
A Brief Introduction to Magnetoencephalography (MEG) and Its Clinical Applications

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Setting up the MEG Experiment
- (a)
- An empty room measurement is recommended for about 2 min before and after the actual experiment.
- (b)
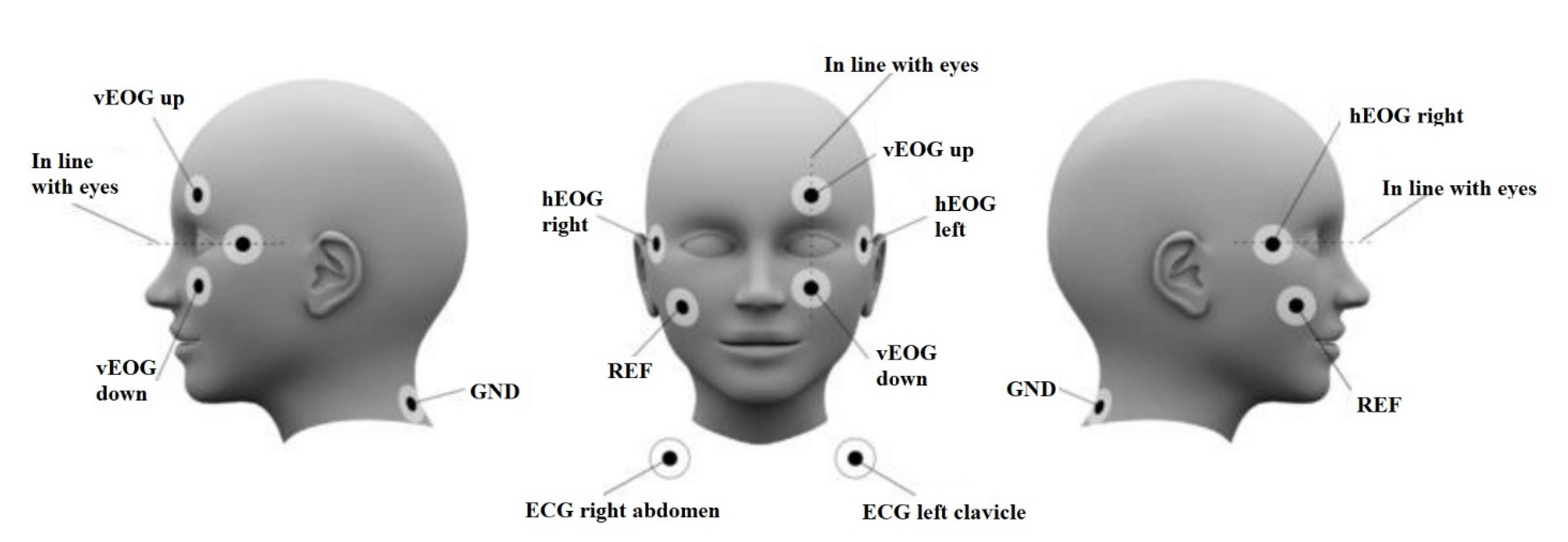
- Simultaneous ECG and EOG acquisition is advisable since it is used for artefact rejections and corrections during pre-processing the data.
- (c)
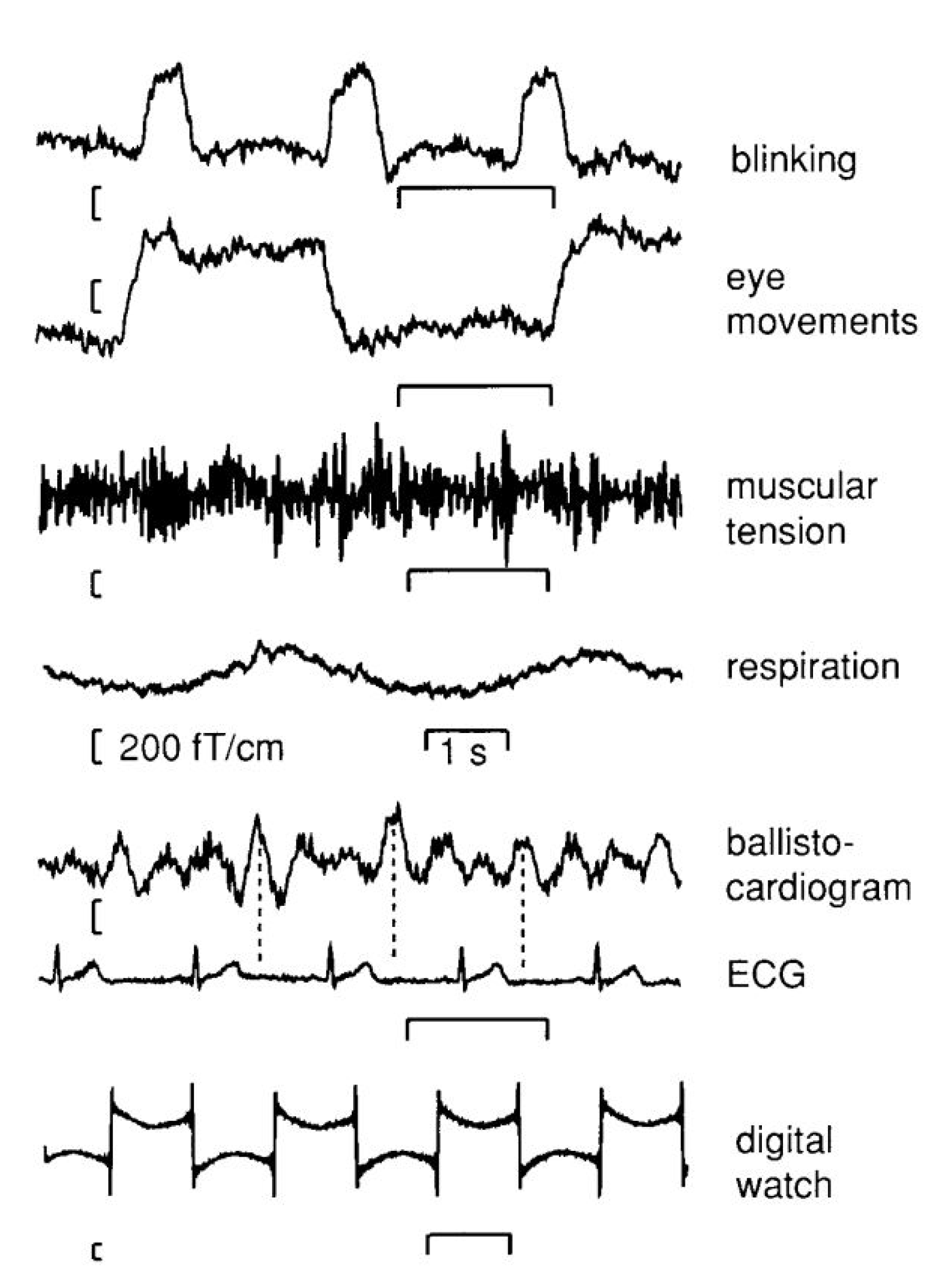
- For experiments involving muscle movements, a recording of muscle activity is advisable.
- (d)
- Suitable subject choice is a must following the exclusion criteria.
- (e)
- Position the participant as close as to the sensors.
- (f)
- Once the subject is positioned in the MEG system, it is recommended to perform 2 min of resting state measurement to ensure proper functioning of all the accessories.
- (g)
- 3D anatomical MRI is advisable if the protocol contains source localization process.
3. MEG Signal Processing and Source Localization
- (a)
- External magnetic field interference caused by sources like electric lines, traffic, and elevators.
- (b)
- System-related issues caused by defective sensors
- (c)
3.1. Signal Space Separation [SSS]
3.2. Software Tools Used in MEG Data Processing
4. Clinical Application
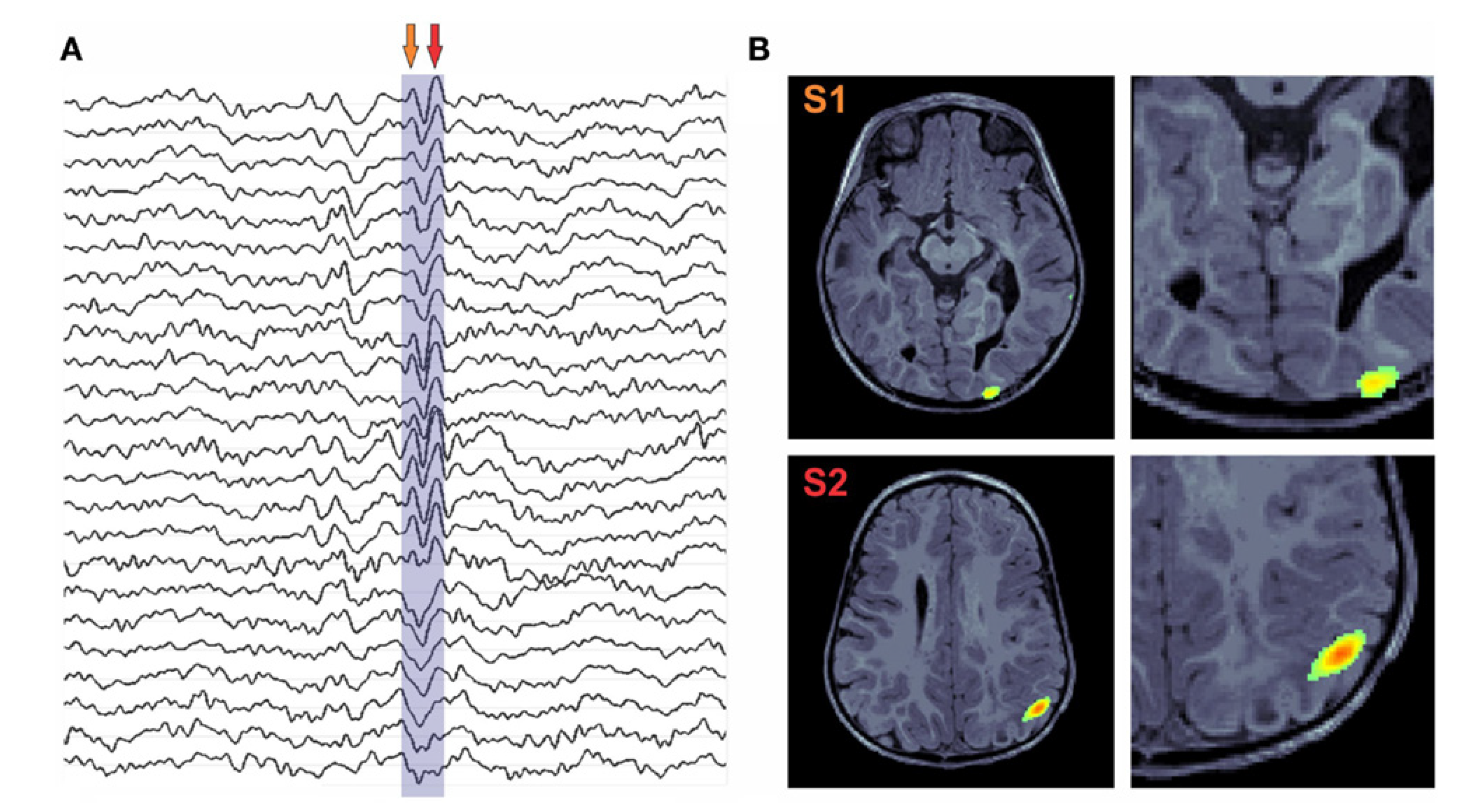
4.1. Epilepsy
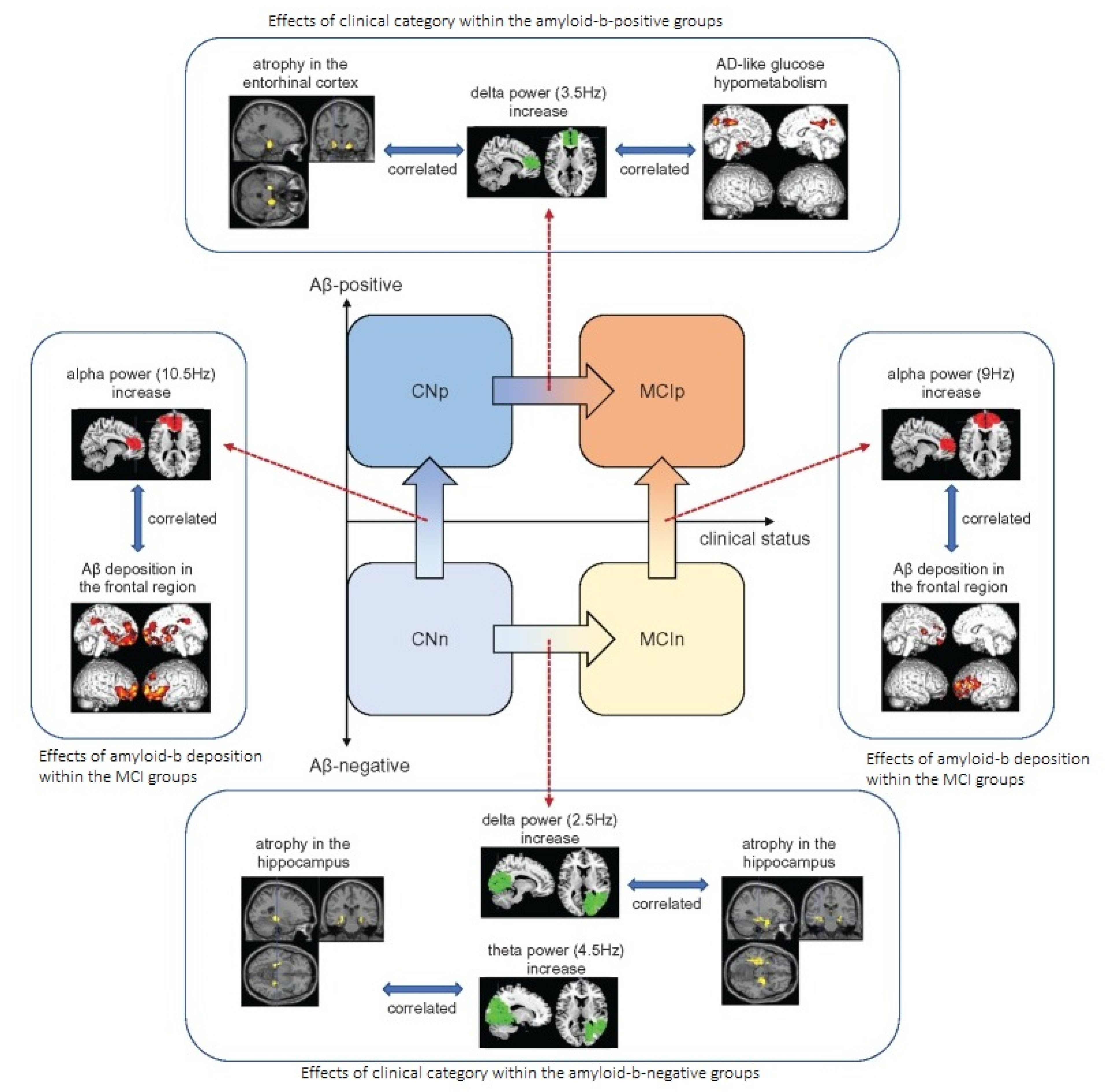
4.2. Alzheimer’s Disease (AD)
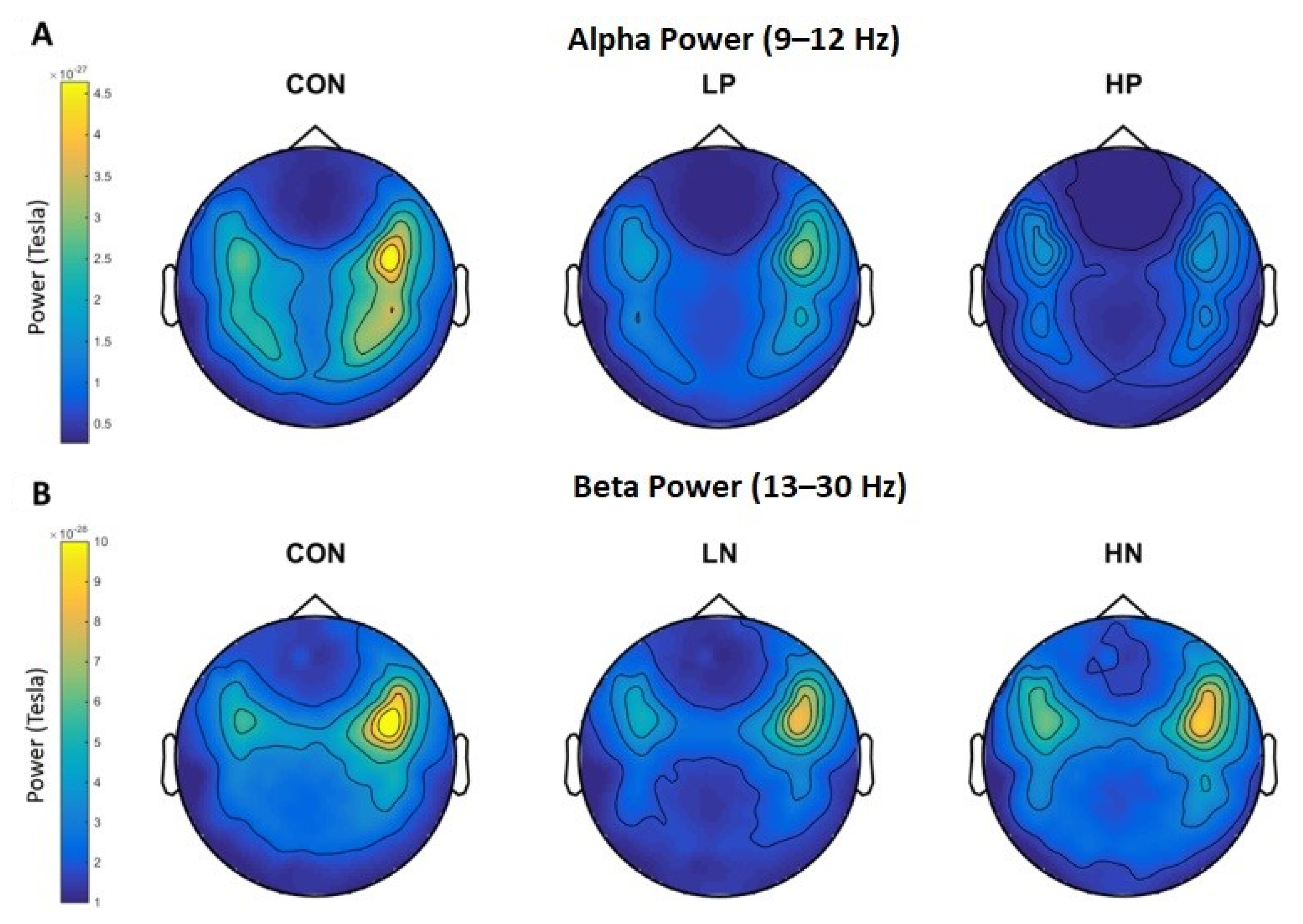
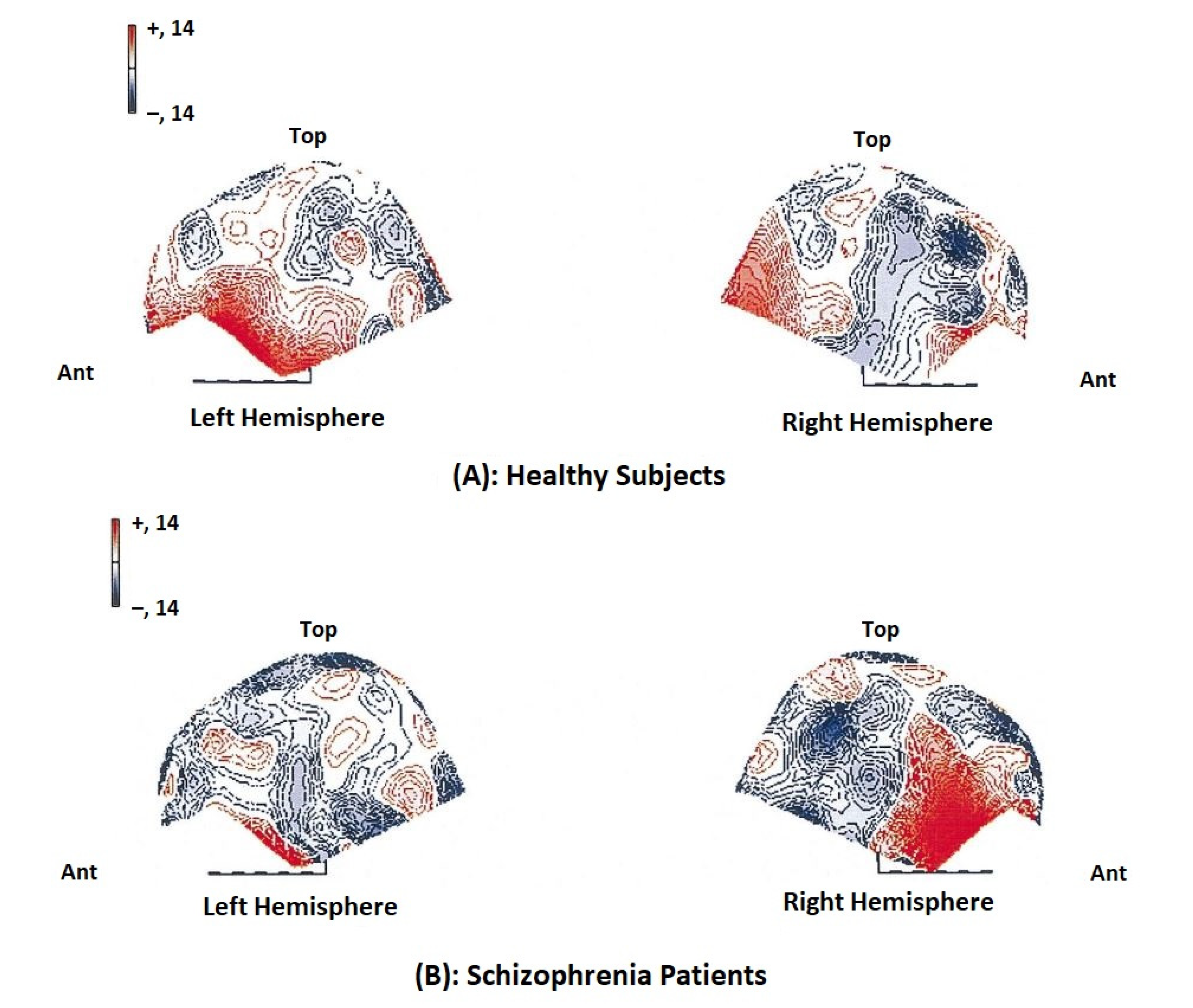
4.3. Schizophrenia
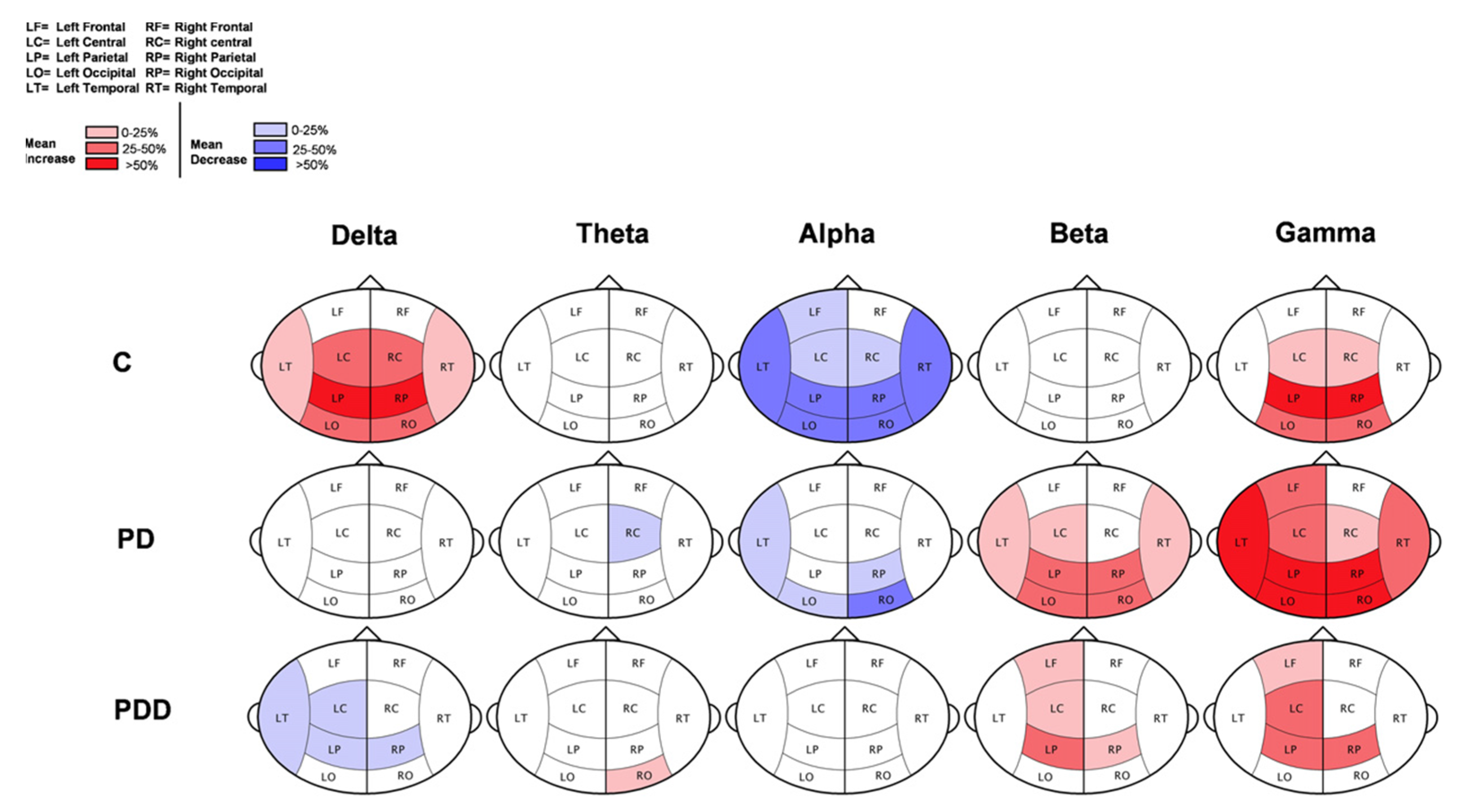
4.4. Parkinson Disease (PD)
4.5. Preoperative Evaluation
5. Inferences from the Narrative Study and Future Scope of MEG
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Feigin, V.L.; Nichols, E.; Alam, T.; Bannick, M.S.; Beghi, E.; Blake, N.; Culpepper, W.J.; Dorsey, E.R.; Elbaz, A.; Ellenbogen, R.G.; et al. Global, regional, and national burden of neurological disorders, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 459–480. [Google Scholar] [CrossRef] [Green Version]
- Kotov, S. MRI Morphometry of the Brain and Neurological Diseases. InNew Insights into Morphometry Studies; Pares-Casanova, P.M., Ed.; IntechOpen: London, UK, 2017. [Google Scholar] [CrossRef] [Green Version]
- Singh, S.P. Magnetoencephalography: Basic principles. Ann. Indian Acad. Neurol. 2014, 17, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Martins, N.R.B.; Angelica, A.; Chakravarthy, K.; Svidinenko, Y.; Boehm, F.J.; Opris, I.; Lebedev, M.A.; Swan, M.; Garan, S.A.; Rosenfeld, J.V.; et al. Human brain/cloud interface. In Advances in Clinical Immunology 2021, Medical Microbiology, COVID-19, and Big Data; Jenny Stanford Publishing: Dubai, United Arab Emirates, 2021; pp. 485–538. [Google Scholar]
- Hari, R.; Aina, P. MEG-EEG Primer; Oxford University Press: New York, NY, USA, 2017. [Google Scholar]
- Hämäläinen, M.; Hari, R.; Ilmoniemi, R.; Knuutila, J.; Lounasmaa, O.V. Magnetoencephalography—Theory, instrumentation, and applications to noninvasive studies of the working human brain. Rev. Mod. Phys. 1993, 65, 413–497. [Google Scholar] [CrossRef] [Green Version]
- Hari, R.; Riitta, S. Human cortical oscillations: A neuromagnetic view through the skull. Trends Neurosci. 1997, 20, 44–49. [Google Scholar] [CrossRef]
- Abhang, P.A.; Gawali, B.W.; Mehrotra, S.C. Technological Basics of EEG Recording and Operation of Apparatus. In Introduction to EEG- and Speech-Based Emotion Recognition; Elsevier: Amsterdam, The Netherlands, 2016; pp. 19–50. [Google Scholar]
- Cohen, D. Magnetoencephalography: Evidence of magnetic fields produced by alpha-rhythm currents. Science 1968, 161, 784–786. [Google Scholar] [CrossRef]
- Cohen, D. Magnetoencephalography: Detection of the brain’s electrical activity with a superconducting magnetometer. Science 1972, 175, 664–666. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, J.E.; Thiene, P.; Harding, J.T. Design and operation of stable rf-biased superconducting point-contact quantum devices, and a note on the properties of perfectly clean metal contacts. J. Appl. Phys. 1970, 41, 1572–1580. [Google Scholar] [CrossRef]
- Pataraia, E.; Baumgartner, C.; Lindinger, G.; Deecke, L. Magnetoencephalography in presurgical epilepsy evaluation. Neurosurg. Rev. 2002, 25, 141–159. [Google Scholar] [CrossRef]
- Paetau, R. Magnetoencephalography in pediatric neuroimaging. Dev. Sci. 2002, 5, 361–370. [Google Scholar] [CrossRef]
- Mäkelä, J.P.; Forss, N.; Jääskeläinen, J.; Kirveskari, E.; Korvenoja, A.; Paetau, R. Magnetoencephalography in Neurosurgery. Neurosurgery 2006, 59, 493–511. [Google Scholar] [CrossRef]
- McDonald, C.R. The use of neuroimaging to study behavior in patients with epilepsy. Epilepsy Behav. 2008, 12, 600–611. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, E.S.; Edgar, J.C.; Gaetz, W.C.; Roberts, T.P.L. Magnetoencephalography. Pediatr. Radiol. 2010, 40, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Bailey, A.J.; Braeutigam, S.; Jousmäki, V.; Swithenby, S.J. Abnormal activation of face processing systems at early and intermediate latency in individuals with autism spectrum disorder: A magnetoencephalographic study. Eur. J. Neurosci. 2005, 21, 2575–2585. [Google Scholar] [CrossRef] [PubMed]
- Kylliäinen, A.; Braeutigam, S.; Hietanen, J.K.; Swithenby, S.J.; Bailey, A.J. Face- and gaze-sensitive neural responses in children with autism: A magnetoencephalographic study. Eur. J. Neurosci. 2006, 24, 2679–2690. [Google Scholar] [CrossRef] [PubMed]
- Dima, D.; Frangou, S.; Burge, L.; Braeutingam, S.; James, A. Abnormal intrinsic and extrinsic connectivity within the magnetic mismatch negativity brain network in schizophrenia: A preliminary study. Schizophr. Res. 2012, 135, 23–27. [Google Scholar] [CrossRef]
- Laaksonen, K.; Helle, L.; Parkkonen, L.; Kirveskari, E.; Mäkelä, J.P.; Mustanoja, S.; Tatlisumak, T.; Kaste, M.; Forss, N. Alterations in Spontaneous Brain Oscillations during Stroke Recovery. PLoS ONE 2013, 8, e61146. [Google Scholar] [CrossRef] [PubMed]
- Lewine, J.D.; Davis, J.T.; Bigler, E.D.; Thoma, R.; Hill, D.; Funke, M.; Sloan, J.H.; Hall, S.L.; Orrison, W.W. Objective documentation of traumatic brain injury subsequent to mild head trauma: Multimodal brain imaging with MEG, SPECT, and MRI. J. Head Trauma Rehabil. 2007, 22, 141–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franzen, J.D.; Wilson, T.W. Amphetamines modulate prefrontal γ oscillations during attention processing. Neuroreport 2012, 23, 731–735. [Google Scholar] [CrossRef] [PubMed]
- Richard, A.E.; Lajiness-O’Neill, R.R.; Bowyer, S.M. Impaired prefrontal gamma band synchrony in autism spectrum disorders during gaze cueing. NeuroReport 2013, 24, 894–897. [Google Scholar] [CrossRef]
- Lajiness-O’Neill, R.; E Richard, A.E.; Moran, J.E.; Olszewski, A.; Pawluk, L.; Jacobson, D.; Mansour, A.; Vogt, K.; Erdodi, L.A.; Moore, A.M.; et al. Neural synchrony examined with magnetoencephalography (MEG) during eye gaze processing in autism spectrum disorders: Preliminary findings. J. Neurodev. Disord. 2014, 6, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brennan, J.R.; Wagley, N.; Kovelman, I.; Bowyer, S.M.; Richard, A.E.; Lajiness-O’Neill, R. MEG reveals atypical sensitivity to linguistic sound sequences in Autism Spectrum Disorder. Neuroreport 2016, 27, 982. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lajiness-O’Neill, R.; Brennan, J.R.; Moran, J.E.; Richard, A.E.; Flores, A.M.; Swick, C.; Goodcase, R.; Andersen, T.; McFarlane, K.; Rusiniak, K.; et al. Patterns of altered neural synchrony in the default mode network in autism spectrum disorder revealed with magnetoencephalography (MEG): Relationship to clinical symptomatology. Autism Res. 2017, 11, 434–449. [Google Scholar] [CrossRef] [PubMed]
- Nazem-Zadeh, M.R.; Bowyer, S.M.; Moran, J.E.; Davoodi-Bojd, E.; Zillgitt, A.; Bagher-Ebadian, H.; Mahmoudi, F.; Elisevich, K.V.; Soltanian-Zadeh, H. Application of DTI connectivity in lateralization of mTLE. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 5525–5528. [Google Scholar]
- Bowyer, S.M.; Zillgitt, A.; Greenwald, M.; Lajiness-O’Neill, R. Language mapping with magnetoencephalography: An update on the current state of clinical research and practice with considerations for clinical practice guidelines. J. Clin. Neurophysiol. 2020, 37, 554–563. [Google Scholar] [CrossRef] [PubMed]
- Neuromag, E.; Neuromag, E. Elekta Neuromag®. 2008. Available online: https://natmeg.se/onewebmedia/NM23083B-A%20Elekta%20Neuromag%20TRIUX%20datasheet.pdf (accessed on 25 April 2022).
- Pfeiffer, C. Preparation of the Participant. NatMEG 2017. Available online: https://natmeg.se/DriversLicense_material/prepare_subject_dec17.pdf (accessed on 25 April 2022).
- Pfeiffer, C.; Andersen, L.M.; Lundqvist, D.; Hamalainen, M.; Schneiderman, J.F.; Oostenveld, R. Localizing on-scalp MEG sensors using an array of magnetic dipole coils. PLoS ONE 2018, 13, e0191111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gross, J.; Baillet, S.; Barnes, G.; Henson, R.N.; Hillebrand, A.; Jensen, O.; Jerbi, K.; Litvak, V.; Maess, B.; Oostenveld, R.; et al. Good practice for conducting and reporting MEG research. NeuroImage 2012, 65, 349–363. [Google Scholar] [CrossRef] [PubMed]
- Niedermeyer, E.; da Silva, F.L. (Eds.) Electroencephalography: Basic Principles, Clinical Applications, and Related Fields, 5th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2005. [Google Scholar]
- Zimmerman, J.E. SQUID instruments and shielding for low-level magnetic measurements. J. Appl. Phys. 1977, 48, 702–710. [Google Scholar] [CrossRef]
- Uusitalo, M.A.; Ilmoniemi, R.J. Signal-space projection method for separating MEG or EEG into components. Med. Biol. Eng. Comput. 1997, 35, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Vrba, J. Multichannel SQUID Biomagnetic Systems Applications of Superconductivity Ed H Weinstock; Wolters Kluwer: Dordrecht, The Netherlands, 2000. [Google Scholar]
- Taulu, S.; Simola, J.; Kajola, M. Applications of the signal space separation method. IEEE Trans. Signal Process. 2005, 53, 3359–3372. [Google Scholar] [CrossRef] [Green Version]
- Taulu, S.; Simola, J. Spatiotemporal signal space separation method for rejecting nearby interference in MEG measurements. Phys. Med. Biol. 2006, 51, 1759. [Google Scholar] [CrossRef]
- Taulu, S.; Hari, R. Removal of magnetoencephalographic artifacts with temporal signal-space separation: Demonstration with single-trial auditory-evoked responses. Hum. Brain Mapp. 2009, 30, 1524–1534. [Google Scholar] [CrossRef] [PubMed]
- Tal, I.; Abeles, M. Cleaning MEG artifacts using external cues. J. Neurosci. Methods 2013, 217, 31–38. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez-Moreno, A.; Aurtenetxe, S.; Lopez-Garcia, M.E.; del Pozo, F.; Maestu, F.; Nevado, A. Signal-to-noise ratio of the MEG signal after preprocessing. J. Neurosci. Methods 2014, 222, 56–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puce, A.; Hämäläinen, M.S. A review of issues related to data acquisition and analysis in EEG/MEG studies. Brain Sci. 2017, 7, 58. [Google Scholar] [CrossRef] [PubMed]
- Zumer, J.M.; Wong, D.D.E.; Guggisberg, A.G.; Nagarajan, S.S.; Dalal, S.S. NUTMEG: Open Source Software for MEG/EEG Source Reconstruction. In Magnetoencephalography; Supek, S., Aine, C., Eds.; Springer: Berlin/Heidelberg, Germany, 2014; pp. 255–262. [Google Scholar] [CrossRef]
- Santosa, H.; Zhai, X.; Fishburn, F.; Huppert, T. The NIRS brain AnalyzIR toolbox. Algorithms 2018, 11, 73. [Google Scholar] [CrossRef] [Green Version]
- Oostenveld, R.; Fries, P.; Maris, E.; Schoffelen, J.-M. FieldTrip: Open source software for advanced analysis of MEG, EEG, and invasive electrophysiological data. Comput. Intell. Neurosci. 2011, 2011, 156869. [Google Scholar] [CrossRef] [PubMed]
- Aguera, P.-E.; Jerbi, K.; Caclin, A.; Bertrand, O. ELAN: A software package for analysis and visualization of MEG, EEG, and LFP signals. Comput. Intell. Neurosci. 2011, 2011, 158970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Litvak, V.; Mattout, J.; Kiebel, S.; Phillips, C.; Henson, R.; Kilner, J.; Barnes, G.; Oostenveld, R.; Daunizeau, J.; Flandin, G.; et al. EEG and MEG Data Analysis in SPM8. Comput. Intell. Neurosci. 2011, 2011, 852961. [Google Scholar] [CrossRef] [PubMed]
- Peyk, P.; de Cesarei, A.; Junghöfer, M. ElectroMagnetoEncephalography software: Overview and integration with other EEG/MEG toolboxes. Comput. Intell. Neurosci. 2011, 2011, 861705. [Google Scholar] [CrossRef]
- Tadel, F.; Baillet, S.; Mosher, J.C.; Pantazis, D.; Leahy, R.M. Brainstorm: A User-Friendly Application for MEG/EEG Analysis. Comput. Intell. Neurosci. 2011, 2011, 879716. [Google Scholar] [CrossRef]
- Mørup, M.; Hansen, L.K.; Arnfred, S.M. ERPWAVELAB: A toolbox for multi-channel analysis of time–frequency transformed event related potentials. J. Neurosci. Methods 2007, 161, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Baillet, S.; Tadel, F.; Leahy, R.M.; Mosher, J.C.; Delorme, A.; Makeig, S.; Oostenveld, R.; Hämäläinen, M.; Dalal, S.S.; Zumer, J.; et al. Academic software toolboxes for the analysis of MEG data. In Proceedings of the 17th International Conference on Biomagnetism Advances in Biomagnetism–Biomag 2010, Dubrovnik, Croatia, 28 March–1 April 2010; Springer: Berlin/Heidelberg, Germany, 2010; pp. 101–104. [Google Scholar]
- Gramfort, A.; Luessi, M.; Larson, E.; Engemann, D.A.; Strohmeier, D.; Brodbeck, C.; Goj, R.; Jas, M.; Brooks, T.; Parkkonen, L.; et al. MEG and EEG data analysis with MNE-Python. Front. Neurosci. 2013, 7, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Hughes, J.R.; Cohen, J.; Mayman, C.I.; Scholl, M.L.; Hendrix, D.E. Relationship of the magnetoencephalogram to abnormal activity in the electroencephalogram. J. Neurol. 1977, 217, 79–93. [Google Scholar] [CrossRef] [PubMed]
- Barth, D.S.; Sutherling, W.; Beatty, J. Fast and slow magnetic phenomena in focal epileptic seizures. Science 1984, 226, 855–857. [Google Scholar] [CrossRef] [PubMed]
- Modena, I.; Ricci, G.; Barbanera, S.; Leoni, R.; Romani, G.L.; Carelli, P. Biomagnetic measurements of spontaneous brain activity in epileptic patients. Electroencephalogr. Clin. Neurophysiol. 1982, 54, 622–628. [Google Scholar] [CrossRef]
- Gallen, C.C.; Sobel, D.F.; Waltz, T.; Aung, M.; Copeland, B.; Schwartz, B.J.; Hirschkoff, E.C.; Bloom, F.E. Noninvasive presurgical neuromagnetic mapping of somatosensory cortex. Neurosurgery 1993, 33, 260–268. [Google Scholar] [CrossRef]
- Al-Khuzaie, F.E.K.; Bayat, O.; Duru, A.D. Diagnosis of Alzheimer disease using 2D MRI slices by convolutional neural network. Appl. Bionics Biomech. 2021, 2021, 6690539. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.; Oh, B.-L.; Lee, K.-U.; Chae, J.H.; Yun, K. Identifying schizophrenia using structural MRI with a deep learning algorithm. Front. Psychiatry 2020, 11, 16. [Google Scholar] [CrossRef] [PubMed]
- Anudeep, P.; Mourya, P.; Anandhi, T. Parkinson’s Disease Detection Using Machine Learning Techniques. In Advances in Electronics 2021, Communication and Computing; Springer: Singapore, 2021; pp. 483–493. [Google Scholar]
- Wilson, S.; Harner, R.; Duffy, F.; Tharp, B.; Nuwer, M.; Sperling, M. Spike detection. I. Correlation and reliability of human experts. Electroencephalogr. Clin. Neurophysiol. 1996, 98, 186–198. [Google Scholar] [CrossRef]
- El-Samie, F.E.A.; Alotaiby, T.N.; Khalid, M.I.; Alshebeili, S.A.; Aldosari, S.A. A Review of EEG and MEG Epileptic Spike Detection Algorithms. IEEE Access 2018, 6, 60673–60688. [Google Scholar] [CrossRef]
- Anderson, C.T.; Carlson, C.E.; Li, Z.; Raghavan, M. Magnetoencephalography in the preoperative evaluation for epilepsy surgery. Curr. Neurol. Neurosci. Rep. 2014, 14, 446. [Google Scholar] [CrossRef]
- Khalid, M.I.; Aldosari, S.A.; Alshebeili, S.A.; Alotaiby, T.; Al-Hameed, M.H.; Jad, L. MEG data classification for healthy and epileptic subjects using linear discriminant analysis. In Proceedings of the 2015 IEEE International Symposium on Signal Processing and Information Technology (ISSPIT), Abu Dhabi, United Arab Emirates, 7–10 December 2015; pp. 360–363. [Google Scholar]
- Migliorelli, C.; Alonso, J.F.; Romero, S.; Nowak, R.; Russi, A.; Mañanas, M.A. Automated detection of epileptic ripples in MEG using beamformer-based virtual sensors. J. Neural Eng. 2017, 14, 046013. [Google Scholar] [CrossRef] [PubMed]
- Knowlton, R.C. The role of FDG-PET, ictal SPECT, and MEG in the epilepsy surgery evaluation. Epilepsy Behav. 2006, 8, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Alotaiby, T.N.; Alrshoud, S.R.; Alshebeili, S.A.; Alhumaid, M.H.; Alsabhan, W.M. Epileptic MEG Spike Detection Using Statistical Features and Genetic Programming with KNN. J. Health Eng. 2017, 2017, 3035606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ge, S.; Wu, T.; Tang, H.Y.; Xiao, X.; Iramina, K.; Wu, W. Coherence analysis for epilepsy patients: An MEG study. World Acad. Sci. Eng. Technol. 2011, 80, 517–519. [Google Scholar]
- Antoniou, P.E.; Adamopoulos, A.; Anninos, P.A.; Piperidou, H.; Kotini, A. Assessing Brain Pathophysiology through Non-Linear Analysis of MEG in Ιdiopathic Generalized Epilepsy Cases. J. Behav. Brain Sci. 2012, 2, 445–453. [Google Scholar] [CrossRef] [Green Version]
- Knowlton, R.C.; Shih, J. Magnetoencephalography in epilepsy. Epilepsia 2004, 45, 61–71. [Google Scholar] [CrossRef]
- Ochi, A.; Otsubo, H. Magnetoencephalography-guided epilepsy surgery for children with intractable focal epilepsy: SickKids experience. Int. J. Psychophysiol. 2008, 68, 104–110. [Google Scholar] [CrossRef]
- Vivekananda, U.; Mellor, S.; Tierney, T.M.; Holmes, N.; Boto, E.; Leggett, J.; Roberts, G.; Hill, R.M.; Litvak, V.; Brookes, M.J.; et al. Optically pumped magnetoencephalography in epilepsy. Ann. Clin. Transl. Neurol. 2020, 7, 397–401. [Google Scholar] [CrossRef] [Green Version]
- Khan, S.; Lefèvre, J.; Baillet, S.; Michmizos, K.P.; Ganesan, S.; Kitzbichler, M.G.; Zetino, M.; Hämäläinen, M.S.; Papadelis, C.; Kenet, T. Encoding cortical dynamics in sparse features. Front. Hum. Neurosci. 2014, 8, 338. [Google Scholar] [CrossRef] [Green Version]
- Villemagne, V.L.; Burnham, S.; Bourgeat, P.; Brown, B.; Ellis, K.A.; Salvado, O.; Szoeke, C.; Macaulay, S.L.; Martins, R.; Maruff, P.; et al. Amyloid β deposition, neurodegeneration, and cognitive decline in sporadic Alzheimer’s disease: A prospective cohort study. Lancet Neurol. 2013, 12, 357–367. [Google Scholar] [CrossRef]
- Morris, J.C. Early-stage and preclinical Alzheimer disease. Alzheimer Dis. Assoc. Disord. 2005, 19, 163–165. [Google Scholar] [PubMed]
- Bateman, R.J.; Xiong, C.; Benzinger, T.L.S.; Fagan, A.M.; Goate, A.; Fox, N.C.; Marcus, D.S.; Cairns, N.J.; Xie, X.; Blazey, T.M.; et al. Clinical and Biomarker Changes in Dominantly Inherited Alzheimer’s Disease. N. Engl. J. Med. 2012, 367, 795–804. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamura, A.; Cuesta, P.; Fernández, A.; Arahata, Y.; Iwata, K.; Kuratsubo, I.; Bundo, M.; Hattori, H.; Sakurai, T.; Fukuda, K.; et al. Electromagnetic signatures of the preclinical and prodromal stages of Alzheimer’s disease. Brain 2018, 141, 1470–1485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández, A.; Hornero, R.; Mayo-Iscar, A.; Poza, J.; Gil-Gregorio, P.; Ortiz, T. MEG spectral profile in Alzheimer’s disease and mild cognitive impairment. Clin. Neurophysiol. 2006, 117, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Gómez, C.; Hornero, R.; Abásolo, D.; Fernández, A.; Escudero, J. Analysis of MEG background activity in Alzheimer’s disease using nonlinear methods and ANFIS. Ann. Biomed. Eng. 2009, 37, 586–594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hatsusaka, N.; Higuchi, M.; Kado, H. Possibility of MEG as an Early Diagnosis Tool for Alzheimer’s Disease: A Study of Event Related Field in Missing Stimulus Paradigm. In Proceedings of the 13th International Conference on Biomedical Engineering, Singapore, 3–6 December 2008; Springer: Berlin/Heidelberg, Germany, 2009; pp. 9–12. [Google Scholar]
- Ashford, J.W.; Salehi, A.; Furst, A.; Bayley, P.; Frisoni, G.B.; Jack, C.R., Jr.; Sabri, O.; Adamson, M.M.; Coburn, K.L.; Olichney, J.; et al. Imaging the Alzheimer brain. J. Alzheimer Dis. 2011, 26, 1–27. [Google Scholar] [CrossRef] [Green Version]
- Alonso, J.F.; Poza, J.; Mañanas, M.; Romero, S.; Fernández, A.; Hornero, R. MEG Connectivity Analysis in Patients with Alzheimer’s Disease Using Cross Mutual Information and Spectral Coherence. Ann. Biomed. Eng. 2010, 39, 524–536. [Google Scholar] [CrossRef]
- Bruña, R.; Poza, J.; Gómez, C.; García, M.; Fernández, A.; Hornero, R. Analysis of spontaneous MEG activity in mild cognitive impairment and Alzheimer’s disease using spectral entropies and statistical complexity measures. J. Neural Eng. 2012, 9, 036007. [Google Scholar] [CrossRef] [Green Version]
- Fernández, A.; Turrero, A.; Zuluaga, P.; Gil-Gregorio, P.; del Pozo, F.; Maestu, F.; Moratti, S. MEG Delta Mapping Along the Healthy Aging-Alzheimer’s Disease Continuum: Diagnostic Implications. J. Alzheimer Dis. 2013, 35, 495–507. [Google Scholar] [CrossRef]
- McClay, W.A.; Yadav, N.; Ozbek, Y.; Haas, A.; Attias, H.T.; Nagarajan, S.S. A Real-Time Magnetoencephalography Brain-Computer Interface Using Interactive 3D Visualization and the Hadoop Ecosystem. Brain Sci. 2015, 5, 419–440. [Google Scholar] [CrossRef] [Green Version]
- Guillon, J.; Attal, Y.; Colliot, O.; La Corte, V.; Dubois, B.; Schwartz, D.; Chavez, M.; Fallani, F.D.V. Loss of brain inter-frequency hubs in Alzheimer’s disease. Sci. Rep. 2017, 7, 10879. [Google Scholar] [CrossRef] [PubMed]
- Maestu, F.; Fernandez, A.; Simos, P.G.; Lopez-Ibor, M.I.; Campo, P.; Criado, J.; Rodriguez-Palancas, A.; Ferre, F.; Amo, C.; Ortiz, T. Profiles of brain magnetic activity during a memory task in patients with Alzheimer’s disease and in non-demented elderly subjects, with or without depression. J. Neurol. Neurosurg. Psychiatry 2004, 75, 1160–1162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uhlhaas, P.J.; Singer, W. Abnormal neural oscillations and synchrony in schizophrenia. Nat. Rev. Neurosci. 2010, 11, 100–113. [Google Scholar] [CrossRef] [PubMed]
- Boutros, N.N.; Arfken, C.; Galderisi, S.; Warrick, J.; Pratt, G.; Iacono, W. The status of spectral EEG abnormality as a diagnostic test for schizophrenia. Schizophr. Res. 2008, 99, 225–237. [Google Scholar] [CrossRef] [Green Version]
- Hinkley, L.B.; Vinogradov, S.; Guggisberg, A.G.; Fisher, M.; Findlay, A.M.; Nagarajan, S.S. Clinical Symptoms and Alpha Band Resting-State Functional Connectivity Imaging in Patients With Schizophrenia: Implications for Novel Approaches to Treatment. Biol. Psychiatry 2011, 70, 1134–1142. [Google Scholar] [CrossRef] [Green Version]
- Ikezawa, K.; Ishii, R.; Iwase, M.; Kurimoto, R.; Canuet, L.; Takahashi, H.; Nakahachi, T.; Azechi, M.; Ohi, K.; Fukumoto, M.; et al. Decreased alpha event-related synchronization in the left posterior temporal cortex in schizophrenia: A magnetoencephalography-beamformer study. Neurosci. Res. 2011, 71, 235–243. [Google Scholar] [CrossRef]
- Zeev-Wolf, M.; Levy, J.; Jahshan, C.; Peled, A.; Levkovitz, Y.; Grinshpoon, A.; Goldstein, A. MEG resting-state oscillations and their relationship to clinical symptoms in schizophrenia. NeuroImage Clin. 2018, 20, 753–761. [Google Scholar] [CrossRef]
- Kissler, J.; Müller, M.M.; Fehr, T.; Rockstroh, B.; Elbert, T. MEG gamma band activity in schizophrenia patients and healthy subjects in a mental arithmetic task and at rest. Clin. Neurophysiol. 2000, 111, 2079–2087. [Google Scholar] [CrossRef] [Green Version]
- Fehr, T.; Kissler, J.; Moratti, S.; Wienbruch, C.; Rockstroh, B.; Elbert, T. Source distribution of neuromagnetic slow waves and MEG-delta activity in schizophrenic patients. Biol. Psychiatry 2001, 50, 108–116. [Google Scholar] [CrossRef] [Green Version]
- Sperling, W.; Martus, P.; Kober, H.; Bleich, S.; Kornhuber, J. Spontaneous, slow and fast magnetoencephalographic activity in patients with schizophrenia. Schizophr. Res. 2002, 58, 189–199. [Google Scholar] [CrossRef]
- Kircher, T.T.; Rapp, A.M.; Grodd, W.; Buchkremer, G.; Weiskopf, N.; Lutzenberger, W.; Ackermann, H.; Mathiak, K. Mismatch Negativity Responses in Schizophrenia: A Combined fMRI and Whole-Head MEG Study. Am. J. Psychiatry 2004, 161, 294–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koh, Y.; Shin, K.S.; Kim, J.S.; Choi, J.-S.; Kang, D.-H.; Jang, J.H.; Cho, K.-H.; O’Donnell, B.F.; Chung, C.K.; Kwon, J.S. An MEG study of alpha modulation in patients with schizophrenia and in subjects at high risk of developing psychosis. Schizophr. Res. 2011, 126, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Fernández, A.; López-Ibor, M.-I.; Turrero, A.; Santos, J.-M.; Morón, M.-D.; Hornero, R.; Gómez, C.; Méndez, M.A.; Ortiz, T.; López-Ibor, J.J. Lempel–Ziv complexity in schizophrenia: A MEG study. Clin. Neurophysiol. 2011, 122, 2227–2235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowyer, S.M.; Gjini, K.; Zhu, X.; Kim, L.; Moran, J.E.; Rizvi, S.U.; Gumenyuk, V.; Tepley, N.; Boutros, N.N. Potential Biomarkers of Schizophrenia from MEG Resting-State Functional Connectivity Networks: Preliminary Data. J. Behav. Brain Sci. 2015, 5, 52984. [Google Scholar] [CrossRef] [Green Version]
- Neustadter, E.; Mathiak, K.; Turetsky, B.I. EEG and MEG probes of schizophrenia pathophysiology. In The Neurobiology of Schizophrenia; Academic Press: Cambridge, MA, USA, 2016; pp. 213–236. [Google Scholar]
- Cetin, M.S.; Houck, J.M.; Rashid, B.; Agacoglu, O.; Stephen, J.M.; Sui, J.; Canive, J.; Mayer, A.; Aine, C.; Bustillo, J.R.; et al. Multimodal Classification of Schizophrenia Patients with MEG and fMRI Data Using Static and Dynamic Connectivity Measures. Front. Neurosci. 2016, 10, 466. [Google Scholar] [CrossRef] [Green Version]
- Anninos, P.; Chatzimichael, A.; Adamopoulos, A.; Kotini, A.; Tsagas, N. A combined study of MEG and pico-Tesla TMS on children with autism disorder. J. Integr. Neurosci. 2016, 15, 497–513. [Google Scholar] [CrossRef]
- Manzano, J.M.; Munoz, J.J.; Santos, J.M.; Serra, A.; Alonso, T.O.; de Erausquin, G. MEG resting-state differences as a marker of clinical subtype in schizophrenia. Neuropsychiatry 2017, 7. [Google Scholar] [CrossRef]
- Grent-‘T-Jong, T.; Rivolta, D.; Sauer, A.; Grube, M.; Singer, W.; Wibral, M.; Uhlhaas, P.J. MEG-measured visually induced gamma-band oscillations in chronic schizophrenia: Evidence for impaired generation of rhythmic activity in ventral stream regions. Schizophr. Res. 2016, 176, 177–185. [Google Scholar] [CrossRef] [Green Version]
- Braak, H.; del Tredici, K.; Rüb, U.; De Vos, R.A.; Steur, E.N.J.; Braak, E. Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol. Aging 2003, 24, 197–211. [Google Scholar] [CrossRef]
- Baillet, S. Magnetoencephalography for brain electrophysiology and imaging. Nat. Neurosci. 2017, 20, 327–339. [Google Scholar] [CrossRef]
- Llinás, R.R.; Ribary, U.; Jeanmonod, D.; Kronberg, E.; Mitra, P.P. Thalamocortical dysrhythmia: A neurological and neuropsychiatric syndrome characterized by magnetoencephalography. Proc. Natl. Acad. Sci. USA 1999, 96, 15222–15227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosboom, J.; Stoffers, D.; Stam, C.; van Dijk, B.; Verbunt, J.; Berendse, H.; Wolters, E. Resting state oscillatory brain dynamics in Parkinson’s disease: An MEG study. Clin. Neurophysiol. 2006, 117, 2521–2531. [Google Scholar] [CrossRef] [PubMed]
- Stam, C.J. Use of magnetoencephalography (MEG) to study functional brain networks in neurodegenerative disorders. J. Neurol. Sci. 2010, 289, 128–134. [Google Scholar] [CrossRef] [PubMed]
- Stoffers, D.; Bosboom, J.; Deijen, J.; Wolters, E.; Stam, C.; Berendse, H. Increased cortico-cortical functional connectivity in early-stage Parkinson’s disease: An MEG study. NeuroImage 2008, 41, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Song, T.; Cui, L.; Gaa, K.; Feffer, L.; Taulu, S.; Lee, R.R.; Huang, M. Signal Space Separation Algorithm and Its Application on Suppressing Artifacts Caused by Vagus Nerve Stimulation for Magnetoencephalography Recordings. J. Clin. Neurophysiol. 2009, 26, 392–400. [Google Scholar] [CrossRef]
- Schoffelen, J.; Gross, J. Source connectivity analysis with MEG and EEG. Hum. Brain Mapp. 2009, 30, 1857–1865. [Google Scholar] [CrossRef]
- Kirchberger, K.; Hummel, C.; Stefan, H. Postoperative multichannel magnetoencephalography in patients with recurrent seizures after epilepsy surgery. Acta Neurol. Scand. 1998, 98, 1–7. [Google Scholar] [CrossRef]
- Stam, C.J.; Jones, B.F.; Manshanden, I.; van Walsum, A.M.V.C.; Montez, T.; Verbunt, J.P.A.; de Munck, J.C.; van Dijk, B.W.; Berendse, H.W.; Scheltens, P. Magnetoencephalographic evaluation of resting-state functional connectivity in Alzheimer’s disease. NeuroImage 2006, 32, 1335–1344. [Google Scholar] [CrossRef]
- Osipova, D.; Rantanen, K.; Ahveninen, J.; Ylikoski, R.; Häppölä, O.; Strandberg, T.; Pekkonen, E. Source estimation of spontaneous MEG oscillations in mild cognitive impairment. Neurosci. Lett. 2006, 405, 57–61. [Google Scholar] [CrossRef]
- Fernández, A.; Maestú, F.; Amo, C.; Gil, P.; Fehr, T.; Wienbruch, C.; Rockstroh, B.; Elbert, T.; Ortiz, T. Focal temporoparietal slow activity in Alzheimer’s disease revealed by magnetoencephalography. Biol. Psychiatry 2002, 52, 764–770. [Google Scholar] [CrossRef] [Green Version]
- Edgar, J.C.; Guha, A.; Miller, G.A. Magnetoencephalography for Schizophrenia. Neuroimaging Clin. 2020, 30, 205–216. [Google Scholar] [CrossRef] [PubMed]
- Hinkley, L.B.; Owen, J.P.; Fisher, M.; Findlay, A.M.; Vinogradov, S.; Nagarajan, S.S. Cognitive impairments in schizophrenia as assessed through activation and connectivity measures of magnetoencephalography (MEG) data. Front. Hum. Neurosci. 2010, 3, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, H.-M.; Hsiao, F.-J.; Chen, R.-S.; Shan, D.E.; Hsu, W.Y.; Chiang, M.C.; Lin, Y.Y. Attenuated NoGo-related beta desynchronisation and synchronisation in Parkinson’s disease revealed by magnetoencephalographic recording. Sci. Rep. 2019, 9, 7235. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Yanagisawa, T.; Fukuma, R.; Tani, N.; Oshino, S.; Mihara, M.; Hattori, N.; Kajiyama, Y.; Hashimoto, R.; Ikeda, M.; et al. Magnetoencephalography detects phase-amplitude coupling in Parkinson’s disease. Sci. Rep. 2022, 12, 1835. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sl. No. | Toolbox | Features | Availability |
| 1 | NUTMEG [43] |
| open-source MATLAB-based toolbox |
| 2 | NIRS Brain AnalyzIR Toolbox [44] |
| open-source MATLAB-based analysis |
| 3 | Field Trip [45] |
| open-source MATLAB-toolbox |
| 4 | ELAN [46] |
| Licenced version C implementation |
| 5 | SPM8 [47] |
| MATLAB-toolbox |
| 6 | Electro Magneto Encephalography Software [48] |
| MATLAB supported toolbox |
| 7 | Brainstorm [49] |
| Cross platform software supports MATLAB, Python and Java scripts |
| 8 | ERP WAVELAB [50] |
| open-source MATLAB-based analysis |
| 9 | MNE python toolbox [52]. |
| Open-source python package, Also avilable in MATLAB and C with limited modules. |
| Neurodisorders | MEG Findings and Clinical Considerations |
|---|---|
| Epilepsy | Accurate localization of spikes when compared with the EEG for both ictal and interictal subjects. It can localize the complex primary intrasylvian epileptiform disturbances associated with Landau–Kleffner syndrome, which aids the presurgical scenario [69]. MEG was found to be robust in the localization of postsurgical epileptiform disturbances [112] |
| Alzheimer’s Disease (AD) | Proficient in the early detection of dementia [113]. Increase in count of dipoles in the delta and theta band [114]. Slow wave activity detection in the right temporal and parietal lobe of the brain [115]. |
| Schizophrenia | Resting-state activity was acquired spontaneously with 5 min duration in the awake state, resting state MEG are able to distinguish different subtypes of schizophrenia [116]. Auditory studies are also done with various stimuli for the distinguishing subtypes of schizophrenia [117]. MEG along with coherence source imaging (CSI) efficiently detects the brain oscillation that distinguishes between normal and schizophrenia subjects [2]. |
| Parkinson Disease (PD) | Changes in beta band were observed in MEG data, PD patients had a significant minimization in beta ERD during the NoGo condition and in beta ERS during both Go and NoGo conditions compared with the healthy subjects [118]. Beta gamma phase magnitude coupling was observed in the resting state [119]. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fred, A.L.; Kumar, S.N.; Kumar Haridhas, A.; Ghosh, S.; Purushothaman Bhuvana, H.; Sim, W.K.J.; Vimalan, V.; Givo, F.A.S.; Jousmäki, V.; Padmanabhan, P.; et al. A Brief Introduction to Magnetoencephalography (MEG) and Its Clinical Applications. Brain Sci. 2022, 12, 788. https://doi.org/10.3390/brainsci12060788
Fred AL, Kumar SN, Kumar Haridhas A, Ghosh S, Purushothaman Bhuvana H, Sim WKJ, Vimalan V, Givo FAS, Jousmäki V, Padmanabhan P, et al. A Brief Introduction to Magnetoencephalography (MEG) and Its Clinical Applications. Brain Sciences. 2022; 12(6):788. https://doi.org/10.3390/brainsci12060788
Chicago/Turabian StyleFred, Alfred Lenin, Subbiahpillai Neelakantapillai Kumar, Ajay Kumar Haridhas, Sayantan Ghosh, Harishita Purushothaman Bhuvana, Wei Khang Jeremy Sim, Vijayaragavan Vimalan, Fredin Arun Sedly Givo, Veikko Jousmäki, Parasuraman Padmanabhan, and et al. 2022. "A Brief Introduction to Magnetoencephalography (MEG) and Its Clinical Applications" Brain Sciences 12, no. 6: 788. https://doi.org/10.3390/brainsci12060788