
Stance Phase Gait Training Post Stroke Using Simultaneous Transcranial Direct Current Stimulation and Motor Learning-Based Virtual Reality-Assisted Therapy: Protocol Development and Initial Testing

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. System Users
2.2. Development of the New Combined Stance Phase Training Protocol
2.2.1. Transcranial Direct Current Stimulation (tDCS)
2.2.2. Virtual Reality (VR) Technology
2.2.3. VR system Components: Treadmill and Harness Safety System
2.3. Construction of the Treatment Protocol of Combined tDCS, VR, Treadmill, Harness System, and Overground Gait Training
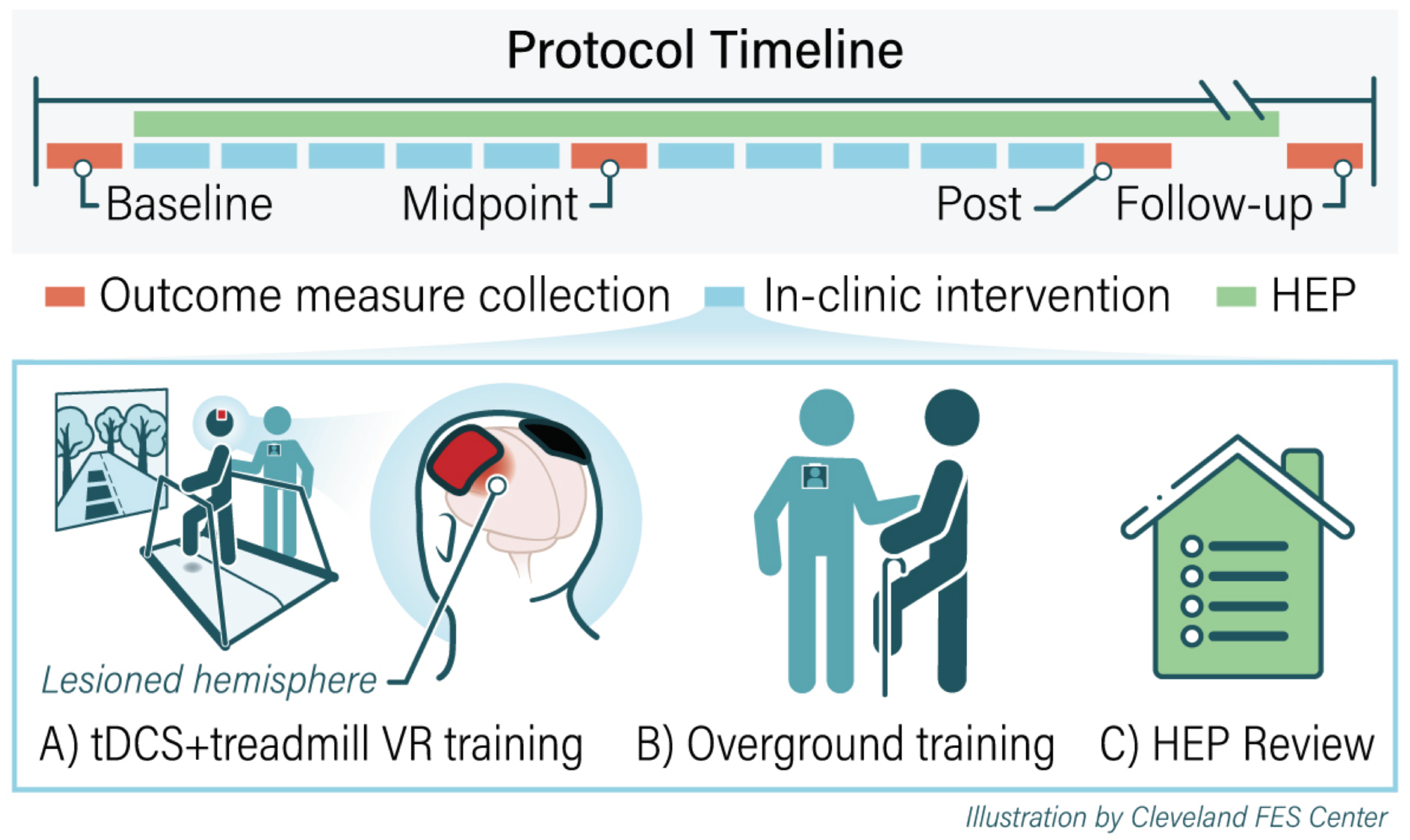
2.3.1. Summary of Treatment Protocol
2.3.2. tDCS Electrical Field Modelling
2.3.3. VR, Treadmill, and Harness SAFETY system
2.3.4. Overground Gait Training
2.3.5. Home Exercise Program
2.4. Outcome Measures
2.4.1. Feasibility
2.4.2. User Performance Measures
2.5. Statistical Analysis
3. Results
3.1. System User Baseline Characteristics
3.2. The Protocol Feasibility
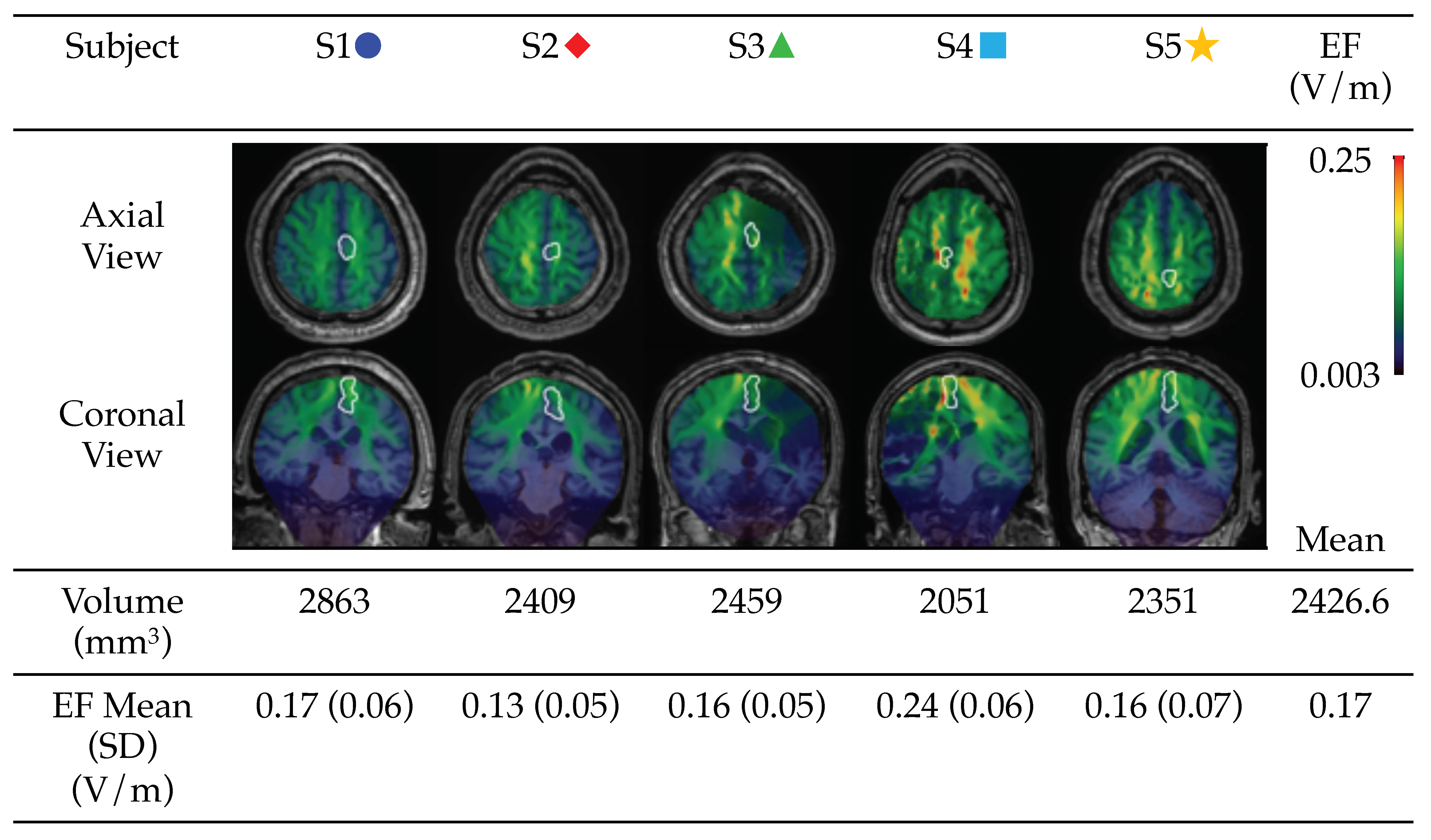
3.3. Modelling of tDCS-Induced Electric Field
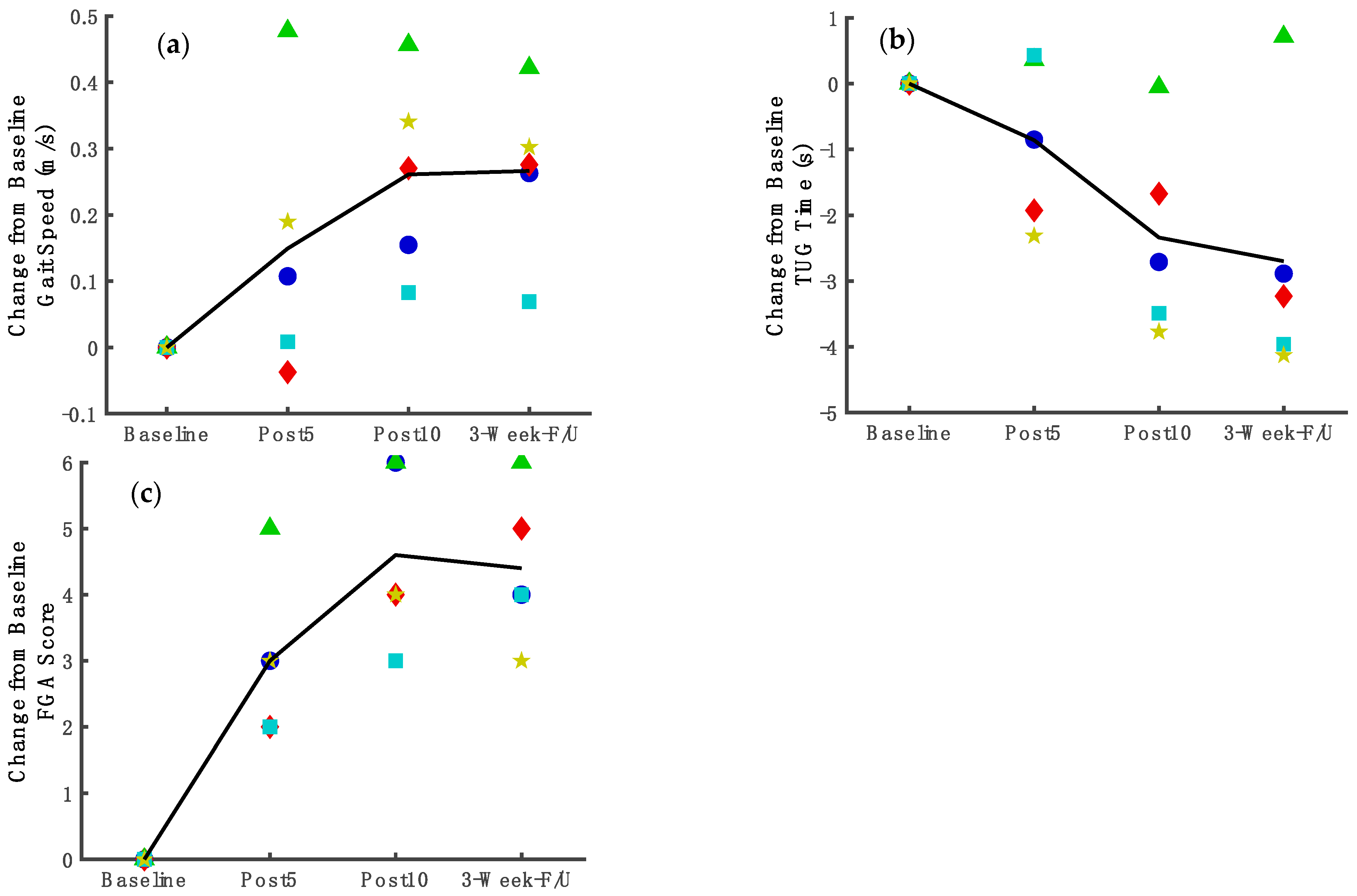
3.4. Functional Mobility Improvement
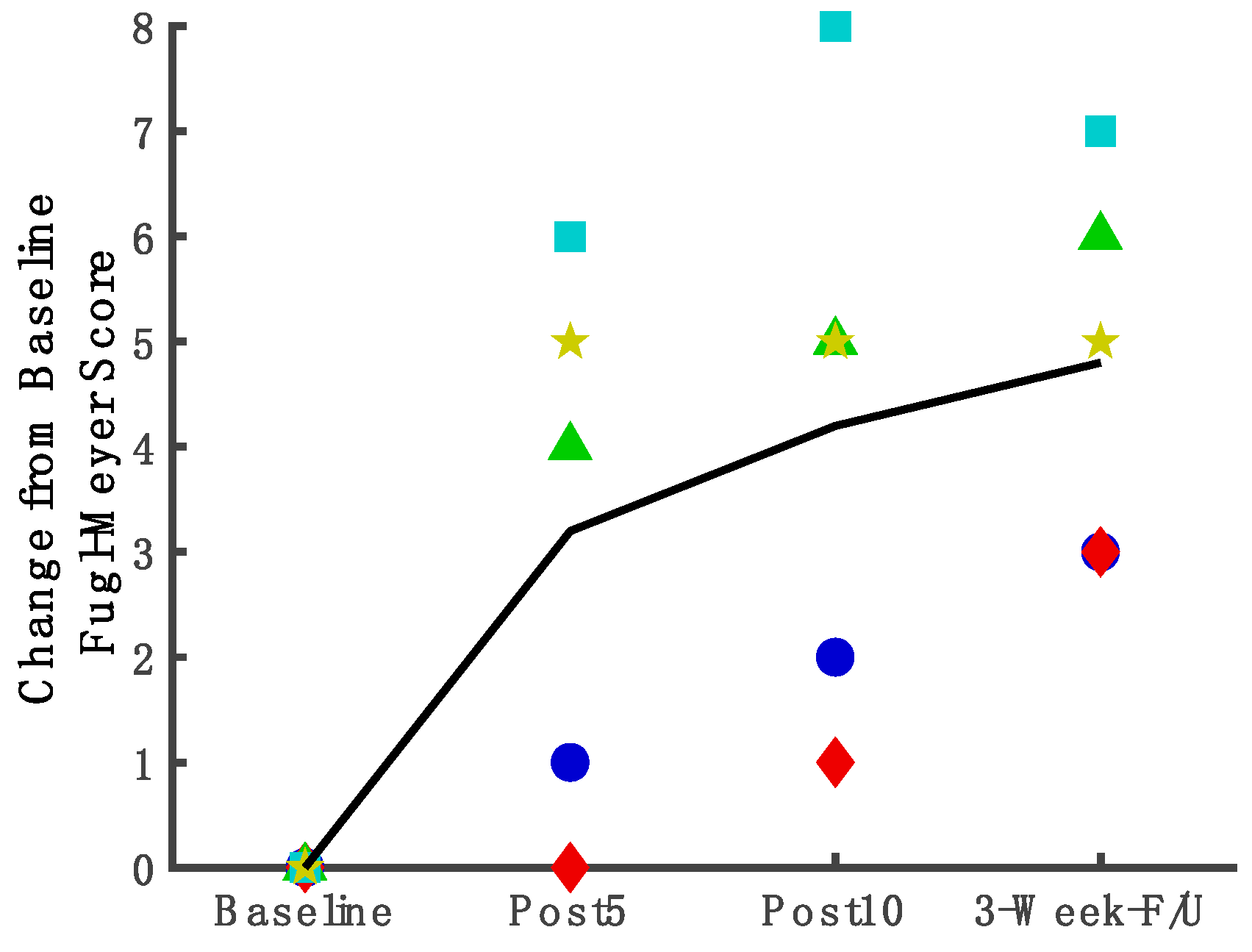
3.5. Measures Assessing Underlying Factors of Stance Phase Control and Coordination of Joint Movements
4. Discussion
4.1. Non-Invasive Brain Stimulation Can Enhance Brain Excitability and Can Be Feasibly Administered to Stroke Survivors within the Framework of A Stance Phase Coordination, Motor Learning Protocol
4.2. Combined Intervention Using Technologies and Motor Learning Principles Provided a Finely Incrementalized Method for Stance Phase Practice
4.3. Combined with Brain Stimulation, Dynamic Stance Phase Motor Exercises Showed Statistically Significant Improvement in Functional Mobility
4.4. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Virani, S.S.; Alonso, A.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics—2020 Update: A Report From the American Heart Association. Circulation 2020, 141, e139–e596. [Google Scholar] [CrossRef] [PubMed]
- Cirstea, C.M. Gait Rehabilitation After Stroke: Should We Re-Evaluate Our Practice? Stroke 2020, 51, 2892–2894. [Google Scholar] [CrossRef] [PubMed]
- Daly, J.J.; McCabe, J.P.; Gansen, J.; Rogers, J.; Butler, K.; Brenner, I.; Burdsall, R.; Nethery, J. Gait Coordination Protocol for Recovery of Coordinated Gait, Function, and Quality of Life Following Stroke. J. Rehabil. Res. Dev. 2012, 49, xix–xxviii. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Francisco, G.E.; Zhou, P. Post-Stroke Hemiplegic Gait: New Perspective and Insights. Front. Physiol. 2018, 9, 1021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sánchez, N.; Finley, J.M. Individual Differences in Locomotor Function Predict the Capacity to Reduce Asymmetry and Modify the Energetic Cost of Walking Poststroke. Neurorehabil. Neural Repair 2018, 32, 701–713. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Mukaino, M.; Ohtsuka, K.; Otaka, Y.; Tanikawa, H.; Matsuda, F.; Tsuchiyama, K.; Yamada, J.; Saitoh, E. Gait Characteristics of Post-Stroke Hemiparetic Patients with Different Walking Speeds. Int. J. Rehabil. Res. 2020, 43, 69–75. [Google Scholar] [CrossRef]
- Carr, J.; Shepherd, R. Stroke Rehabilitation: Guidelines for Exercise and Training to Optimize Motor Skill; Elselvier Science Limited: Amsterdam, The Netherlands, 2003. [Google Scholar]
- Hornby, T.G.; Campbell, D.D.; Kahn, J.H.; Demott, T.; Moore, J.L.; Roth, H.R. Enhanced Gait-Related Improvements after Therapist-versus Robotic-Assisted Locomotor Training in Subjects with Chronic Stroke: A Randomized Controlled Study. Stroke 2008, 39, 1786–1792. [Google Scholar] [CrossRef]
- Moore, J.L.; Roth, E.J.; Killian, C.; Hornby, T.G. Locomotor Training Improves Daily Stepping Activity and Gait Efficiency in Individuals Poststroke Who Have Reached a “Plateau” in Recovery. Stroke 2010, 41, 129–135. [Google Scholar] [CrossRef]
- Hornby, T.G.; Straube, D.S.; Kinnaird, C.R.; Holleran, C.L.; Echauz, A.J.; Rodriguez, K.S.; Wagner, E.J.; Narducci, E.A. Importance of Specificity, Amount, and Intensity of Locomotor Training to Improve Ambulatory Function in Patients Poststroke. Top. Stroke Rehabil. 2011, 18, 293–307. [Google Scholar] [CrossRef]
- Routson, R.L.; Clark, D.J.; Bowden, M.G.; Kautz, S.A.; Neptune, R.R. The Influence of Locomotor Rehabilitation on Module Quality and Post-Stroke Hemiparetic Walking Performance. Gait. Posture 2013, 38, 511–517. [Google Scholar] [CrossRef] [Green Version]
- Hollands, K.L.; Pelton, T.A.; Tyson, S.F.; Hollands, M.A.; van Vliet, P.M. Interventions for Coordination of Walking Following Stroke: Systematic Review. Gait. Posture 2012, 35, 349–359. [Google Scholar] [CrossRef] [PubMed]
- Daly, J.J.; Zimbelman, J.; Roenigk, K.L.; McCabe, J.P.; Rogers, J.M.; Butler, K.; Burdsall, R.; Holcomb, J.P.; Marsolais, E.B.; Ruff, R.L. Recovery of Coordinated Gait: Randomized Controlled Stroke Trial of Functional Electrical Stimulation (FES) versus No FES, with Weight-Supported Treadmill and over-Ground Training. Neurorehabil. Neural Repair 2011, 25, 588–596. [Google Scholar] [CrossRef] [PubMed]
- Pundik, S.; Holcomb, J.; McCabe, J.; Daly, J.J. Enhanced Life-Role Participation in Response to Comprehensive Gait Training in Chronic-Stroke Survivors. Disabil. Rehabil. 2012, 34, 1535–1539. [Google Scholar] [CrossRef] [PubMed]
- Leech, K.A.; Roemmich, R.T.; Gordon, J.; Reisman, D.S.; Cherry-Allen, K.M. Updates in Motor Learning: Implications for Physical Therapist Practice and Education. Phys. Ther. 2022, 102, pzab250. [Google Scholar] [CrossRef]
- Maier, M.; Ballester, B.R.; Verschure, P.F.M.J. Principles of Neurorehabilitation After Stroke Based on Motor Learning and Brain Plasticity Mechanisms. Front. Syst. Neurosci. 2019, 13, 74. [Google Scholar] [CrossRef]
- Sakuma, K.; Tateuchi, H.; Nishishita, S.; Okita, Y.; Kitatani, R.; Koyama, Y.; Ibuki, S.; Ichihashi, N. Immediate Effects of Stance and Swing Phase Training on Gait in Patients with Stroke. Int. J. Rehabil. Res. 2021, 44, 152–158. [Google Scholar] [CrossRef]
- Moore, J.L.; Nordvik, J.E.; Erichsen, A.; Rosseland, I.; Bø, E.; Hornby, T.G.; Barkenæs, T.; Bratlie, H.; Byhring, M.; Grimstad, I.; et al. Implementation of High-Intensity Stepping Training During Inpatient Stroke Rehabilitation Improves Functional Outcomes. Stroke 2020, 51, 563–570. [Google Scholar] [CrossRef]
- Radman, T.; Ramos, R.L.; Brumberg, J.C.; Bikson, M. Role of Cortical Cell Type and Morphology in Subthreshold and Suprathreshold Uniform Electric Field Stimulation in Vitro. Brain Stimul. 2009, 2, 215–228.e3. [Google Scholar] [CrossRef] [Green Version]
- Lefebvre, S.; Dricot, L.; Laloux, P.; Desfontaines, P.; Evrard, F.; Peeters, A.; Jamart, J.; Vandermeeren, Y. Increased Functional Connectivity One Week after Motor Learning and TDCS in Stroke Patients. Neuroscience 2017, 340, 424–435. [Google Scholar] [CrossRef]
- Chang, M.C.; Kim, D.Y.; Park, D.H. Enhancement of Cortical Excitability and Lower Limb Motor Function in Patients with Stroke by Transcranial Direct Current Stimulation. Brain Stimul. 2015, 8, 561–566. [Google Scholar] [CrossRef]
- Yamada, Y.; Sumiyoshi, T. Neurobiological Mechanisms of Transcranial Direct Current Stimulation for Psychiatric Disorders; Neurophysiological, Chemical, and Anatomical Considerations. Front. Hum. Neurosci. 2021, 15, 631838. [Google Scholar] [CrossRef] [PubMed]
- Morya, E.; Monte-Silva, K.; Bikson, M.; Esmaeilpour, Z.; Biazoli, C.E.; Fonseca, A.; Bocci, T.; Farzan, F.; Chatterjee, R.; Hausdorff, J.M.; et al. Beyond the Target Area: An Integrative View of TDCS-Induced Motor Cortex Modulation in Patients and Athletes. J. NeuroEng. Rehabil. 2019, 16, 141. [Google Scholar] [CrossRef] [PubMed]
- Santos Ferreira, I.; Teixeira Costa, B.; Lima Ramos, C.; Lucena, P.; Thibaut, A.; Fregni, F. Searching for the Optimal TDCS Target for Motor Rehabilitation. J. Neuroeng. Rehabil. 2019, 16, 90. [Google Scholar] [CrossRef] [PubMed]
- Hsu, W.Y.; Cheng, C.H.; Liao, K.K.; Lee, I.H.; Lin, Y.Y. Effects of Repetitive Transcranial Magnetic Stimulation on Motor Functions in Patients with Stroke: A Meta-Analysis. Stroke 2012, 43, 1849–1857. [Google Scholar] [CrossRef] [Green Version]
- Chieffo, R.; Comi, G.; Leocani, L. Noninvasive Neuromodulation in Poststroke Gait Disorders: Rationale, Feasibility, and State of the Art. Neurorehabil. Neural Repair 2016, 30, 71–82. [Google Scholar] [CrossRef]
- Madhavan, S.; Cleland, B.T.; Sivaramakrishnan, A.; Freels, S.; Lim, H.; Testai, F.D.; Corcos, D.M. Cortical Priming Strategies for Gait Training after Stroke: A Controlled, Stratified Trial. J. Neuroeng. Rehabil. 2020, 17, 111. [Google Scholar] [CrossRef]
- Park, S.D.; Kim, J.Y.; Song, H.S. Effect of Application of Transcranial Direct Current Stimulation during Task-Related Training on Gait Ability of Patients with Stroke. J. Phys. Ther. Sci. 2015, 27, 623–625. [Google Scholar] [CrossRef] [Green Version]
- Kakuda, W.; Abo, M.; Nakayama, Y.; Kiyama, A.; Yoshida, H. High-Frequency RTMS Using a Double Cone Coil for Gait Disturbance. Acta Neurol. Scand. 2013, 128, 100–106. [Google Scholar] [CrossRef]
- Wang, R.Y.; Tseng, H.Y.; Liao, K.K.; Wang, C.J.; Lai, K.L.; Yang, Y.R. RTMS Combined with Task-Oriented Training to Improve Symmetry of Interhemispheric Corticomotor Excitability and Gait Performance after Stroke: A Randomized Trial. Neurorehabil. Neural Repair 2012, 26, 222–230. [Google Scholar] [CrossRef]
- Madhavan, S.; Weber, K.A.; Stinear, J.W. Non-Invasive Brain Stimulation Enhances Fine Motor Control of the Hemiparetic Ankle: Implications for Rehabilitation. Exp. Brain Res. 2011, 209, 9–17. [Google Scholar] [CrossRef]
- de Rooij, I.J.; van de Port, I.G.; Meijer, J.W.G. Feasibility and Effectiveness of Virtual Reality Training on Balance and Gait Recovery Early after Stroke: A Pilot Study. Int. J. Phys. Med. Rehabil. 2017, 5, 418. [Google Scholar] [CrossRef]
- Corbetta, D.; Imeri, F.; Gatti, R. Rehabilitation That Incorporates Virtual Reality Is More Effective than Standard Rehabilitation for Improving Walking Speed, Balance and Mobility after Stroke: A Systematic Review. J. Physiother. 2015, 61, 117–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fung, J.; Richards, C.L.; Malouin, F.; McFadyen, B.J.; Lamontagne, A. A Treadmill and Motion Coupled Virtual Reality System for Gait Training Post-Stroke. Cyberpsychol. Behav. 2006, 9, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Rossi, S.; Hallett, M.; Rossini, P.M.; Pascual-Leone, A. Safety, Ethical Considerations, and Application Guidelines for the Use of Transcranial Magnetic Stimulation in Clinical Practice and Research. Clin. Neurophysiol. 2009, 120, 2008–2039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, Y.; Thomas, C.; Datta, A.; Parra, L.C. Optimized TDCS for Targeting Multiple Brain Regions: An Integrated Implementation. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 17–22 July 2018; pp. 3545–3548. [Google Scholar]
- Dong, K.; Meng, S.; Guo, Z.; Zhang, R.; Xu, P.; Yuan, E.; Lian, T. The Effects of Transcranial Direct Current Stimulation on Balance and Gait in Stroke Patients: A Systematic Review and Meta-Analysis. Front. Neurol. 2021, 12, 650925. [Google Scholar] [CrossRef] [PubMed]
- Fusco, A.; De Angelis, D.; Morone, G.; Maglione, L.; Paolucci, T.; Bragoni, M.; Venturiero, V. The ABC of TDCS: Effects of Anodal, Bilateral and Cathodal Montages of Transcranial Direct Current Stimulation in Patients with Stroke—A Pilot Study. Stroke Res. Treat. 2013, 2013, 837595. [Google Scholar] [CrossRef] [PubMed]
- Jayaram, G.; Stinear, J.W. The Effects of Transcranial Stimulation on Paretic Lower Limb Motor Excitability during Walking. J. Clin. Neurophysiol. 2009, 26, 272–279. [Google Scholar] [CrossRef]
- Feng, W.; Kautz, S.A.; Schlaug, G.; Meinzer, C.; George, M.S.; Chhatbar, P.Y. Transcranial Direct Current Stimulation for Poststroke Motor Recovery: Challenges and Opportunities. PM R 2018, 10, S157–S164. [Google Scholar] [CrossRef] [Green Version]
- TDCS Overview—Transcranial Direct Current Stimulation—Soterix Medical. Available online: https://soterixmedical.com/research/1x1/tdcs (accessed on 28 April 2022).
- Chhatbar, P.Y.; Ramakrishnan, V.; Kautz, S.; George, M.S.; Adams, R.J.; Feng, W. Transcranial Direct Current Stimulation Post-Stroke Upper Extremity Motor Recovery Studies Exhibit a Dose–Response Relationship. Brain Stimul. 2016, 9, 16–26. [Google Scholar] [CrossRef] [Green Version]
- Bolognini, N.; Russo, C.; Souza Carneiro, M.I.; Nicotra, A.; Olgiati, E.; Spandri, V.; Agostoni, E.; Salmaggi, A.; Vallar, G. Bi-Hemispheric Transcranial Direct Current Stimulation for Upper-Limb Hemiparesis in Acute Stroke: A Randomized, Double-Blind, Sham-Controlled Trial. Eur. J. Neurol. 2020, 27, 2473–2482. [Google Scholar] [CrossRef]
- Gugino, L.D.; Romero, J.R.; Aglio, L.; Titone, D.; Ramirez, M.; Pascual-Leone, A.; Grimson, E.; Weisenfeld, N.; Kikinis, R.; Shenton, M.E. Transcranial Magnetic Stimulation Coregistered with MRI: A Comparison of a Guided versus Blind Stimulation Technique and Its Effect on Evoked Compound Muscle Action Potentials. Clin. Neurophysiol. 2001, 112, 1781–1792. [Google Scholar] [CrossRef] [Green Version]
- Rossini, P.M.; Burke, D.; Chen, R.; Cohen, L.G.; Daskalakis, Z.; Di Iorio, R.; Di Lazzaro, V.; Ferreri, F.; Fitzgerald, P.B.; George, M.S.; et al. Non-Invasive Electrical and Magnetic Stimulation of the Brain, Spinal Cord, Roots and Peripheral Nerves: Basic Principles and Procedures for Routine Clinical and Research Application. An Updated Report from an I.F.C.N. Committee. Clin. Neurophysiol. 2015, 126, 1071–1107. [Google Scholar] [CrossRef] [PubMed]
- Bikson, M.; Rahman, A.; Datta, A. Computational Models of Transcranial Direct Current Stimulation. Clin. EEG Neurosci. 2012, 43, 176–183. [Google Scholar] [CrossRef] [PubMed]
- Datta, A.; Baker, J.M.; Bikson, M.; Fridriksson, J. Individualized Model Predicts Brain Current Flow during Transcranial Direct-Current Stimulation Treatment in Responsive Stroke Patient. Brain Stimul. 2011, 4, 169–174. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.; Liu, A.A.; Lafon, B.; Friedman, D.; Dayan, M.; Wang, X.; Bikson, M.; Doyle, W.K.; Devinsky, O.; Parra, L.C. Measurements and Models of Electric Fields in the in Vivo Human Brain during Transcranial Electric Stimulation. eLife 2017, 6, e18834. [Google Scholar] [CrossRef]
- Bushnell, C.; Bettger, J.P.; Cockroft, K.M.; Cramer, S.C.; Edelen, M.O.; Hanley, D.; Katzan, I.L.; Mattke, S.; Nilsen, D.M.; Piquado, T.; et al. Chronic Stroke Outcome Measures for Motor Function Intervention Trials: Expert Panel Recommendations. Circ. Cardiovasc. Qual. Outcomes 2015, 8, S163–S169. [Google Scholar] [CrossRef] [Green Version]
- Fulk, G.D.; Ludwig, M.; Dunning, K.; Golden, S.; Boyne, P.; West, T. Estimating Clinically Important Change in Gait Speed in People with Stroke Undergoing Outpatient Rehabilitation. J. Neurol. Phys. Ther. 2011, 35, 82–89. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The Timed “Up & Go”: A Test of Basic Functional Mobility for Frail Elderly Persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef]
- Chan, P.P.; Si Tou, J.I.; Tse, M.M.; Ng, S.S. Reliability and Validity of the Timed Up and Go Test with a Motor Task in People with Chronic Stroke. Arch. Phys. Med. Rehabil. 2017, 98, 2213–2220. [Google Scholar] [CrossRef]
- Lin, J.-H.; Hsu, M.-J.; Hsu, H.-W.; Wu, H.-C.; Hsieh, C.-L. Psychometric Comparisons of 3 Functional Ambulation Measures for Patients with Stroke. Stroke 2010, 41, 2021–2025. [Google Scholar] [CrossRef] [Green Version]
- Beninato, M.; Fernandes, A.; Plummer, L.S. Minimal Clinically Important Difference of the Functional Gait Assessment in Older Adults. Phys. Ther. 2014, 94, 1594–1603. [Google Scholar] [CrossRef] [PubMed]
- Fugl-Meyer, A.R.; Jaasko, L.; Leyman, I.; Olsson, S.; Steglind, S. The Post-Stroke Hemiplegic Patient. 1. A Method for Evaluation of Physical Performance. Scand. J. Rehabil. Med. 1975, 7, 13–31. [Google Scholar] [PubMed]
- Mehrholz, J.; Pohl, M.; Elsner, B. Treadmill Training and Body Weight Support for Walking after Stroke. Cochrane Database Syst. Rev. 2014, 8, CD002840. [Google Scholar] [CrossRef]
- Moreira, M.C.; de Amorim Lima, A.M.; Ferraz, K.M.; Benedetti Rodrigues, M.A. Use of Virtual Reality in Gait Recovery among Post Stroke Patients—A Systematic Literature Review. Disabil. Rehabil. Assist. Technol. 2013, 8, 357–362. [Google Scholar] [CrossRef]
- Pennycott, A.; Wyss, D.; Vallery, H.; Klamroth-Marganska, V.; Riener, R. Towards More Effective Robotic Gait Training for Stroke Rehabilitation: A Review. J. Neuroeng. Rehabil. 2012, 9, 65. [Google Scholar] [CrossRef] [Green Version]
- Bonnyaud, C.; Pradon, D.; Zory, R.; Bussel, B.; Bensmail, D.; Vuillerme, N.; Roche, N. Effects of a Gait Training Session Combined with a Mass on the Non-Paretic Lower Limb on Locomotion of Hemiparetic Patients: A Randomized Controlled Clinical Trial. Gait. Posture. 2013, 37, 627–630. [Google Scholar] [CrossRef]
- Caliandro, P.; Molteni, F.; Simbolotti, C.; Guanziroli, E.; Iacovelli, C.; Reale, G.; Giovannini, S.; Padua, L. Exoskeleton-Assisted Gait in Chronic Stroke: An EMG and Functional near-Infrared Spectroscopy Study of Muscle Activation Patterns and Prefrontal Cortex Activity. Clin. Neurophysiol. 2020, 131, 1775–1781. [Google Scholar] [CrossRef]
- Feng, W.W.; Bowden, M.G.; Kautz, S. Review of Transcranial Direct Current Stimulation in Poststroke Recovery. Top. Stroke Rehabil. 2013, 20, 68–77. [Google Scholar] [CrossRef]
- Lindenberg, R.; Renga, V.; Zhu, L.L.; Nair, D.; Schlaug, G. Bihemispheric Brain Stimulation Facilitates Motor Recovery in Chronic Stroke Patients. Neurology 2010, 75, 2176–2184. [Google Scholar] [CrossRef]
- Alisar, D.C.; Ozen, S.; Sozay, S. Effects of Bihemispheric Transcranial Direct Current Stimulation on Upper Extremity Function in Stroke Patients: A Randomized Double-Blind Sham-Controlled Study. J. Stroke Cereb. Dis. 2020, 29, 104454. [Google Scholar] [CrossRef]
- Learmonth, G.; Benwell, C.S.Y.; Märker, G.; Dascalu, D.; Checketts, M.; Santosh, C.; Barber, M.; Walters, M.; Muir, K.W.; Harvey, M. Non-Invasive Brain Stimulation in Stroke Patients (NIBS): A Prospective Randomized Open Blinded End-Point (PROBE) Feasibility Trial Using Transcranial Direct Current Stimulation (TDCS) in Post-Stroke Hemispatial Neglect. Neuropsychol. Rehabil. 2021, 31, 1163–1189. [Google Scholar] [CrossRef] [PubMed]
- Bikson, M.; Grossman, P.; Thomas, C.; Zannou, A.L.; Jiang, J.; Adnan, T.; Mourdoukoutas, A.P.; Kronberg, G.; Truong, D.; Boggio, P.; et al. Safety of Transcranial Direct Current Stimulation: Evidence Based Update 2016. Brain Stimul. 2016, 9, 641–661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, A.; Vöröslakos, M.; Kronberg, G.; Henin, S.; Krause, M.R.; Huang, Y.; Opitz, A.; Mehta, A.; Pack, C.C.; Krekelberg, B.; et al. Immediate Neurophysiological Effects of Transcranial Electrical Stimulation. Nat. Commun. 2018, 9, 5092. [Google Scholar] [CrossRef] [PubMed]
- Datta, A.; Bansal, V.; Diaz, J.; Patel, J.; Reato, D.; Bikson, M. Gyri-Precise Head Model of Transcranial Direct Current Stimulation: Improved Spatial Focality Using a Ring Electrode versus Conventional Rectangular Pad. Brain Stimul. 2009, 2, 201–207.e1. [Google Scholar] [CrossRef] [Green Version]
- Ruffini, G.; Wendling, F.; Merlet, I.; Molaee-Ardekani, B.; Mekonnen, A.; Salvador, R.; Soria-Frisch, A.; Grau, C.; Dunne, S.; Miranda, P.C. Transcranial Current Brain Stimulation (TCS): Models and Technologies. IEEE Trans. Neural Syst. Rehabil. Eng. 2013, 21, 333–345. [Google Scholar] [CrossRef]
- Datta, A.; Truong, D.; Minhas, P.; Parra, L.C.; Bikson, M. Inter-Individual Variation during Transcranial Direct Current Stimulation and Normalization of Dose Using MRI-Derived Computational Models. Front. Psychiatry 2012, 3, 91. [Google Scholar] [CrossRef] [Green Version]
- Llera, A.; Wolfers, T.; Mulders, P.; Beckmann, C.F. Inter-Individual Differences in Human Brain Structure and Morphology Link to Variation in Demographics and Behavior. eLife 2019, 8, e44443. [Google Scholar] [CrossRef]
- Tahtis, V.; Kaski, D.; Seemungal, B.M. The Effect of Single Session Bi-Cephalic Transcranial Direct Current Stimulation on Gait Performance in Sub-Acute Stroke: A Pilot Study. Restor. Neurol. Neurosci. 2014, 32, 527–532. [Google Scholar] [CrossRef]
- Singh, R.E.; Iqbal, K.; White, G. Proficiency-Based Recruitment of Muscle Synergies in a Highly Perturbed Walking Task (Slackline). Eng. Rep. 2020, 2, e12253. [Google Scholar] [CrossRef]
- Boissoneault, C.; Grimes, T.; Rose, D.K.; Waters, M.F.; Khanna, A.; Datta, S.; Daly, J.J. Innovative Long-Dose Neurorehabilitation for Balance and Mobility in Chronic Stroke: A Preliminary Case Series. Brain Sci. 2020, 10, 555. [Google Scholar] [CrossRef]
- Boissoneault, C.; Rose, D.K.; Grimes, T.; Waters, M.F.; Khanna, A.; Datta, S.; Daly, J.J. Trajectories of Stroke Recovery of Impairment, Function, and Quality of Life in Response to 12-Month Mobility and Fitness Intervention. NeuroRehabilitation 2021, 49, 573–584. [Google Scholar] [CrossRef] [PubMed]
- Thair, H.; Holloway, A.L.; Newport, R.; Smith, A.D. Transcranial Direct Current Stimulation (TDCS): A Beginner’s Guide for Design and Implementation. Front. Neurosci. 2017, 11, 641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, E.K.; Kim, Y.K.; Sohn, H.M.; Cohen, L.G.; Paik, N.J. Improved Picture Naming in Aphasia Patients Treated with Cathodal TDCS to Inhibit the Right Broca’s Homologue Area. Restor. Neurol. Neurosci. 2011, 29, 141–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, I.; Yeldan, I.; Mustafaoglu, R. The Adjunct of Electric Neurostimulation to Rehabilitation Approaches in Upper Limb Stroke Rehabilitation: A Systematic Review with Network Meta-Analysis of Randomized Controlled Trials. Neuromodulation, 2022; ahead of print. [Google Scholar] [CrossRef]
- Lazzaro, G.; Fucà, E.; Caciolo, C.; Battisti, A.; Costanzo, F.; Varuzza, C.; Vicari, S.; Menghini, D. Understanding the Effects of Transcranial Electrical Stimulation in Numerical Cognition: A Systematic Review for Clinical Translation. J. Clin. Med. 2022, 11, 2082. [Google Scholar] [CrossRef]
- Tilson, J.K.; Sullivan, K.J.; Cen, S.Y.; Rose, D.K.; Koradia, C.H.; Azen, S.P.; Duncan, P.W. Locomotor Experience Applied Post Stroke (LEAPS) Investigative Team Meaningful Gait Speed Improvement during the First 60 Days Poststroke: Minimal Clinically Important Difference. Phys. Ther. 2010, 90, 196–208. [Google Scholar] [CrossRef]
- Jaffe, D.L.; Brown, D.A.; Pierson-Carey, C.D.; Buckley, E.L.; Lew, H.L. Stepping over Obstacles to Improve Walking in Individuals with Poststroke Hemiplegia. J. Rehabil. Res. Dev. 2004, 41, 283–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohannon, R.W.; Glenney, S.S. Minimal Clinically Important Difference for Change in Comfortable Gait Speed of Adults with Pathology: A Systematic Review. J. Eval. Clin. Pract. 2014, 20, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Flansbjer, U.B.; Holmback, A.M.; Downham, D.; Patten, C.; Lexell, J. Reliability of Gait Performance Tests in Men and Women with Hemiparesis after Stroke. J. Rehabil. Med. 2005, 37, 75–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| User | Age | Gender | Months Post Stroke | Lesioned Hemisphere | Stroke Type |
|---|---|---|---|---|---|
S1  | 58 | Male | 64 | Left | Hemorrhagic |
S2  | 55 | Male | 36 | Left | Hemorrhagic |
S3  | 56 | Male | 158 | Left | Ischemic |
S4  | 52 | Male | 21 | Right | Ischemic |
S5  | 72 | Male | 61 | Left | Ischemic |
| User | Fugl-Meyer (Points) | Gait Speed (m/s) | TUG (s) | FGA (Points) |
|---|---|---|---|---|
| S1 | 28 | 1.03 | 11.50 | 17 |
| S2 | 22 | 0.96 | 13.61 | 14 |
| S3 | 17 | 1.16 | 7.73 | 8 |
| S4 | 17 | 0.39 | 27.24 | 11 |
| S5 | 22 | 1.11 | 11.92 | 16 |
| Mean (SD) | 21.2 (4.5) | 0.93 (0.31) | 14.40 (7.49) | 13.2 (3.7) |
| Feasibility Factors | Findings |
|---|---|
| User (stroke survivors) recruitment | Eight stroke survivor users were evaluated for participation in the study. Five met the inclusion criteria and completed the study. |
| Retention for the planned duration of the treatment and testing time | All five enrolled users completed all treatment and testing sessions |
| User preparation and donning time of equipment | Equipment donning required an average of 15 min. |
| Reported comfort of the system | Users reported no discomfort regarding tDCS electrode placement or current intensity. Users reported no discomfort with the harness system or visual/auditory features of the VR. |
| Capability to wear and use the technologies. | All five users were able to wear the technologies and reported engagement in the presented motor tasks during tDCS and VR/treadmill training. |
| User endurance of the technologies for the planned treatment time | All five users demonstrated endurance for the length of each treatment session. We found it important to offer rest periods between walking practice trials on the treadmill and during phase two overground practice. Users performed a mean of 191.8 ± 32.8 (SD) obstacle-clearance steps per VR treadmill training session. |
| Technology flexibility in providing the incremental levels of difficulty needed for progressively more challenging motor learning stance phase practice | The technology offered numerous domains across which task difficulty could be progressed. These included treadmill speed, timing of the frequency of walking obstacles in the VR system, height of obstacles in the VR system, use of knee cage to protect joint structures during walking practice, ankle dorsi-flex assist to protect knee joint structures and assist with swing phase dorsiflexion, upper limb support, physical assist by the treating therapist, and verbal cues from the treating therapist. ** |
| User’s ability to attempt the progression of planned challenges during stance phase motor learning | All five users showed capability to attempt task progression across one or more domains of task difficulty. |
| Ability to show progressive improvement in performing progressively more challenging aspects of the motor learning protocol using the technologies | All five users progressed across one or more domains of task difficulty (details provided below in the results for individual users). |
| Safety | All participants completed 10 training sessions with no adverse events. No users experienced a fall or near fall. |
| Users | Baseline | After Treatment |
|---|---|---|
| S1 | Uncontrolled/forceful knee hyperextension during weight shift/forward stepping and during mid- to terminal stance at chosen gait speed | Knee maintained in neutral position (no hyperextension) during weight shift/forward stepping at slow speed with focused attention/ upper limb support. Knee hyperextension only in very late stance with less force at chosen gait speed |
| S2 | Knee hyperextension, pelvic retraction, +Trendelenberg sign * and forward flexed trunk when attempting to bear weight on the paretic limb. | Improved alignment of trunk/pelvis/hip/knee/ankle during weight shift and stepping practice; controlling knee in neutral with upper limb support while shifting weight onto paretic limb. |
| S3 | Severe/forceful knee hyperextension, +Trendelenberg sign, and pelvic retraction when attempting to bear weight on the paretic limb. | Able to protect the knee joint from excessive hyperextension forces during weight bearing by working on stance with the knee in 10° flexion. Improved alignment of paretic pelvis/hip/knee/ankle during forward weight shift to midstance. |
| S4 | Knee hyperextension, pelvic retraction with hip external rotation, +Trendelenberg sign with center of mass between quad cane, and non-paretic limb. Step-to gait pattern with decreased time in single limb support on paretic limb. | Improved alignment of paretic pelvis/hip/knee/ankle during weight bearing with upper limb support. During chosen speed walking, taking longer steps with uninvolved limb, and pelvic retraction lessened. |
| S5 | Knee hyperflexion,+Trendeleberg sign, with center of mass maintained between the non-paretic limb and quad cane. | Improved alignment of paretic pelvis/hip/knee/ankle during weight bearing with upper limb support, demonstrating knee control at neutral. During chosen speed walking, exhibited improved knee position (less flexion) during stance phase. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salameh, A.; McCabe, J.; Skelly, M.; Duncan, K.R.; Chen, Z.; Tatsuoka, C.; Bikson, M.; Hardin, E.C.; Daly, J.J.; Pundik, S. Stance Phase Gait Training Post Stroke Using Simultaneous Transcranial Direct Current Stimulation and Motor Learning-Based Virtual Reality-Assisted Therapy: Protocol Development and Initial Testing. Brain Sci. 2022, 12, 701. https://doi.org/10.3390/brainsci12060701
Salameh A, McCabe J, Skelly M, Duncan KR, Chen Z, Tatsuoka C, Bikson M, Hardin EC, Daly JJ, Pundik S. Stance Phase Gait Training Post Stroke Using Simultaneous Transcranial Direct Current Stimulation and Motor Learning-Based Virtual Reality-Assisted Therapy: Protocol Development and Initial Testing. Brain Sciences. 2022; 12(6):701. https://doi.org/10.3390/brainsci12060701
Chicago/Turabian StyleSalameh, Ahlam, Jessica McCabe, Margaret Skelly, Kelsey Rose Duncan, Zhengyi Chen, Curtis Tatsuoka, Marom Bikson, Elizabeth C. Hardin, Janis J. Daly, and Svetlana Pundik. 2022. "Stance Phase Gait Training Post Stroke Using Simultaneous Transcranial Direct Current Stimulation and Motor Learning-Based Virtual Reality-Assisted Therapy: Protocol Development and Initial Testing" Brain Sciences 12, no. 6: 701. https://doi.org/10.3390/brainsci12060701