
Surpass Evolve Flow Diverter for the Treatment of Intracranial Aneurysm: A Systematic Review


Abstract
:1. Background
2. Materials and Methods
2.1. Search Strategy
2.2. Criteria for Considering Studies for the Review
2.3. Study Selection Process
2.4. Quality Assessment
2.5. Data Extraction
2.6. Data Analysis
3. Results
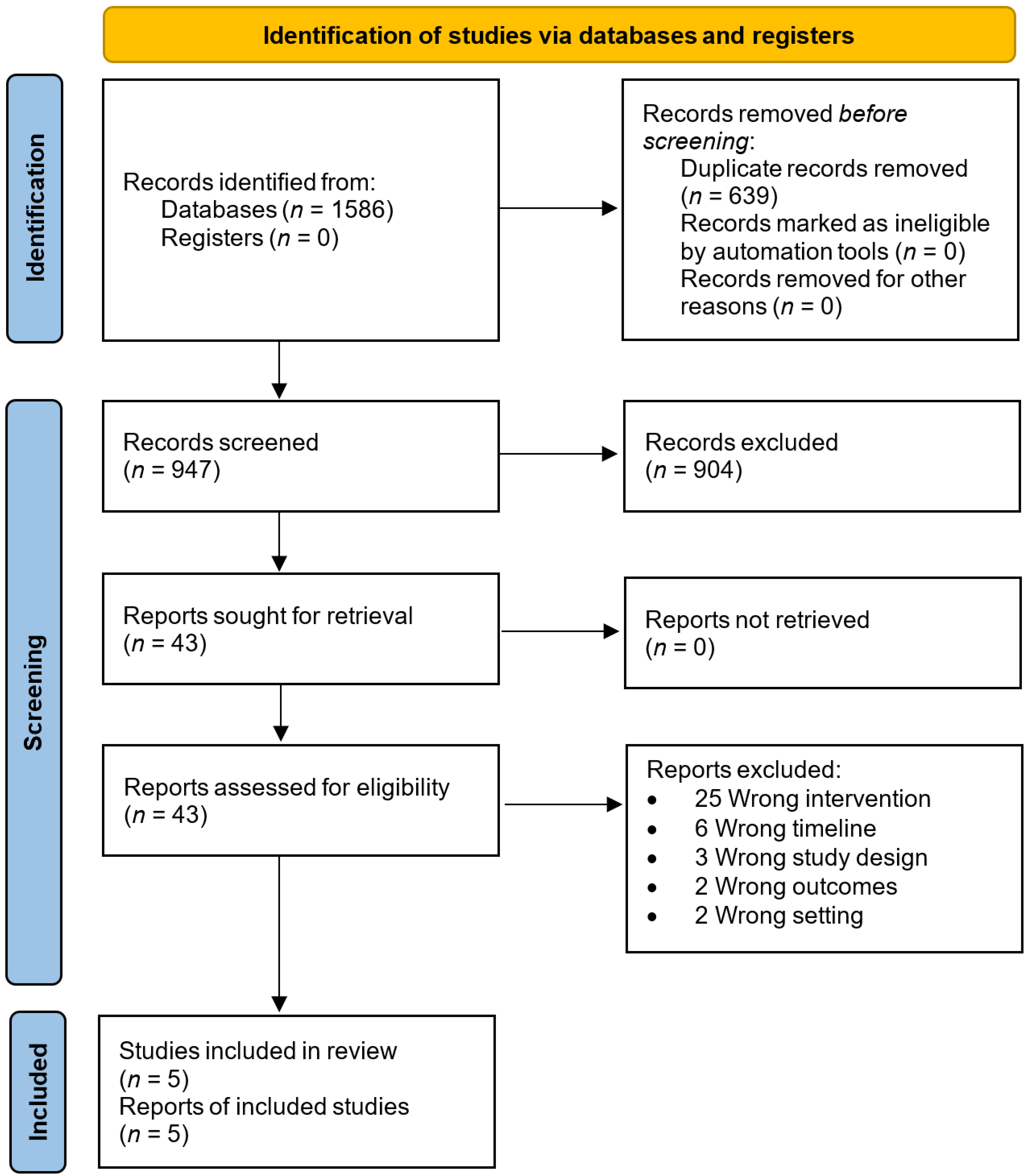
3.1. Studies Identified
3.2. Quality Assessment
3.3. Included Studies Characteristics
3.4. Studies Aims, Outcomes, and Conclusions
3.5. Studies Type of Aneurysms, Follow-Up Period, and Description of the Procedure
3.6. SE Complications and Outcomes
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huang, J.; van Gelder, J.M. The probability of sudden death from rupture of intracranial aneurysms: A meta-analysis. Neurosurgery 2002, 51, 1101–1105, discussion 1105. [Google Scholar] [CrossRef] [PubMed]
- Vlak, M.H.; Algra, A.; Brandenburg, R.; Rinkel, G.J. Prevalence of unruptured intracranial aneurysms, with emphasis on sex, age, comorbidity, country, and time period: A systematic review and meta-analysis. Lancet Neurol. 2011, 10, 626–636. [Google Scholar] [CrossRef]
- Pyysalo, L.; Luostarinen, T.; Keski-Nisula, L.; Öhman, J. Long-term excess mortality of patients with treated and untreated unruptured intracranial aneurysms. J. Neurol. Neurosurg. Psychiatry 2013, 84, 888–892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Briganti, F.; Leone, G.; Marseglia, M.; Mariniello, G.; Caranci, F.; Brunetti, A.; Maiuri, F. Endovascular treatment of cerebral aneurysms using flow-diverter devices: A systematic review. Neuroradiol. J. 2015, 28, 365–375. [Google Scholar] [CrossRef] [Green Version]
- Brinjikji, W.; Murad, M.H.; Lanzino, G.; Cloft, H.J.; Kallmes, D.F. Endovascular treatment of intracranial aneurysms with flow diverters: A meta-analysis. Stroke 2013, 44, 442–447. [Google Scholar] [CrossRef] [Green Version]
- Cancelliere, N.M.; Nicholson, P.; Radovanovic, I.; Mendes, K.M.; Orru, E.; Krings, T.; Pereira, V.M. Comparison of intra-aneurysmal flow modification using optical flow imaging to evaluate the performance of Evolve and Pipeline flow diverting stents. J. Neurointerv. Surg. 2020, 12, 814–817. [Google Scholar] [CrossRef]
- Agrawal, A.; Moscote-Salazar, L.R.; Janjua, T. Intracranial aneurysm: Research in preclinical outcome models and human effectiveness of intraluminal devices. Rom. Neurosurg. 2013, 35, 239–240. [Google Scholar] [CrossRef]
- Alderazi, Y.J.; Shastri, D.; Kass-Hout, T.; Prestigiacomo, C.J.; Gandhi, C.D. Flow diverters for intracranial aneurysms. Stroke Res. Treat. 2014, 2014, 415653. [Google Scholar] [CrossRef]
- Lee, I.T.-L.; Kao, Y.-S.; Lai, Y.-J.; Yen, H.-H. Flow diverter retreatment for intracranial aneurysms: A meta-analysis of efficacy and feasibility. Interv. Neuroradiol. 2022. [Google Scholar] [CrossRef]
- Becske, T.; Potts, M.B.; Shapiro, M.; Kallmes, D.F.; Brinjikji, W.; Saatci, I.; McDougall, C.G.; Szikora, I.; Lanzino, G.; Moran, C.J.; et al. Pipeline for uncoilable or failed aneurysms: 3-year follow-up results. J. Neurosurg. 2017, 127, 81–88. [Google Scholar] [CrossRef] [Green Version]
- Fischer, S.; Aguilar-Pérez, M.; Henkes, E.; Kurre, W.; Ganslandt, O.; Bäzner, H.; Henkes, H. Initial Experience with p64: A Novel Mechanically Detachable Flow Diverter for the Treatment of Intracranial Saccular Sidewall Aneurysms. AJNR Am. J. Neuroradiol. 2015, 36, 2082–2089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jou, L.-D.; Chintalapani, G.; Mawad, M.E. Metal coverage ratio of pipeline embolization device for treatment of unruptured aneurysms: Reality check. Interv. Neuroradiol. 2016, 22, 42–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jou, L.-D. In vitro digital subtraction angiographic evaluation of flow diverters in a patient-specific aneurysm. Interv. Neuroradiol. 2017, 23, 260–266. [Google Scholar] [CrossRef] [PubMed]
- Dandapat, S.; Mendez-Ruiz, A.; Martínez-Galdámez, M.; Macho, J.; Derakhshani, S.; Foa Torres, G.; Pereira, V.M.; Arat, A.; Wakhloo, A.K.; Ortega-Gutierrez, S. Review of current intracranial aneurysm flow diversion technology and clinical use. J. Neurointerv. Surg. 2021, 13, 54–62. [Google Scholar] [CrossRef]
- Rautio, R.; Alpay, K.; Sinisalo, M.; Numminen, J. Treatment of intracranial aneurysms using the new Surpass Evolve flow diverter: Safety outcomes and six-month imaging follow-up. J. Neuroradiol. 2022, 49, 80–86. [Google Scholar] [CrossRef]
- Orru, E.; Rice, H.; De Villiers, L.; Klostranec, J.M.; Wakhloo, A.K.; Coon, A.L.; Radovanovic, I.; Kortman, H.; Bhatia, K.D.; Krings, T.; et al. First clinical experience with the new Surpass Evolve flow diverter: Technical and clinical considerations. J. Neurointerv. Surg. 2020, 12, 974–980. [Google Scholar] [CrossRef]
- Lieber, B.B.; Sadasivan, C. Endoluminal scaffolds for vascular reconstruction and exclusion of aneurysms from the cerebral circulation. Stroke 2010, 41, S21–S25. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Murad, M.H.; Sultan, S.; Haffar, S.; Bazerbachi, F. Methodological quality and synthesis of case series and case reports. BMJ Evid. Based Med. 2018, 23, 60–63. [Google Scholar] [CrossRef] [Green Version]
- Critical Appraisal Skills Programme. CASP Cohort Study Checklist. 2018. Available online: https://casp-uk.net/casp-tools-checklists/ (accessed on 21 May 2022).
- Jee, T.K.; Yeon, J.Y.; Kim, K.H.; Kim, J.-S.; Hong, S.-C.; Jeon, P. Early clinical experience of using the Surpass Evolve flow diverter in the treatment of intracranial aneurysms. Neuroradiology 2022, 64, 343–351. [Google Scholar] [CrossRef]
- Lee, W.; Han, H.J.; Kim, J.; Park, K.Y.; Kim, Y.B.; Jang, C.K.; Chung, J. Flow diverter for the treatment of large (>10 mm) vertebral artery dissecting aneurysms. Acta Neurochir. 2021, 164, 1247–1254. [Google Scholar] [CrossRef] [PubMed]
- Maus, V.; Weber, W.; Berlis, A.; Maurer, C.; Fischer, S. Initial Experience with Surpass Evolve Flow Diverter in the Treatment of Intracranial Aneurysms. Clin. Neuroradiol. 2021, 31, 681–689. [Google Scholar] [CrossRef] [PubMed]
- Wakhloo, A.K.; Lylyk, P.; de Vries, J.; Taschner, C.; Lundquist, J.; Biondi, A.; Hartmann, M.; Szikora, I.; Pierot, L.; Sakai, N.; et al. Surpass flow diverter in the treatment of intracranial aneurysms: A prospective multicenter study. AJNR Am. J. Neuroradiol. 2015, 36, 98–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meyers, P.M.; Coon, A.L.; Kan, P.T.; Wakhloo, A.K.; Hanel, R.A. SCENT Trial. Stroke 2019, 50, 1473–1479. [Google Scholar] [CrossRef]
- Cerejo, R.; Bain, M.; Moore, N.; Hardman, J.; Bauer, A.; Hussain, M.S.; Masaryk, T.; Rasmussen, P.; Toth, G. Flow diverter treatment of intracranial vertebral artery dissecting pseudoaneurysms. J. Neurointerv. Surg. 2017, 9, 1064–1068. [Google Scholar] [CrossRef]
- Hanel, R.A.; Kallmes, D.F.; Lopes, D.K.; Nelson, P.K.; Siddiqui, A.; Jabbour, P.; Pereira, V.M.; Szikora István, I.; Zaidat, O.O.; Bettegowda, C.; et al. Prospective study on embolization of intracranial aneurysms with the pipeline device: The PREMIER study 1 year results. J. Neurointerv. Surg. 2020, 12, 62–66. [Google Scholar] [CrossRef]
- Pierot, L.; Spelle, L.; Berge, J.; Januel, A.-C.; Herbreteau, D.; Aggour, M.; Piotin, M.; Biondi, A.; Barreau, X.; Mounayer, C.; et al. SAFE study (Safety and efficacy Analysis of FRED Embolic device in aneurysm treatment): 1-year clinical and anatomical results. J. Neurointerv. Surg. 2019, 11, 184–189. [Google Scholar] [CrossRef]
- Briganti, F.; Leone, G.; Cirillo, L.; de Divitiis, O.; Solari, D.; Cappabianca, P. Postprocedural, midterm, and long-term results of cerebral aneurysms treated with flow-diverter devices: 7-year experience at a single center. Neurosurg. Focus 2017, 42, E3. [Google Scholar] [CrossRef]
- Florez, W.A.; Garcia-Ballestas, E.; Quiñones-Ossa, G.A.; Janjua, T.; Konar, S.; Agrawal, A.; Moscote-Salazar, L.R. Silk® Flow Diverter Device for Intracranial Aneurysm Treatment: A Systematic Review and Meta-Analysis. Neurointervention 2021, 16, 222–231. [Google Scholar] [CrossRef]
- Burrows, A.M.; Cloft, H.; Kallmes, D.F.; Lanzino, G. Periprocedural and mid-term technical and clinical events after flow diversion for intracranial aneurysms. J. Neurointerv. Surg. 2015, 7, 646–651. [Google Scholar] [CrossRef]
- Lubicz, B.; Collignon, L.; Raphaeli, G.; De Witte, O. Pipeline flow-diverter stent for endovascular treatment of intracranial aneurysms: Preliminary experience in 20 patients with 27 aneurysms. World Neurosurg. 2011, 76, 114–119. [Google Scholar] [CrossRef] [PubMed]
- Chalouhi, N.; Tjoumakaris, S.I.; Gonzalez, L.F.; Hasan, D.; Pema, P.J.; Gould, G.; Rosenwasser, R.H.; Jabbour, P.M. Spontaneous delayed migration/shortening of the pipeline embolization device: Report of 5 cases. AJNR Am. J. Neuroradiol. 2013, 34, 2326–2330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, Y.-H.; Wong, H.-F.; Hsu, S.-W. Endovascular management of spontaneous delayed migration of the flow-diverter stent. J. Neuroradiol. 2020, 47, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Möhlenbruch, M.A.; Herweh, C.; Jestaedt, L.; Stampfl, S.; Schönenberger, S.; Ringleb, P.A.; Bendszus, M.; Pham, M. The FRED flow-diverter stent for intracranial aneurysms: Clinical study to assess safety and efficacy. AJNR Am. J. Neuroradiol. 2015, 36, 1155–1161. [Google Scholar] [CrossRef] [Green Version]
- Kallmes, D.F.; Hanel, R.; Lopes, D.; Boccardi, E.; Bonafé, A.; Cekirge, S.; Fiorella, D.; Jabbour, P.; Levy, E.; McDougall, C.; et al. International retrospective study of the pipeline embolization device: A multicenter aneurysm treatment study. AJNR Am. J. Neuroradiol. 2015, 36, 108–115. [Google Scholar] [CrossRef] [Green Version]
- Nelson, P.K.; Lylyk, P.; Szikora, I.; Wetzel, S.G.; Wanke, I.; Fiorella, D. The pipeline embolization device for the intracranial treatment of aneurysms trial. AJNR Am. J. Neuroradiol. 2011, 32, 34–40. [Google Scholar] [CrossRef] [Green Version]
- Rouchaud, A.; Brinjikji, W.; Lanzino, G.; Cloft, H.J.; Kadirvel, R.; Kallmes, D.F. Delayed hemorrhagic complications after flow diversion for intracranial aneurysms: A literature overview. Neuroradiology 2016, 58, 171–177. [Google Scholar] [CrossRef] [Green Version]
- Becske, T.; Kallmes, D.F.; Saatci, I.; McDougall, C.G.; Szikora, I.; Lanzino, G.; Moran, C.J.; Woo, H.H.; Lopes, D.K.; Berez, A.L.; et al. Pipeline for uncoilable or failed aneurysms: Results from a multicenter clinical trial. Radiology 2013, 267, 858–868. [Google Scholar] [CrossRef]
- Gory, B.; Berge, J.; Bonafé, A.; Pierot, L.; Spelle, L.; Piotin, M.; Biondi, A.; Cognard, C.; Mounayer, C.; Sourour, N.; et al. Flow diverters for intracranial aneurysms: The DIVERSION national prospective cohort study. Stroke 2019, 50, 3471–3480. [Google Scholar] [CrossRef]
- Lv, X.; Yang, H.; Liu, P.; Li, Y. Flow-diverter devices in the treatment of intracranial aneurysms: A meta-analysis and systematic review. Neuroradiol. J. 2016, 29, 66–71. [Google Scholar] [CrossRef] [Green Version]
- Pierot, L.; Spelle, L.; Berge, J.; Januel, A.-C.; Herbreteau, D.; Aggour, M.; Piotin, M.; Biondi, A.; Barreau, X.; Mounayer, C.; et al. Feasibility, complications, morbidity, and mortality results at 6 months for aneurysm treatment with the Flow Re-Direction Endoluminal Device: Report of SAFE study. J. Neurointerv. Surg. 2018, 10, 765–770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shraim, B.A.; Shraim, M.A.; Ibrahim, A.R.; Elgamal, M.E.; Al-Omari, B.; Shraim, M. The association between early MRI and length of disability in acute lower back pain: A systematic review and narrative synthesis. BMC Musculoskelet. Disord. 2021, 22, 983. [Google Scholar] [CrossRef] [PubMed]
- Al-Omari, B.; McMeekin, P.; Bate, A. Systematic review of studies using conjoint analysis techniques to investigate patients’ preferences regarding osteoarthritis treatment. Patient Prefer. Adherence 2021, 15, 197–211. [Google Scholar] [CrossRef] [PubMed]
- Kühn, A.L.; Gounis, M.J.; Puri, A.S. Introduction: History and development of flow diverter technology and evolution. Neurosurgery 2020, 86, S3–S10. [Google Scholar] [CrossRef] [PubMed]
- ClinicalTrials.gov. Evaluation of Safety and Effectiveness of Stryker Surpass EvolveTM Flow Diverter System—Full Text View. Available online: https://clinicaltrials.gov/ct2/show/NCT04195568?term=surpass+evolve&cond=Intracranial+Aneurysm&draw=2&rank=1 (accessed on 20 February 2022).
- Ghorbani, M.; Shojaei, H.; Bavand, K.; Azar, M. Surpass Streamline Flow-Diverter Embolization Device for Treatment of Iatrogenic and Traumatic Internal Carotid Artery Injuries. AJNR Am. J. Neuroradiol. 2018, 39, 1107–1111. [Google Scholar] [CrossRef]
- Becske, T.; Brinjikji, W.; Potts, M.B.; Kallmes, D.F.; Shapiro, M.; Moran, C.J.; Levy, E.I.; McDougall, C.G.; Szikora, I.; Lanzino, G.; et al. Long-Term Clinical and Angiographic Outcomes Following Pipeline Embolization Device Treatment of Complex Internal Carotid Artery Aneurysms: Five-Year Results of the Pipeline for Uncoilable or Failed Aneurysms Trial. Neurosurgery 2017, 80, 40–48. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Items for Case Series Design | Jee et al. (2021) [21] | Lee et al. (2021) [22] | Maus et al. (2021) [23] | Orru et al. (2020) [16] | Rautio et al. (2021) [15] |
|---|---|---|---|---|---|
| 1. Does the patient(s) represent(s) the whole experience of the investigator (center) or is the selection method unclear to the extent that other patients with similar presentation may not have been reported? | ✵ | ✵ | ✵ | ✵ | |
| 2. Was the exposure adequately ascertained? | ✵ | ✵ | ✵ | ✵ | |
| 3. Was the outcome adequately ascertained? | ✵ | ✵ | ✵ | ✵ | |
| 4. Were other alternative causes that may explain the observation ruled out? | ✵ | ✵ | ? | ✵ | |
| 5. Is the case(s) described with sufficient details to allow other investigators to replicate the research or to allow practitioners make inferences related to their own practice? | ✵ | ✵ | ✵ | ✵ | |
| Items for cohort design | |||||
| 1. Did the study address a clearly focused issue? | ✵ | ||||
| 2. Was the cohort recruited in an acceptable way? | ✵ | ||||
| 3. Was the exposure accurately measured to minimize bias? | ✵ | ||||
| 4. Was the outcome accurately measured to minimize bias? | ✵ | ||||
| 5. Have the authors identified all important confounding factors? | ? | ||||
| 6. Have they taken account of the confounding factors in the design and/or analysis? | ? | ||||
| 7. Was the follow up of subjects complete enough? | ? | ||||
| 8. Was the follow up of subjects long enough? | ✵ | ||||
| 9. Do you believe the results? | ✵ | ||||
| 10. Can the results be applied to the local population? | ✵ | ||||
| 11. Do the results of this study fit with other available evidence? | ✵ | ||||
| 12. What are the implications of this study for practice? | ? | ||||
| Total stars out of 12 | 8/12 | 5/5 | 5/5 | 4/5 | 5/5 |
| References | Research Methods | Country of Study | Population | Sample Size | No. of Aneurysms/No. of SE | Participants’ Age Mean/Range | Participants (M/F) |
|---|---|---|---|---|---|---|---|
| Jee et al. (2021) [21] | Retrospective Cohort | Republic of Korea | Group 1 (SE-FD): patients with intracranial aneurysms treated with SE between June 2019 and December 2020 Group 2 (PED-FD and SS-FD): patients with intracranial aneurysms treated with other FDs (PED-FD and SS-FD) between July 2014 and December 2020 | 84 | 84/31 | 57.5 ± 13.9 Years | Group 1: 16M/15F Group 2: 26M/27F |
| Lee et al. (2021) [22] | Retrospective Case Series | Republic of Korea | Patients with unruptured VADAs between March 2013 and October 2020 were treated with FDs | 12 | 12/5 | 54.6/(42–77) Years | 9M/3F |
| Maus et al. (2021) [23] | Retrospective Case series | Germany | Patients with intracranial aneurysms treated with SE between May 2019 to June 2020 | 42 | 46/57 | 58/(28–84) Years | 10M/32F |
| Orru et al. (2020) [16] | Prospective Case series | Canada | Adults with anterior and posterior circulation aneurysms using SE between April and October 2019 | 25 | 26/29 | 58/(36–86) Years | 5M/20F |
| Rautio et al. (2021) [15] | Retrospective Case series | Finland | Adults with intracranial aneurysms (24 unruptured aneurysms, 5 ruptured aneurysms) from May 2019 to January 2020 | 29 | 30/31 | 55.5/(32–72) Years | 8M/21F |
| References | Study Main Aims | Primary Outcome | Secondary Outcome | Conclusion |
|---|---|---|---|---|
| Jee et al. (2021) [21] | Feasibility and safety profile in comparison with a control group treated with other types of flow diverters. | Technical failures, major complications, and unfavorable functional outcomes within 6 months after flow diversion | Procedural time, balloon angioplasty, and diffusion-weighted imaging (DWI)-positive lesions on post-procedural MRI | SE is safe and easy to deploy. However, a study on the long-term safety and efficacy outcomes is required for this new device. |
| Lee et al. (2021) [22] | Evaluate the outcomes of FDD in large VADAs and assess the safety and feasibility of FDD in the treatment of unruptured large VADAs. | Clinical outcome of last follow-up using modified Rankin Scale (mRS) | Radiographic outcome immediately and 6 months after the procedure using OKM grade | Treatment of large VADAs using FDD is feasible and effective based on the favorable occlusion rate and clinical outcome. |
| Maus et al. (2021) [23] | Examine the feasibility, efficacy, and safety profile of the new SE flow diverter in the treatment of intracranial wide-necked aneurysms. | Technical success: favorable navigation to the target vessel and successful deployment of the SE | Favorable aneurysm occlusion is defined as OKM grade on follow-up, procedure-related complications, and retreatment | SE flow diverter is safe and effective with promising occlusion rates at short-term follow-up. |
| Orru et al. (2020) [16] | Describe the results in patients treated with SE. | Immediate post-procedure aneurysm thrombosis using OKM grade | Radiological follow-up, clinical status using mRS, and neurological complications | Demonstrated excellent success rate, good safety, and efficacy of the SE with excellent navigability and resistance to twisting while maintaining high flow diverting effect and positioning. |
| Rautio et al. (2021) [15] | Safety and six-month follow-up outcomes using the new SE flow diverter in the treatment of intracranial aneurysms. | Clinical safety was assessed by the absence of death, absence of major and minor stroke, and absence of a transient ischemic attack | Treatment efficacy by angiographic occlusion using the OKM grading scale immediately after the procedure and at 6 months follow-up | SE works well with no intraprocedural thromboembolic complications and occlusion rates comparable to other FDs. |
| References | Type of Aneurysms | Type of Aneurysms Treated with SE | Period of Follow up | Description of Procedure |
|---|---|---|---|---|
| Jee et al. (2021) [21] | Group 1 Location: Anterior circulation: n = 20 (64.5%) Posterior circulation: n = 11 (35.5%) Size: Mean diameter 18.4 ± 7.6 mm Small n = 4 (12.9%) Large n = 17 (54.8%) Giant n = 10 (32.3%) Shape: Saccular n = 11 (35.5%) Non-saccular n = 20 (64.5%) Group 2 Location: Anterior circulation: n = 35 (66.1%) Posterior circulation: n = 18 (34%) Size: Mean diameter 20.6 ± 7.0 mm Small n = 0 (0.0%) Large n = 37 (69.8%) Giant n = 16 (30.2%) Shape: Saccular n = 25 (47.2%) Non-saccular n = 28 (52.8%) | Location: Anterior circulation: n = 20 (64.5%) Posterior circulation: n = 11 (35.5%) Size: Mean diameter 18.4 ± 7.6 mm Small n = 4 (12.9%) Large n = 17 (54.8%) Giant n = 10 (32.3%) Shape: Non-saccular n = 20 (64.5%) Saccular n = 11 (35.5%) | Six months | DAPT aspirin 100 mg + clopidogrel 75 mg for 5–14 days OR loading dose (300 mg) aspirin + clopidogrel for 1 or 2 days given before procedure. Platelet function test was assessed in all patients using VerifyNow Assay. Poor responders were switched to ticlopidine 250 mg twice a day. Specific flow diverter selection was based on the operator’s preference. Immediate and post-flow diversion angiography, as well as, Dyna CT imaging performed in all cases. Balloon angioplasty was performed to improve vessel wall apposition if necessary. Incomplete coverage of target aneurysm neck resulted in additional stenting. |
| Lee et al. (2021) [22] | Location: Posterior circulation: n = 12 -At level PICA n = 4 -Proximal to PICA n = 4 -Distal to PICA n = 4 Size: Large n = 11 Giant n = 1 Shape: All dissecting aneurysms | Location: Posterior circulation: n = 5 -At level PICA n = 1 -Proximal to PICA n = 2 -Distal to PICA n = 2 Size: Large n = 5 Shape: All dissecting aneurysms | 6–16 months | DAPT aspirin 100 mg + clopidogrel 75 mg daily at least 5 days before the procedure and heparin during the procedure. Platelet function tests were assessed using VerifyNow Assay. The FDD was accessed through the femoral artery. No additional coiling was used. The size of FDD was determined based on the diameter of the parent artery and the length of dissecting segment. VasoCT was performed to confirm wall opposition. DAPT continued for 6 months post-op then switched to aspirin alone. |
| Maus et al. (2021) [23] | Location: Anterior circulation: n = 41 (89%) Posterior circulation: n = 5 (11%) Size: Median size 6.6 mm (IQR 4.0–12.2 mm) Median neck width 4 mm (IQR 2.2–5.4 mm) Small n = 34 (74%) Large/Giant n = 12 (26%) Shape: Saccular n = 30 (65%) Fusiform n = 10 (22%) Blister n = 4 (9%) Dissecting n = 2 (4%) | Location: Anterior circulation: n = 41 (89%) Posterior circulation: n = 5 (11%) Size: Median aneurysm size 6.6 mm (IQR 4.0–12.2 mm) Median neck width 4 mm (IQR 2.2–5.4 mm) Small n = 34 (74%) Large/Giant n = 12 (26%) Shape: Saccular n = 30 (65%) Fusiform n = 10 (22%) Blister n = 4 (9%) Dissecting n = 2 (4%) | Follow-up median 116 days/IQR 92–134 days | DAPT aspirin 100 mg + clopidogrel 75 mg for 5 days prior to procedure. Platelet function test assessed using Multiplate Analyzer. Poor responders either had dose escalation of clopidogrel 150 mg/day or switched to prasugrel. Bolus heparin was administered during the procedure. The FDD was accessed through the femoral artery. The number flow diverter was deployed based on the operator’s discretion. CT scan was performed to confirm aneurysm occlusion. DAPT continued for 3 months post-op then switched to aspirin alone or life. |
| Orru et al. (2020) [16] | Location: Anterior circulation n = 25 (96%) Posterior circulation n = 1 (4%) Size: Mean diameter 11mm (range 3–30 mm) Small n = 16 (58%) Large n = 8 (31%) Giant n = 2 (8%) Shape: Saccular n = 24 (92%) Fusiform n = 1 (4%) Dissecting n = 1 (4%) | Location: Anterior circulation n = 25 (96%) Posterior circulation n = 1 (4%) Size: Mean diameter 11mm (range 3–30 mm) Small n = 16 (58%) Large n = 8 (31%) Giant n = 2 (8%) Fusiform partially thrombosed n = 1 (4%) Shape: Saccular n = 24 (92%) Fusiform n = 1 (4%) Dissecting n = 1 (4%) | Five days–six months | DAPT aspirin + ticagrelor/clopidogrel for 3 days before the procedure and continued for at least 6 months. Intravenous heparin was administered intraoperatively. The FD was accessed through the femoral artery or radial artery. Additional FD implanted when indicated and adjunctive coils placed upon operator preference. VasoCT was performed to confirm correct FD wall opposition. |
| Rautio et al. (2021) [15] | Location: Anterior circulation n = 24 Posterior circulation n = 6 Size: Small n = 20 Large n = 9 Giant n = 1 Shape: Saccular n = 28 Fusiform n = 2 | Location: Anterior circulation n = 24 Posterior circulation n = 6 Size: Small n = 20 Large n = 9 Giant n = 1 Shape: Saccular n = 28 Fusiform n = 2 | 3–6 months | DAPT aspirin 100 mg + prasugrel 10 mg or clopidogrel 75 mg for at least 5–7 days preoperatively. Platelet function test assessed using Multiplate Analyzer or VerifyNow in elective cases. Bolus heparin was administered intraoperatively. Acute cases were given intravenous 250–500 mg aspirin before, during, and after the procedure with a prasugrel loading dose. FD was accessed through the femoral artery or radial artery. Adjunctive coils are placed upon the operator’s preference. The size of FD was determined based on the diameter of the artery and the main operator decision. VasoCT/DSA imaging was performed to confirm wall opposition. |
| References | Complete/Partial Occlusion Good Clinical Outcome | mRS/Period | Technical Success | Radiological Outcome |
|---|---|---|---|---|
| Jee et al. (2021) [21] | Complete occlusion n = 11 (35%)/Partial occlusion NR at 6-month follow-up. | NR for all patients | 90.3% | Postprocedural MRI within 5 days of flow diversion. DSA, MRI, and/or CT angiography, at 6 months after flow diversion. |
| Lee et al. (2021) [22] | Complete occlusion n = 3 (60%)/Partial occlusion n = 2 (40%) at 6 months follow up | mRS ≤ 2/15.8 months | NR | Immediately: OKM B3 n = 3 OKM A3 n = 2 Follow up: OKM C3 n = 2 OKM D n = 3 |
| Maus et al. (2021) [23] | Complete occlusion n = 27 (75%)/Partial occlusion n = 4 (11%) at median follow-up was 116 days. | mRS ≤ 2/at discharge | 96% | Follow up: OKM D n = 27 OKM C1–C3 n = 4 OKM B1 & B3 n = 3 OKM A2 n = 2 |
| Orru et al. (2020) [16] | Complete occlusion n = 13/23 (57%) /Partial occlusion n = 9/23 (39%) at 4 months follow up | mRS ≤ 2/at discharge | Excellent technical success rates in all cases | Immediately: OKM D n = 1 OKM B n = 12 OKM A n = 13 (12 of these lesions OKM grade = A3) |
| Rautio et al. (2021) [15] | Immediate post-op occlusion: Complete occlusion n = 0 (0%)/Partial occlusion n = 3 (10%) Follow-up 6 months: Complete occlusion 15/27 (56%)/Partial occlusion n = 6/27 (22%) | mRS ≤ 2/NR | Encouraging technical success and Good radiological outcomes | Immediately: OKM D n = 0/30 OKM C n = 3/30 OKM B n = 7/30 OKM A n = 20/30 Follow up: OKM D n = 15/27 OKM C n = 6/27 OKM B n = 6/27 OKM A n = 0/27 |
| References | Perioperative Complications | Postoperative Complications | Long-Term Morbidity (n) | Deaths (n)/days Post-Procedure |
|---|---|---|---|---|
| Jee et al. (2021) [21] | Incomplete wall opposition n = 1 (3.2%)—Large Stent migration n = 1 (3.2%)—Giant Aneurysm rupture NR | Delayed stent migration n = 1 (3.2%) Stent thrombosis n = 1 (3.2%) Delayed aneurysm rupture n = 1 (3.2%) Ischemic stroke n = 1 (3.2%) RIPH Hemorrhage n = 0 (0%) Neurological n = 0 (0%) Intimal hyperplasia NR | 0 long-term morbidity | 1 death/16 days |
| Lee et al. (2021) [22] | No intraprocedural complications | Delayed stent migration NR Stent thrombosis n = 0 (0%) Delayed aneurysm rupture n = 0 (0%) Ischemic stroke n = 0 (0%) RIPH Hemorrhage n = 0 (0%) ASA obstruction n = 0 (0%) Neurological n = 0 (0%) Intimal hyperplasia n = 2 (40%) | 0 long-term morbidity | 0/0 |
| Maus et al. (2021) [23] | Incomplete wall opposition n = 1 (2%) Stent migration n = 1 (2%) Stent thrombosis n = 1 (2%) Aneurysm rupture n = 0 (0%) | Delayed stent migration NR Stent thrombosis n = 1 (2%) Delayed aneurysm rupture n = 0 (0%) Ischemic stroke n = 3 (7%) RIPH Hemorrhage n = 0 (0%) Neurological (minor) n = 1 (2%) Intimal hyperplasia (mild) n = 3/34 (9%) (Severe) n = 1/34 (3%) | 0 long-term morbidity | 1 death/10 days |
| Orru et al. (2020) [16] | No intraprocedural complications | Delayed stent migration NR Stent thrombosis n = 1 (4%) Delayed aneurysm rupture NR Ischemic stroke n = 1 (4%) RIPH Hemorrhage n = 0 (0%) Neurological (minor) n = 5 (20%) (Major) n = 1 (4%) Intimal hyperplasia NR Others n = 3 (12%) | mRS score 4 in one patient suffered a left-sided hemispheric stroke | 0/0 |
| Rautio et al. (2021) [15] | No intraprocedural complications | Delayed stent migration NR Stent thrombosis n = 2 (7%) Delayed aneurysm rupture n = 1 (3%)—Large Ischemic stroke n = 1 (3%)—Large RIPH Hemorrhage n = 2 (7%) (1 SAH & SAH + ICH)—1 Small, 1 Large Neurological (minor) n = 1 (3%) (Major) n = 1 (3%) Intimal hyperplasia (minor) n = 11 (45%) | One patient’s mRS status changed from 1 to 2 after SAH | 2 deaths/6 and 12 days |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Issa, R.; Al-Homedi, Z.; Syed, D.H.; Aziz, W.; Al-Omari, B. Surpass Evolve Flow Diverter for the Treatment of Intracranial Aneurysm: A Systematic Review. Brain Sci. 2022, 12, 810. https://doi.org/10.3390/brainsci12060810
Issa R, Al-Homedi Z, Syed DH, Aziz W, Al-Omari B. Surpass Evolve Flow Diverter for the Treatment of Intracranial Aneurysm: A Systematic Review. Brain Sciences. 2022; 12(6):810. https://doi.org/10.3390/brainsci12060810
Chicago/Turabian StyleIssa, Rania, Zahrah Al-Homedi, Dawood Hasan Syed, Waseem Aziz, and Basem Al-Omari. 2022. "Surpass Evolve Flow Diverter for the Treatment of Intracranial Aneurysm: A Systematic Review" Brain Sciences 12, no. 6: 810. https://doi.org/10.3390/brainsci12060810