P.; Schüpbach, W.M.M.; Bassetti, C.L.A. Apathy in Parkinson’s disease with REM sleep behavior disorder. J. Neurol. Sci. 2019, 399, 194–198. [Google Scholar] [CrossRef]
- Barber, T.R.; Muhammed, K.; Drew, D.; Lawton, M.; Crabbe, M.; Rolinski, M.; Quinnell, T.; Zaiwalla, Z.; Ben-Shlomo, Y.; Husain, M.; et al. Apathy in rapid eye movement sleep behaviour disorder is common and under-recognized. Eur. J. Neurol. 2018, 25, 469-e32. [Google Scholar] [CrossRef] [Green Version]
- Desouza, C.V.; Padala, P.R.; Haynatzki, G.; Anzures, P.; Demasi, C.; Shivaswamy, V. Role of apathy in the effectiveness of weight management programmes. Diabetes Obes. Metab. 2012, 14, 419–423. [Google Scholar] [CrossRef]
- Baker, F.C.; De Zambotti, M.; Colrain, I.M.; Bei, B. Sleep problems during the menopausal transition: Prevalence, impact, and management challenges. Nat. Sci. Sleep 2018, 10, 73. [Google Scholar] [CrossRef] [Green Version]
- Sharkey, K.M.; Crawford, S.L.; Kim, S.; Joffe, H. Objective sleep interruption and reproductive hormone dynamics in the menstrual cycle. Sleep Med. 2014, 15, 688–693. [Google Scholar] [CrossRef] [Green Version]
- Israel, S.L.; Schneller, O. The thermogenic property of progesterone. Obstet. Gynecol. Surv. 1950, 5, 532–533. [Google Scholar] [CrossRef]
- Van Someren, E.J. More than a marker: Interaction between the circadian regulation of temperature and sleep, age-related changes, and treatment possibilities. Chronobiol. Int. 2000, 17, 313–354. [Google Scholar] [CrossRef] [PubMed]
- Sateia, M.J.; Buysse, D.J.; Krystal, A.D.; Neubauer, D.N.; Heald, J.L. Clinical Practice Guideline for the Pharmacologic Treatment of Chronic Insomnia in Adults: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med. 2017, 13, 307–349. [Google Scholar] [CrossRef]
- Michelson, D.; Snyder, E.; Paradis, E.; Chengan-Liu, M.; Snavely, D.B.; Hutzelmann, J.; Walsh, J.K.; Krystal, A.D.; Benca, R.M.; Cohn, M. Safety and efficacy of suvorexant during 1-year treatment of insomnia with subsequent abrupt treatment discontinuation: A phase 3 randomised, double-blind, placebo-controlled trial. Lancet Neurol. 2014, 13, 461–471. [Google Scholar] [CrossRef]
- Khan, M.S.; Aouad, R. The effects of insomnia and sleep loss on cardiovascular disease. Sleep Med. Clin. 2017, 12, 167–177. [Google Scholar] [CrossRef] [PubMed]
- Nagata, J.M.; Garber, A.K.; Tabler, J.; Murray, S.B.; Vittinghoff, E.; Bibbins-Domingo, K. Disordered eating behaviors and cardiometabolic risk among young adults with overweight or obesity. Int. J. Eat. Disord. 2018, 51, 931–941. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | Mean (SD) | Percent |
|---|---|---|
| Age | 25.98 (4.69) | |
| Race | ||
| White | 33.33 | |
| Black or African American | 15.78 | |
| American Indian/Alaska Native | 1.75 | |
| Asian | 36.84 | |
| Native Hawaiian or Other Pacific Islander | 0 | |
| More than one race | 5.26 | |
| Unknown/do not want to specify | 7.01 | |
| Ethnicity | ||
| Hispanic | 15.78 | |
| Non-Hispanic | 80.70 | |
| Do not know/Do not want to specify | 3.50 | |
| Student Status | ||
| Yes | 47.36 | |
| No | 52.63 | |
| Marital Status | ||
| Single, never married | 91.22 | |
| Married | 8.77 | |
| Age of Menarche | 12.05 (1.07) | |
| BMI | 24.48 (4.37) | |
| Waist Circumference (cm) | 79.63 (4.37) |
| Symptom | Estimate | Standard Error | T Value | p-Value | Model Characteristics |
|---|---|---|---|---|---|
| Insomnia | |||||
| Depressed mood | −0.071033 | 0.202361 | −0.351 | 0.7271 | Residual standard error: 0.5061 on 49 degrees of freedom; Multiple R-squared: 0.327; Adjusted R-squared: 0.2309; F-statistic: 3.401 on 7 and 49 DF, p-value: 0.004865 |
| Anxiety | 0.006171 | 0.153829 | 0.04 | 0.9682 | |
| Mood swings | −0.068889 | 0.19377 | −0.356 | 0.7237 | |
| Anger | 0.096548 | 0.173253 | 0.557 | 0.5799 | |
| Low interest | 0.486635 | 0.210894 | 2.307 | 0.0253 * | |
| Difficulty concentrating | 0.182399 | 0.189285 | 0.964 | 0.34 | |
| Felt overwhelmed | 0.040668 | 0.168132 | 0.242 | 0.8099 | |
| Hypersomnia | |||||
| Depressed mood | 0.19182 | 0.188628 | 1.017 | 0.314 | Residual standard error: 0.4717 on 49 degrees of freedom; Multiple R-squared: 0.2437; Adjusted R-squared: 0.1356; F-statistic: 2.255 on 7 and 49 DF; p-value: 0.04517 |
| Anxiety | 0.09615 | 0.14339 | 0.671 | 0.506 | |
| Mood swings | 0.073938 | 0.18062 | 0.409 | 0.684 | |
| Anger | −0.077098 | 0.161495 | −0.477 | 0.635 | |
| Low interest | 0.103627 | 0.196582 | 0.527 | 0.6 | |
| Difficulty concentrating | 0.198554 | 0.176439 | 1.125 | 0.266 | |
| Felt overwhelmed | 0.008952 | 0.156722 | 0.057 | 0.955 | |
| Increased appetite/eating | |||||
| Depressed mood | −0.2243 | 0.19172 | −1.17 | 0.2477 | Residual standard error: 0.4794 on 49 degrees of freedom; Multiple R-squared: 0.3138; Adjusted R-squared: 0.2157; F-statistic: 3.201 on 7 and 49 DF; p-value: 0.007163 |
| Anxiety | 0.07801 | 0.14574 | 0.535 | 0.5949 | |
| Mood swings | 0.09274 | 0.18358 | 0.505 | 0.6157 | |
| Anger | 0.15952 | 0.16414 | 0.972 | 0.3359 | |
| Low interest | 0.4543 | 0.1998 | 2.274 | 0.0274 * | |
| Difficulty concentrating | 0.09768 | 0.17933 | 0.545 | 0.5884 | |
| Felt overwhelmed | −0.08705 | 0.15929 | −0.547 | 0.5872 | |
| Food cravings | |||||
| Depressed mood | −0.095265 | 0.208594 | −0.457 | 0.6499 | Residual standard error: 0.5216 on 49 degrees of freedom; Multiple R-squared: 0.2241; Adjusted R-squared: 0.1133; F-statistic: 2.022 on 7 and 49 DF; p-value: 0.07104 |
| Anxiety | −0.008728 | 0.158568 | −0.055 | 0.9563 | |
| Mood swings | 0.12784 | 0.199739 | 0.64 | 0.5251 | |
| Anger | 0.210877 | 0.17859 | 1.181 | 0.2434 | |
| Low interest | 0.009962 | 0.21739 | 0.046 | 0.9636 | |
| Difficulty concentrating | 0.381662 | 0.195116 | 1.956 | 0.0562 | |
| Felt overwhelmed | −0.194214 | 0.173312 | −1.121 | 0.2679 | |
| Symptom | Estimate | Standard Error | T Value | p-Value | Model Characteristics |
|---|---|---|---|---|---|
| Occupational impairment | |||||
| Insomnia | 0.39341 | 0.11237 | 3.501 | 0.00096 *** | Residual standard error: 0.4158 on 52 degrees of freedom Multiple R-squared: 0.3835, Adjusted R-squared: 0.336 F-statistic: 8.086 on 4 and 52 DF, p-value: 3.794 × 10−5 |
| Hypersomnia | 0.08241 | 0.1282 | 0.643 | 0.52317 | |
| Food cravings | 0.03363 | 0.14688 | 0.229 | 0.8198 | |
| Increased appetite/eating | 0.17491 | 0.16027 | 1.091 | 0.28015 | |
| Recreational impairment | |||||
| Insomnia | 0.35136 | 0.09594 | 3.662 | 0.000586 *** | Residual standard error: 0.355 on 52 degrees of freedom Multiple R-squared: 0.4755, Adjusted R-squared: 0.4351 F-statistic: 11.78 on 4 and 52 DF, p-value: 6.912 × 10−7 |
| Hypersomnia | 0.14466 | 0.10946 | 1.322 | 0.1921 | |
| Food cravings | 0.29946 | 0.1254 | 2.388 | 0.020611 * | |
| Increased appetite/eating | −0.05736 | 0.13684 | −0.419 | 0.676798 | |
| Relational impairment | |||||
| Insomnia | 0.35352 | 0.12213 | 2.895 | 0.00554 ** | Residual standard error: 0.355 on 52 degrees of freedom Multiple R-squared: 0.4755, Adjusted R-squared: 0.4351 F-statistic: 11.78 on 4 and 52 DF, p-value: 6.912 × 10−7 |
| Hypersomnia | 0.08699 | 0.13934 | 0.624 | 0.53518 | |
| Food cravings | −0.08686 | 0.15963 | −0.544 | 0.58868 | |
| Increased appetite/eating | 0.20062 | 0.17419 | 1.152 | 0.25468 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dang, N.; Khalil, D.; Sun, J.; Naveed, A.; Soumare, F.; Nusslock, R.; Hamidovic, A. Behavioral Symptomatology in the Premenstruum. Brain Sci. 2022, 12, 814. https://doi.org/10.3390/brainsci12070814
Dang N, Khalil D, Sun J, Naveed A, Soumare F, Nusslock R, Hamidovic A. Behavioral Symptomatology in the Premenstruum. Brain Sciences. 2022; 12(7):814. https://doi.org/10.3390/brainsci12070814
Chicago/Turabian StyleDang, Nhan, Dina Khalil, Jiehuan Sun, Aamina Naveed, Fatimata Soumare, Robin Nusslock, and Ajna Hamidovic. 2022. "Behavioral Symptomatology in the Premenstruum" Brain Sciences 12, no. 7: 814. https://doi.org/10.3390/brainsci12070814