
Evaluation of the Efficacy of a New Dichoptic Digital Platform to Treat the Anisometropic and Isometropic Amblyopia

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Clinical Protocol
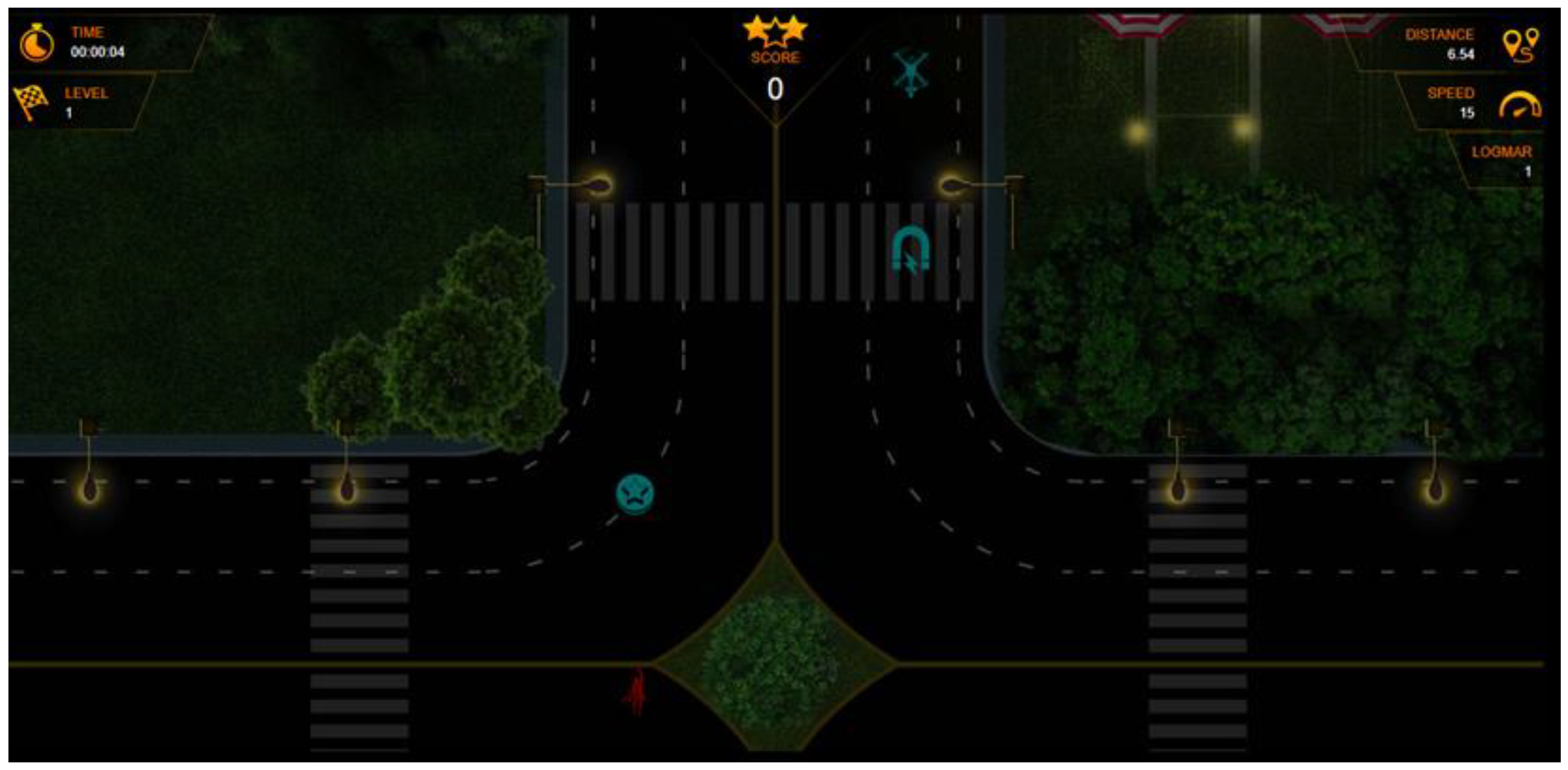
2.3. Visual Training Protocol
2.4. Statistical Analysis
3. Results
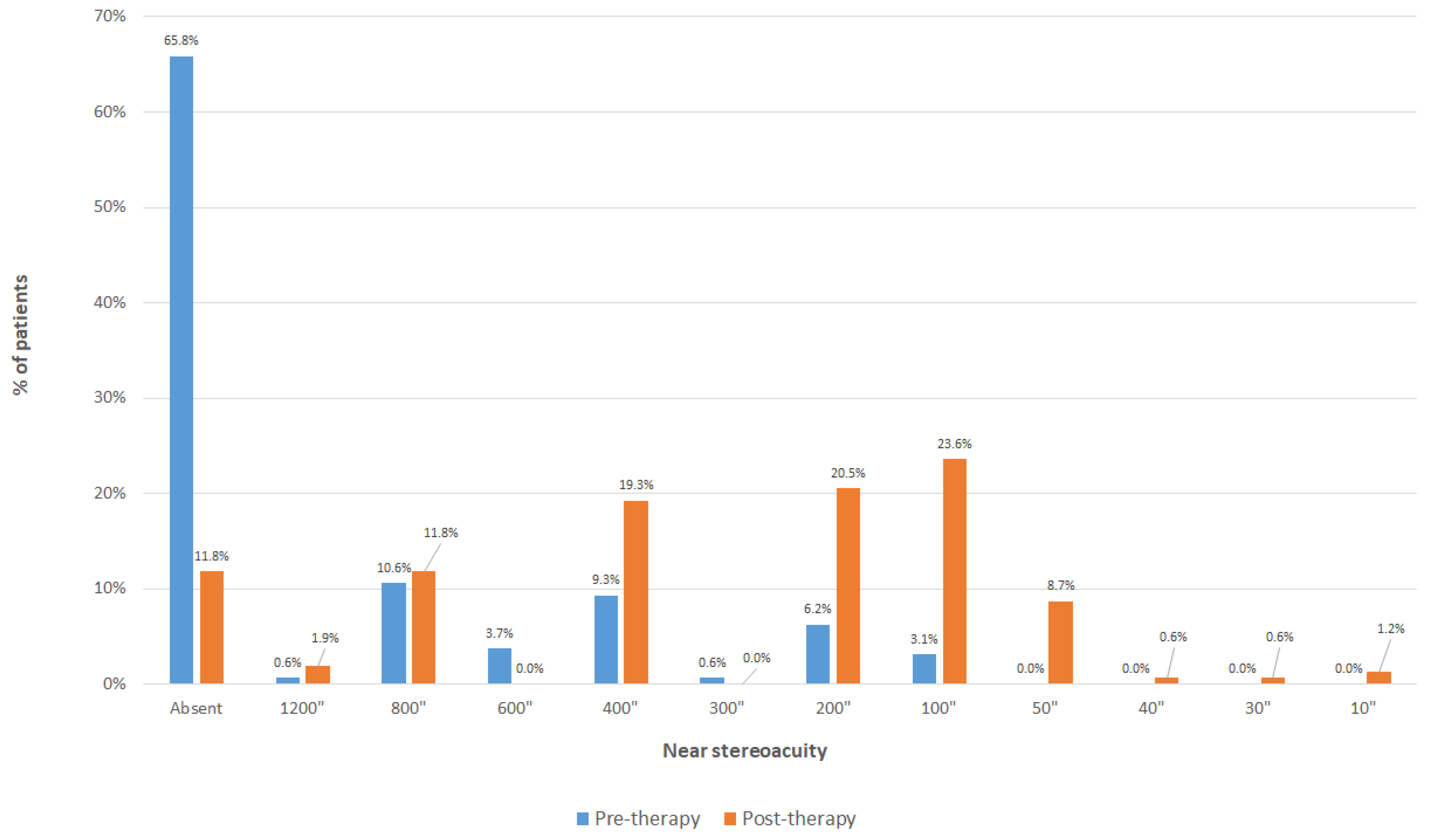
3.1. Analysis of the Whole Sample
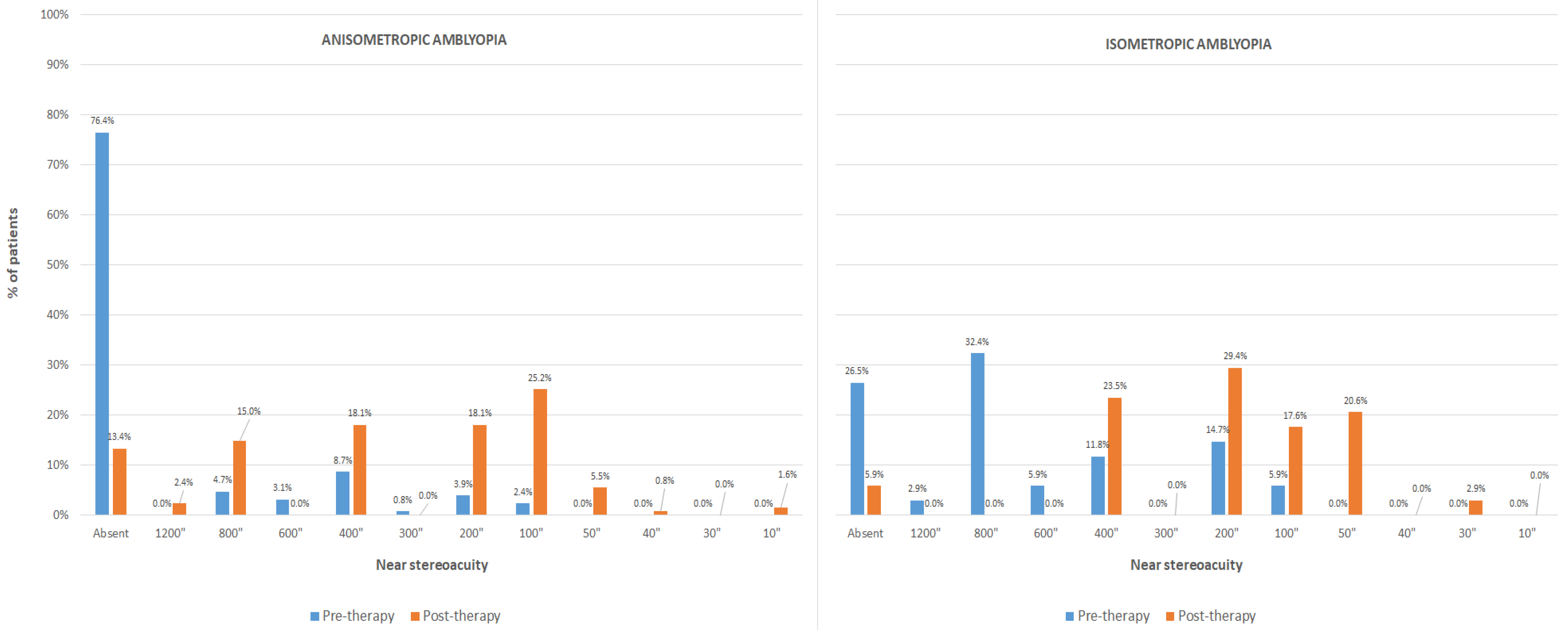
3.2. Analysis of the Anisometropic Amblyopia Group
3.3. Analysis of the Isometropic Amblyopia Group
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kiorpes, L.; Daw, N. Cortical correlates of amblyopia. Vis. Neurosci. 2018, 35, E016. [Google Scholar] [CrossRef] [PubMed]
- Foss, A.J. Use of video games for the treatment of amblyopia. Curr. Opin. Ophthalmol. 2017, 28, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Thompson, B.; Lam, C.S.; Deng, D.; Chan, L.Y.; Maehara, G.; Woo, G.C.; Yu, M.; Hess, R.F. The role of suppression in amblyopia. Invest. Ophthalmol. Vis. Sci. 2011, 52, 4169–4176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boniquet-Sanchez, S.; Sabater-Cruz, N. Current management of amblyopia with new technologies for binocular treatment. Vision 2021, 5, 31. [Google Scholar] [CrossRef]
- Bach, M. Dichoptic training for amblyopia. Ophthalmologe 2016, 113, 304–307. [Google Scholar] [CrossRef]
- Hernández-Rodríguez, C.J.; Piñero, D.P.; Molina-Martín, A.; Morales-Quezada, L.; De Fez, D.; Leal-Vega, L.; Arenillas, J.F.; Coco-Martín, M.B. Stimuli characteristics and psychophysical requirements for visual training in amblyopia: Anarrative review. J. Clin. Med. 2020, 9, 3985. [Google Scholar] [CrossRef]
- Xiao, S.; Angjeli, E.; Wu, H.C.; Gaier, E.D.; Gomez, S.; Travers, D.A.; Binenbaum, G.; Langer, R.; Hunter, D.G.; Repka, M.X.; et al. Randomized controlled trial of a dichoptic digital therapeutic for amblyopia. Ophthalmology 2022, 129, 77–85. [Google Scholar] [CrossRef]
- Manny, R.E.; Holmes, J.M.; Kraker, R.T.; Li, Z.; Waters, A.L.; Kelly, K.R.; Kong, L.; Crouch, E.R.; Lorenzana, I.J.; Alkharashi, M.S.; et al. Pediatric Eye Disease Investigator Group. A randomized trial of binocular Dig Rush game treatment for amblyopia in children aged 4 to 6 years. Optom. Vis. Sci. 2022, 99, 213–227. [Google Scholar]
- Huang, Y.T.; Lin, H.J.; Liao, W.L.; Tsai, Y.Y.; Hsieh, Y.C. Effects of vision therapy on bilateral amblyopia unresponsive to conventional treatment: A retrospective comparative study. Children 2022, 9, 205. [Google Scholar] [CrossRef]
- Jost, R.M.; Hudgins, L.A.; Dao, L.M.; Stager, D.R., Jr.; Luu, B.; Beauchamp, C.L.; Hunter, J.S.; Giridhar, P.; Wang, Y.Z.; Birch, E.E. Randomized clinical trial of streaming dichoptic movies versus patching for treatment of amblyopia in children aged 3 to 7 years. Sci. Rep. 2022, 12, 4157. [Google Scholar] [CrossRef]
- Xiao, S.; Gaier, E.D.; Wu, H.C.; Angjeli, E.; Nuth, P.L.; Bohra, L.I.; Miller, A.M.; Mazow, M.L.; Stout, A.U.; Morse, C.L.; et al. Digital therapeutic improves visual acuity and encourages high adherence in amblyopic children in open-label pilot study. J. AAPOS 2021, 25, e1–e87. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.Y.; Zhang, Y.W.; Gao, F.; Chen, F.; Zhang, J.Y. Dichoptic perceptual training in children with amblyopia with or without patching history. Investig. Ophthalmol. Vis. Sci. 2021, 62, 4. [Google Scholar] [CrossRef] [PubMed]
- Pang, P.C.K.; Lam, C.S.Y.; Hess, R.F.; Thompson, B. Effect of dichoptic video game treatment on mild amblyopia—A pilot study. Acta Ophthalmol. 2021, 99, e423–e432. [Google Scholar] [CrossRef] [PubMed]
- Birch, E.E.; Jost, R.M.; De La Cruz, A.; Kelly, K.R.; Beauchamp, C.L.; Dao, L.; Stager, D., Jr.; Leffler, J.N. Binocular amblyopia treatment with contrast-rebalanced movies. J. AAPOS 2019, 23, e1–e160. [Google Scholar] [CrossRef]
- Mezad-Koursh, D.; Rosenblatt, A.; Newman, H.; Stolovitch, C. Home use of binocular dichoptic video content device for treatment of amblyopia: A pilot study. J. AAPOS 2018, 22, 134–138. [Google Scholar] [CrossRef]
- Gambacorta, C.; Nahum, M.; Vedamurthy, I.; Bayliss, J.; Jordan, J.; Bavelier, D.; Levi, D.M. An action video game for the treatment of amblyopia in children: A feasibility study. Vis. Res. 2018, 148, 1–14. [Google Scholar] [CrossRef]
- Bossi, M.; Tailor, V.K.; Anderson, E.J.; Bex, P.J.; Greenwood, J.A.; Dahlmann-Noor, A.; Dakin, S.C. Binocular therapy for childhood amblyopia improves vision without breaking interocular suppression. Investig. Ophthalmol. Vis. Sci. 2017, 58, 3031–3043. [Google Scholar] [CrossRef] [Green Version]
- Li, S.L.; Reynaud, A.; Hess, R.F.; Wang, Y.Z.; Jost, R.M.; Morale, S.E.; De La Cruz, A.; Dao, L.; Stager, D., Jr.; Birch, E.E. Dichoptic movie viewing treats childhood amblyopia. J. AAPOS 2015, 19, 401–405. [Google Scholar] [CrossRef] [Green Version]
- Birch, E.E.; Li, S.L.; Jost, R.M.; Morale, S.E.; De La Cruz, A.; Stager, D., Jr.; Dao, L.; Stager, D.R., Sr. Binocular iPad treatment for amblyopia in preschool children. J. AAPOS 2015, 19, 6–11. [Google Scholar] [CrossRef] [Green Version]
- Pediatric Eye Disease Investigator Group; Holmes, J.M.; Manny, R.E.; Lazar, E.L.; Birch, E.E.; Kelly, K.R.; Summers, A.I.; Martinson, S.R.; Raghuram, A.; Colburn, J.D.; et al. A randomized trial of binocular dig rush game treatment for amblyopia in children aged 7 to 12 years. Ophthalmology 2019, 126, 456–466. [Google Scholar] [CrossRef]
- Gao, T.Y.; Guo, C.X.; Babu, R.J.; Black, J.M.; Bobier, W.R.; Chakraborty, A.; Dai, S.; Hess, R.F.; Jenkins, M.; Jiang, Y.; et al. Effectiveness of a binocular video game vs placebo video game for improving visual functions in older children, teenagers, and adults with amblyopia: A randomized clinical trial. JAMA Ophthalmol. 2018, 136, 172–181. [Google Scholar] [CrossRef] [PubMed]
- Kadhum, A.; Tan, E.T.C.; Levi, D.M.; Colpa, L.; Fronius, M.; Simonsz, H.J.; Loudon, S.E. Barriers to successful dichoptic treatment for amblyopia in young children. Graefes Arch. Clin. Exp. Ophthalmol. 2021, 259, 3149–3157. [Google Scholar] [CrossRef] [PubMed]
- Shoshany, T.N.; Michalak, S.; Staffa, S.J.; Chinn, R.N.; Bishop, K.; Hunter, D.G. Effect of Primary Occlusion Therapy in Asymmetric, Bilateral Amblyopia. Am. J. Ophthalmol. 2020, 211, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.M.; Kuo, H.K.; Fang, P.C.; Lin, H.F.; Lin, P.W.; Lin, S.A. The effects of CAM vision stimulator for bilateral amblyopia of different etiologies. Chang. Gung Med. J. 2008, 31, 592–598. [Google Scholar]
- Webber, A.L.; Wood, J.M.; Thompson, B.; Birch, E.E. From suppression to stereoacuity: A composite binocular function score for clinical research. Ophthalmic Physiol. Opt. 2019, 39, 53–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halicka, J.; Bittsansky, M.; Sivak, S.; Piñero, D.P.; Ziak, P. Virtual reality visual training in an adult patient with anisometropic amblyopia: Visual and functional magnetic resonance outcomes. Vision 2021, 5, 22. [Google Scholar] [CrossRef]
- Lygo, F.A.; Richard, B.; Wade, A.R.; Morland, A.B.; Baker, D.H. Neural markers of suppression in impaired binocular vision. Neuroimage 2021, 230, 117780. [Google Scholar] [CrossRef]
- Zhou, J.; Huang, P.C.; Hess, R.F. Interocular suppression in amblyopia for global orientation processing. J. Vis. 2013, 13, 19. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Hess, R.F.; Chan, L.Y.L.; Deng, D.; Yang, X.; Chen, X.; Yu, M.; Thompson, B. Quantitative measurement of interocular suppression in anisometropic amblyopia: A case-control study. Ophthalmology 2013, 120, 1672–1680. [Google Scholar] [CrossRef]
- Maehara, G.; Thompson, B.; Mansouri, B.; Farivar, R.; Hess, R.F. The perceptual consequences of interocular suppression in amblyopia. Investig. Ophthalmol. Vis. Sci. 2011, 52, 9011–9017. [Google Scholar] [CrossRef]
- Chen, H.; He, Z.; Xu, J.; Mao, Y.; Liang, Y.; Lin, D.; Xu, M.; Dai, Z.; Chen, X.; Zhou, J.; et al. A convenient and robust test to quantify interocular suppression for children with amblyopia. Iperception 2019, 10, 2041669519864971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong-Kee-You, A.M.B.; Wei, H.; Hou, C. Feature counting under dichoptic viewing in anisometropic and strabismic amblyopia. Transl. Vis. Sci. Technol. 2020, 9, 13. [Google Scholar] [CrossRef] [PubMed]
- Liang, M.; Xie, B.; Yang, H.; Yin, X.; Wang, H.; Yu, L.; He, S.; Wang, J. Altered interhemispheric functional connectivity in patients with anisometropic and strabismic amblyopia: A resting-state fMRI study. Neuroradiology 2017, 59, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, R.; Conner, I.P.; Odom, J.V.; Schwartz, T.L.; Mendola, J.D. Relating binocular and monocular vision in strabismic and anisometropic amblyopia. Arch. Ophthalmol. 2006, 124, 844–850. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fawcett, S.L.; Wang, Y.Z.; Birch, E.E. The critical period for susceptibility of human stereopsis. Investig. Ophthalmol. Vis. Sci. 2005, 46, 521–525. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean (SD) Median (Range) | Pre-Therapy | Post-Therapy | p-Value |
|---|---|---|---|
| Whole sample | |||
| Non-dominant BCVA | 0.58 (0.22) | 0.19 (0.19) | <0.001 |
| 0.52 (0.20 to 1.10) | 0.10 (0.00 to 0.70) | - | |
| Dominant BCVA | 0.11 (0.22) | 0.03 (0.09) | <0.001 |
| 0.00 (0.00 to 1.10) | 0.00 (0.00 to 0.60) | - | |
| BF | 4.14 (1.14) | 2.59 (0.91) | <0.001 |
| 5.00 (2.00 to 5.00) | 2.30 (1.00 to 5.00) | - | |
| Anisometropic group | |||
| Non-dominant BCVA | 0.59 (0.23) | 0.20 (0.20) | <0.001 |
| 0.54 (0.20 to 1.10) | 0.20 (0.00 to 0.70) | - | |
| Dominant BCVA | 0.00 (0.02) | 0.00 (0.00) | 0.18 |
| 0.00 (0.00 to 0.17) | 0.00 (0.00 to 0.00) | - | |
| BF | 4.39 (1.04) | 2.67 (0.97) | <0.001 |
| 5.00 (2.00 to 5.00) | 2.30 (1.00 to 5.00) | - | |
| Isometropic group BCVA | |||
| Non-dominant BCVA | 0.51 (0.19) | 0.14 (0.15) | <0.001 |
| 0.50 (0.24 to 1.10) | 0.10 (0.00 to 0.60) | - | |
| Dominant BCVA | 0.49 (0.19) | 0.15 (0.15) | <0.001 |
| 0.49 (0.22 to 1.10) | 0.15 (0.00 to 0.60) | - | |
| BF | 3.22 (1.01) | 2.27 (0.56) | <0.001 |
| 2.90 (2.00 to 5.00) | 2.30 (1.48 to 4.00) | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdal, M.O.; Bhombal, F.; Nankani, G.J.; Nankani, S.G.; Lad, S.; Dholam, A.; Kumari, R.; Mahajan, J.; Piñero, D.P. Evaluation of the Efficacy of a New Dichoptic Digital Platform to Treat the Anisometropic and Isometropic Amblyopia. Brain Sci. 2022, 12, 815. https://doi.org/10.3390/brainsci12070815
Abdal MO, Bhombal F, Nankani GJ, Nankani SG, Lad S, Dholam A, Kumari R, Mahajan J, Piñero DP. Evaluation of the Efficacy of a New Dichoptic Digital Platform to Treat the Anisometropic and Isometropic Amblyopia. Brain Sciences. 2022; 12(7):815. https://doi.org/10.3390/brainsci12070815
Chicago/Turabian StyleAbdal, Md Oliullah, Faiza Bhombal, Gul J. Nankani, Sonia G. Nankani, Shruti Lad, Aditi Dholam, Richa Kumari, Jinal Mahajan, and David P. Piñero. 2022. "Evaluation of the Efficacy of a New Dichoptic Digital Platform to Treat the Anisometropic and Isometropic Amblyopia" Brain Sciences 12, no. 7: 815. https://doi.org/10.3390/brainsci12070815