
IL-10 Gene Polymorphisms and IL-10 Serum Levels in Patients with Multiple Sclerosis in Lithuania

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Polymorphism Selection
2.3. The DNA Extraction and Genotyping
2.4. Quantification of IL-10 Serum Levels
2.5. Statistical Analysis
3. Results
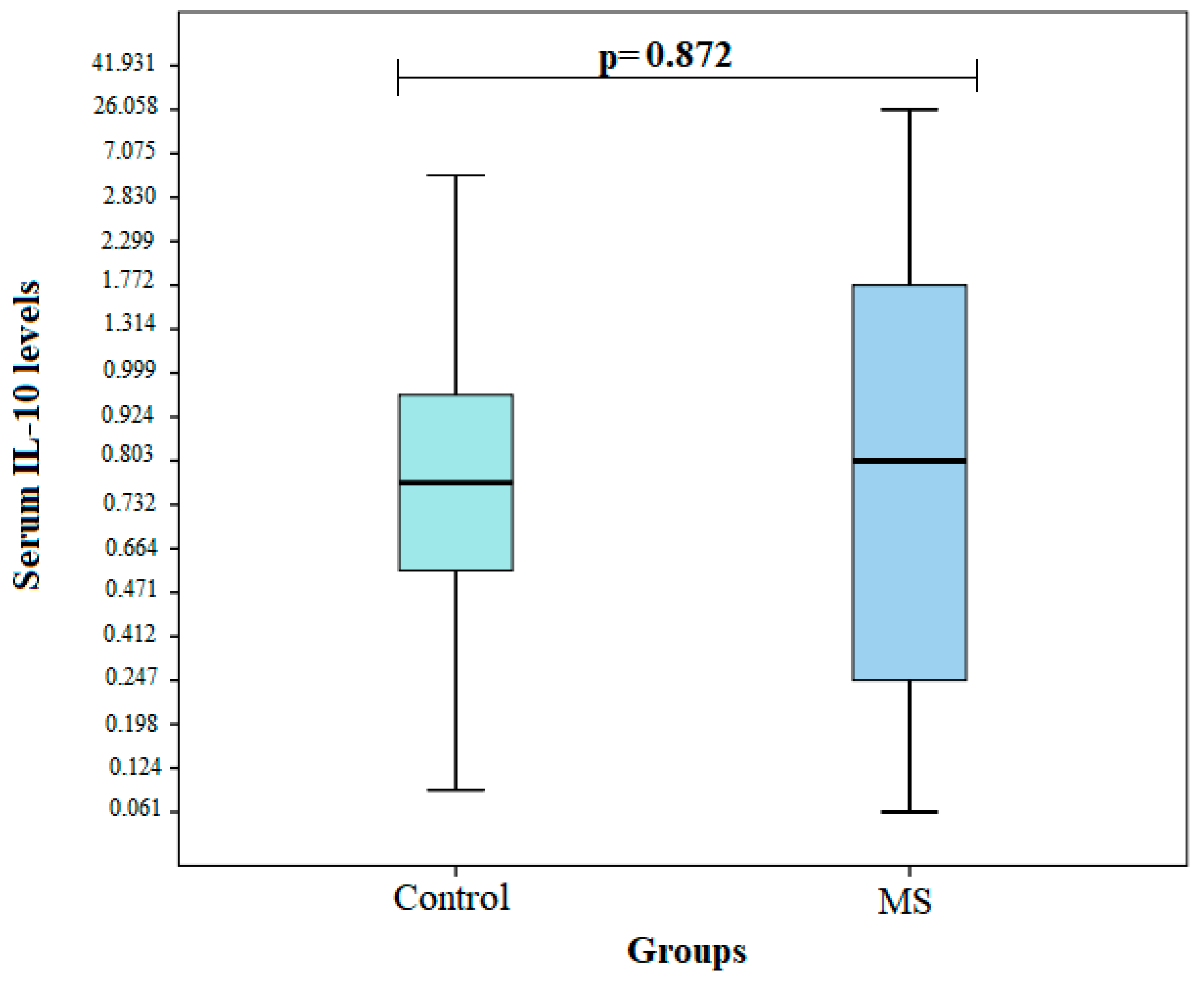
3.1. IL-10 Serum Levels in MS and Control Groups
3.2. IL-10 Haplotype Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thompson, A.J.; Baranzini, S.E.; Geurts, J.; Hemmer, B.; Ciccarelli, O. Multiple sclerosis. Lancet 2018, 391, 1622–1636. [Google Scholar] [CrossRef]
- Koch-Henriksen, N.; Sørensen, P.S. The changing demographic pattern of multiple sclerosis epidemiology. Lancet Neurol. 2010, 9, 520–532. [Google Scholar] [CrossRef]
- Leray, E.; Moreau, T.; Fromont, A.; Edan, G. Epidemiology of multiple sclerosis. Rev. Neurol. 2016, 172, 3–13. [Google Scholar] [CrossRef]
- Tullman, M.J. Overview of the epidemiology, diagnosis, and disease progression associated with multiple sclerosis. Am. J. Manag. Care 2013, 19 (Suppl. S2), S15–S20. [Google Scholar]
- Marabita, F.; Almgren, M.; Sjöholm, L.K.; Kular, L.; Liu, Y.; James, T.; Kiss, N.B.; Feinberg, A.P.; Olsson, T.; Kockum, I.; et al. Smoking induces DNA methylation changes in Multiple Sclerosis patients with exposure-response relationship. Sci. Rep. 2017, 1, 7. [Google Scholar] [CrossRef] [Green Version]
- Karussis, D. The diagnosis of multiple sclerosis and the various related demyelinating syndromes: A critical review. J. Autoimmun. 2014, 48, 134–142. [Google Scholar] [CrossRef]
- Xia, Z.; White, C.C.; Owen, E.K.; von Korff, A.; Clarkson, S.R.; McCabe, C.A.; Cimpean, M.; Winn, P.A.; Hoesing, A.; Steele, S.U.; et al. Genes and Environment in Multiple Sclerosis project: A platform to investigate multiple sclerosis risk. Ann. Neurol. 2016, 79, 178–189. [Google Scholar] [CrossRef]
- Ramakrishnan, V.; Akram Husain, R.S.; Ahmed, S.S. Genetic predisposition of IL-10 promoter polymorphisms with risk of multiple sclerosis: A meta-analysis. J. Neuroimmunol. 2017, 306, 11–18. [Google Scholar] [CrossRef]
- Shahbazi, M.; Abadi, J.S.A.; Roshandel, D.; Koochaki, M.; Amiri, H.; Kohansal, R.; Baghbanian, S.M.; Zamani, M. Combination of interleukin-10 gene promoter polymorphisms with HLA-DRB1*15 allele is associated with multiple sclerosis. Indian J. Med. Res. 2017, 145, 746–752. [Google Scholar] [CrossRef]
- Feigin, V.L.; Abajobir, A.A.; Abate, K.H.; Abd-Allah, F.; Abdulle, A.M.; Abera, S.F.; Abyu, G.Y.; Ahmed, M.B.; Aichour, A.N.; Aichour, I.; et al. Global, regional, and national burden of neurological disorders during 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Neurol. 2017, 16, 877–897. [Google Scholar] [CrossRef] [Green Version]
- Huang, W.J.; Chen, W.W.; Zhang, X. Multiple sclerosis: Pathology, diagnosis and treatments. Exp. Ther. Med. 2017, 13, 3163–3166. [Google Scholar] [CrossRef] [Green Version]
- Filippi, M.; Rocca, M.A.; Ciccarelli, O.; De Stefano, N.; Evangelou, N.; Kappos, L.; Rovira, A.; Sastre-Garriga, J.; Tintorè, M.; Frederiksen, J.L.; et al. MRI criteria for the diagnosis of multiple sclerosis: MAGNIMS consensus guidelines. Lancet Neurol. 2016, 15, 292–303. [Google Scholar] [CrossRef] [Green Version]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Mohammadi, S.; Saghaeian Jazi, M.; Zare Ebrahimabad, M.; Eghbalpour, F.; Abdolahi, N.; Tabarraei, A.; Yazdani, Y. Interleukin 10 gene promoter polymorphisms (rs1800896, rs1800871 and rs1800872) and haplotypes are associated with the activity of systemic lupus erythematosus and IL10 levels in an Iranian population. Int. J. Immunogenet. 2019, 46, 20–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luomala, M.; Lehtimäki, T.; Huhtala, H.; Ukkonen, M.; Koivula, T.; Hurme, M.; Elovaara, I. Promoter polymorphism of IL-10 and severity of multiple sclerosis. Acta Neurol. Scand. 2003, 108, 396–400. [Google Scholar] [CrossRef] [PubMed]
- Asgharzadeh, M.; Sanajoo, D.; Mahdavi, P.B.; Samadi, K.H.; Gholizadeh, P.; Rashedi, J. Interleukin-10 Promoter and the CCR5 Polymorphisms in Iranian Azari Population with Multiple Sclerosis. Iran. J. Immunol. 2021, 18, 241–248. [Google Scholar]
- Al-Naseri, M.A.; Salman, E.D.; Ad’hiah, A.H. Association between interleukin-4 and interleukin-10 single nucleotide polymorphisms and multiple sclerosis among Iraqi patients. Neurol. Sci. 2019, 40, 2383–2389. [Google Scholar] [CrossRef]
- Mihailova, S.; Ivanova, M.; Mihaylova, A.; Quin, L.; Mikova, O.; Naumova, E. Pro- and anti-inflammatory cytokine gene polymorphism profiles in Bulgarian multiple sclerosis patients. J. Neuroimmunol. 2005, 168, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Azarpira, N.; Haghighi, A.B.; Pourjafar, M.; Shariat, A. Interleukin 10 gene polymorphism in Iranian patients with multiple sclerosis. Acta. Neurol. Taiwan 2010, 19, 107–111. [Google Scholar] [PubMed]
- de Jong, B.A.; Schrijver, H.M.; Huizinga, T.W.J.; Bollen, E.L.E.M.; Polman, C.H.; Uitdehaag, B.M.J.; Kersbergen, M.C.; Sturk, A.; Westendorp, R.G.J. Innate Production of Interleukin-10 and Tumor Necrosis Factor Affects the Risk of Multiple Sclerosis. Ann. Neurol. Off. J. Am. Neurol. Assoc. Child Neurol. Soc. 2000, 48, 641–646. [Google Scholar] [CrossRef]
- Myhr, K.M.; Vågnes, K.S.; Marøy, T.H.; Aarseth, J.H.; Nyland, H.I.; Vedeler, C.A. Interleukin-10 promoter polymorphisms in patients with multiple sclerosis. J. Neurol. Sci. 2002, 202, 93–97. [Google Scholar] [CrossRef]
- Silva, T.; Fragoso, Y.D.; Rodrigues, M.F.S.D.; Gomes, A.O.; da Silva, F.C.; Andreo, L.; Viana, A.; da Silva, D.D.T.; Chavantes, M.C.; Horliana, A.C.R.T.; et al. Effects of photobiomodulation on interleukin-10 and nitrites in individuals with relapsing-remitting multiple sclerosis—Randomized clinical trial. PLoS ONE 2020, 15, e0230551. [Google Scholar] [CrossRef] [PubMed]
- Kwilasz, A.J.; Grace, P.M.; Serbedzija, P.; Maier, S.F.; Watkins, L.R. The therapeutic potential of interleukin-10 in neuroimmune diseases. Neuropharmacology 2015, 96, 55–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molina-Holgado, E.; Arévalo-Martín, A.; Castrillo, A.; Boscá, L.; Vela, J.M.; Guaza, C. Interleukin-4 and interleukin-10 modulate nuclear factor kappaB activity and nitric oxide synthase-2 expression in Theiler’s virus-infected brain astrocytes. J. Neurochem. 2002, 81, 1242–1252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trenova, A.G.; Slavov, G.S.; Draganova-Filipova, M.N.; Mateva, N.G.; Manova, M.G.; Miteva, L.D.; Stanilova, S.A. Circulating levels of interleukin-17A, tumor necrosis factor-alpha, interleukin-18, interleukin-10, and cognitive performance of patients with relapsing-remitting multiple sclerosis. Neurol. Res. 2018, 40, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Sedeeq, M.S.; El-Nahrery, E.M.A.; Shalaby, N.; Hussein, M.; Shehata, H.; el Aal, R.A.; Ghaffar, N.F.A.; Mohamed, M.M. Micro-RNA-96 and interleukin-10 are independent biomarkers for multiple sclerosis activity. J. Neurol. Sci. 2019, 403, 92–96. [Google Scholar] [CrossRef] [PubMed]
- Bettelli, E.; Das, M.P.; Howard, E.D.; Weiner, H.L.; Sobel, R.A.; Kuchroo, V.K. IL-10 is critical in the regulation of autoimmune encephalomyelitis as demonstrated by studies of IL-10- and IL-4-deficient and transgenic mice. J. Immunol. 1998, 161, 3299–3306. [Google Scholar] [PubMed]
- Samoilova, E.B.; Horton, J.L.; Chen, Y. Acceleration of experimental autoimmune encephalomyelitis in interleukin-10-deficient mice: Roles of interleukin-10 in disease progression and recovery. Cell Immunol. 1998, 188, 118–124. [Google Scholar] [CrossRef] [Green Version]
- Nagelkerken, L.; Blauw, B.; Tielemans, M. IL-4 abrogates the inhibitory effect of IL-10 on the development of experimental allergic encephalomyelitis in SJL mice. Int. Immunol. 1997, 9, 1243–1251. [Google Scholar] [CrossRef] [Green Version]
- Cannella, B.; Gao, Y.L.; Brosnan, C.; Raine, C.S. IL-10 Fails to Abrogate Experimental Autoimmune Encephalomyelitis. J. Neurosci. Res. 1996, 45, 735–746. [Google Scholar] [CrossRef]
- Cua, D.J.; Hutchins, B.; LaFace, D.M.; Stohlman, S.A.; Coffman, R.L. Central nervous system expression of IL-10 inhibits autoimmune encephalomyelitis. J. Immunol. 2001, 166, 602–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Croxford, J.L.; Feldmann, M.; Chernajovsky, Y.; Baker, D. Different therapeutic outcomes in experimental allergic encephalomyelitis dependent upon the mode of delivery of IL-10: A comparison of the effects of protein, adenoviral or retroviral IL-10 delivery into the central nervous system. J. Immunol. 2001, 166, 4124–4130. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Characteristics | Group | p-Value | |
|---|---|---|---|
| I Group: Subjects with MS (n = 148) | II Group: Control Group (n = 213) | ||
| Men, n (%) | 54 (36.5) | 65 (30.5) | 0.235 |
| Women, n (%) | 94 (63.5) | 148 (69.5) | |
| Age, median (IQR) | 36 (16) | 31 (19) | 0.269 |
| SNP | Genotype/Allele | MS Group (n = 148) N (%) | Control Group (n = 213) N (%) | p-Value | HWE p-Value |
|---|---|---|---|---|---|
| IL-10 rs1800871 | GG | 89 (60.1) | 118 (55.4) | 0.547 | 0.946 |
| AG | 53 (35.8) | 82 (38.5) | |||
| AA | 6 (4.1) | 13 (6.1) | |||
| In total: | 148 (100) | 213 (100) | |||
| Allele: G A | 231(78) 65 (22) | 318 (74.6) 108 (25.4) | 0.294 | ||
| IL-10 rs1800872 | GG | 87 (58.8) | 119 (55.9) | 0.785 | 0.869 |
| TG | 54 (36.5) | 81 (38.0) | |||
| TT | 7 (4.7) | 13 (6.1) | |||
| In total: | 148 (100) | 213 (100) | |||
| Allele: G T | 228 (77) 68 (23) | 319 (74.9) 107 (25.1) | 0.508 | ||
| IL-10 rs1800896 | TT | 42 (28.4) | 75 (35.2) | 0.312 | 0.207 |
| TC | 71 (48.0) | 98 (46.0) | |||
| CC | 35 (23.6) | 40 (18.8) | |||
| In total: | 148 (100) | 213 (100) | |||
| Alelle: T C | 155 (52.4) 141 (47.6) | 248 (58.2) 178 (41.8) | 0.119 |
| SNP | Genotype/Allele | ≤30 Age | p-Value | >30 Age | p-Value | ||
|---|---|---|---|---|---|---|---|
| MS Group (n = 49) N (%) | Control Group (n = 105) N (%) | MS Group (n = 99) N (%) | Control Group (n = 108) N (%) | ||||
| IL-10 rs1800871 | GG | 25 (51.0) | 58 (55.2) | 0.532 | 64 (64.7) | 60 (55.6) | 0.407 |
| AG | 22 (44.9) | 39 (37.1) | 31 (31.3) | 43 (39.8) | |||
| AA | 2 (4.1) | 8 (7.6) | 4 (4.0) | 5 (4.6) | |||
| Allele: A G | 72 (73.5) 26 (26.5) | 155 (73.8) 55 (26.2) | 0.949 | 159 (80.3) 39 (19.7) | 163 (75.5) 53 (24.5) | 0.237 | |
| IL-10 rs1800872 | GG | 24 (49.0) | 58 (55.2) | 0.430 | 63 (63.6) | 61 (56.5) | 0.522 |
| GT | 23 (46.9) | 39 (37.1) | 31 (31.3) | 42 (38.9) | |||
| TT | 2 (4.1) | 8 (7.6) | 5 (5.1) | 5 (4.6) | |||
| Allele: G T | 71 (72.4) 27 (27.6) | 155 (73.8) 55 (26.2) | 0.801 | 157 (79.3) 41 (20.7) | 164 (75.9) 52 (24.1) | 0.412 | |
| IL-10 rs1800896 | TT | 18 (36.7) | 43 (41.0) | 0.883 | 24 (24.2) | 32 (29.6) | 0.580 |
| TC | 23 (46.9) | 46 (43.8) | 48 (48.5) | 52 (48.1) | |||
| CC | 8 (16.3) | 16 (15.2) | 27 (27.3) | 24 (22.2) | |||
| Allele: C T | 59 (60.2) 39 (39.2) | 132 (62.9) 78 (37.1) | 0.655 | 96 (48.5) 102 (51.5) | 116 (53.7) 100 (46.3) | 0.289 | |
| SNP | Genotype/Allele | Men | p-Value | Women | p-Value | ||
|---|---|---|---|---|---|---|---|
| MS Group (n = 54) % | Control Group (n = 65) % | MS Group (n = 94) Proc. | Control Group (n = 148) % | ||||
| IL-10 rs1800871 | GG | 33 (61.1) | 36 (55.4) | 0.751 | 56 (59.6) | 82 (55.4) | 0.463 |
| AG | 18 (33.3) | 26 (40.0) | 35 (37.2) | 56 (37.8) | |||
| AA | 3 (5.6) | 3 (4.6) | 3 (3.2) | 10 (6.8) | |||
| Allele: A G | 84 (77.8) 24 (22.2) | 98 (75.4) 32 (24.6) | 0.665 | 147 (78.2) 41 (21.8) | 220 (74.3) 76 (25.7) | 0.333 | |
| IL-10 rs1800872 | GG | 30 (55.6) | 36 (55.4) | 0.795 | 57 (60.6) | 83 (56.1) | 0.453 |
| TG | 20 (37.0) | 26 (40.0) | 34 (36.2) | 55 (37.2) | |||
| TT | 4 (7.4) | 3 (4.6) | 3 (3.2) | 10 (6.8) | |||
| Allele: G T | 80 (74.1) 28 (25.9) | 98 (75.4) 32 (24.6) | 0.817 | 148 (78.7) 40 (21.3) | 221 (74.7) 75 (25.3) | 0.306 | |
| IL-10 rs1800896 | TT | 16 (29.6) | 19 (29.2) | 0.987 | 26 (27.7) | 56 (37.8) | 0.204 |
| TC | 25 (46.3) | 31 (47.7) | 46 (48.9) | 67 (45.3) | |||
| CC | 13 (24.1) | 15 (23.1) | 22 (23.4) | 25 (16.9) | |||
| Allele: C T | 57 (52.8) 51 (47.2) | 69 (53.1) 61 (46.9) | 0.963 | 98 (52.1) 90 (47.9) | 179 (60.5) 117 (39.5) | 0.070 | |
| Genotype | IL-10 Serum Level | p Value * | |
|---|---|---|---|
| MS Median (IQR) | Control Median (IQR) | ||
| rs1800871 | |||
| GG | 0.698 (1.445) | 0.817 (1.844) | 0.699 |
| GA + AA | 0.828 (1.703) | 0.756 (0.304) | 0.934 |
| rs1800872 | |||
| GG | 0.924 (1.366) | 0.817 (1.844) | 0.828 |
| GT + TT | 0.732 (2.245) | 0.756 (0.304) | 0.908 |
| rs1800896 | |||
| TT | 0.732 (1.410) | 0.756 (0.304) | 0.895 |
| TC+CC | 0.924 (1.525) | 0.817 (4.823) | 0.628 |
| SNPs | MS vs. Controls | ||
|---|---|---|---|
| D’ | r2 | p-Value | |
| rs1800871—rs1800872 | 0.9459 | 0.8813 | 0.0 |
| rs1800871—rs1800896 | 0.9434 | 0.2222 | 0.0 |
| rs1800872—rs1800896 | 0.9064 | 0.2080 | 0.0 |
| Haplotype | rs1800871 | rs1800872 | rs1800896 | Frequency (%) | OR (95% CI) | p-Value | ||
|---|---|---|---|---|---|---|---|---|
| MS | Controls | Total | ||||||
| 1 | G | G | C | 45.22 | 41.55 | 42.99 | 1.00 | --- |
| 2 | G | G | T | 30.06 | 32.86 | 31.79 | 0.85 (0.60–1.20) | 0.36 |
| 3 | A | T | T | 19.25 | 24.88 | 22.58 | 0.75 (0.50–1.11) | 0.15 |
| rare | * | * | * | NA | NA | 2.64 | 5.99 (1.68–21.34) | 0.006 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Masilionyte, U.; Gedvilaite, G.; Kaikaryte, K.; Vilkeviciute, A.; Kriauciuniene, L.; Glebauskiene, B.; Balnyte, R.; Liutkeviciene, R. IL-10 Gene Polymorphisms and IL-10 Serum Levels in Patients with Multiple Sclerosis in Lithuania. Brain Sci. 2022, 12, 800. https://doi.org/10.3390/brainsci12060800
Masilionyte U, Gedvilaite G, Kaikaryte K, Vilkeviciute A, Kriauciuniene L, Glebauskiene B, Balnyte R, Liutkeviciene R. IL-10 Gene Polymorphisms and IL-10 Serum Levels in Patients with Multiple Sclerosis in Lithuania. Brain Sciences. 2022; 12(6):800. https://doi.org/10.3390/brainsci12060800
Chicago/Turabian StyleMasilionyte, Ugne, Greta Gedvilaite, Kriste Kaikaryte, Alvita Vilkeviciute, Loresa Kriauciuniene, Brigita Glebauskiene, Renata Balnyte, and Rasa Liutkeviciene. 2022. "IL-10 Gene Polymorphisms and IL-10 Serum Levels in Patients with Multiple Sclerosis in Lithuania" Brain Sciences 12, no. 6: 800. https://doi.org/10.3390/brainsci12060800